
The Reliability and Validation of the Children’s Eating Attitude Test among Chinese Samples
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. ChEAT
2.2.2. Children’s BMI
2.3. Statistical Analysis
3. Results
3.1. Demographic Information of Children
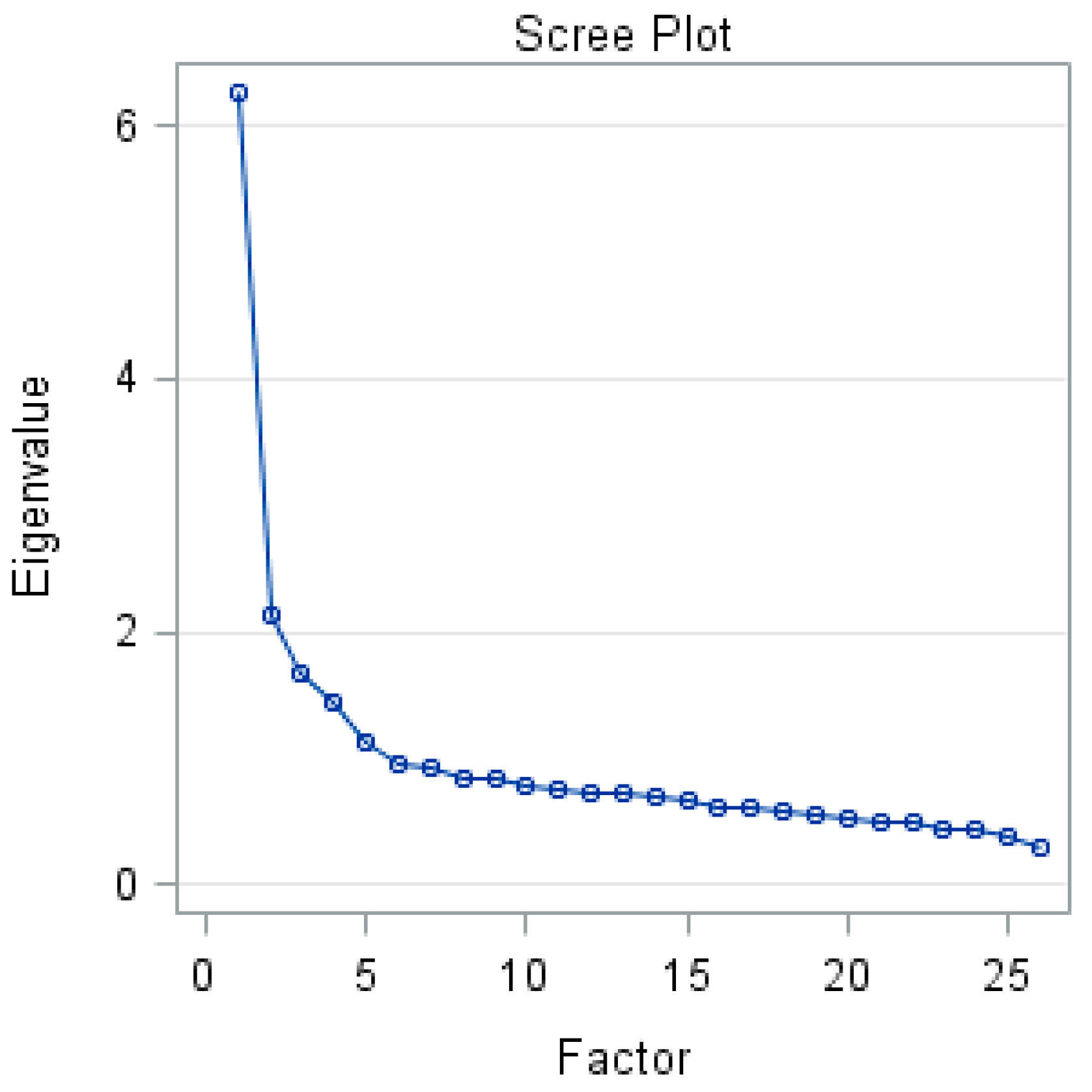
3.2. Exploratory Factor Analysis
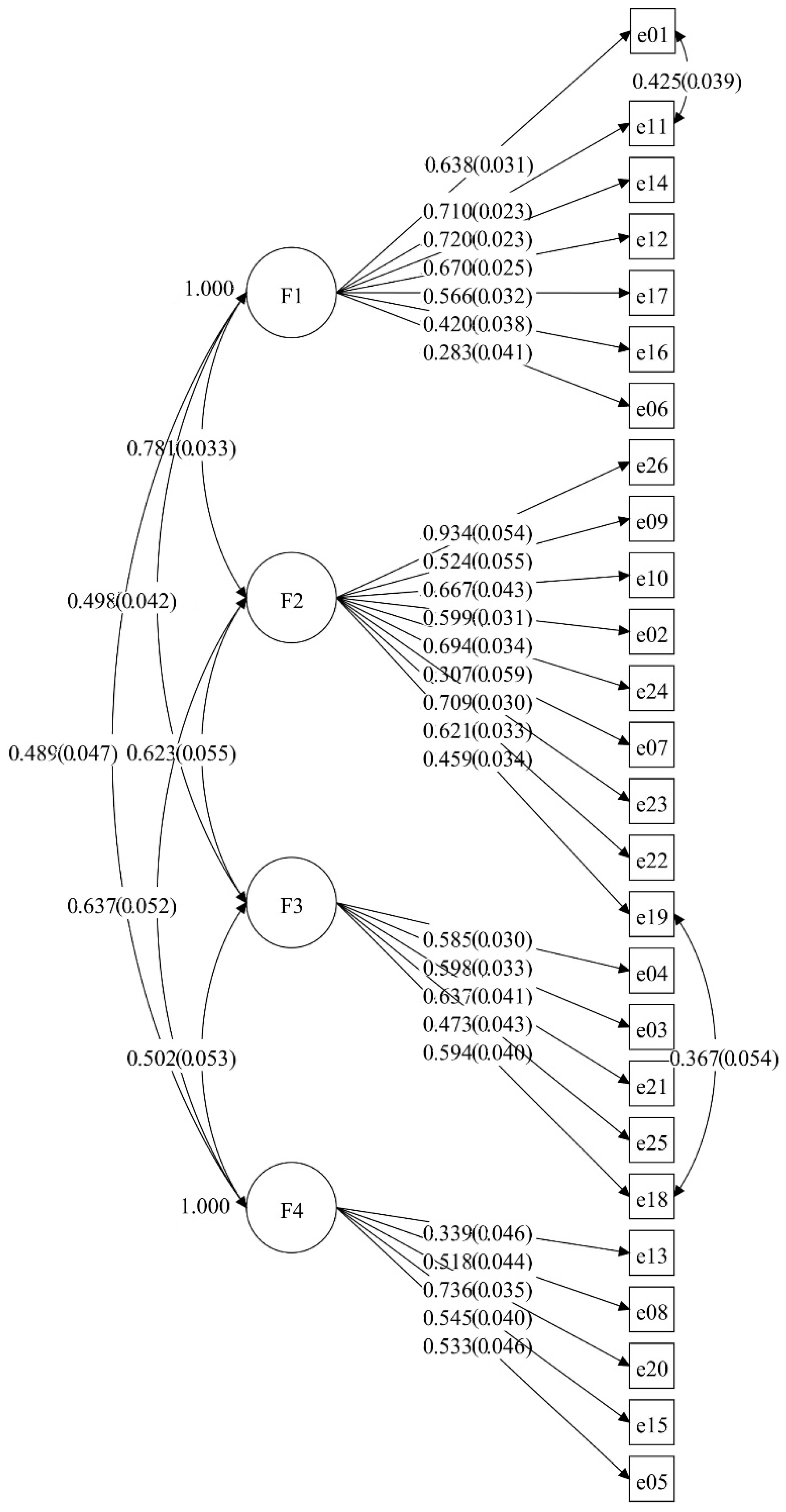
3.3. Confirmatory Factor Analysis (CFA)
3.4. Reliability of the ChEAT
3.5. Descriptive Statistics of the ChEAT
3.6. The Associations between ChEAT Scores and BMI
3.7. The ChEAT Scores in Different BMI Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Factor | Item | Estimate | S.E. | Est./S.E. | AVE | CR |
|---|---|---|---|---|---|---|
| F1 | 0.351 | 0.779 | ||||
| E01 | 0.638 | 0.031 | 20.291 | |||
| E11 | 0.710 | 0.023 | 31.414 | |||
| E14 | 0.720 | 0.023 | 31.051 | |||
| E12 | 0.670 | 0.025 | 27.201 | |||
| E17 | 0.566 | 0.032 | 17.943 | |||
| E16 | 0.420 | 0.038 | 10.956 | |||
| E06 | 0.283 | 0.041 | 6.937 | |||
| F2 | 0.403 | 0.850 | ||||
| E26 | 0.934 | 0.054 | 17.284 | |||
| E09 | 0.524 | 0.055 | 9.583 | |||
| E10 | 0.667 | 0.043 | 15.392 | |||
| E02 | 0.599 | 0.031 | 19.213 | |||
| E24 | 0.694 | 0.034 | 20.721 | |||
| E07 | 0.307 | 0.059 | 5.218 | |||
| E23 | 0.709 | 0.030 | 23.645 | |||
| E22 | 0.621 | 0.033 | 18.699 | |||
| E19 | 0.459 | 0.034 | 13.605 | |||
| F3 | 0.336 | 0.715 | ||||
| E04 | 0.585 | 0.030 | 19.793 | |||
| E03 | 0.598 | 0.033 | 18.312 | |||
| E21 | 0.637 | 0.041 | 15.714 | |||
| E25 | 0.473 | 0.043 | 10.944 | |||
| E18 | 0.594 | 0.040 | 14.842 | |||
| F4 | 0.301 | 0.671 | ||||
| E13 | 0.339 | 0.046 | 7.437 | |||
| E08 | 0.518 | 0.044 | 11.752 | |||
| E20 | 0.736 | 0.035 | 20.894 | |||
| E15 | 0.545 | 0.040 | 13.717 | |||
| E05 | 0.533 | 0.046 | 11.702 |
References
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S.O.R. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [Green Version]
- Mallick, N.; Ray, S.; Mukhopadhyay, S. Eating behaviours and body weight concerns among adolescent girls. Adv. Public Health 2014, 2014, 257396. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, S.G.; Newton, J.R.; Bosanac, P.; Rossell, S.L.; Nesci, J.B.; Castle, D.J. Classification of eating disorders: Comparison of relative prevalence rates using DSM-IV and DSM-5 criteria. Br. J. Psychiatry 2015, 206, 519–520. [Google Scholar] [CrossRef] [Green Version]
- Neumark-Sztainer, D.; Wall, M.; Larson, N.I.; Eisenberg, M.E.; Loth, K. Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. J. Am. Diet. Assoc. 2011, 111, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, M.; Waldherr, K.; Philipp, J.; Nitsch, M.; Dür, W.; Karwautz, A.; Wagner, G. Prevalence of eating disorder risk and associations with health-related quality of life: Results from a large school-based population screening. Eur. Eat. Disord. Rev. 2016, 24, 9–18. [Google Scholar] [CrossRef]
