
Impacts of Indoor Radon on Health: A Comprehensive Review on Causes, Assessment and Remediation Strategies

 , , , and
, , , and 
Abstract
:1. Introduction
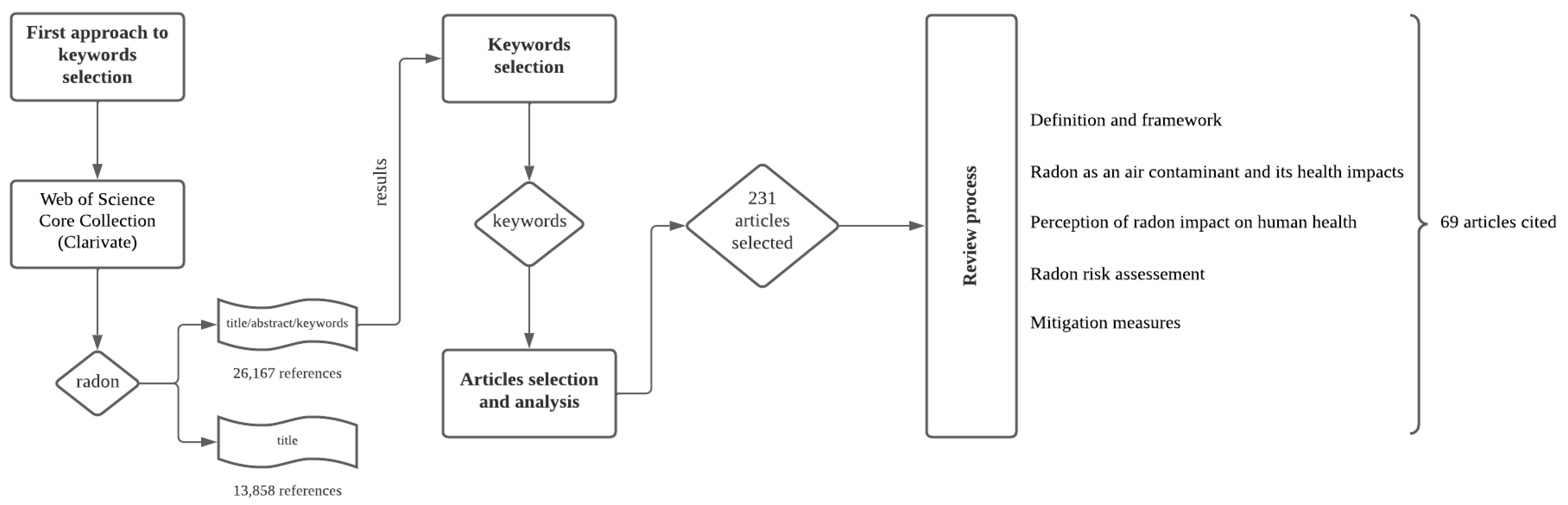
2. Materials and Methods
3. State-of-the Art
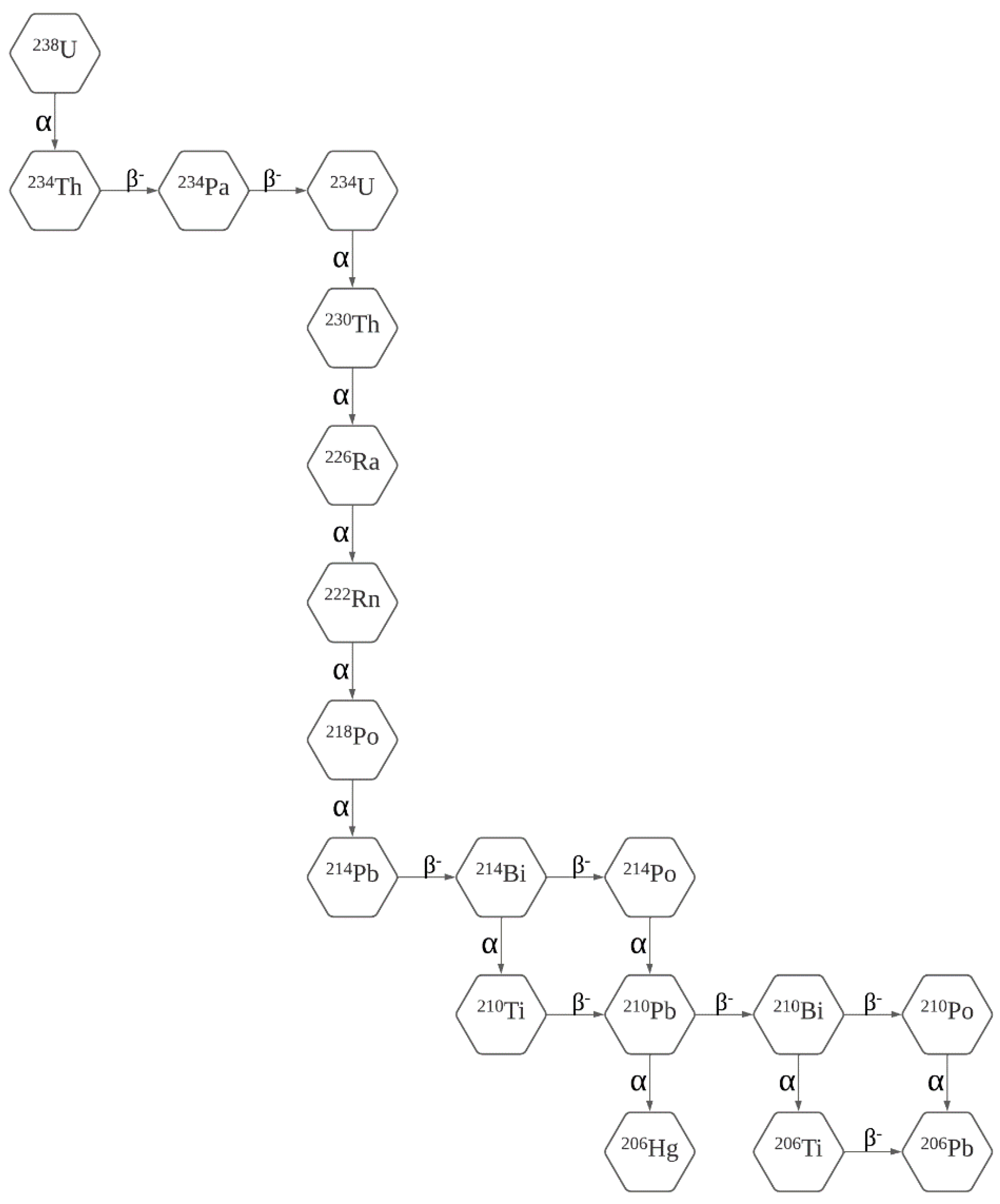
3.1. Definition and Framework
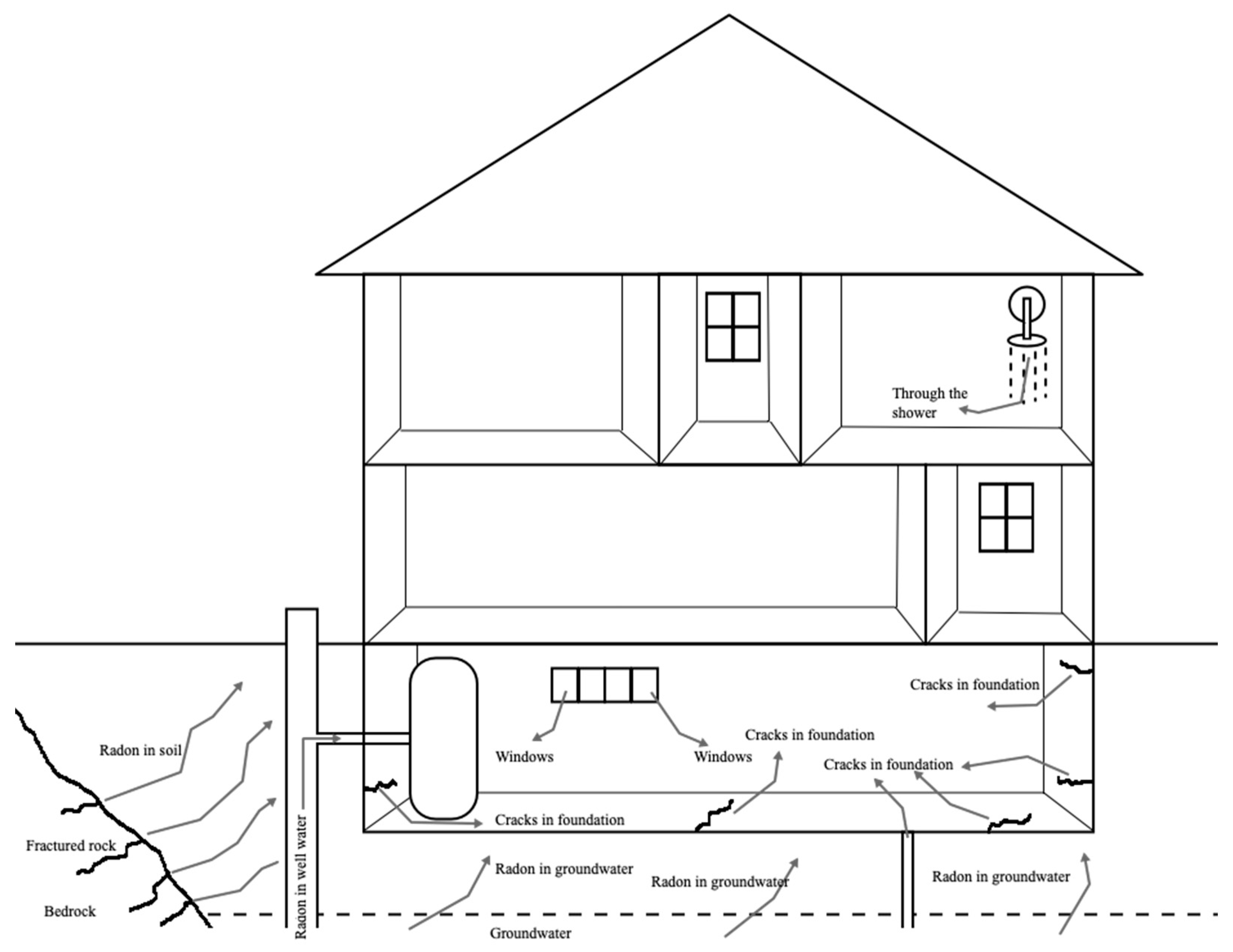
3.2. Radon as an Air Contaminant and Its Health Impacts
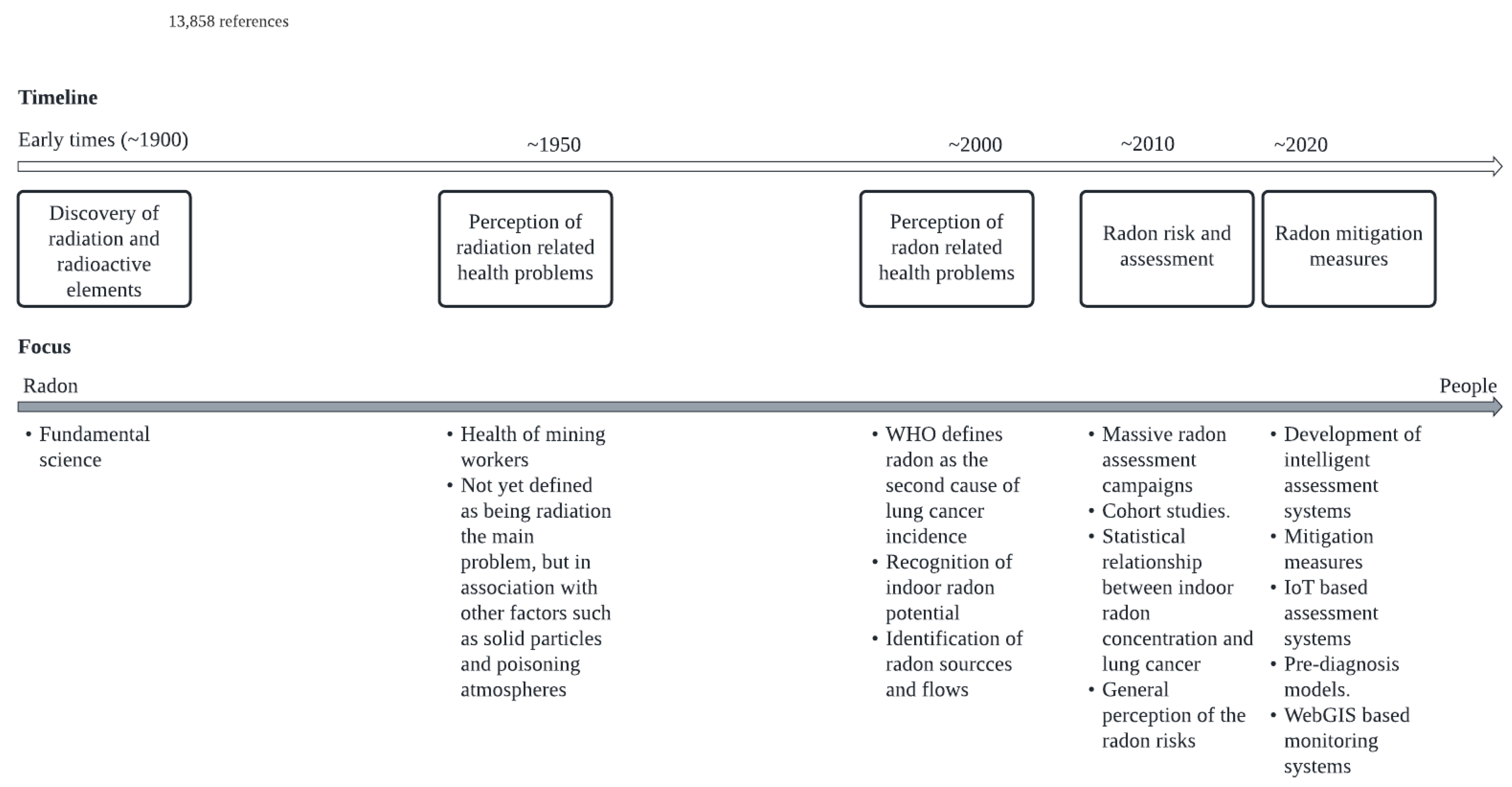
3.3. Perception of Radon Impact on Human Health
3.4. Radon Risk Assessement
3.5. Mitigation Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Handbook on Indoor Radon: A Public Health Perspective; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Samet, J.M.; Hornung, R.W. Review of radon and lung cancer risk. Risk Anal. 1990, 10, 65–75. [Google Scholar] [CrossRef]
- Lowry, S. Housing and health: Indoor air quality. BMJ Br. Med. J. 1989, 299, 1388. [Google Scholar] [CrossRef] [Green Version]
- Sethi, T.K.; El-Ghamry, M.N.; Kloecker, G.H. Radon and lung cancer. Clin. Adv. Hematol. Oncol. 2012, 10, 157–164. [Google Scholar]
- Zielinski, J.M.; Carr, Z.; Krewski, D.; Repacholi, M. World Health Organization’s International Radon Project. J. Toxicol. Environ. Health Part A 2006, 69, 759–769. [Google Scholar] [CrossRef]
- World Health Organization. International Radon Project: Survey on Radon Guidelines, Programmes and Activities; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Ruano-Ravina, A.; Faraldo-Vallés, M.J.; Barros-Dios, J.M. Is there a specific mutation of p53 gene due to radon exposure? A systematic review. Int. J. Radiat. Biol. 2009, 85, 614–621. [Google Scholar] [CrossRef]
- Darby, S.; Hill, D.; Auvinen, A.; Barros-Dios, J.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M. Radon in homes and risk of lung cancer: Collaborative analysis of individual data from 13 European case-control studies. BMJ 2005, 330, 223. [Google Scholar] [CrossRef] [Green Version]
- Möhner, M. Re:“Reanalysis of diesel engine exhaust and lung cancer mortality in the Diesel Exhaust in Miners Study cohort using alternative exposure estimates and radon adjustment” and “diesel exhaust and lung cancer—Aftermath of becoming an IARC Group 1 carcinogen”. Am. J. Epidemiol. 2019, 188, 484–485. [Google Scholar] [CrossRef]
