

Exploring Hospital Inpatients’ Awareness of Their Falls Risk: A Qualitative Exploratory Study

Abstract
:1. Introduction
Aim
2. Design and Methods
2.1. Ethical Considerations
2.2. Recruitment
2.3. Data Collection
2.4. Position of the Researcher
2.5. Data Analysis
3. Findings
3.1. Description of Participants
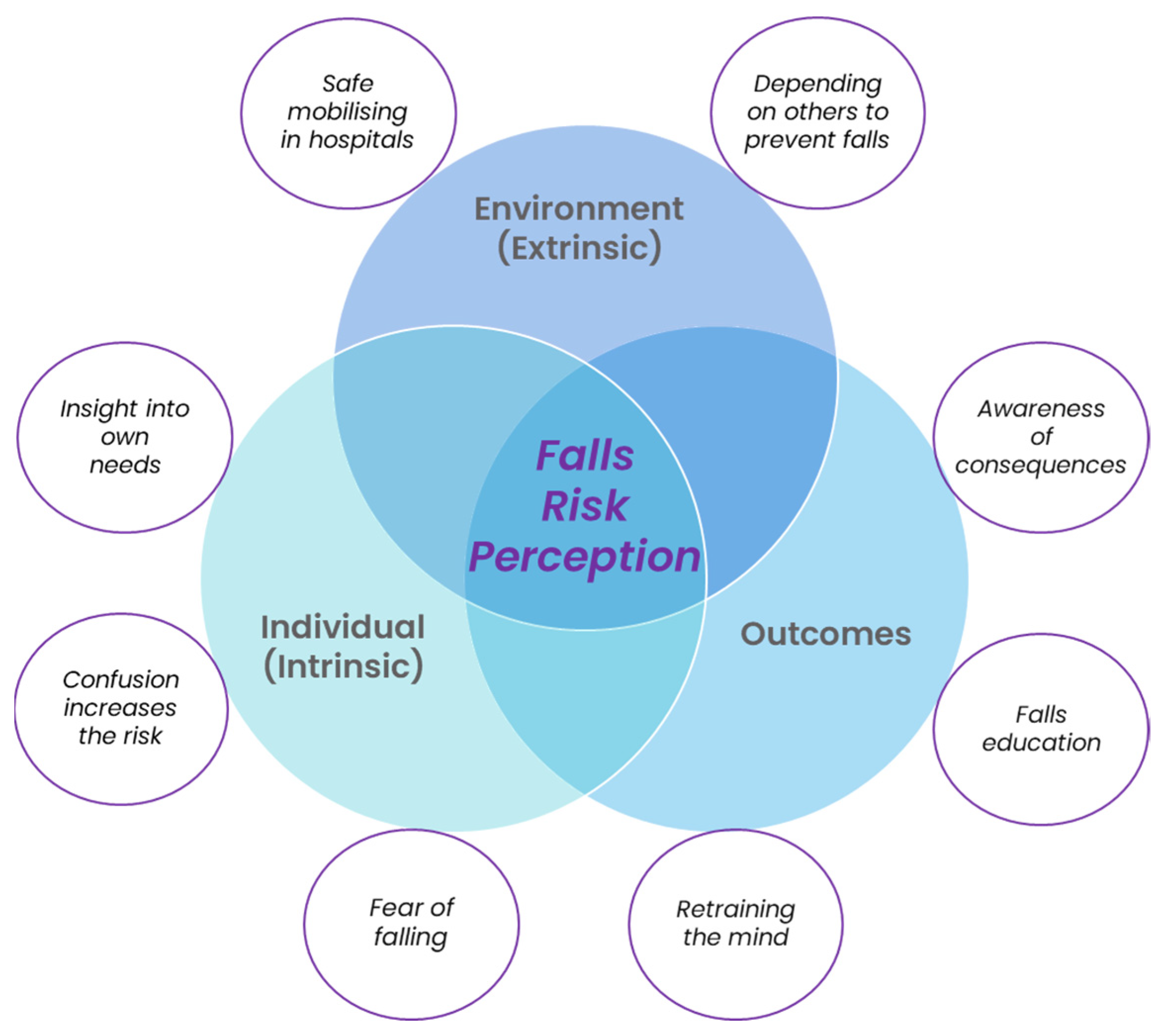
3.2. Description of Themes
3.3. Theme One: Environment (Extrinsic)
3.3.1. Safe Mobilising in Hospitals
“They’ve got to keep everything in its place. So that makes me feel safe”[P15]
3.3.2. Depending on Others to Prevent Falls
“If I ask for assistance it comes, so I don’t have to take any risks”[P1]
“There are times when I’m ringing for a bell. I’m ringing the red lights and no one comes and I want to use the bottle. They don’t come and I’m getting desperate”[P7]
“I don’t expect them to drop everything for me. I just find I need help going to the toilet. I know they’re busy. When you want to get back to bed, I buzz and then I say to myself, ‘You’re being selfish’”[P6]
“There needs to be some kind of collar, like an electronic tracking bracelet that they would put on the patients and nurses at the front desk who’ll be monitoring those bracelets to see where the patients are, once they bypass the sensor from their door from the room”[P5]
“I think the patients have gotta take responsibility to some extent. You can’t just come in and be pandered over … patients gotta take responsibility for what they can do and what they can’t do. They can ask for assistance. That’s why we’ve got the bell”[P8]
3.4. Theme Two: Individual (Intrinsic)
3.4.1. Insight into Own Needs
“‘cause there’s help always and I won’t do anything unless I’ve got help with me. I won’t try and do anything that I know I’m not gonna be able to do”[P16]
“Am I at risk of falling? Not as long as I do what I’m told”[P7]
“I do it myself, I just … there’s no other, no other way to do it. I’m gonna have to do it at home”[P18]
“I’m noticing a lot with old people they’ll get up out of their bed. They might be gasping for oxygen and they’ll stand up too quickly out of bed. They’ll try and catch themselves and then they’ll start wandering or calling out and they’ll lose blood pressure very quickly and they’ll fall over. I’ve seen this happen a couple of times”[P5]
“Not concentrating, I believe. Or getting their ambitions and their capabilities mixed up. Just thinking they’re better than they really are at the time”[P14]
3.4.2. Confusion Increases the Risk
“I’ve seen elderly patients get out of bed and wear bed pans as their shoes ‘cause they thought they were their shoes. I’ve seen dementia people walk around and just fall over”[P5]
“If I’m not look well, not watched and guarded, probably yeah I could (fall)”[P11]
“It was a small case of fright, I didn’t know where the heck I was! I didn’t know anything”[P15]
3.4.3. Fear of Falling
