
Ten-Year Probabilities of Death Due to Cancer and Cardiovascular Disease among Breast Cancer Patients Diagnosed in North-Eastern Spain

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Methods
2.2.1. Risk of Death Due to Causes Other Than BC Compared to the General Population
2.2.2. 10-Year Cause-Specific Probabilities of Death in the Cohort: Competing Risks Analysis
3. Results
3.1. Descriptive Analysis
3.2. 10-Year Cause-Specific Probabilities of Death in the Cohort
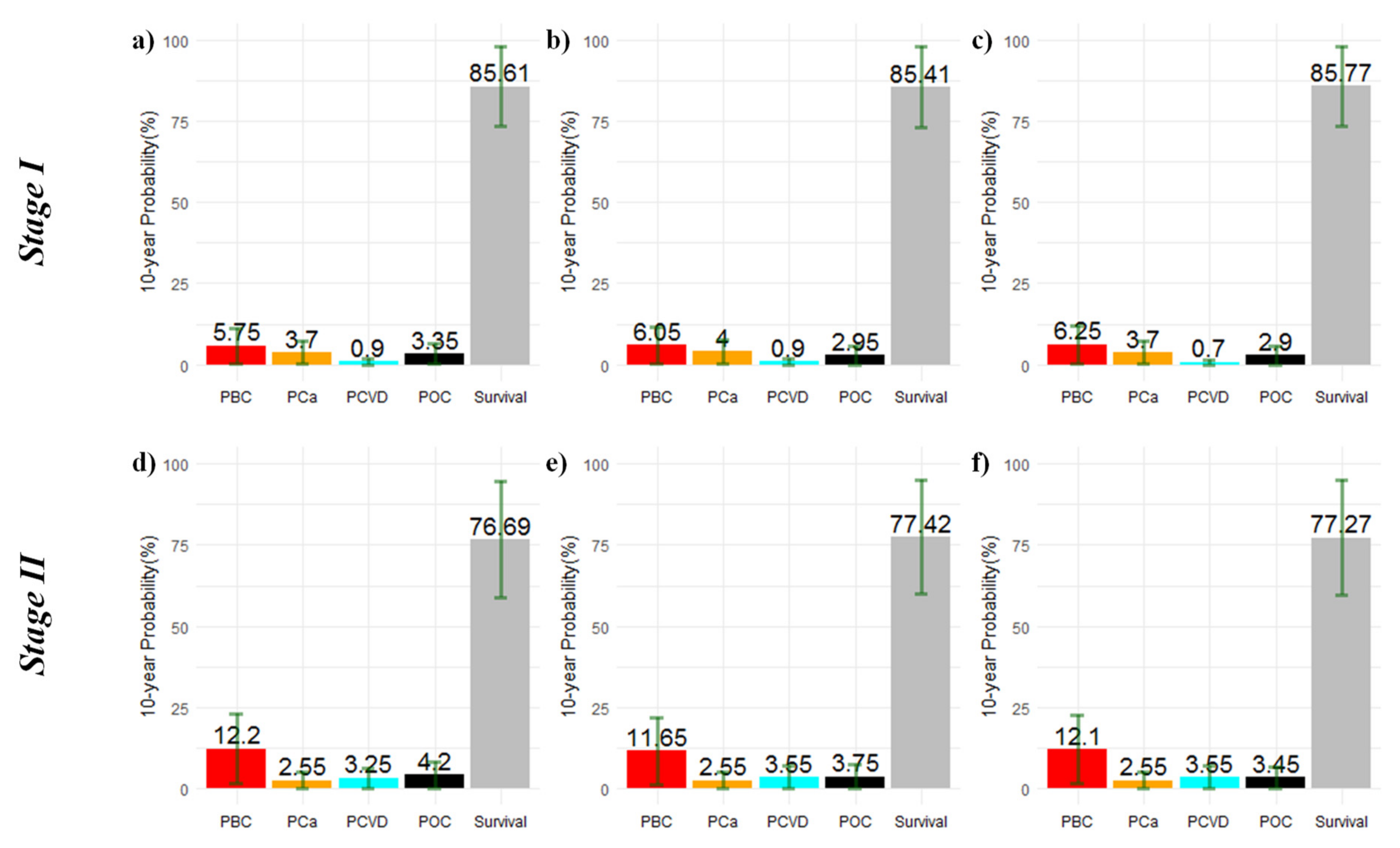
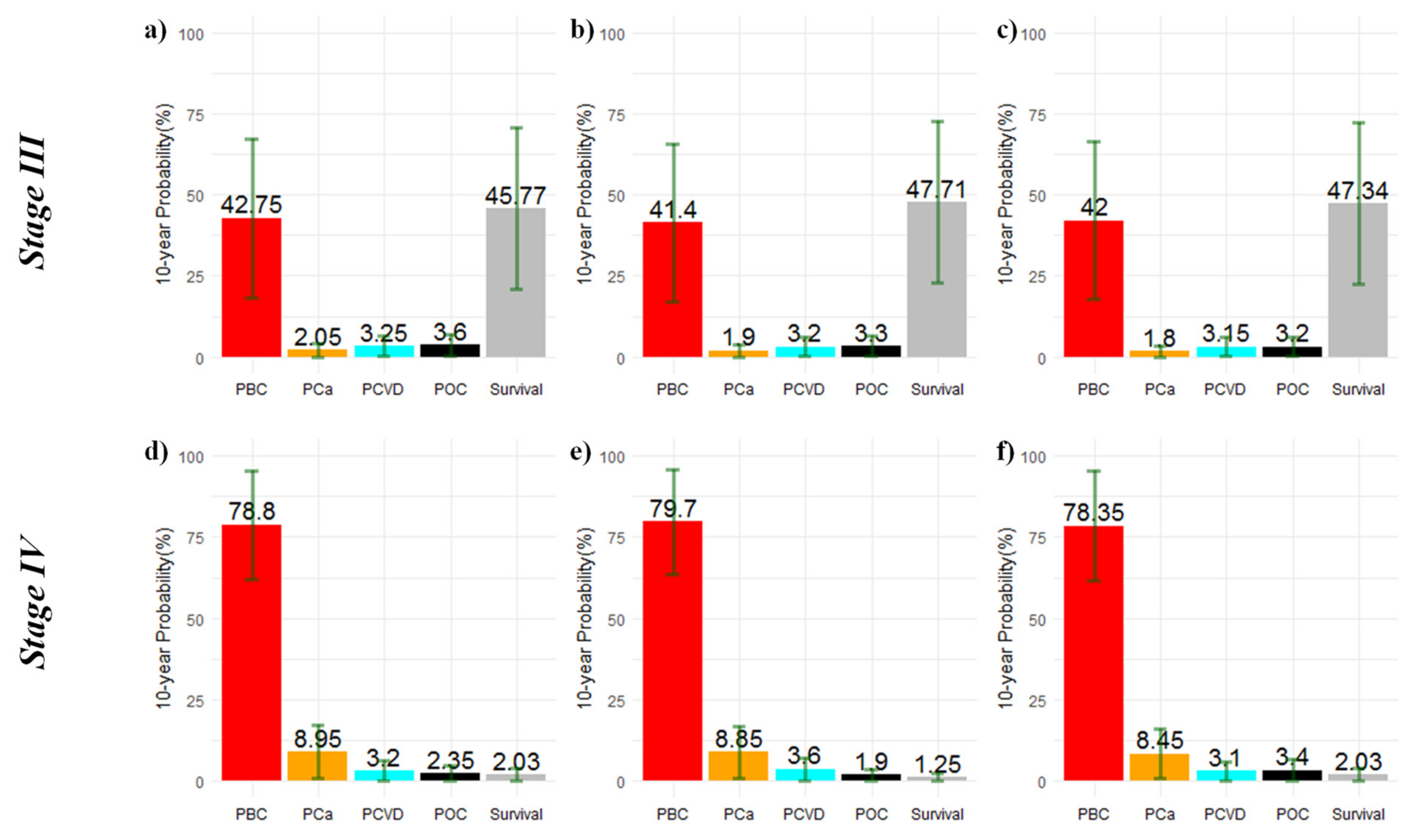
3.2.1. Probabilities of Death According to Age and Stage at Diagnosis
3.2.2. Probabilities of Death According to Stage at Diagnosis when Hormone Receptor Data Is Available
4. Discussion
4.1. Cancer Causes
4.2. Cardiovascular Mortality
4.3. Other Causes of Death
4.4. Cardiovascular Disease as the Competing Risk of Death to Cancer
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dalmartello, M.; La Vecchia, C.; Bertuccio, P.; Boffetta, P.; Levi, F.; Negri, E.; Malvezzi, M. European cancer mortality predictions for the year 2022 with focus on ovarian cancer. Ann. Oncol. 2022, 33, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Dal Maso, L.; Panato, C.; Tavilla, A.; Guzzinati, S.; Serraino, D.; Mallone, S.; Botta, L.; Boussari, O.; Capocaccia, R.; Colonna, M.; et al. Cancer cure for 32 cancer types: Results from the EUROCARE-5 study. Int. J. Epidemiol. 2020, 49, 1517–1525. [Google Scholar] [CrossRef]
- Johansson, A.L.V.; Trewin, C.B.; Fredriksson, I.; Reinertsen, K.V.; Russnes, H. In modern times, how important are breast cancer stage, grade and receptor subtype for survival: A population-based cohort study. Breast Cancer Res. 2021, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Panel Members. Tailoring therapies—improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA-J. Am. Med. Assoc. 2019, 321, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Liu, Z.; Du, S.; Li, J.; Ma, L.; Li, L. Diagnosis and treatment of breast cancer in the precision medicine era. Methods Mol. Biol. 2020, 2204, 53–61. [Google Scholar] [PubMed]
- Allemani, C.; Minicozzi, P.; Berrino, F.; Bastiaannet, E.; Gavin, A.; Galceran, J.; Ameijide, A.; Siesling, S.; Mangone, L.; Ardanaz, E.; et al. Predictions of survival up to 10 years after diagnosis for European women with breast cancer in 2000–2002. Int. J. Cancer 2013, 132, 2404–2412. [Google Scholar] [CrossRef]
- Colzani, E.; Liljegren, A.; Johansson, A.L.; Adolfsson, J.; Hellborg, H.; Hall, P.F.; Czene, K. Prognosis of patients with breast cancer: Causes of death and effects of time since diagnosis, age, and tumour characteristics. J. Clin. Oncol. 2011, 29, 4014–4021. [Google Scholar] [CrossRef]
- Riihimäki, M.; Thomsen, H.; Brandt, A.; Sundquist, J.; Hemminki, K. Death causes in breast cancer patients. Ann. Oncol. 2012, 23, 604–610. [Google Scholar] [CrossRef]
- Ursaru, M.; Jari, I.; Naum, A.; Scripcariu, V.; Negru, D. Causes of Death in Patients With Stage 0-Ii Breast Cancer. Rev. Med. Chir. Soc. Med. Nat. Iasi. 2015, 119, 374–378. [Google Scholar]
- Ameijide, A.; Clèries, R.; Carulla, M.; Buxó, M.; Marcos-Gragera, R.; Martínez, J.M.; Vilardell, M.L.; Vilardell, M.; Espinàs, J.A.; Borràs, J.M.; et al. Cause-specific mortality after a breast cancer diagnosis: A cohort study of 10,195 women in Girona and Tarragona. Clin. Transl. Oncol. 2019, 21, 1014–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afifi, A.M.; Saad, A.M.; Al-Husseini, M.J.; Elmehrath, A.O.; Northfelt, D.W.; Sonbol, M.B. Causes of death after breast cancer diagnosis: A US population-based analysis. Cancer 2020, 126, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Font, R.; Buxó, M.; Ameijide, A.; Martínez, J.M.; Marcos-Gragera, R.; Carulla, M.; Puigdemont, M.; Vilardell, M.; Civit, S.; Viñas, G.; et al. Using population—based data to evaluate the impact of adherence to endocrine therapy on survival in breast cancer through the web—application BreCanSurvPred. Sci. Rep. 2022, 12, 8097. [Google Scholar] [CrossRef] [PubMed]