- Field, R.W.; Steck, D.J.; Smith, B.J.; Brus, C.P.; Fisher, E.L.; Neuberger, J.S.; Platz, C.E.; Robinson, R.A.; Woolson, R.F.; Lynch, C.F. Residential radon gas exposure and lung cancer: The Iowa Radon Lung Cancer Study. Am. J. Epidemiol. 2000, 151, 1091–1102. [Google Scholar] [CrossRef] [Green Version]
- Gaskin, J.; Coyle, D.; Whyte, J.; Krewksi, D. Global estimate of lung cancer mortality attributable to residential radon. Environ. Health Perspect. 2018, 126, 057009. [Google Scholar] [CrossRef]
- Ruano-Ravina, A.; Lema, L.V.; Talavera, M.G.; Gómez, M.G.; Muñoz, S.G.; Santiago-Pérez, M.I.; Rey-Brandariz, J.; Barros-Dios, J.; Pérez-Ríos, M. Lung cancer mortality attributable to residential radon exposure in Spain and its regions. Environ. Res. 2021, 199, 111372. [Google Scholar] [CrossRef]
- Vogeltanz-Holm, N.; Schwartz, G.G. Radon and lung cancer: What does the public really know? J. Environ. Radioact. 2018, 192, 26–31. [Google Scholar] [CrossRef]
- Lopes, S.I.; Nunes, L.J.; Curado, A. Designing an Indoor Radon Risk Exposure Indicator (IRREI): An Evaluation Tool for Risk Management and Communication in the IoT Age. Int. J. Environ. Res. Public Health 2021, 18, 7907. [Google Scholar] [CrossRef]
- Lorenzo-Gonzalez, M.; Ruano-Ravina, A.; Torres-Duran, M.; Kelsey, K.T.; Provencio, M.; Parente-Lamelas, I.; Piñeiro-Lamas, M.; Varela-Lema, L.; Perez-Rios, M.; Fernandez-Villar, A. Lung cancer risk and residential radon exposure: A pooling of case-control studies in northwestern Spain. Environ. Res. 2020, 189, 109968. [Google Scholar] [CrossRef]
- Rodríguez-Martínez, Á.; Torres-Duran, M.; Barros-Dios, J.M.; Ruano-Ravina, A. Residential radon and small cell lung cancer. A systematic review. Cancer Lett. 2018, 426, 57–62. [Google Scholar] [CrossRef]
- Mudd, G.M. Radon sources and impacts: A review of mining and non-mining issues. Rev. Environ. Sci. Bio/Technol. 2008, 7, 325–353. [Google Scholar] [CrossRef]
