
Effectiveness of Smoking Prevention Programs on the Knowledge, Attitudes, and Anti-Smoking Exposure Self-Efficacy among Non-Smoking Rural Seventh-Grade Students in Taiwan


Abstract
:1. Introduction
Aim
- Improving the knowledge of the health risks of smoking and SHS exposure;
- Promoting more negative attitudes toward smoking and SHS exposure;
- Supporting anti-smoking and SHS exposure avoidance self-efficacy.
2. Materials and Methods
2.1. Study Design
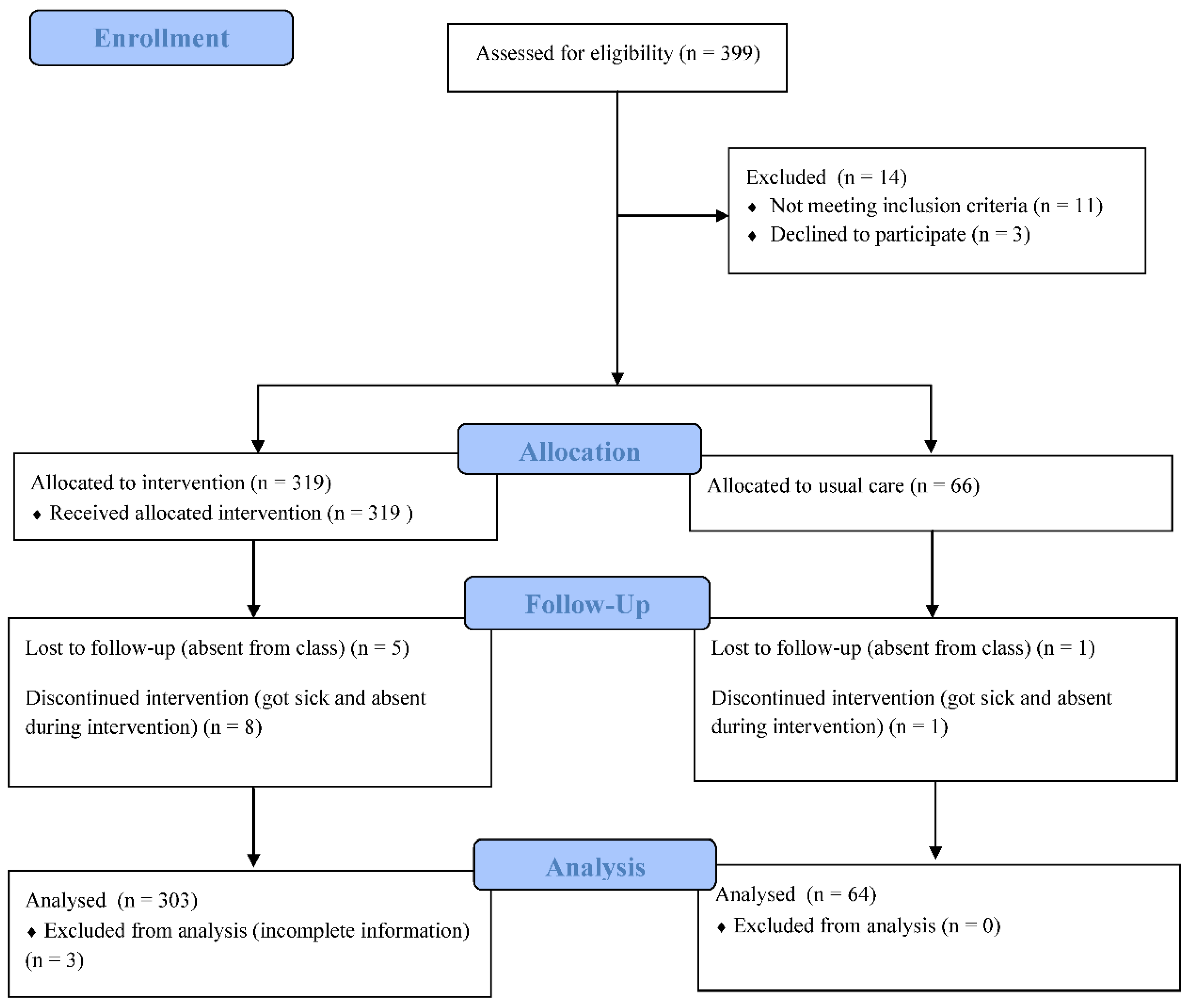
2.2. Participants
2.3. Intervention
2.4. Process of Research
2.5. Instruments
2.5.1. Background Characteristics