- Clèries, R.; Buxó, M.; Vilardell, M.; Ameijide, A.; Martínez, J.M.; Font, R.; Marcos-Gragera, R.; Puigdemont, M.; Viñas, G.; Carulla, M.; et al. No Excess Mortality up to 10 Years in Early Stages of Breast Cancer in Women Adherent to Oral Endocrine Therapy: A Probabilistic Graphical Modeling Approach. Int. J. Environ. Res. Public Health 2022, 19, 3605. [Google Scholar] [CrossRef] [PubMed]
- Clèries, R.; Ameijide, A.; Buxó, M.; Martínez, J.M.; Marcos-Gragera, R.; Vilardell, M.L.; Carulla, M.; Yasui, Y.; Vilardell, M.; Espinàs, J.A.; et al. Long-term crude probabilities of death among breast cancer patients by age and stage: A population-based survival study in Northeastern Spain (Girona–Tarragona 1985–2004). Clin. Transl. Oncol. 2018, 20, 1252–1260. [Google Scholar] [CrossRef] [Green Version]
- Agha, A.; Wang, X.; Wang, M.; Lehrer, E.J.; Horn, S.R.; Rosenberg, J.C.; Trifiletti, D.M.; Diaz, R.; Louie, A.V.; Zaorsky, N.G. Long-Term Risk of Death From Heart Disease Among Breast Cancer Patients. Front. Cardiovasc. Med. 2022, 9, 784409. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Richardson, D.B.; Keil, A.P.; Cole, S.R.; MacLehose, R.F. Observed and expected mortality in cohort studies. Am. J. Epidemiol. 2017, 185, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Salmerón, D.; Botta, L.; Martínez, J.M.; Trama, A.; Gatta, G.; Borràs, J.M.; Capocaccia, R.; Clèries, R.; Information Network on Rare Cancers (RARECARENet) Working Group. Estimating Country-Specific Incidence Rates of Rare Cancers: Comparative Performance Analysis of Modeling Approaches Using European Cancer Registry Data. Am. J. Epidemiol. 2022, 191, 487–498. [Google Scholar] [CrossRef]
- Lunn, D.J.; Thomas, A.; Best, N.; Spiegelhalter, D. WinBUGS—A Bayesian modelling framework: Concepts, structure, and extensibility. Stat. Comput. 2000, 10, 325–337. [Google Scholar] [CrossRef]
- Sturtz, S.; Ligges, U.; Gelman, A. R2WinBUGS: A Package for Running WinBUGS. J. Stat. Softw. 2005, 12, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Richardson, S.; Thomson, A.; Best, N.; Elliott, P. Interpreting posterior relative risk estimates in disease-mapping studies. Environ. Health Perspect. 2004, 112, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Kalbfleisch, J.D.; Prentice, R.L. The Statistical Analysis of Failure Time Data; John Wiley and Sons: New York, NY, USA, 2002. [Google Scholar]
- Austin, P.C.; Putter, H.; Lee, D.S.; Steyerberg, E.W. Estimation of the Absolute Risk of Cardiovascular Disease and Other Events: Issues With the Use of Multiple Fine-Gray Subdistribution Hazard Models. Circ. Cardiovasc. Qual. Outcomes 2022, 15, ee008368. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.K.; Geskus, R.B.; De Witte, T.; Putter, H. Competing risks in epidemiology: Possibilities and pitfalls. Int. J. Epidemiol. 2012, 41, 861–870. [Google Scholar] [CrossRef] [Green Version]
- De Glas, N.A.; Kiderlen, M.; Vandenbroucke, J.P.; de Craen, A.J.; Portielje, J.E.; van de Velde, C.J.; Liefers, G.J.; Bastiaannet, E.; Le Cessie, S. Performing Survival Analyses in the Presence of Competing Risks: A Clinical Example in Older Breast Cancer Patients. J. Natl. Cancer Inst. 2016, 108, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putter, H.; Fiocco, M.; Geskus, R.B. Tutorial in biostatistics: Competing risks and multi-state models. Stat. Med. 2007, 26, 2389–2430. [Google Scholar] [CrossRef]