- Schubert, M.; Paschke, A.; Lieberman, E.; Burnett, W.C. Air–water partitioning of 222Rn and its dependence on water temperature and salinity. Environ. Sci. Technol. 2012, 46, 3905–3911. [Google Scholar] [CrossRef]
- Sextro, R.G. Radon and the natural environment. Radon Preval. Meas. Health Risks Control. 1994, 15, 9–32. [Google Scholar]
- Weigel, F. Radon. Chem. Ztg 1978, 102, 287–299. [Google Scholar]
- Lauria, D.C. Evaluating the occurrence and spatial distribution of the radioactive isotopes 226Ra, 228Ra, 222Rn and 238U in the groundwaters of região dos lagos-rj brazil. Hidrogeologia 2004, 4, 47–55. [Google Scholar]
- Pressyanov, D.S.; Guelev, M.G.; Sharkov, B.G. Radon and radon progeny outdoors in a valley of enhanced natural radioactivity. Atmos. Environ. 1995, 29, 3433–3439. [Google Scholar] [CrossRef]
- Cowart, J.; Burnett, W. The Distribution of Uranium and Thorium Decay-Series Radionuclides in the Environment—A Review. J. Environ. Qual. 1994, 23, 651–662. [Google Scholar] [CrossRef]
- Williams, R.W.; Gill, J.B. Effects of partial melting on the uranium decay series. Geochim. Cosmochim. Acta 1989, 53, 1607–1619. [Google Scholar] [CrossRef]
- Ku, T.-L. The uranium-series methods of age determination. Annu. Rev. Earth Planet. Sci. 1976, 4, 347–379. [Google Scholar] [CrossRef]
- Wilkening, M. Radon in the Environment; Elsevier: Amsterdam, The Netherlands, 1990. [Google Scholar]
- Robertson, A.; Allen, J.; Laney, R.; Curnow, A. The cellular and molecular carcinogenic effects of radon exposure: A review. Int. J. Mol. Sci. 2013, 14, 14024–14063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakoda, A.; Ishimori, Y.; Yamaoka, K.; Kataoka, T.; Mitsunobu, F. Absorbed doses of lungs from radon retained in airway lumens of mice and rats. Radiat. Environ. Biophys. 2013, 52, 389–395. [Google Scholar] [CrossRef]
- Samet, J.M.; Avila-Tang, E.; Boffetta, P.; Hannan, L.M.; Olivo-Marston, S.; Thun, M.J.; Rudin, C.M. Lung cancer in never smokers: Clinical epidemiology and environmental risk factors. Clin. Cancer Res. 2009, 15, 5626–5645. [Google Scholar] [CrossRef] [Green Version]