2.5.2. Knowledge of Smoking and SHS
2.5.3. Attitudes toward Cigarette Smoking and Avoiding SHS
2.5.4. Avoidance of SHS
2.5.5. Anti-Smoking Self-Efficacy and Self-Efficacy of SHS Avoidance
2.6. Statistical Analyses
3. Results
3.1. Participant Characteristics and Clinical Factors
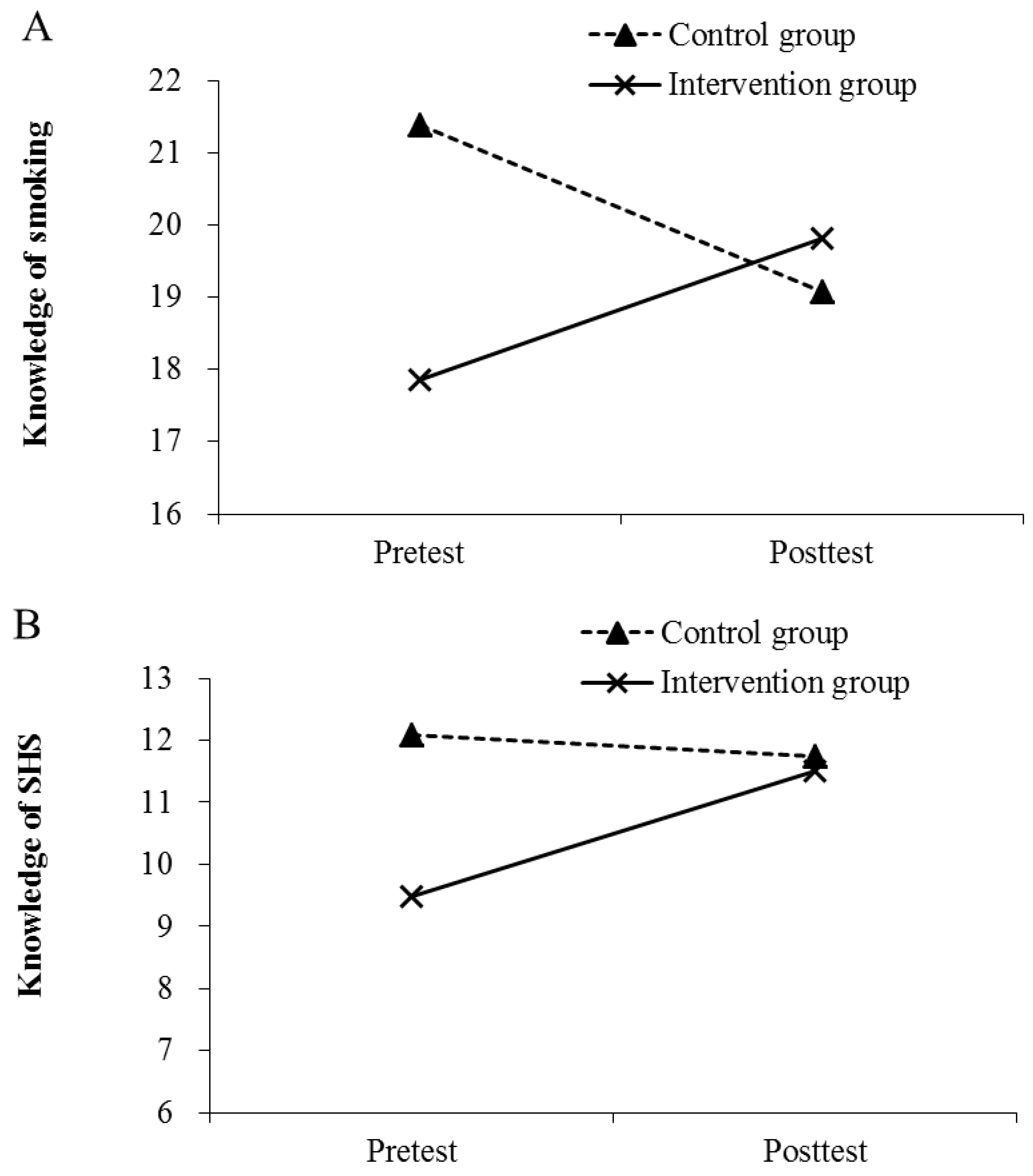
3.2. Changes in Knowledge of Smoking-Related Health Risks and SHS Exposure
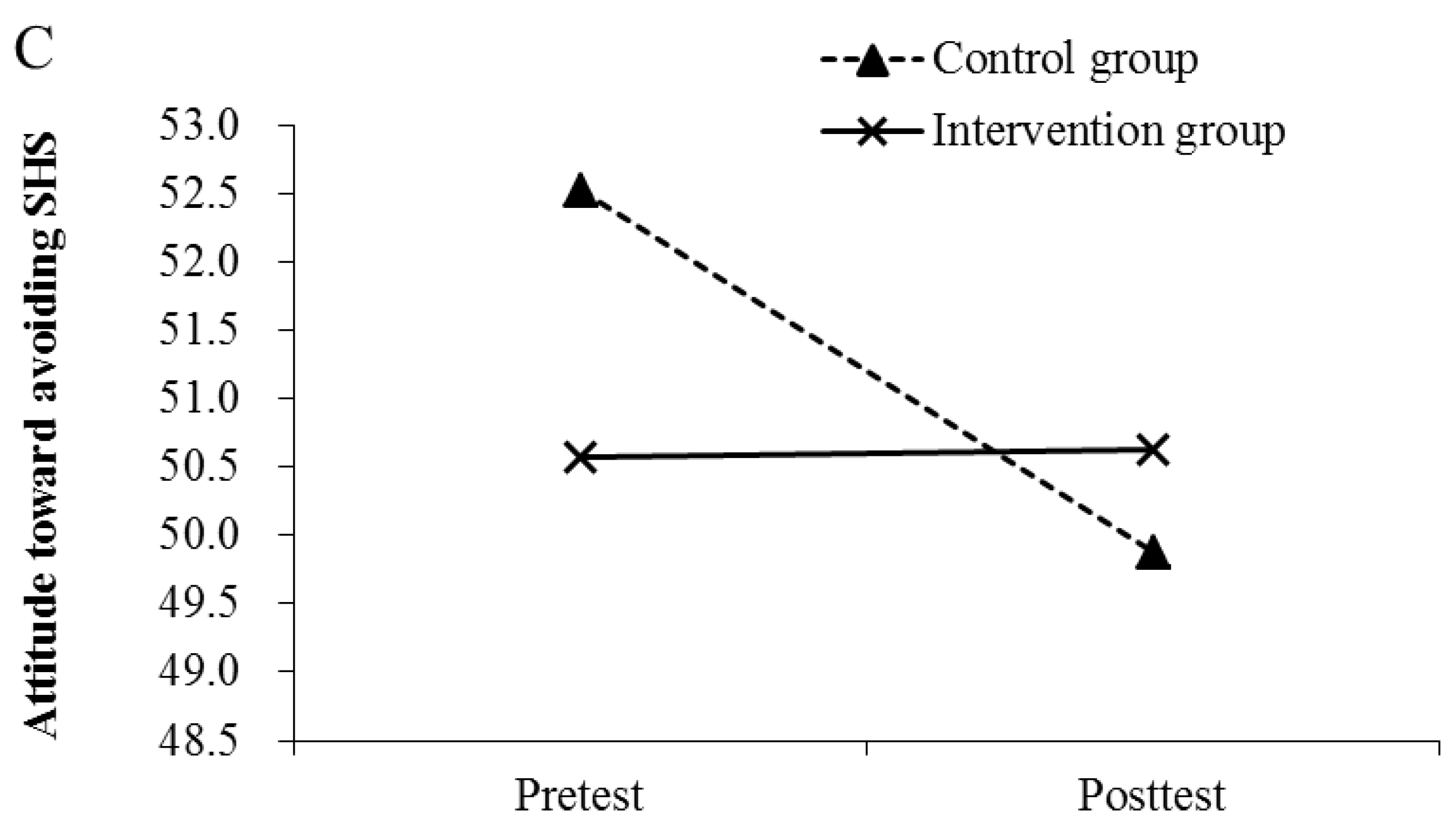
3.3. Changes in Attitudes toward Smoking and Avoiding SHS
3.4. Changes in Anti-Smoking and SHS Exposure Avoidance Self-Efficacy
4. Discussion
4.1. Effects of Smoking Prevention Programs on Knowledge and Attitudes
4.2. Effects of Smoking Prevention Programs on Anti-Smoking Exposure Self-Efficacy
4.3. Strengths and Limitations
4.4. Clinical Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maciosek, M.V.; Xu, X.; Butani, A.L.; Pechacek, T.F. Smoking-attributable medical expenditures by age, sex, and smoking status estimated using a relative risk approach. Prev. Med. 2015, 77, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health and Welfare. Adult Smoking Behavior Surveillance System, ASBS. Republic of China (Taiwan). Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1718&pid=9913 (accessed on 13 January 2022).