- DeLeel, M.L.; Hughes, T.L.; Miller, J.A.; Hipwell, A.; Theodore, L.A. Prevalence of eating disturbance and body image dissatisfaction in young girls: An examination of the variance across racial and socioeconomic groups. Psychol. Sch. 2009, 46, 767–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, U.; Wick, K.; Hölling, H.; Schlack, R.; Bormann, B.; Brix, C.; Sowa, M.; Schwartze, D.; Strauß, B. Screening of disordered eating in 12 year old girls and boys: Psychometric analysis of the german versions of SCOFF and EAT-26. Eur. Psychiatry 2011, 26, 712. [Google Scholar] [CrossRef]
- Veses, A.M.; Gómez-Martínez, S.; de Heredia, F.P.; Esteban-Cornejo, I.; Castillo, R.; Estecha, S.; García-Fuentes, M.; Veiga, O.; Calle, M.E.; Marcos, A. Cognition and the risk of eating disorders in Spanish adolescents: The AVENA and AFINOS studies. Eur. J. Pediatr. 2015, 174, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Hautala, L.A.; Junnila, J.; Helenius, H.; Väänänen, A.M.; Liuksila, P.R.; Räihä, H.; Välimäki, M.; Saarijärvi, S. Towards understanding gender differences in disordered eating among adolescents. J. Clin. Nurs. 2008, 17, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kim, J.; Yoon, J. Disturbed eating attitudes and behaviors in South Korean boys and girls: A school-based cross-sectional study. Yonsei Med. J. 2010, 51, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Li, Y.; Liu, A.; Hu, X.; Ma, G.; Xu, G. Associations between body mass index, weight control concerns and behaviors, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health 2010, 10, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, X.; Guo, L.; Liu, K. A cross-sectional investigation on eating disorders in 1486 female students from universities, senior high schools and junior high schools in Chengdu. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2008, 29, 321–324. [Google Scholar] [PubMed]
- Watson, H.J.; Hamer, R.M.; Thornton, L.M.; Peat, C.M.; Kleiman, S.C.; Du, S.; Wang, H.; Bulik, C.M. Prevalence of screening-detected eating disorders in Chinese females and exploratory associations with dietary practices. Eur. Eat Disord. Rev. 2015, 23, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Herpertz-Dahlmann, B.; Dempfle, A.; Konrad, K.; Klasen, F.; Ravens-Sieberer, U.; Group, B.S. Eating disorder symptoms do not just disappear: The implications of adolescent eating-disordered behaviour for body weight and mental health in young adulthood. Eur. Child Adolesc. Psychiatry 2015, 24, 675–684. [Google Scholar] [CrossRef]
- Stice, E.; Ng, J.; Shaw, H. Risk factors and prodromal eating pathology. J. Child Psychol. Psychiatry 2010, 51, 518–525. [Google Scholar] [CrossRef]