- De Wreede, L.C.; Fiocco, M.; Putter, H. The mstate package for estimation and prediction in non- and semi-parametric multi-state and competing risks models. Comput. Methods Programs Biomed. 2010, 99, 261–274. [Google Scholar] [CrossRef]
- Guan, T.; Zhang, H.; Yang, J.; Lin, W.; Wang, K.; Su, M.; Peng, W.; Li, Y.; Lai, Y.; Liu, C. Increased Risk of Cardiovascular Death in Breast Cancer Patients Without Chemotherapy or (and) Radiotherapy: A Large Population-Based Study. Front. Oncol. 2021, 10, 619622. [Google Scholar] [CrossRef]
- Wang, D.; Yi, L.; Zhang, L.; Wang, Z. Cause-specific mortality among patients with different molecular subtypes of T1-2N0M0 breast cancer: A population-based study. Medicine 2021, 100, e27605. [Google Scholar] [CrossRef]
- Barretina-Ginesta, M.; Galceran, J.; Pla, H.; Meléndez, C.; Carbo Bague, A.; Ameijide, A.; Carulla, M.; Barretina, J.; Izquierdo, A.; Marcos-Gragera, R. Gynaecological malignancies after breast cancer diagnosis: A population-based study. Clin. J. Obstet. Gynecol. 2019, 2, 113–118. [Google Scholar] [CrossRef]
- Akhmedkhanov, A.; Zeleniuch-Jacquotte, A.; Toniolo, P. Role of exogenous and endogenous hormones in endometrial cancer review of the evidence and research perspectives. Ann. N. Y. Acad. Sci. 2001, 943, 296–315. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, F.E.; Benraadt, J.; Coebergh, J.W.; Kiemeney, L.A.; Gimbrère, C.H.; Otter, R.; Schouten, L.J.; Damhuis, R.A.; Bontenbal, M.; Diepenhorst, F.W.; et al. Risk of endometrial cancer after tamoxifen treatment of breast cancer. Lancet 1994, 343, 448–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, B.; Costantino, J.P.; Redmond, C.K.; Fisher, E.R.; Wickerham, D.L.; Cronin, W.M. Endometrial cancer in tamoxifen-treated breast cancer patients: Findings from the national surgical adjuvant breast and bowel project (NSABP) B-14. J. Natl. Cancer Inst. 1994, 86, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.E.; van Leeuwen, F.E.; Hoogendoorn, W.E.; Mourits, M.J.; Hollema, H.; van Boven, H.; Press, M.F.; Bernstein, L.; Swerdlow, A.J. Endometrial cancer survival after breast cancer in relation to tamoxifen treatment: Pooled results from three countries. Breast Cancer Res. 2012, 14, R91. [Google Scholar] [CrossRef] [Green Version]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Jiang, W.; Mao, K.; An, Y.; Su, F.; Kim, B.Y.; Liu, Q.; Jacobs, L.K. Elevated risks of subsequent endometrial cancer development among breast cancer survivors with different hormone receptor status: A SEER analysis. Breast Cancer Res. Treat. 2015, 150, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Trentham-Dietz, A.; Newcomb, P.A.; Nichols, H.B.; Hampton, J.M. Breast cancer risk factors and second primary malignancies among women with breast cancer. Breast Cancer Res. Treat. 2007, 105, 195–207. [Google Scholar] [CrossRef]
- Molina-Montes, E.; Pollán, M.; Payer, T.; Molina, E.; Dávila-Arias, C.; Sánchez, M.J. Risk of second primary cancer among women with breast cancer: A population-based study in Granada (Spain). Gynecol. Oncol. 2013, 130, 340–345. [Google Scholar] [CrossRef]
- Sung, H.; Freedman, R.A.; Siegel, R.L.; Hyun, N.; DeSantis, C.E.; Ruddy, K.J.; Jemal, A. Risks of subsequent primary cancers among breast cancer survivors according to hormone receptor status. Cancer 2021, 127, 3310–3324. [Google Scholar] [CrossRef]