“I’ve just had a massive fall at home less than a week ago and I’m just absolutely terrified of falling again. This is where I make sure I’ve got one or two people with me when I get up and go to the toilet and back”[P9]
“I have never had a fall, that’s why I’m so paranoid I think. I just don’t want to it’s the last thing I want to do”[P12]
3.5. Theme Three: Outcomes
3.5.1. Awareness of Consequences
“They break their hip, get pneumonia and then they’re on their way out. They just don’t get better and better and it’s all part of the grand scheme of death basically”[P5]
“After having my falls, it makes you concentrate more. ‘Cause it’s scary being on the floor, flopping around like a dying fish. So that’s what keeps you a lot more focused if you have had a fall”[P16]
3.5.2. Falls Education
“I figured that they know what they’re doing, so if you want to get better, you listen and do”[P3]
“No. Be nice if they did” [P11], with another commenting, “Not that I know of or remember. They may have, but I don’t remember”[P15]
“I always say to everybody to ring my wife first to keep her in the loop ‘cause when you get old like us they seem to think that your brain is gone and you can’t think for yourself”[P7]
“If I survive this ordeal and come out of hospital, I’ll have to do something about it because it seems like simple little falls are gonna be a tragedy to me”[P7]
3.5.3. Retraining the Mind
“Sometimes I forget and I’ll start to head off and then the alarm goes and I realise I’m not supposed to stand up. I’ve spent 70 years doing [things] how I want to and I’ve been here a month it takes a long time to get over old habits. You know but I’m gonna have to learn because I can’t afford to have too many more falls”[P2]
“Your mind is not [the] same as your body. Your mind is still strong, you know? But your body, it doesn’t give the same amount, so you have to work it out. What you can do and what you can’t do. You have to teach yourself, train yourself again to be really strong”[P10]
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Schedule for Patients
- Do you think that you at risk of falling here in hospital?
- Why/why not?
- What do you think are the reasons why someone could fall in hospital?
- In hospital, where do you think people are most likely to fall?
- Has someone spoken to you about falling in hospital and what you can do to stop it?
- What is your understanding of what can happen if you have a fall?
- Can you please describe any information or plans that you have been given about stopping falls?
- Did you find this information helpful?
- Were you involved in developing any plans or strategies to try to keep you from falling in hospital?
- Have there been times here in hospital when you haven’t followed these plans? If so, why is that?
- Before this hospital stay, had anyone ever spoken to you about falling? (after answer: if yes) Could you please describe that conversation? What are your thoughts about what was said?