- Ministry of Health and Welfare. Global Youth Tobacco Survey (GYTS). Republic of China (Taiwan). Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=1489 (accessed on 13 January 2022).
- Ministry of Health and Welfare. Global Youth Tobacco Survey (GYTS) Survey Result. Republic of China (Taiwan). Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1725&pid=9931 (accessed on 17 January 2022).
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014. [Google Scholar]
- Veeranki, S.P.; Mamudu, H.M.; Zheng, S.; John, R.M.; Cao, Y.; Kioko, D.; Anderson, J.; Ouma, A.E.O. Secondhand smoke exposure among never-smoking youth in 168 countries. J. Adolesc. Health 2015, 56, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Okoli, C.T.; Kodet, J. A systematic review of secondhand tobacco smoke exposure and smoking behaviors: Smoking status, susceptibility, initiation, dependence, and cessation. Addict. Behav. 2015, 47, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Faber, T.; Kumar, A.; Mackenbach, J.P.; Millett, C.; Basu, S.; Sheikh, A.; Been, J.V. Effect of tobacco control policies on perinatal and child health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e420–e437. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Nadhiroh, S.R.; Djokosujono, K.; Utari, D.M. The association between secondhand smoke exposure and growth outcomes of children: A systematic literature review. Tob. Induc. Dis. 2020, 18, 12. [Google Scholar] [CrossRef]
- Shu, D.; Chen, F.; Zhang, C.; Guo, W.; Dai, S. Environmental tobacco smoke and carotid intima–media thickness in healthy children and adolescents: A systematic review. Open Heart 2022, 9, e001790. [Google Scholar] [CrossRef]
- Schwartz, J.; Graham, R.B.; Richardson, C.G.; Okoli, C.T.; Struik, L.L.; Bottorff, J.L. An examination of exposure and avoidance behavior related to second-hand cigarette smoke among adolescent girls in Canada. BMC Public Health 2014, 14, 468. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.E.; Chen, M.Y.; Chiang, Y.F.; Lin, M.S. Cigarette smoking behavior and the related factors for adolescents on one junior high school in coastal rural area, Western Taiwan. Chin. J. Sch. Health 2016, 69, 21–42. [Google Scholar]
- Huang, C.M.; Yen, Y.Y.; Chen, F.L.; Hsu, C.C.; Lee, C.H.; Lin, Y.; Huang, H.L. School-level policy for tobacco control and individual-level characteristics in relation to cigarette smoking among children: A multilevel study of elementary schools in Pingtung County. Taiwan J. Public Health 2010, 29, 145–158. [Google Scholar]
- Lim, K.H.; Ghazali, S.M.; Lim, H.L.; Cheong, K.C.; Teh, C.H.; Lim, K.K.; Heng, P.P.; Cheah, Y.K.; Lim, J.H. Smoking susceptibility among non-smoking school-going adolescents in Malaysia: Findings from a national school-based survey. BMJ Open 2019, 9, e031164. [Google Scholar] [CrossRef]
- Stigler, M.H.; Perry, C.L.; Arora, M.; Shrivastav, R.; Mathur, C.; Reddy, K.S. Intermediate outcomes from Project MYTRI: Mobilizing youth for tobacco-related initiatives in India. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1050–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, X.; Li, L.; Griffiths, S.M.; Gao, Y.; Lau, J.F.; Mo, P.H. Smoking behaviors and intentions among adolescents in rural China: The application of the Theory of Planned Behavior and the role of social influence. Addict. Behav. 2015, 48, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, H.; Unger, J.B.; Chou, C.; Sun, P.; Palmer, P.H.; Zhou, Y.; Yao, J.; Xie, B.; Gallaher, P.E.; Guo, Q.; et al. Risk factors for adolescent smoking in urban and rural China: Findings from the China seven cities study. Addict. Behav. 2008, 33, 1081–1085. [Google Scholar] [CrossRef]