- Druesne-Pecollo, N.; Touvier, M.; Barrandon, E.; Chan, D.S.; Norat, T.; Zelek, L.; Hercberg, S.; Latino-Martel, P. Excess body weight and second primary cancer risk after breast cancer: A systematic review and meta-analysis of prospective studies. Breast Cancer Res. Treat. 2012, 135, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Wijayabahu, A.T.; Egan, K.M.; Yaghjyan, L. Uterine cancer in breast cancer survivors: A systematic review. Breast Cancer Res. Treat. 2020, 180, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Frias-Gomez, J.; Peremiquel-Trillas, P.; Alemany, L.; Ameijide, A.; Marcos-Gragera, R.; Ponce, J.; Brunet, J.; Matias-Guiu, X.; Galceran, J.; Izquierdo, Á.; et al. Predicting the rising incidence and mortality of endometrial cancers among women aged 65-74 years in Catalonia. Maturitas 2021, 144, 11–15. [Google Scholar] [CrossRef]
- Peremiquel-Trillas, P.; Frias-Gomez, J.; Alemany, L.; Ameijide, A.; Vilardell, M.; Marcos-Gragera, R.; Paytubi, S.; Ponce, J.; Martínez, J.M.; Pineda, M.; et al. Predicting Ovarian-Cancer Burden in Catalonia by 2030: An Age–Period–Cohort Modelling. Int. J. Environ. Res. Public Health 2022, 19, 1404. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Olivotto, I.A.; Foulkes, W.D.; Warner, E.; Olopade, O.; Eisen, A.; Weber, B.; et al. The risk of ovarian cancer after breast cancer in BRCA1 and BRCA2 carriers. Gynecol. Oncol. 2005, 96, 222–226. [Google Scholar] [CrossRef]
- Pennington, K.P.; Swisher, E.M. Hereditary ovarian cancer: Beyond the usual suspects. Gynecol. Oncol. 2012, 124, 347–353. [Google Scholar] [CrossRef]
- Berrington de Gonzalez, A.; Curtis, R.E.; Gilbert, E.; Berg, C.D.; Smith, S.A.; Stovall, M.; Ron, E. Second solid cancers after radiotherapy for breast cancer in SEER cancer registries. Br. J. Cancer 2010, 102, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Long, Q.; Wang, Y.; Che, G. Primary lung cancer after treatment for breast cancer. Int. J. Womens Health 2021, 13, 1217–1225. [Google Scholar] [CrossRef]
- Xiao, W.; Zheng, S.; Liu, P.; Zou, Y.; Xie, X.; Yu, P.; Tang, H.; Xie, X. Risk factors and survival outcomes in patients with breast cancer and lung metastasis: A population-based study. Cancer Med. 2018, 7, 922–930. [Google Scholar] [CrossRef]
- Simonetto, C.; Wollschläger, D.; Kundrát, P.; Ulanowski, A.; Becker, J.; Castelletti, N.; Güthlin, D.; Shemiakina, E.; Eidemüller, M. Estimating long-term health risks after breast cancer radiotherapy: Merging evidence from low and high doses. Radiat. Environ. Biophys. 2021, 60, 459–474. [Google Scholar] [CrossRef]
- Clèries, R.; Ameijide, A.; Marcos-Gragera, R.; Pareja, L.; Carulla, M.; Vilardell, M.L.; Esteban, L.; Buxó, M.; Espinàs, J.A.; Puigdefàbregas, A.; et al. Predicting the cancer burden in Catalonia between 2015 and 2025: The challenge of cancer management in the elderly. Clin. Transl. Oncol. 2018, 20, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Cheng, L.; Zhu, X.; Gao, Y.; Fan, L.; Wang, Z. Risk and prognostic factors of breast cancer with liver metastases. BMC. Cancer 2021, 21, 238. [Google Scholar] [CrossRef] [PubMed]
- Purushotham, A.; Shamil, E.; Cariati, M.; Agbaje, O.; Muhidin, A.; Gillett, C.; Mera, A.; Sivanadiyan, K.; Harries, M.; Sullivan, R.; et al. Age at diagnosis and distant metastasis in breast cancer—A surprising inverse relationship. Eur. J. Cancer 2014, 50, 1697–1705. [Google Scholar] [CrossRef]
- Chen, Q.W.; Li, H.J.; Chen, Y.N.; Ning, Z.Y.; Gao, S.; Shen, Y.H.; Meng, Z.Q.; Vargulick, S.; Wang, B.Y.; Chen, H. Hepatic lesions detected after mastectomy, in breast cancer patients with hepatitis background may need to undergo liver biopsy to rule out second primary hepatocellular carcinoma. PLoS ONE 2016, 11, e0139782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonapasta, S.A.; Gregori, M.; Lanza, R.; Sangiorgi, E.; Menghi, A.; Scarpini, M.; Modesti, M. Metastasis to the pancreas from breast cancer: Difficulties in diagnosis and controversies in treatment. Breast Care 2010, 5, 170–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagao, A.; Noie, T.; Horiuch, H.; Yamada, H.; Momiyama, M.; Nakajima, K.; Satou, S.; Satodate, H.; Nara, S.; Harihara, Y. Long-term survival after pancreatic metastasis resection from breast cancer: A systematic literature review. Surg. Case Rep. 2021, 7, 39. [Google Scholar] [CrossRef]