- Liao, Y.; Liu, T.; Cheng, Y.; Wang, J.; Deng, Y.; Hao, W.; Chen, X.; Xu, Y.; Wang, X.; Tang, J. Changes in eating attitudes, eating disorders and body weight in Chinese medical university students. Int. J. Soc. Psychiatry 2013, 59, 578–585. [Google Scholar] [CrossRef]
- Tao, Z.L. Epidemiological Risk Factor Study Concerning Abnormal Attitudes toward Eating and Adverse Dieting Behaviours among 12-to 25-Years-Old Chinese Students. Eur. Eat Disord. Rev. 2010, 18, 507–514. [Google Scholar] [CrossRef]
- Xian-jun, Y.; Xun, J.; Yu-hai, Z.; Li-jun, S. Development and Evaluation of Preschooler’s Eating Behaviour Scale. Chin. J. Child Health Care 2012, 20, 682–685. [Google Scholar]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef]
- Garner, D.; Olmsted, M.; Bohr, Y.; Garfinkel, P. The Eating Attitudes Test: Psychometric features. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.; Waller, G.; Miller, J.; Slade, P. The development of Eating Attitude Test scores in adolescence. Int. J. Eat. Disord. 1992, 11, 279–282. [Google Scholar] [CrossRef]
- Maloney, M.J.; McGUIRE, J.B.; Daniels, S.R. Reliability testing of a children’s version of the Eating Attitude Test. J. Am. Acad. Child Adolesc. Psychiatry 1988, 27, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Nathan, J.; Allison, D. 3 Psychological and Physical Assessment of Persons with Eating. Neurobiol. Treat. Eat. Disord. 1998, 4, 47. [Google Scholar]
- Smolak, L.; Levine, M.P. Psychometric properties of the children’s eating attitudes test. Int. J. Eat. Disord. 1994, 16, 275–282. [Google Scholar] [CrossRef]
- Teixeira, M.D.C.B.; Pereira, A.T.F.; Saraiva, J.M.T.; Marques, M.; Soares, M.J.; Bos, S.C.; Valente, J.; Azevedo, M.H.P.D.; Macedo, A.J.F.D. Portuguese validation of the children’s eating attitudes test. Arch. Clin. Psychiatry 2012, 39, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Pilecki, M.W.; Kowal, M.; Woronkowicz, A.; Kryst, A.; Sobiecki, J. Psychometric properties of Polish version of the Children’s Eating Attitudes Test. Arch. Psychiatry Psychother. 2013, 15, 35–43. [Google Scholar]
- Chiba, H.; Nagamitsu, S.; Sakurai, R.; Mukai, T.; Shintou, H.; Koyanagi, K.; Yamashita, Y.; Kakuma, T.; Uchimura, N.; Matsuishi, T. Children’s eating attitudes test: Reliability and validation in Japanese adolescents. Eat. Behav. 2016, 23, 120–125. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F. Towards a simplified definition of childhood obesity? A focus on the extended IOTF references. Pediatr. Obes. 2012, 7, 259–260. [Google Scholar] [CrossRef]
- Jorn, H.; Klotz, J. Exact distribution of the K sample Mood and Brown median test. J. Nonparametr. Stat. 2002, 14, 249–257. [Google Scholar] [CrossRef]