- Tollefsen, T.; Gruber, V.; Bossew, P.; De Cort, M. Status of the European indoor radon map. Radiat. Prot. Dosim. 2011, 145, 110–116. [Google Scholar] [CrossRef]
- Ruano-Ravina, A.; Wakeford, R. The increasing exposure of the global population to ionizing radiation. Epidemiology 2020, 31, 155–159. [Google Scholar] [CrossRef]
- Bersimbaev, R.I.; Bulgakova, O. The health effects of radon and uranium on the population of Kazakhstan. Genes Environ. 2015, 37, 18. [Google Scholar] [CrossRef] [Green Version]
- Popp, W.; Plappert, U.; Müller, W.-U.; Rehn, B.; Schneider, J.; Braun, A.; Bauer, P.; Vahrenholz, C.; Presek, P.; Brauksiepe, A. Biomarkers of genetic damage and inflammation in blood and bronchoalveolar lavage fluid among former German uranium miners: A pilot study. Radiat. Environ. Biophys. 2000, 39, 275–282. [Google Scholar] [CrossRef]
- Darby, S.; Hill, D.; Deo, H.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Falk, R.; Farchi, S.; Figueiras, A. Residential radon and lung cancer—Detailed results of a collaborative analysis of individual data on 7148 persons with lung cancer and 14 208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand. J. Work Environ. Health 2006, 32, 1–84. [Google Scholar]
- Neri, A.; Stewart, S.L.; Angell, W. Peer reviewed: Radon control activities for lung cancer prevention in National Comprehensive Cancer Control Program plans, 2005–2011. Prev. Chronic Dis. 2013, 10, E132. [Google Scholar] [CrossRef] [Green Version]
- Sabbarese, C.; Ambrosino, F.; D’Onofrio, A. Development of radon transport model in different types of dwellings to assess indoor activity concentration. J. Environ. Radioact. 2021, 227, 106501. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.M.; Pearson, D.D.; Rönnqvist, T.; Nielsen, M.E.; Taron, J.M.; Goodarzi, A.A. Rising Canadian and falling Swedish radon gas exposure as a consequence of 20th to 21st century residential build practices. Sci. Rep. 2021, 11, 17551. [Google Scholar] [CrossRef] [PubMed]