- Mocci, E.; Milne, R.L.; Méndez-Villamil, E.Y.; Hopper, J.L.; John, E.M.; Andrulis, I.L.; Chung, W.K.; Daly, M.; Buys, S.S.; Malats, N.; et al. Risk of pancreatic cancer in breast cancer families from the breast cancer family registry. Cancer Epidemiol. Biomark. Prev. 2013, 22, 803–811. [Google Scholar] [CrossRef] [Green Version]
- Castro, M.; Vierkoetter, K.; Prager, D.; Montgomery, S.; Sedgwick, K. Synchronous Onset of Breast and Pancreatic Cancers: Results of Germline and Somatic Genetic Analysis. Case Rep. Oncol. 2016, 9, 387–394. [Google Scholar] [CrossRef]
- Vo, J.B.; Ramin, C.; Barac, A.; Berrington de Gonzalez, A.; Veiga, L. Trends in heart disease mortality among breast cancer survivors in the US, 1975–2017. Breast Cancer Res. Treat. 2022, 192, 611–622. [Google Scholar] [CrossRef]
- Zhu, Q.; Kirova, Y.M.; Cao, L.; Arsene-Henry, A.; Chen, J. Cardiotoxicity associated with radiotherapy in breast cancer: A question-based review with current literatures. Cancer Treat Rev. 2018, 68, 9–15. [Google Scholar] [CrossRef]
- Henson, K.E.; McGale, P.; Darby, S.C.; Parkin, M.; Wang, Y.; Taylor, C.W. Cardiac mortality after radiotherapy, chemotherapy and endocrine therapy for breast cancer: Cohort study of 2 million women from 57 cancer registries in 22 countries. Int. J. Cancer. 2020, 147, 1437–1449. [Google Scholar] [CrossRef] [PubMed]
- Blaes, A.; Beckwith, H.; Florea, N.; Hebbel, R.; Solovey, A.; Potter, D.; Yee, D.; Vogel, R.; Luepker, R.; Duprez, D. Vascular function in breast cancer survivors on aromatase inhibitors: A pilot study. Breast Cancer Res. Treat. 2017, 166, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Mehta, L.S.; Watson, K.E.; Barac, A.; Beckie, T.M.; Bittner, V.; Cruz-Flores, S.; Dent, S.; Kondapalli, L.; Ky, B.; Okwuosa, T.; et al. Cardiovascular Disease and Breast Cancer: Where These Entities Intersect: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e30–e66. [Google Scholar] [CrossRef] [PubMed]
- Bikiewicz, A.; Banach, M.; von Haehling, S.; Maciejewski, M.; Bielecka-Dabrowa, A. Adjuvant breast cancer treatments cardiotoxicity and modern methods of detection and prevention of cardiac complications. ESC Heart Fail. 2021, 8, 2397–2418. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.F.; Jones, L.W. Breast cancer treatment-associated cardiovascular toxicity and effects of exercise countermeasures. Cardio-Oncology 2016, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamirani, Y.; Fanous, I.; Kramer, C.M.; Wong, A.; Salerno, M.; Dillon, P. Anthracycline- and trastuzumab-induced cardiotoxicity: A retrospective study. Med. Oncol. 2016, 33, 20–22. [Google Scholar] [CrossRef] [Green Version]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [Green Version]
- Azoury, F.; Misra, S.; Barry, A.; Helou, J. Role of radiation therapy in triple negative breast cancer: Current state and future directions—A narrative review. Precis. Cancer Med. 2022, 5, 3. [Google Scholar] [CrossRef]
- Li, P.; Wang, T.; Zeng, C.; Yang, M.; Li, G.; Han, J.; Wu, W. Association between metabolic syndrome and prognosis of breast cancer: A meta-analysis of follow-up studies. Diabetol. Metab. Syndr. 2020, 12, 10. [Google Scholar] [CrossRef]