- Mood, A.M. On the asymptotic efficiency of certain nonparametric two-sample tests. Ann. Math. Stat. 1954, 25, 514–522. [Google Scholar] [CrossRef]
- Satterthwaite, F.E. An approximate distribution of estimates of variance components. Biom. Bull. 1946, 2, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015; ISBN 146251779X. [Google Scholar]
- Geldhof, G.J.; Preacher, K.J.; Zyphur, M.J. Reliability estimation in a multilevel confirmatory factor analysis framework. Psychol Methods 2014, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Sancho, C.; Asorey, O.; Arija, V.; Canals, J. Psychometric characteristics of the children’s eating attitudes test in a Spanish sample. Eur. Eat. Disord. Rev. Prof. J. Eat. Disord. Assoc. 2005, 13, 338–343. [Google Scholar] [CrossRef]
- Lommi, S.; Viljakainen, H.T.; Weiderpass, E.; de Oliveira Figueiredo, R.A. Children’s Eating Attitudes Test (ChEAT): A validation study in Finnish children. Eat. Weight Disord. -Stud. Anorex. Bulim. Obes. 2019, 25, 961–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pike, K.M.; Dunne, P.E. The rise of eating disorders in Asia: A review. J. Eat. Disord. 2015, 3, 33. [Google Scholar] [CrossRef] [Green Version]
- Sidani, J.E.; Shensa, A.; Hoffman, B.; Hanmer, J.; Primack, B.A. The association between social media use and eating concerns among US young adults. J. Acad. Nutr. Diet 2016, 116, 1465–1472. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, S.; Haddon, L.; Görzig, A.; Ólafsson, K. Risks and Safety on the Internet: The Perspective of European Children: Full Findings and Policy Implications from the EU Kids Online Survey of 9–16 Year Olds and Their Parents in 25 Countries; London School of Economics and Political Science: London, UK, 2011. [Google Scholar]
- Oksanen, A.; Garcia, D.; Räsänen, P. Proanorexia communities on social media. Pediatrics 2016, 137, e20153372. [Google Scholar] [CrossRef] [Green Version]
- Thelen, M.H.; Powell, A.L.; Lawrence, C.; Kuhnert, M.E. Eating and body image concern among children. J. Clin. Child Adolesc. 1992, 21, 41–46. [Google Scholar] [CrossRef]
- Evans, E.H.; Adamson, A.J.; Basterfield, L.; Le Couteur, A.; Reilly, J.K.; Reilly, J.J.; Parkinson, K.N. Risk factors for eating disorder symptoms at 12 years of age: A 6-year longitudinal cohort study. Appetite 2017, 108, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Fairburn, C.G.; Welch, S.L.; Doll, H.A.; Davies, B.A.; O’Connor, M.E. Risk factors for bulimia nervosa: A community-based case-control study. Arch. Gen. Psychiatry 1997, 54, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, K.; Neumark-Sztainer, D.; Story, M.; Resnick, M. Weight control behaviors among obese, overweight, and nonoverweight adolescents. J. Pediatr. Psychol. 