- Elío, J.; Crowley, Q.; Scanlon, R.; Hodgson, J.; Zgaga, L. Estimation of residential radon exposure and definition of Radon Priority Areas based on expected lung cancer incidence. Environ. Int. 2018, 114, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Alvarellos, A.; Lopez Chao, A.; Rabuñal, J.R.; García-Vidaurrázaga, M.D.; Pazos, A. Development of an Automatic Low-Cost Air Quality Control System: A Radon Application. Appl. Sci. 2021, 11, 2169. [Google Scholar] [CrossRef]
- Lopes, S.I.; Moreira, P.M.; Cruz, A.M.; Martins, P.; Pereira, F.; Curado, A. RnMonitor: A WebGIS-based platform for expedite in situ deployment of IoT edge devices and effective Radon Risk Management. In Proceedings of the 2019 IEEE International Smart Cities Conference (ISC2), Casablanca, Morocco, 14–17 October 2019; pp. 451–457. [Google Scholar]
- Martins, P.; Lopes, S.I.; Pereira, F.; Curado, A. RnMonitor: An IoT-Enabled Platform for Radon Risk Management in Public Buildings. In Proceedings of the International Summit Smart City 360°, Braga, Portugal, 4–6 December 2019; pp. 49–55. [Google Scholar]
- Chen, J. Risk assessment for radon exposure in various indoor environments. Radiat. Prot. Dosim. 2019, 185, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Nero, A.V.; Nazaroff, W. Characterising the source of radon indoors. Radiat. Prot. Dosim. 1984, 7, 23–39. [Google Scholar] [CrossRef]
- Nazaroff, W.W. Radon transport from soil to air. Rev. Geophys. 1992, 30, 137–160. [Google Scholar] [CrossRef]
- Vaupotič, J. Search for radon sources in buildings—Kindergartens. J. Environ. Radioact. 2002, 61, 365–372. [Google Scholar] [CrossRef]
- Persily, A.K. Modeling Radon Transport in Multistory Residential Buildings; ASTM Special Technical Publication, ASTM: Philadelphia, PA, USA, 1993; pp. 226–242. [Google Scholar]
- Teiri, H.; Nazmara, S.; Abdolahnejad, A.; Hajizadeh, Y.; Amin, M.M. Indoor radon measurement in buildings of a university campus in central Iran and estimation of its effective dose and health risk assessment. J. Environ. Health Sci. Eng. 2021, 19, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Curado, A.; Silva, J.P.; Lopes, S.I. Radon risk assessment in a low-energy consumption school building: A dosimetric approach for effective risk management. Energy Rep. 2020, 6, 897–902. [Google Scholar] [CrossRef]