- Dong, S.; Wang, Z.; Shen, K.; Chen, X. Metabolic Syndrome and Breast Cancer: Prevalence, Treatment Response, and Prognosis. Front. Oncol. 2021, 11, 629666. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, X.; Gu, C.; Xia, J. Influence of diabetes mellitus on mortality in breast cancer patients. ANZ J. Surg. 2015, 85, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Dubose, A.C.; Chu, Q.D.; Li, B.D.L.; Kim, R.H. Is chronic kidney disease an independent risk factor for mortality in breast cancer? J. Surg. Res. 2013, 184, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Pascual, M.C.; Montaño, J.J.; Franch, P.; Sánchez-Contador, C.; Ramos, M. Survival of Breast Cancer by Stage, Grade and Molecular Groups in Mallorca, Spain. J. Clin. Med. 2022, 11, 5708. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.; Aitken, J.F.; Pyke, C.; Baade, P.D. Competing mortality risks among women aged 50-79 years when diagnosed with invasive breast cancer, Queensland, 1997-2012. Breast 2018, 41, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.; Austin, P.C.; Lee, D.S.; Amir, E.; Tu, J.V.; Thavendiranathan, P.; Fung, K.; Anderson, G.M. A Population-Based Study of Cardiovascular Mortality Following Early-Stage Breast Cancer. JAMA Cardiol. 2017, 2, 88–93. [Google Scholar] [CrossRef]
- Derks, M.G.M.; Bastiaannet, E.; van de Water, W.; de Glas, N.A.; Seynaeve, C.; Putter, H.; Nortier, J.W.R.; Rea, D.; Hasenburg, A.; Markopoulos, C.; et al. Impact of age on breast cancer mortality and competing causes of death at 10 years follow-up in the adjuvant TEAM trial. Eur. J. Cancer 2018, 99, 1–8. [Google Scholar] [CrossRef]
- Kolodziejczyk, C.; Jakobsen, M.; Sall Jensen, M.; Poulsen, P.B.; Khan, H.; Kümler, T.; Andersson, M. Mortality from cardiovascular disease in women with breast cancer—a nationwide registry study. Acta Oncol. 2021, 60, 1257–1263. [Google Scholar] [CrossRef]
- Xu, Y.B.; Liu, H.; Cao, Q.H.; Ji, J.L.; Dong, R.R.; Xu, D. Evaluating overall survival and competing risks of survival in patients with early-stage breast cancer using a comprehensive nomogram. Cancer Med. 2020, 9, 4095–4106. [Google Scholar] [CrossRef] [Green Version]
- Leung, A.M.; Vu, H.N.; Nguyen, K.A.; Thacker, L.R.; Bear, H.D. Effects of Surgical Excision on Survival of Patients With Stage IV Breast Cancer. J. Surg. Res. 2010, 161, 83–88. [Google Scholar] [CrossRef]
- Wang, R.; Zhu, Y.; Liu, X.; Liao, X.; He, J.; Niu, L. The Clinicopathological Features and Survival Outcomes of Patients With Different Metastatic Sites in Stage IV Breast Cancer. BMC Cancer. 2019, 19, 1091. [Google Scholar] [CrossRef] [Green Version]
- Rogoz, B.; Houzé de l’Aulnoit, A.; Duhamel, A.; Houzé de l’Aulnoit, D. Thirty-Year Trends of Survival and Time-Varying Effects of Prognostic Factors in Patients With Metastatic Breast Cancer-A Single Institution Experience. Clin. Breast Cancer 2018, 18, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Wissing, M.D.; Greenwald, Z.R.; Franco, E.L. Improving the reporting of cancer-specific mortality and survival in research using cancer registry data. Cancer Epidemiol. 2019, 59, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Izci, H.; Tambuyzer, T.; Vandeven, J.; Xicluna, J.; Wildiers, H.; Punie, K.; Willers, N.; Oldenburger, E.; Van Nieuwenhuysen, E.; Berteloot, P.; et al. Cause of death for patients with breast cancer: Discordance between death certificates and medical files, and impact on survival estimates. Arch. Public Heal. 2021, 79, 111. [Google Scholar] [CrossRef]
- Lafourcade, A.; His, M.; Baglietto, L.; Boutron-Ruault, M.C.; Dossus, L.; Rondeau, V. Factors associated with breast cancer recurrences or mortality and dynamic prediction of death using history of cancer recurrences: The French E3N cohort. BMC Cancer 2018, 18, 171. [Google Scholar] [CrossRef] [PubMed]