2002, 27, 531–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumark-Sztainer, D.; Hannan, P.J. Weight-related behaviors among adolescent girls and boys: Results from a national survey. Arch. Pediatr. Adolesc. Med. 2000, 154, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.R.; Marmorstein, N.; Iacono, W.; Rosenbaum, D.; Espel-Huynh, H.; Muratore, A.F.; Lantz, E.L.; Zhang, F. Body concerns and BMI as predictors of disordered eating and body mass in girls: An 18-year longitudinal investigation. J. Abnorm. Psychol. 2019, 128, 32. [Google Scholar] [CrossRef] [PubMed]
- Tanofsky-Kraff, M.; Yanovski, S.Z.; Wilfley, D.E.; Marmarosh, C.; Morgan, C.M.; Yanovski, J.A. Eating-disordered behaviors, body fat, and psychopathology in overweight and normal-weight children. J. Consult Clin. Psych. 2004, 72, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colton, P.A.; Olmsted, M.P.; Rodin, G.M. Eating disturbances in a school population of preteen girls: Assessment and screening. Int. J. Eat. Disord. 2007, 40, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Micali, N.; De Stavola, B.; Ploubidis, G.; Simonoff, E.; Treasure, J.; Field, A. Adolescent eating disorder behaviours and cognitions: Gender-specific effects of child, maternal and family risk factors. Br. J. Psychiatry 2015, 207, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Rohde, P.; Stice, E.; Marti, C.N. Development and predictive effects of eating disorder risk factors during adolescence: Implications for prevention efforts. Int. J. Eat. Disord. 2015, 48, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Jackson, T.; Chen, H. Predicting changes in eating disorder symptoms among Chinese adolescents: A 9-month prospective study. J. Psychosom. Res. 2008, 64, 87–95. [Google Scholar] [CrossRef]
- Zhang, J.; Yi, Z.; Feng, X.Q.; Li, W.R.; Lyu, Y.B.; Astell-Burt, T.; Zhao, P.Y.; Shi, X.M. Gender differences in the prevalence of overweight and obesity, associated behaviors, and weight-related perceptions in a national survey of primary school children in China. Biomed Env. Sci 2018, 31, 1–11. [Google Scholar]
- Song, Y.; Wang, H.; Ma, J.; Wang, Z. Secular trends of obesity prevalence in urban Chinese children from 1985 to 2010: Gender disparity. PLoS ONE 2013, 8, e53069. [Google Scholar] [CrossRef] [PubMed]
- Rojo Moreno, L.; García Miralles, I.; Plumed, J.; Barberá, M.; Morales, M.M.; Ruiz, E.; Livianos, L. Children’s eating attitudes test: Validation in a sample of Spanish schoolchildren. Int. J. Eat. Disord. 2011, 44, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007. [Google Scholar]


| Variable | Total, n (%) | Normal, n (%) | Abnormal, n (%) | χ2 ** |
|---|---|---|---|---|
| Gender | ||||
| Boys | 484 (53.42) | 432 (47.68) | 52 (5.74) | 0.002 |
| Girls | 422 (46.58) | 377 (41.61) | 45 (4.97) | |
| Grade | ||||
| Three | 323 (35.65) | 287 (31.68) | 36 (3.97) | 2.80 |