- Fuente, M.; Rábago, D.; Goggins, J.; Fuente, I.; Sainz, C.; Foley, M. Radon mitigation by soil depressurisation case study: Radon concentration and pressure field extension monitoring in a pilot house in Spain. Sci. Total Environ. 2019, 695, 133746. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.M.; Gomes, J.; Krewski, D.R. Radon interventions around the globe: A systematic review. Heliyon 2019, 5, e01737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-H.; Koh, S.-B.; Lee, C.-M.; Kim, C.; Kang, D.R. Indoor radon and lung cancer: Estimation of attributable risk, disease burden, and effects of mitigation. Yonsei Med. J. 2018, 59, 1123–1130. [Google Scholar] [CrossRef]
- Venoso, G.; Iacoponi, A.; Pratesi, G.; Guazzini, M.; Boccini, L.; Corbani, E.; Bucci, S.; Leonardi, F.; Trevisi, R.; Ampollini, M. Impact of temporal variability of radon concentration in workplaces on the actual radon exposure during working hours. Sci. Rep. 2021, 11, 16984. [Google Scholar] [CrossRef]
- Szajerski, P.; Zimny, A. Numerical analysis and modeling of two-loop experimental setup for measurements of radon diffusion rate through building and insulation materials. Environ. Pollut. 2020, 256, 113393. [Google Scholar] [CrossRef]
- Richter, M.; Horn, W.; Juritsch, E.; Klinge, A.; Radeljic, L.; Jann, O. Natural Building Materials for Interior Fitting and Refurbishment—What about Indoor Emissions? Materials 2021, 14, 234. [Google Scholar] [CrossRef]
- Levasseur, M.-E.; Poulin, P.; Campagna, C.; Leclerc, J.-M. Integrated management of residential indoor air quality: A call for stakeholders in a changing climate. Int. J. Environ. Res. Public Health 2017, 14, 1455. [Google Scholar] [CrossRef] [Green Version]
- D’Avino, V.; Pugliese, M.; Verde, G.L. Effectiveness of passive ventilation on radon indoor level in Puglia Region according to European Directive 2013/59/EURATOM. Indoor Built Environ. 2020, 30, 1580–1586. [Google Scholar] [CrossRef]