- Roel, E.; Pistillo, A.; Recalde, M.; Fernández-Bertolín, S.; Aragón, M.; Soerjomataram, I.; Jenab, M.; Puente, D.; Prieto-Alhambra, D.; Burn, E.; et al. Cancer and the risk of coronavirus disease 2019 diagnosis, hospitalisation and death: A population-based multistate cohort study including 4 618 377 adults in Catalonia, Spain. Int. J. Cancer 2022, 150, 782–794. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total cohort 2000–2009 (N = 6758) | Diagnosed 2000–2004 (N = 3296) | Diagnosed 2005–2009 (N = 3462) | p Value | |
|---|---|---|---|---|
| Registry | ||||
| Girona | 3213 (47.5%) | 1549 (47.1%) | 1664 (48.1%) | 0.77 |
| Tarragona | 3545 (52.5%) | 1747 (52.9%) | 1798 (51.9%) | |
| Age | ||||
| Mean (SD) | 59.1 (14.3) | 59.7 (14.9) | 58.6 (13.6) | 0.35 (a) |
| Age group | ||||
| ≤49 | 1880 (27.8%) | 863 (26.2%) | 1017 (29.4%) | 0.18 |
| 50–68 | 3718 (55.0%) | 1844 (55.9%) | 1874 (54.1%) | |
| ≥69 | 1163 (17.2%) | 592 (17.9%) | 571 (16.5%) | |
| Stage | ||||
| I | 2257 (33.9%) | 1084 (32.9%) | 1173 (33.9%) | <0.01 |
| II | 2478 (36.7%) | 1284 (39.0%) | 1194 (34.5%) | |
| III | 1080 (16.0%) | 475 (14.4%) | 605 (17.5%) | |
| IV | 463 (6.8%) | 208 (6.3%) | 255 (7.4%) | |
| Missing | 484 (7.1%) | 249 (7.4%) | 235 (6.7%) | |
| Cause of death | ||||
| Breast cancer | 1296 (19.2%) | 744 (21.5%) | 552 (15.9%) | <0.01 |
| Other cancer (a) | 196 (2.9%) | 95 (2.7%) | 101 (3.0%) | |
| Cardiovascular disease | 218 (3.2%) | 112 (3.2%) | 106 (3.2%) | |
| Other causes | 306 (4.5%) | 136 (3.9%) | 170 (4.9%) | |
| Alive | 4582 (67.8%) | 2056 (59.3%) | 2526 (72.9%) | |
| Follow-up (years) | ||||
| Mean (SD) | 8.3 (2.9) | 8.0 (3.1) | 8.6 (2.7) | 0.33 (a) |
| Molecular subtype | ||||
| HR+ | 2748 (40.6%) | * | 2748 (70.4%) | (b) |
| HR− | 547 (8.1%) | * | 547 (15.8%) | |
| Unknown | 3463 (51.2%) | * | 167 (4.8%) |
| 2000–2004 Cohort | 2005–2009 Cohort | Ratio | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cause | O1 | % | SMR1 | PSMR1 | O2 | % | SMR2 | PSMR2 | SMR2/SMR1 | PRatio |
| All causes (except breast cancer) | 337 | 100.0 | 1.16 | 0.98 | 365 | 100.0 | 1.14 | 0.97 | 0.98 | 0.14 |
| Infectious diseases | 7 | 2.1 | 1.22 | 0.66 | 7 | 1.9 | 1.07 | 0.53 | 0.88 | 0.35 |
| Tumours (except breast) | 95 | 28.2 | 1.34 | 0.98 | 101 | 27.7 | 1.24 | 0.97 | 0.92 | 0.22 |
| Diseases of the blood/hematopoietic organs | 1 | 0.3 | 0.34 | 0.05 | 1 | 0.3 | 0.51 | 0.14 | 1.50 | 0.75 |
| Endocrine, nutritional-metabolic diseases | 13 | 3.8 | 1.17 | 0.67 | 15 | 4.1 | 1.41 | 0.88 | 1.21 | 0.69 |
| Mental and behavioural disorders | 14 | 4.2 | 0.79 | 0.15 | 17 | 4.7 | 0.69 | 0.04 | 0.87 | 0.36 |
| Diseases of the nervous system/organs of the senses | 20 | 5.9 | 1.07 | 0.59 | 20 | 5.5 | 0.77 | 0.10 | 0.72 | 0.21 |
| Cardiovascular disease/circulatory system | 112 | 33.2 | 1.13 | 0.90 | 106 | 29.0 | 1.32 | 0.99 | 1.17 | 0.97 |
| Diseases of the respiratory system | 21 | 6.2 | 0.85 | 0.21 | 37 | 10.1 | 1.24 | 0.89 | 1.46 | 0.91 |
| Diseases of the digestive system | 20 | 5.9 | 1.37 | 0.91 | 17 | 4.7 | 0.74 | 0.08 | 0.54 | 0.12 |
| Diseases of the skin and subcutaneous tissue | 1 | 0.3 | 0.67 | 0.22 | 2 | 0.6 | 1.96 | 0.73 | 2.93 | 0.81 |
| Musculoskeletal system and connective tissue | 4 | 1.2 | 1.50 | 0.72 | 8 | 2.2 | 1.68 | 0.79 | 1.32 | 0.70 |
| Diseases of the genitourinary system | 11 | 3.3 | 1.38 | 0.82 | 18 | 4.9 | 1.20 | 0.75 | 0.87 | 0.37 |
| Congenital malformations | 4 | 1.2 | 5.72 | 0.99 | 0 | 0.0 | 0.00 | 0.36 | 0.00 | 0.14 |
| Symptoms, signs, and abnormal findings | 7 | 2.1 | 1.30 | 0.72 | 8 | 2.2 | 1.38 | 0.77 | 1.06 | 0.54 |