- Giannotta, F.; Vigna-Taglianti, F.; Galanti, M.R.; Scatigna, M.; Faggiano, F. Short-term mediating factors of a school-based intervention to prevent youth substance use in Europe. J. Adolesc. Health 2014, 54, 565–573. [Google Scholar] [CrossRef]
- Isensee, B.; Hansen, J.; Maruska, K.; Hanewinkel, R. Effects of a school-based prevention programme on smoking in early adolescence: A 6-month follow-up of the ‘Eigenständig werden’ cluster randomised trial. BMJ Open 2014, 4, e004422. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Wang, M.; Zhong, J.M.; Fang, L.; Wang, H. Prevalence and associated factors of smoking in middle and high school students: A school-based cross-sectional study in Zhejiang Province, China. BMJ Open 2016, 6, e010379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, M.A.; Zare, Z.; Ng, K.W.; Celedonia, K.L.; Lowery Wilson, M. Tobacco Use and Parental Monitoring—Observations from Three Diverse Island Nations—Cook Islands, Curaçao, and East Timor. Int. J. Environ. Res. Public Health 2020, 17, 7360. [Google Scholar] [CrossRef]
- Wu, T.S.; Chaffee, B.W. Parental awareness of youth tobacco use and the role of household tobacco rules in use prevention. Pediatrics 2020, 146, e20194034. [Google Scholar] [CrossRef]
- Kao, Y.T. Compare the Effectiveness of Three Smoking Prevention Programs: An example of 7th Grade Students in a Junior High School in Taipei County. Master’s Thesis, National Taiwan Normal University, Taipei, Taiwan, 2002. [Google Scholar]
- Liao, H.J. Study on the Effects of a Smoking Prevention Program among the Junior High School Students in Taipei City. Master’s Thesis, National Taiwan Normal University, Taipei, Taiwan, 2006. [Google Scholar]
- Shi, J.; Mo, X.; Sun, Z. Content Validity Index in Scale Development. J. Cent. South Univ. Med. Sci. 2012, 37, 152–155. [Google Scholar]
- Kurtz, M.E.; Azikiwe, U.; Kurtz, J.C. Nigerian urban married women’s perceptions of exposure to secondary tobacco smoke. Health Care Women Int. 1993, 14, 239–248. [Google Scholar] [CrossRef]
- Wang, W.L.; Wang, C.J.; Tung, Y.Y.; Peng, J.H. Factors influencing adolescent second-hand smoke avoidance behavior from the perspective of pender’s health promotion model. J. Evid. Based Nurs. 2007, 3, 280–288. [Google Scholar]
- Tseng, S.C. The Related Factors for Smoking Behavior of Junior High School Students: Take a Junior High School in Taoyuan County as an Example. Master’s Thesis, National Taiwan Normal University, Taipei, Taiwan, 2011. [Google Scholar]
- Li, M.F.; Wang, R.H. Factors related to avoidance of environmental tobacco smoke among adolescents in southern Taiwan. J. Nurs. Res. 2006, 14, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, A.M. Testing a model of avoiding environmental tobacco smoke in young adults. J. Nurs. Scholarsh. 1999, 31, 237–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, A.M.; Agazio, J.; Flaherty, N.; Ephraim, P.M. Testing a model of exposure to environmental tobacco smoke in military women with children. Mil. Med. 2002, 167, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nor Afiah, M.Z.; Suriani, I.; Rohaiza Aida, H.F.; Muhamad Syahir Asyraf, A.R. Knowledge, attitude and perceptions on second hand smoke (SHS) exposure among undergraduate students contribute to avoidance of second hand smoke. Int. J. Public Health Clin. Sci. 2017, 4, 53–65. [Google Scholar]