- Dovjak, M.; Virant, B.; Krainer, A.; Zavrl, M.Š.; Vaupotič, J. Determination of optimal ventilation rates in educational environment in terms of radon dosimetry. Int. J. Hyg. Environ. Health 2021, 234, 113742. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Moir, D.; Whyte, J. Canadian population risk of radon induced lung cancer: A re-assessment based on the recent cross-Canada radon survey. Radiat. Prot. Dosim. 2012, 152, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.; Aker, A.; Kim, J.; Li, Y.; Brand, K.; Copes, R. Lung cancer risk from radon in Ontario, Canada: How many lung cancers can we prevent? Cancer Causes Control 2013, 24, 2013–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simms, J.A.; Pearson, D.D.; Cholowsky, N.L.; Irvine, J.L.; Nielsen, M.E.; Jacques, W.R.; Taron, J.M.; Peters, C.E.; Carlson, L.E.; Goodarzi, A.A. Younger North Americans are exposed to more radon gas due to occupancy biases within the residential built environment. Sci. Rep. 2021, 11, 6724. [Google Scholar] [CrossRef]
- Barros-Dios, J.M.; Barreiro, M.A.; Ruano-Ravina, A.; Figueiras, A. Exposure to residential radon and lung cancer in Spain: A population-based case-control study. Am. J. Epidemiol. 2002, 156, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Ruano-Ravina, A.; Aragonés, N.; Pérez-Ríos, M.; López-Abente, G.; Barros-Dios, J.M. Residential radon exposure and esophageal cancer. An ecological study from an area with high indoor radon concentration (Galicia, Spain). Int. J. Radiat. Biol. 2014, 90, 299–305. [Google Scholar] [CrossRef]
- Barbosa-Lorenzo, R.; Barros-Dios, J.M.; Ruano-Ravina, A. Radon and stomach cancer. Int. J. Epidemiol. 2017, 46, 767–768. [Google Scholar] [CrossRef]
- Messier, K.P.; Serre, M.L. Lung and stomach cancer associations with groundwater radon in North Carolina, USA. Int. J. Epidemiol. 2017, 46, 676–685. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.-K.; Seo, S.; Jin, Y.W. Health effects of radon exposure. Yonsei Med. J. 2019, 60, 597–603. [Google Scholar] [CrossRef]
- Nagy, K.; Berhés, I.; Kovács, T.; Kávási, N.; Somlai, J.; Kovacs, L.; Barna, I.; Bender, T. Study on endocronological effects of radon speleotherapy on respiratory diseases. Int. J. Radiat. Biol. 2009, 85, 281–290. [Google Scholar] [CrossRef]