| Four | 276 (30.46) | 241 (26.60) | 35 (3.86) | |
| Five | 307 (33.89) | 281 (31.02) | 26 (2.87) | |
| School | ||||
| A | 366 (40.40) | 320 (35.32) | 46 (5.08) | 2.36 |
| B | 325 (35.87) | 293 (32.34) | 32 (3.53) | |
| C | 215 (23.73) | 196 (21.63) | 19 (2.10) | |
| Age (NA * = 78, 8.61%) | ||||
| 8–9 | 134 (16.18) | 118 (14.25) | 16 (1.93) | 2.66 |
| 10 | 277 (33.45) | 247 (29.83) | 30 (3.62) | |
| 11 | 245 (29.59) | 216 (26.09) | 29 (3.50) | |
| 12 | 150 (18.12) | 138 (16.67) | 12 (1.45) | |
| 13 | 17 (2.29) | 17 (2.05) | 2 (0.24) | |
| 14–16 | 3 (0.36) | 3 (0.36) | 0 (0) | |
| Annual household income (USD; NA = 128, 14.13%) | ||||
| <3000 | 57 (7.33) | 49 (6.30) | 8 (1.03) | 4.32 |
| 3000–6000 | 98 (12.60) | 82 (10.54) | 16 (2.06) | |
| 6000–9000 | 151 (19.41) | 135 (17.35) | 16 (2.06) | |
| 9000–12,000 | 111 (14.27) | 100 (12.85) | 11 (1.41) | |
| 12,000–15,000 | 142 (18.25) | 127 (16.32) | 15 (1.93) | |
| ≥15,000 | 219 (28.15) | 199 (25.58) | 20 (2.57) | |
| Mother’s education (NA = 93, 10.26%) | ||||
| Illiteracy/Primary school | 96 (11.81) | 86 (10.58) | 10 (1.23) | 0.70 |
| Middle school | 298 (36.65) | 265 (32.60) | 33 (4.06) | |
| High school | 200 (24.60) | 179 (22.02) | 21 (2.58) | |
| University | 214 (26.32) | 192 (23.62) | 22 (2.71) | |
| Post college | 5 (0.62) | 5 (0.62) | 0 (0) | |
| Father’s education (NA = 89, 9.82%) | ||||
| Illiteracy/Primary school | 31 (3.79) | 27 (3.30) | 4 (0.49) | 2.48 |
| Middle school | 312 (38.19) | 278 (34.03) | 34 (416) | |
| High school | 222 (27.17) | 199 (24.36) | 23 (2.82) | |
| University | 233 (28.52) | 208 (25.46) | 25 (3.06) | |
| Post college | 19 (2.33) | 19 (2.33) | 0 (0) | |
| Siblings (NA = 73, 8.06%) | ||||
| Single child | 477 (57.26) | 426 (54.76) | 51 (6.56) | 1.76 |
| Non-single child | 356 (42.74) | 317 (40.75) | 39 (5.01) | |
| Total | 906 (100) | 809 (89.30) | 97 (10.71) | |
| No. | Items | Factor 1 Fear of Getting Fat | Factor 2 Dieting and Purging Behaviors | Factor 3 Bulimia and Food Occupation | Factor 4 Social Pressure to Eat |
|---|---|---|---|---|---|
| 11 | I think a lot about wanting to be thinner | 0.798 | |||
| 01 | I am scared about being overweight | 0.728 | |||
| 14 | I think a lot about having fat on my body | 0.669 | |||
| 12 | I think about burning up energy (calories) when I exercise | 0.617 | |||
| 17 | I eat diet foods | 0.496 | |||
| 16 | I stay away from foods with sugar in them | 0.364 | |||
| 06 | I am aware of the energy (calorie) content in foods that I eat | 0.317 | |||
| 26 | I have the urge to vomit after eating | 0.740 | |||
| 09 | I vomit after I have eaten | 0.734 | |||
| 10 | I feel very guilty after eating | 0.577 | |||
| 02 | I stay away from eating when I am hungry | 0.545 | |||
| 24 | I like my stomach to be empty | 0.513 | |||