- We’re up to the last question now. Do you think that you are at risk of falling here in hospital?
References
- LeLaurin, J.H.; Shorr, R.I. Preventing falls in hospitalized patients: State of the science. Clin. Geriatr. Med. 2019, 35, 273–283. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Falls in Older People: Assessing Risk and Prevention. Available online: https://www.nice.org.uk/guidance/cg161/chapter/Introduction (accessed on 14 October 2022).
- Australian Commission on Safety and Quality in Health Care. Falls Resulting in Fracture or Intracranial Injury. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Falls-resulting-in-fracture-of-intracranial-injury-detailed-fact-sheet.pdf (accessed on 13 October 2022).
- Morello, R.T.; Barker, A.L.; Watts, J.J.; Haines, T.; Zavarsek, S.S.; Hill, K.D.; Brand, C.; Sherrington, C.; Wolfe, R.; Bohensky, M.A.; et al. The extra resource burden of in-hospital falls: A cost of falls study. Med. J. Aust. 2015, 203, 367. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.; O’Riordan, S. Prevention of falls in hospital. Clin. Med. (Lond.) 2017, 17, 360–362. [Google Scholar] [CrossRef] [Green Version]
- Cameron, I.D.; Dyer, S.M.; Panagoda, C.E.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst. Rev. 2018, 9, CD005465. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Health Care Quality and Safety. Available online: https://www.aihw.gov.au/reports/health-care-quality-performance/health-care-safety-and-quality (accessed on 16 December 2022).
- Australian Institute of Health and Welfare. Admitted Patient Care 2020-21 8 Safety and Quality of the Health Systems. Available online: https://www.aihw.gov.au/reports-data/myhospitals/sectors/admitted-patients#more-data (accessed on 17 October 2022).
- Australian and New Zealand Falls Prevention Society. The Problem and Prevalence of Falls; Australian and New Zealand Falls Prevention Society: Perth, Australia, 2021. [Google Scholar]
- World Health Organisation. Step Safely: Strategies for Preventing and Managing Falls across the Life-Course; World Health Organisation: Geneva, Switzerland, 2021. [Google Scholar]
- Deandrea, S.; Bravi, F.; Turati, F.; Lucenteforte, E.; La Vecchia, C.; Negri, E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2013, 56, 407–415. [Google Scholar] [CrossRef]
- Heng, H.; Slade, S.C.; Jazayeri, D.; Jones, C.; Hill, A.-M.; Kiegaldie, D.; Shorr, R.I.; Morris, M.E. Patient perspectives on hospital falls prevention education. Front. Public Health 2021, 9, 592440. [Google Scholar] [CrossRef]
- Oliver, D.; Daly, F.; Martin, F.C.; McMurdo, M.E.T. Risk factors and risk assessment tools for falls in hospital in-patients: A systematic review. Age Ageing 2004, 33, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Dabkowski, E.; Cooper, S.; Duncan, J.R.; Missen, K. Adult inpatients’ perceptions of their fall risk: A scoping review. Healthcare 2022, 10, 995. [Google Scholar] [CrossRef]
- Dolan, H.; Slebodnik, M.; Taylor-Piliae, R. Older adults’ perceptions of their fall risk in the hospital: An integrative review. J. Clin. Nurs. 2021, 1, 2418–2436. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; van der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. World guidelines for falls prevention and management for older adults: A global initiative. Age Ageing 2022, 51, 6730755. [Google Scholar] [CrossRef]
- Cerilo, P.C.; Siegmund, L.A. Pilot testing of nurse led multimodal intervention for falls prevention. Geriatr. Nurs. 2022, 43, 242–248. [Google Scholar] [CrossRef]
- Sonnad, S.S.; Mascioli, S.; Cunningham, J.; Goldsack, J. Do patients accurately perceive their fall risk? Nursing2021 2014, 44, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Shuman, C.; Liu, J.; Montie, M.; Galinato, J.G.; Todd, M.A.; Hegstad, M.; Titler, M. Patient perceptions and experiences with falls during hospitalization and after discharge. Appl. Nurs. Res. 2016, 31, 79–85. [Google Scholar] [CrossRef]
- Lim, M.L.; Seow, J.P.; Ang, S.Y.; Lopez, V. Disparity between perceived and physiological risks of falling among older patients in an acute care hospital. Appl. Nurs. Res. 2018, 42, 77–82. [Google Scholar] [CrossRef]
