

Computed Tomography Angiography Markers and Intraluminal Thrombus Morphology as Predictors of Abdominal Aortic Aneurysm Rupture
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
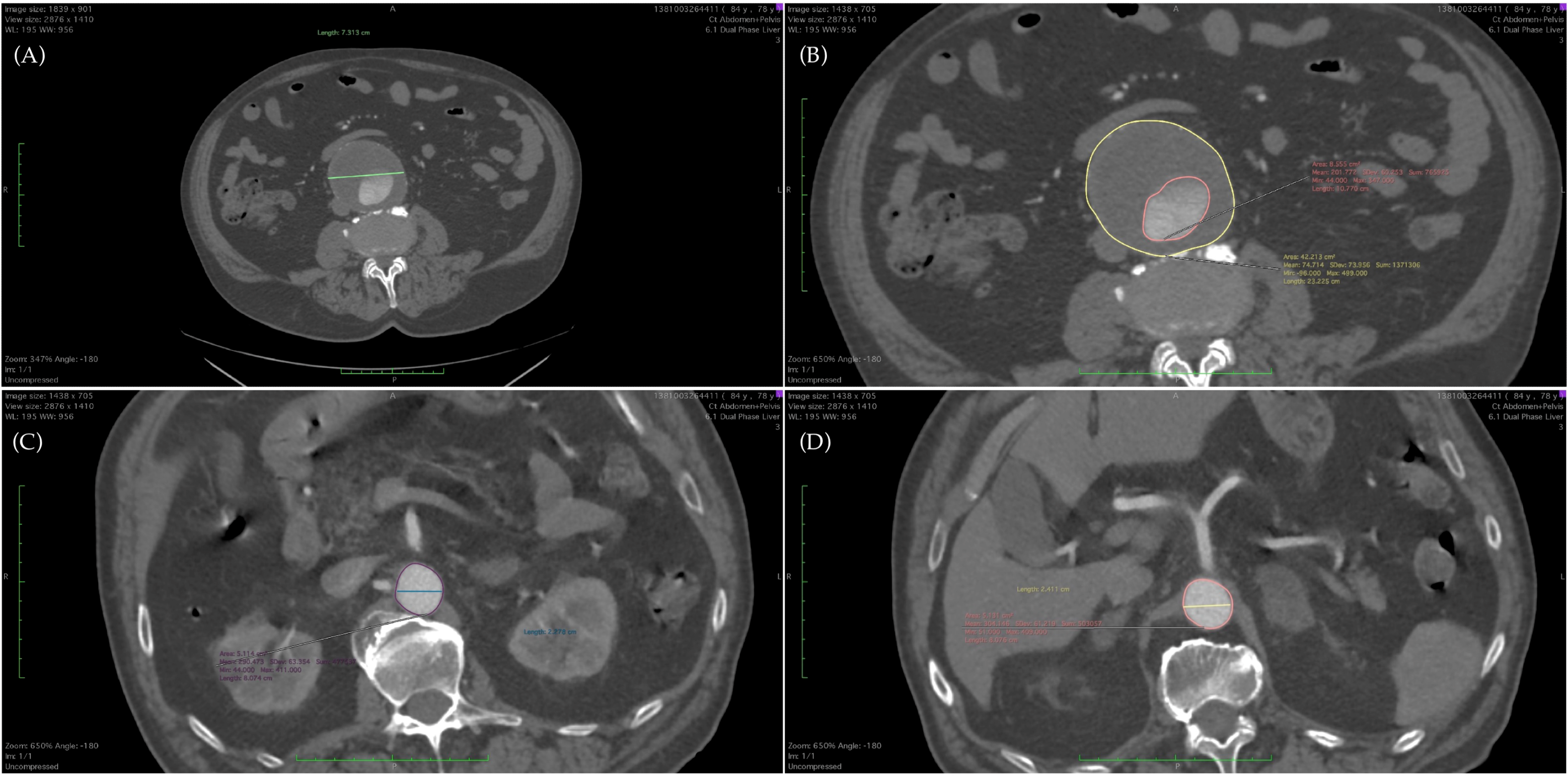
2.3. CTA Markers
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, L.J.; Prabhakar, A.M.; Kwolek, C.J. Current Status of the Treatment of Infrarenal Abdominal Aortic Aneurysms. Cardiovasc. Diagn. Ther. 2018, 8, S191–S199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuivaniemi, H.; Elmore, J.R. Opportunities in Abdominal Aortic Aneurysm Research: Epidemiology, Genetics, and Pathophysiology. Ann. Vasc. Surg. 2012, 26, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Arbănași, E.-M.; Russu, E.; Mureșan, A.V.; Arbănași, E.-M. Late Rupture of a Thrombosed Aortic Abdominal Aneurysm—A Case Report. J. Cardiovasc. Emergencies 2021, 7, 84–87. [Google Scholar] [CrossRef]
- Russu, E.; Mureșan, A.V.; Kaller, R.; Toma, L.; Coșarcă, C.M.; Chibelean, C.B.; Arbănași, E.M.; Arbănași, E.M. Innovative Technical Solution Using the Renal Artery Stump after Nephrectomy as an Inflow Artery for Lower Limb Revascularization—A Case Report. Front. Surg. 2022, 9, 864846. [Google Scholar] [CrossRef] [PubMed]
- Kaller, R.; Mureșan, A.V.; Popa, D.G.; Arbănași, E.-M.; Russu, E. Fatal Aortoduodenal Fistula Caused by a Ruptured Abdominal Aortic Aneurysm—A Case Report. J. Cardiovasc. Emergencies 2021, 7, 129–132. [Google Scholar] [CrossRef]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E.; Gordon, I.L.; Chute, E.P.; Littooy, F.N.; Krupski, W.C.; Bandyk, D.; Barone, G.W.; Graham, L.M.; et al. Relationship of Age, Gender, Race, and Body Size to Infrarenal Aortic Diameter. The Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Investigators. J. Vasc. Surg. 1997, 26, 595–601. [Google Scholar] [CrossRef] [Green Version]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E. Abdominal Aortic Aneurysm in Women. J. Vasc. Surg. 2001, 34, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery Practice Guidelines on the Care of Patients with an Abdominal Aortic Aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Ashton, H.A.; Gao, L.; Buxton, M.J.; Scott, R.A.P.; on behalf of the Multicentre Aneurysm Screening Study (MASS) Group. Final Follow-up of the Multicentre Aneurysm Screening Study (MASS) Randomized Trial of Abdominal Aortic Aneurysm Screening. Br. J. Surg. 2012, 99, 1649–1656. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.M.; Zelt, D.T.; Sobolev, B. The Risk of Rupture in Untreated Aneurysms: The Impact of Size, Gender, and Expansion Rate. J. Vasc. Surg. 2003, 37, 280–284. [Google Scholar] [CrossRef]