| 07 | I try to stay away from foods such as breads, potatoes, and rice | 0.461 | |||
| 23 | I have been dieting | 0.430 | |||
| 22 | I feel uncomfortable after eating sweets | 0.418 | |||
| 19 | I can show self-control around food | 0.355 | |||
| 04 | I have gone on eating binges where I feel that I might not be able to stop | 0.709 | |||
| 03 | I think about food a lot of the time | 0.658 | |||
| 21 | I give too much time and thought to food | 0.596 | |||
| 25 | I enjoy trying new rich foods | 0.588 | |||
| 18 | I think that food controls my life | 0.585 | |||
| 13 | Other people think I am too thin | 0.699 | |||
| 8 | I feel that others would like me to eat more | 0.671 | |||
| 20 | I feel that others pressure me to eat | 0.576 | |||
| 15 | I take longer than others to eat my meals | 0.402 | |||
| 5 | I cut my food into small pieces | 0.367 |
| Dimension | Item Number | Cronbach’s α | Split-Half Reliability |
|---|---|---|---|
| F1 Fear of getting fat | 7 | 0.728 | 0.502 |
| F2 Dieting and purging behaviors | 9 | 0.699 | 0.700 |
| F3 Bulimia and food occupation | 5 | 0.645 | 0.617 |
| F4 Social pressure to eat | 5 | 0.536 | 0.442 |
| Total | 26 | 0.819 | 0.816 |
| Gender | Median | IQR | χ2 | Mean ± SD | t |
|---|---|---|---|---|---|
| Total | |||||
| Boys | 6 | 2–12 | 1.820 | 8.79 ± 9.08 | −1.511 |
| Girls | 8 | 3–14 | 9.70 ± 9.13 | ||
| Total | 7 | 3–13 | 9.21 ± 9.11 | ||
| Factor 1, fear of getting fat | |||||
| Boys | 2 | 0–6 | 10.630 ** | 3.78 ± 4.42 | −2.923 ** |
| Girls | 3 | 0–7 | 4.67 ± 4.68 | ||
| Total | 3 | 0–7 | 4.20 ± 4.56 | ||
| Factor 2, dieting and purging behaviors | |||||
| Boys | 0 | 0–2 | 0.499 | 1.49 ± 2.88 | 0.502 |
| Girls | 0 | 0–2 | 1.39 ± 2.87 | ||
| Total | 0 | 0–2 | 1.44 ± 2.87 | ||
| Factor3, bulimia and food occupation | |||||
| Boys | 0 | 0–2 | 6.133 * | 1.35 ± 2.39 | 1.495 |
| Girls | 0 | 0–1 | 1.12 ± 2.23 | ||
| Total | 0 | 0–2 | 1.24 ± 2.32 | ||
| Factor 4, social pressure to eat | |||||
| Boys | 1 | 0–3 | 3.850 * | 2.17 ± 2.78 | −1.884 |
| Girls | 2 | 0–4 | 2.53 ± 2.95 | ||
| Total | 1 | 0–4 | 2.33 ± 2.86 | ||
| Factor | Total Sample | Girls | Boys | |||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Factor 1 Fear of getting fat | 0.268 | <0.001 | 0.355 | <0.001 | 0.309 | <0.001 |
| Factor 2 Dieting and purging behaviors | 0.140 | <0.001 | 0.160 | 0.002 | −0.105 | 0.043 |
| Factor 3 Bulimia and Food preoccupation | 0.052 | 0.136 | 0.065 | 0.198 | 0.064 | 0.224 |
| Factor 4 Social pressure to eat | −0.202 | <0.001 | −0.161 | 0.001 | −0.233 | <0.001 |
| Total score | 0.114 | 0.002 | 0.184 | 0.001 | 0.092 | 0.079 |
| Factor | BMI Categories | Kruskal–Wallis | ||||||
|---|---|---|---|---|---|---|---|---|