- Lin, P.L.; Huang, H.L.; Lu, K.Y.; Chen, T.; Lin, W.T.; Lee, C.H.; Hsu, H.M. Second-hand smoke exposure and the factors associated with avoidance behavior among the mothers of pre-school children: A school-based cross-sectional study. BMC Public Health 2010, 10, 606. [Google Scholar] [CrossRef] [Green Version]
- Tahlil, T.; Woodman, R.J.; Coveney, J.; Ward, P.R. Six-months follow-up of a cluster randomized trial of school-based smoking prevention education programs in Aceh, Indonesia. BMC Public Health 2015, 15, 1088. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Wu, D.M.; Lai, H.R.; Chu, N.F. The impacts of a school-wide no smoking strategy and classroom-based smoking prevention curriculum on the smoking behavior of junior high school students. Addict. Behav. 2007, 32, 2099–2107. [Google Scholar] [CrossRef]
- Flay, B. The promise of long-term effectiveness of school-based smoking prevention programs: A critical review of reviews. Tob. Induc. Dis. 2009, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Yeh, S.H.; Tseng, H.F.; Yang, S.F. Smoking behavior and its associated factors among teenagers in Kaohsiung City. J. Healthc. Adm. 2005, 1, 76–86. [Google Scholar] [CrossRef]
- Chen, L.; Chen, Y.; Hao, Y.; Gu, J.; Guo, Y.; Ling, W. Effectiveness of school-based smoking intervention in middle school students of Linzhi Tibetan and Guangzhou Han ethnicity in China. Addict. Behav. 2014, 39, 189–195. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Topic | Contents | Material/Teaching Methods | Time |
|---|---|---|---|
| Information about cigarette smoking and its Health risks | History of tobacco Cigarettes components Health risks of cigarette smoking Smoking rates of Taiwan adolescents | PowerPoint Videos/Group discussion and feedback | 50 min |
| Media awareness | Increase awareness of message delivered by media and cigarette advertising Tobacco Hazards Prevention Act | PowerPoint Learning sheets Videos/Discussion and feedback | 50 min |
| Stress and coping & decision making skills | Dealing with pressure from peers and adults Improve the understanding of the decision-making process Learning refusal skills and resisting temptation to smoke | Power Point Learning sheets Video/Discussion and feedback | 50 min |
| Smoke-free environments | Strengthening anti-smoking attitudes Strengthening the advantage of smoke-free environment Learning to create smoke-free environment | Power Point Learning sheets Video/Discussion and feedback | 50 min |
| Variable | Control, n(%) | Experimental, n(%) | χ2 (p Value)/t Test (p Value) |
|---|---|---|---|
| 64 (17.4) | 303 (82.6) | ||
| Sociodemographic and background factors | |||
| Sex | 0.02 (0.86) | ||
| Female | 32 (50.0) | 148 (49.0) | |
| Male | 32 (50.0) | 154 (51.0) | |
| Mother’s education level | 4.40 (0.04) * | ||
| High school | 33 (51.6) | 192 (65.5) | |
| Less than high school | 31 (48.4) | 101 (34.5) | |
| Father’s education level | 1.38 (0.24) | ||
| High school | 29 (45.3) | 157 (53.4) | |
| Less than high school | 35 (54.7) | 137 (46.6) | |
| Perceived family economy status (compared to his/her peers) | 1.59 (0.45) | ||
| rich | 16 (25.8) | 77 (25.6) | |
| the same | 29 (46.8) | 162 (53.8) | |
| poor | 17 (27.4) | 62 (20.6) | |
| Academic achievement/academic performance # | 1.53 (0.47) | ||
| high | 23 (35.9) | 113 (39.0) | |
| Medium | 27 (42.2) | 132 (45.5) | |
| Low | 14 (21.9) | 45 (15.5) | |
| Perceived health (compared to his/her peers) | 7.99 (0.02) * | ||
| Good | 33 (52.4) | 101 (33.6) | |