- Al-Zoughool, M.; Krewski, D. Health effects of radon: A review of the literature. Int. J. Radiat. Biol. 2009, 85, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Laurier, D.; Valenty, M.; Tirmarche, M. Radon exposure and the risk of leukemia: A review of epidemiological studies. Health Phys. 2001, 81, 272–288. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.P.; Lopes, N.; Curado, A.; Nunes, L.J.R.; Lopes, S.I. Designing a qualitative pre-diagnosis model for the evaluation of radon potential in indoor environments. In Proceedings of the ICEER 21—8th International Conference on Energy and Environment Research, Porto, Portugal, 13–17 September 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Keywords | Results (Nr. of Indexed Publications) |
|---|---|
| “Radon” + “lung cancer” | 2659 |
| “Radon risk assessment” | 835 |
| “Radon mitigation measures” | 155 |
| “Radiation effects on health” | 8423 |
| “Radon effects on the environment” | 339 |
| “Radon sources” | 3003 |
| “Radon mutagenic effects” | 30 |
| “Indoor radon potential” | 514 |
| “Radon detection equipment” | 28 |
| “Radon current developments” | 77 |
| “Radon induced diseases” | 70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, L.J.R.; Curado, A.; Graça, L.C.C.d.; Soares, S.; Lopes, S.I. Impacts of Indoor Radon on Health: A Comprehensive Review on Causes, Assessment and Remediation Strategies. Int. J. Environ. Res. Public Health 2022, 19, 3929. https://doi.org/10.3390/ijerph19073929
Nunes LJR, Curado A, Graça LCCd, Soares S, Lopes SI. Impacts of Indoor Radon on Health: A Comprehensive Review on Causes, Assessment and Remediation Strategies. International Journal of Environmental Research and Public Health. 2022; 19(7):3929. https://doi.org/10.3390/ijerph19073929
Chicago/Turabian StyleNunes, Leonel J. R., António Curado, Luís C. C. da Graça, Salete Soares, and Sérgio Ivan Lopes. 2022. "Impacts of Indoor Radon on Health: A Comprehensive Review on Causes, Assessment and Remediation Strategies" International Journal of Environmental Research and Public Health 19, no. 7: 3929. https://doi.org/10.3390/ijerph19073929