- Johnson, M.; George, A.; Tran, D.T. Analysis of falls incidents: Nurse and patient preventive behaviours. Int. J. Nurs. Pract. 2011, 17, 60–66. [Google Scholar] [CrossRef]
- Hill, A.-M.; Francis-Coad, J.; Haines, T.P.; Waldron, N.; Etherton-Beer, C.; Flicker, L.; Ingram, K.; McPhail, S.M. ‘My independent streak may get in the way’: How older adults respond to falls prevention education in hospital. BMJ Open 2016, 6, e012363. [Google Scholar] [CrossRef] [Green Version]
- Gettens, S.; Fulbrook, P.; Jessup, M.; Choy, N.L. The patients’ perspective of sustaining a fall in hospital: A qualitative study. J. Clin. Nurs. 2018, 27, 743–752. [Google Scholar] [CrossRef]
- Haines, T.; Lee, D.-C.A.; O’Connell, B.; McDermott, F.; Hoffmann, T. Why do hospitalized older adults take risks that may lead to falls? Health Expect 2012, 18, 233–249. [Google Scholar] [CrossRef] [Green Version]
- Francis-Coad, J.; Hill, A.-M.; Jacques, A.; Chandler, A.M.; Richey, P.A.; Mion, L.C.; Shorr, R.I. Association between characteristics of injurious falls and fall preventive interventions in acute medical and surgical units. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, e152. [Google Scholar] [CrossRef]
- Hignett, S.; Sands, G.; Griffiths, P. In-patient falls: What can we learn from incident reports? Age Ageing 2013, 42, 527–531. [Google Scholar] [CrossRef]
- Oliver, D.; Healey, F.; Haines, T.P. Preventing falls and fall-related injuries in hospitals. Clin. Geriatr. Med. 2010, 26, 645–692. [Google Scholar] [CrossRef] [PubMed]
- Mihaljcic, T.; Haines, T.P.; Ponsford, J.L.; Stolwyk, R.J. Investigating the relationship between reduced self-awareness of falls risk, rehabilitation engagement and falls in older adults. Arch. Gerontol. Geriatr. 2017, 69, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; SAGE Publications Inc.: Great Britain, UK, 2018. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Molloy, D.W.; Standish, T.I. A guide to the standardized mini-mental state examination. Int. Psychogeriatr. 1997, 9 (Suppl. S1), 87–94; discussion 143–150. [Google Scholar] [CrossRef]
- Taylor, J.S.; DeMers, S.M.; Vig, E.K.; Borson, S. The disappearing subject: Exclusion of people with cognitive impairment and dementia from geriatrics research. J. Am. Geriatr. Soc. 2012, 60, 413–419. [Google Scholar] [CrossRef]
- Turner, D.W. Qualitative interview design: A practical guide for novice investigators. Qual. Rep. 2010, 15, 754–760. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2015, 26, 1753–1760. [Google Scholar] [CrossRef]
- Finlay, L.; Gough, B. (Eds.) Reflexivity: A Practical Guide for Researchers in Health and Social Sciences; Blackwell Science: Oxford, UK, 2003. [Google Scholar]
- Braun, V.; Clark, V. Thematic Analysis: A Practical Guide; Sage Publications Ltd.: London, UK, 2022. [Google Scholar]
- Braun, V.; Clarke, V. Conceptual and design thinking for thematic analysis. Qual. Psychol. 2021, 9, 3–26. [Google Scholar] [CrossRef]
- Twibell, R.K.; Siela, D.; Delaney, L.; Avila, P.; Spradlin, A.M.; Coers, G. Perspectives of inpatients with cancer on engagement in fall prevention. Oncol. Nurs. Forum 2020, 47, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.L.; Ang, S.G.M.; Teo, K.Y.; Wee, Y.H.C.; Yee, S.P.; Lim, S.H.; Ang, S.Y. Patients’ experience after a fall and their perceptions of fall prevention: A qualitative study. J. Nurs. Care Qual. 2018, 33, 46–52. [Google Scholar] [CrossRef]
- Dolan, H.; Rishel, C.; Rainbow, J.G.; Taylor-Piliae, R. Relying on myself: The lived experience of being at risk for falling in the hospital among older adults. Geriatr. Nurs. 2022, 47, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Haines, T.P. Pride comes before denial of a fall? BMJ 2018, 360, k438. [Google Scholar] [CrossRef]
- Kiyoshi-Teo, H.; Northrup-Snyder, K.; Robert Davis, M.; Garcia, E.; Leatherwood, A.; Izumi, S. Qualitative descriptions of patient perceptions about fall risks, prevention strategies and self-identity: Analysis of fall prevention motivational interviewing conversations. J. Clin. Nurs. 2020, 29, 4281–4288. [Google Scholar] [CrossRef] [PubMed]