| External causes of mortality | 7 | 2.1 | 1.01 | 0.47 | 8 | 2.2 | 0.97 | 0.40 | 0.96 | 0.46 |
| Cox Modelling * | Cause-Specific Hazard (CSH) ** | ||
|---|---|---|---|
| All-Cause | BC | Non-BC | |
| Mortality | Mortality | Mortality | |
| RR (HR− vs HR+) | RR (HR− vs HR+) | RR (HR− vs HR+) | |
| Dataset | 95% CI | 95% CI | 95% CI |
| Stage I | 1.72 (1.08; 2.77) | 6.11 (1.97; 9.59) | 0.76 (0.35; 1.37) |
| Stage II | 1.18 (1.09; 1.79) | 1.62 (1.13; 3.63) | 0.95 (0.78; 2.22) |
| Stage III | 1.38 (1.11; 1.96) | 1.68 (1.21; 3.85) | 0.67 (0.26; 2.72) |
| Stage IV | 1.08 (1.02; 1.35) | 1.29 (1.08; 4.44) | 0.75 (0.42; 1.47) |
| Age at Diagnosis of BC | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤49 Years | 50–68 Years | ≥69 Years | ||||||||||||||
| PBC (%) | PCa (%) | PCVD (%) | POC (%) | Total (%) | PBC (%) | PCa (%) | PCVD (%) | POC (%) | Total (%) | PBC (%) | PCa (%) | PCVD (%) | POC (%) | Total (%) | ||
| Stage I | HR+ | 1.81 | 3.71 | 1.21 | 3.31 | 10.04 | 1.71 | 3.64 | 1.42 | 3.21 | 9.98 | 1.71 | 4.11 | 1.31 | 3.12 | 10.25 |
| HR− | 9.71 | 3.72 | 0.61 | 3.40 | 17.44 | 10.42 | 4.42 | 0.41 | 2.71 | 17.96 | 10.82 | 3.33 | 0.12 | 2.71 | 16.98 | |
| Ratio | (−/+) | 5.36 | 1.00 | 0.50 | 1.03 | 1.74 | 6.09 | 1.21 | 0.29 | 0.84 | 1.80 | 6.33 | 0.81 | 0.09 | 0.87 | 1.66 |
| Stage II | HR+ | 9.31 | 2.51 | 3.23 | 5.14 | 20.19 | 9.01 | 2.04 | 3.01 | 5.01 | 19.07 | 9.61 | 2.41 | 3.41 | 4.42 | 19.85 |
| HR− | 15.12 | 2.61 | 3.34 | 3.32 | 24.39 | 14.11 | 2.82 | 3.86 | 2.43 | 23.22 | 14.65 | 2.72 | 3.71 | 2.51 | 23.59 | |
| Ratio | (−/+) | 1.62 | 1.04 | 1.03 | 0.65 | 1.21 | 1.53 | 1.21 | 1.17 | 0.48 | 1.16 | 1.52 | 1.13 | 1.09 | 0.57 | 1.19 |
| Stage III | HR+ | 32.21 | 2.91 | 3.23 | 3.75 | 42.10 | 32.99 | 2.91 | 3.11 | 3.82 | 42.83 | 32.91 | 3.11 | 3.11 | 4.28 | 43.41 |
| HR− | 53.34 | 1.23 | 3.31 | 3.52 | 61.40 | 49.94 | 0.94 | 3.31 | 2.84 | 57.03 | 52.15 | 0.54 | 3.25 | 2.77 | 58.71 | |
| Ratio | (−/+) | 1.66 | 0.42 | 1.02 | 0.94 | 1.41 | 1.51 | 0.32 | 1.06 | 0.74 | 1.33 | 1.58 | 0.17 | 1.05 | 0.65 | 1.38 |
| Stage IV | HR+ | 70.31 | 12.43 | 3.16 | 3.39 | 89.29 | 72.61 | 12.22 | 3.43 | 2.76 | 91.02 | 70.61 | 13.76 | 2.84 | 4.75 | 91.96 |
| HR− | 87.35 | 5.57 | 3.33 | 1.44 | 97.69 | 86.82 | 5.56 | 3.85 | 1.15 | 97.38 | 87.14 | 5.21 | 3.43 | 2.12 | 97.90 | |
| Ratio | (−/+) | 1.24 | 0.45 | 1.05 | 0.42 | 1.09 | 1.20 | 0.45 | 1.12 | 0.42 | 1.07 | 1.23 | 0.38 | 1.21 | 0.45 | 1.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clèries, R.; Ameijide, A.; Buxó, M.; Vilardell, M.; Martínez, J.M.; Font, R.; Marcos-Gragera, R.; Puigdemont, M.; Viñas, G.; Carulla, M.; et al. Ten-Year Probabilities of Death Due to Cancer and Cardiovascular Disease among Breast Cancer Patients Diagnosed in North-Eastern Spain. Int. J. Environ. Res. Public Health 2023, 20, 405. https://doi.org/10.3390/ijerph20010405
Clèries R, Ameijide A, Buxó M, Vilardell M, Martínez JM, Font R, Marcos-Gragera R, Puigdemont M, Viñas G, Carulla M, et al. Ten-Year Probabilities of Death Due to Cancer and Cardiovascular Disease among Breast Cancer Patients Diagnosed in North-Eastern Spain. International Journal of Environmental Research and Public Health. 2023; 20(1):405. https://doi.org/10.3390/ijerph20010405
Chicago/Turabian StyleClèries, Ramon, Alberto Ameijide, Maria Buxó, Mireia Vilardell, José Miguel Martínez, Rebeca Font, Rafael Marcos-Gragera, Montse Puigdemont, Gemma Viñas, Marià Carulla, and et al. 2023. "Ten-Year Probabilities of Death Due to Cancer and Cardiovascular Disease among Breast Cancer Patients Diagnosed in North-Eastern Spain" International Journal of Environmental Research and Public Health 20, no. 1: 405. https://doi.org/10.3390/ijerph20010405