| the same | 19 (30.2) | 122 (40.5) | |
| Poor | 11 (17.5) | 78 (25.9) | |
| Social influences and environmental factors | |||
| Parental disapproval of adolescent smoking | 0.08 (0.78) | ||
| strongly disapprove | 58 (90.6) | 271 (89.4) | |
| Disapprove | 6 (9.4) | 32 (10.6) | |
| approve | 0 | 0 | |
| Age (Mean ± SD) ※ | 12.59 ± 0.29 | 12.60 ± 0.30 | −0.31 (0.76) |
| the number of smoking family (Mean ± SD) ※ | 1.11 ± 0.91 | 0.95 ± 0.94 | 1.26 (0.21) |
| Exercise in school (Mean ± SD) ※ | 3.39 ± 1.94 | 3.24 ± 1.74 | 0.60 (0.55) |
| Exercise out school (Mean ± SD) ※ | 3.61 ± 2.13 | 3.53 ± 2.02 | 0.27 (0.79) |
| Variable | Control (n = 64) | t-Test | Experimental (n = 303) | t-Test | ||
|---|---|---|---|---|---|---|
| Pretest | Posttest | t | Pretest | Posttest | t | |
| Knowledge of smoking | 21.4 ± 3.2 | 19.1 ± 5.8 | −3.53 ** | 17.9 ± 5.7 | 19.8 ± 5.4 | 6.73 *** |
| Knowledge of SHS | 12.1 ± 3.0 | 11.7 ± 3.7 | −0.84 | 9.5 ± 4.3 | 11.5 ± 3.8 | 8.3 *** |
| Attitudes toward cigarette smoking | 57.5 ± 9.6 | 55.9 ± 9.6 | −1.05 | 56.8 ± 7.2 | 56.5 ± 7.2 | −0.66 |
| Attitude toward avoiding SHS | 52.5 ± 7.9 | 49.9 ± 9.6 | −2.27 * | 50.6 ± 8.9 | 50.6 ± 8.2 | 0.28 |
| Avoidance of SHS | 28.7 ± 4.9 | 27.9 ± 4.4 | −1.54 | 28.6 ± 4.7 | 28.4 ± 4.5 | −0.28 |
| Anti-smoking self-efficacy | 140.7 ± 21.6 | 132.4 ± 24.9 | −3.76 *** | 137.8 ± 28.5 | 133.9 ± 28.6 | −2.02 * |
| Self-efficacy of avoiding SHS | 52.2 ± 12.1 | 50.8 ± 11.1 | −0.92 | 50.3 ± 14.1 | 50.7 ± 11.7 | 0.37 |
| Parameter | Knowledge of Smoking | Knowledge of SHS | Attitudes toward Cigarette Smoking | Attitude toward Avoiding SHS | Avoidance of SHS | Anti-Smoking Self-Efficacy | Self-Efficacy of Avoiding SHS | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | p | B | p | B | p | B | p | B | p | B | p | B | p | |
| Intercept | 21.36 *** | <0.001 | 12.10 *** | <0.001 | 56.50 *** | <0.001 | 51.58 *** | <0.001 | 28.21 *** | <0.001 | 134.21 *** | <0.001 | 50.58 *** | <0.001 |
| Time | ||||||||||||||
| Posttest vs. Pretest | −2.40 *** | <0.001 | −0.37 | 0.416 | −1.68 | 0.295 | −2.92 * | 0.023 | −1.03 | 0.084 | −8.79 *** | <0.001 | −1.25 | 0.475 |
| Group | ||||||||||||||
| Exp. vs. Con. | −3.70 *** | <0.001 | −2.59 *** | <0.001 | −0.41 | 0.758 | −1.66 | 0.153 | 0.01 | 0.985 | −2.28 | 0.472 | −0.47 | 0.785 |
| Interaction | ||||||||||||||
| Group × Time | 4.38 *** | <0.001 | 2.35 *** | <0.001 | 1.35 | 0.420 | 3.03 * | 0.031 | 0.82 | 0.213 | 4.82 | 0.091 | 1.44 | 0.467 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, S.-E.; Chen, M.-Y.; Okoli, C.; Chiang, Y.-F. Effectiveness of Smoking Prevention Programs on the Knowledge, Attitudes, and Anti-Smoking Exposure Self-Efficacy among Non-Smoking Rural Seventh-Grade Students in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 9767. https://doi.org/10.3390/ijerph19159767
Guo S-E, Chen M-Y, Okoli C, Chiang Y-F. Effectiveness of Smoking Prevention Programs on the Knowledge, Attitudes, and Anti-Smoking Exposure Self-Efficacy among Non-Smoking Rural Seventh-Grade Students in Taiwan. International Journal of Environmental Research and Public Health. 2022; 19(15):9767. https://doi.org/10.3390/ijerph19159767
Chicago/Turabian StyleGuo, Su-Er, Mei-Yen Chen, Chizimuzo Okoli, and Yi-Fan Chiang. 2022. "Effectiveness of Smoking Prevention Programs on the Knowledge, Attitudes, and Anti-Smoking Exposure Self-Efficacy among Non-Smoking Rural Seventh-Grade Students in Taiwan" International Journal of Environmental Research and Public Health 19, no. 15: 9767. https://doi.org/10.3390/ijerph19159767