- Jellett, J.; Williams, C.; Clayton, D.; Plummer, V.; Haines, T. Falls risk score removal does not impact inpatient falls: A stepped-wedge, cluster-randomised trial. J. Clin. Nurs. 2020, 29, 4505–4513. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Haines, T.; Hill, A.M.; Cameron, I.D.; Jones, C.; Jazayeri, D.; Mitra, B.; Kiegaldie, D.; Shorr, R.I.; McPhail, S.M. Divesting from a scored hospital fall risk assessment tool (FRAT): A cluster randomized non-inferiority trial. J. Am. Geriatr. Soc. 2021, 69, 2598–2604. [Google Scholar] [CrossRef]
- Murphy, J.; Isaacs, B. The post-fall syndrome. A study of 36 elderly patients. Gerontology 1982, 28, 265–270. [Google Scholar] [CrossRef]
- Harding, S.; Gardner, A. Fear of falling. Aust. J. Adv. Nurs. 2009, 27, 94–100. [Google Scholar]
- Zhang, H.; Si, W.; Pi, H. Incidence and risk factors related to fear of falling during the first mobilisation after total knee arthroplasty among older patients with knee osteoarthritis: A cross-sectional study. J. Clin. Nurs. 2021, 30, 2665–2672. [Google Scholar] [CrossRef]
- Çinarli, T.; Koç, Z. Fear and risk of falling, activities of daily living, and quality of life: Assessment when older adults receive emergency department care. Nurs. Res. 2017, 66, 330–335. [Google Scholar] [CrossRef]
- Turner, N.; Jones, D.; Dawson, P.; Tait, B. The perceptions and rehabilitation experience of older people after falling in the hospital. Rehabil. Nurs. 2019, 44, 141–150. [Google Scholar] [CrossRef]
- Morris, M.E.; Webster, K.; Jones, C.; Hill, A.-M.; Haines, T.; McPhail, S.; Kiegaldie, D.; Slade, S.; Jazayeri, D.; Heng, H.; et al. Interventions to reduce falls in hospitals: A systematic review and meta-analysis. Age Ageing 2022, 51, afac077. [Google Scholar] [CrossRef] [PubMed]
- Mion, L.C. When the falls expert becomes the fall risk patient: Through the looking-glass. Geriatr. Nurs. 2016, 37, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care. Partnering with Consumers Standard. Available online: https://www.safetyandquality.gov.au/standards/nsqhs-standards/partnering-consumers-standard (accessed on 16 September 2021).
- Härlein, J.; Dassen, T.; Halfens, R.J.; Heinze, C. Fall risk factors in older people with dementia or cognitive impairment: A systematic review. J. Adv. Nurs. 2009, 65, 922–933. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Speechley, M. Falls in cognitively impaired older adults: Implications for risk assessment and prevention. J. Am. Geriatr. Soc. 2018, 66, 367–375. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Admission Diagnosis for Each Participant | |||
|---|---|---|---|
| P1 | Subdural haemorrhage | P10 | Orthopaedic complications post knee surgery |
| P2 | Exacerbation of Parkinson’s Disease | P11 | Cardiac complaint |
| P3 | Fractured pelvis and shoulder | P12 | Uncontrolled peristomal leakage |
| P4 | Fractured hip | P13 | Unstable angina |
| P5 | End of life care: cystic fibrosis | P14 | Toe amputation |
| P6 | Neuropathy causing multiple falls | P15 | Fractured tibia and fibula |
| P7 | Syncope and falls | P16 | Fractured hip (Past history: Stroke) |
| P8 | End stage liver cirrhosis | P17 | Gait training post transtibial amputation |
| P9 | Fall at home | P18 | Fractured ankle |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabkowski, E.; Cooper, S.J.; Duncan, J.R.; Missen, K. Exploring Hospital Inpatients’ Awareness of Their Falls Risk: A Qualitative Exploratory Study. Int. J. Environ. Res. Public Health 2023, 20, 454. https://doi.org/10.3390/ijerph20010454
Dabkowski E, Cooper SJ, Duncan JR, Missen K. Exploring Hospital Inpatients’ Awareness of Their Falls Risk: A Qualitative Exploratory Study. International Journal of Environmental Research and Public Health. 2023; 20(1):454. https://doi.org/10.3390/ijerph20010454
Chicago/Turabian StyleDabkowski, Elissa, Simon J. Cooper, Jhodie R. Duncan, and Karen Missen. 2023. "Exploring Hospital Inpatients’ Awareness of Their Falls Risk: A Qualitative Exploratory Study" International Journal of Environmental Research and Public Health 20, no. 1: 454. https://doi.org/10.3390/ijerph20010454