| ChEAT | Thinness Grade 3 (Mean ± SD) | Thinness Grade 2 (Mean ± SD) | Thinness Grade 1 (Mean ± SD) | Fit (Mean ± SD) | Overweight (Mean ± SD) | Obesity (Mean ± SD) | χ2 | p |
| Factor 1 Fear of getting fat | * T: 1.83 ± 2.83 ** G: 1.69 ± 3.04 *** B: 2.20 ± 2.49 | T: 2.26 ± 3.44 G: 2.33 ± 3.99 B: 2.08 ± 1.66 | T: 2.59 ± 3.01 G: 2.49 ± 2.60 B: 2.74 ± 3.58 | T: 4.07 ± 4.56 G: 5.03 ± 4.82 B: 3.17 ± 4.12 | T: 5.65 ± 5.01 G: 6.81 ± 4.77 B: 4.86 ± 5.05 | T: 5.68 ± 5.18 G: 5.76 ± 5.08 B: 5.63 ± 5.28 | T: 45.412 G: 42.595 B: 20.511 | T: <0.0001 G: <0.0001 B: 0.001 |
| Factor 2 Dieting and purging behaviors | T: 0.63 ± 0.83 G: 0.43 ± 0.76 B: 1.20 ± 0.84 | T: 0.67 ± 1.22 G: 0.54 ± 1.14 B: 0.93 ± 1.38 | T: 1.08 ± 2.24 G: 0.67 ± 1.14 B: 1.71 ± 3.18 | T: 1.28 ± 2.70 G: 1.26 ± 2.14 B: 1.29 ± 3.15 | T: 1.73 ± 2.84 G: 1.89 ± 3.08 B: 1.62 ± 2.68 | T: 2.15 ± 3.64 G: 2.29 ± 4.88 B: 2.08 ± 2.80 | T: 16.085 G: 12.375 B: 11.672 | T: 0.007 G: 0.030 B: 0.040 |
| Factor 3 Bulimia and food occupation | T: 1.12 ± 2.37 G: 0.58 ± 1.73 B: 2.40 ± 3.36 | T: 1.00 ± 1.49 G: 1.09 ± 1.60 B: 0.79 ± 1.25 | T: 0.81 ± 1.64 G: 0.55 ± 1.24 B: 1.21 ± 2.06 | T: 1.26 ± 2.53 G: 1.28 ± 2.62 B: 1.25 ± 2.45 | T: 1.17 ± 2.02 G: 1.35 ± 2.16 B: 1.06 ± 1.92 | T: 1.45 ± 2.33 G: 0.88 ± 1.64 B: 1.73 ± 2.56 | T: 4.421 G: 6.770 B: 5.222 | T: 0.491 G: 0.238 B: 0.389 |
| Factor 4 Social pressure to eat | T: 3.26 ± 3.31 G: 2.86 ± 3.08 B: 4.40 ± 4.04 | T: 3.56 ± 2.86 G: 3.26 ± 3.00 B: 4.33 ± 2.39 | T: 2.90 ± 2.90 G: 3.10 ± 2.96 B: 2.63 ± 2.83 | T: 2.36 ± 2.90 G: 2.42 ± 2.82 B: 2.31 ± 2.98 | T: 1.88 ± 2.73 G: 2.25 ± 3.00 B: 1.63 ± 2.52 | T: 1.83 ± 2.55 G: 2.29 ± 2.88 B: 1.58 ± 2.34 | T: 28.778 G: 7.595 B: 22.319 | T: <0.0001 G: 0.180 B: 0.001 |
| Total score of ChEAT | T: 6.41 ± 6.23 G: 4.83 ± 5.94 B: 10.20 ± 5.72 | T: 8.05 ± 6.62 G: 7.63 ± 7.54 B: 9.09 ± 3.59 | T: 6.64 ± 6.24 G: 6.65 ± 4.16 B: 6.62 ± 8.78 | T: 8.90 ± 9.74 G: 10.06 ± 9.37 B: 7.83 ± 9.98 | T: 9.67 ± 8.87 G: 11.93 ± 9.40 B: 7.93 ± 8.08 | T: 10.05 ± 8.68 G: 10.14± 9.35 B: 10.00± 8.39 | T: 8.385 G: 13.357 B: 10.436 | T: 0.136 G: 0.020 B: 0.064 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Wang, C.; Tong, L. The Reliability and Validation of the Children’s Eating Attitude Test among Chinese Samples. Int. J. Environ. Res. Public Health 2023, 20, 738. https://doi.org/10.3390/ijerph20010738
Huang Y, Wang C, Tong L. The Reliability and Validation of the Children’s Eating Attitude Test among Chinese Samples. International Journal of Environmental Research and Public Health. 2023; 20(1):738. https://doi.org/10.3390/ijerph20010738
Chicago/Turabian StyleHuang, Ying, Chang Wang, and Lian Tong. 2023. "The Reliability and Validation of the Children’s Eating Attitude Test among Chinese Samples" International Journal of Environmental Research and Public Health 20, no. 1: 738. https://doi.org/10.3390/ijerph20010738