- Hatakeyama, T.; Shigematsu, H.; Muto, T. Risk Factors for Rupture of Abdominal Aortic Aneurysm Based on Three-Dimensional Study. J. Vasc. Surg. 2001, 33, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E.; Ballard, D.J.; Jordan, W.D.; Blebea, J.; Littooy, F.N.; Freischlag, J.A.; Bandyk, D.; Rapp, J.H.; et al. Rupture Rate of Large Abdominal Aortic Aneurysms in Patients Refusing or Unfit for Elective Repair. JAMA 2002, 287, 2968–2972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.C.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 Practice Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic). Circulation 2006, 113, e463–e654. [Google Scholar] [CrossRef] [Green Version]
- Khosla, S.; Morris, D.R.; Moxon, J.V.; Walker, P.J.; Gasser, T.C.; Golledge, J. Meta-Analysis of Peak Wall Stress in Ruptured, Symptomatic and Intact Abdominal Aortic Aneurysms. Br. J. Surg. 2014, 101, 1350–1357; discussion 1357. [Google Scholar] [CrossRef] [PubMed]
- Indrakusuma, R.; Jalalzadeh, H.; Planken, R.N.; Marquering, H.A.; Legemate, D.A.; Koelemay, M.J.W.; Balm, R. Biomechanical Imaging Markers as Predictors of Abdominal Aortic Aneurysm Growth or Rupture: A Systematic Review. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2016, 52, 475–486. [Google Scholar] [CrossRef] [Green Version]
- Chung, T.K.; Gueldner, P.H.; Kickliter, T.M.; Liang, N.L.; Vorp, D.A. An Objective and Repeatable Sac Isolation Technique for Comparing Biomechanical Metrics in Abdominal Aortic Aneurysms. Bioengineering 2022, 9, 601. [Google Scholar] [CrossRef]
- Murali Krishna, S.; Morton, S.K.; Li, J.; Golledge, J. Risk Factors and Mouse Models of Abdominal Aortic Aneurysm Rupture. Int. J. Mol. Sci. 2020, 21, 7250. [Google Scholar] [CrossRef]
- Singh, T.P.; Moxon, J.V.; Gasser, T.C.; Golledge, J. Systematic Review and Meta-Analysis of Peak Wall Stress and Peak Wall Rupture Index in Ruptured and Asymptomatic Intact Abdominal Aortic Aneurysms. J. Am. Heart Assoc. 2021, 10, e019772. [Google Scholar] [CrossRef]
- Metaxa, E.; Tzirakis, K.; Kontopodis, N.; Ioannou, C.V.; Papaharilaou, Y. Correlation of Intraluminal Thrombus Deposition, Biomechanics, and Hemodynamics with Surface Growth and Rupture in Abdominal Aortic Aneurysm—Application in a Clinical Paradigm. Ann. Vasc. Surg. 2018, 46, 357–366. [Google Scholar] [CrossRef]
- Manenti, A.; Farinetti, A.; Manco, G.; Mattioli, A.V. Intraluminal Thrombus and Abdominal Aortic Aneurysm Complications. Ann. Vasc. Surg. 2022, 83, e11–e12. [Google Scholar] [CrossRef]
- Polzer, S.; Gasser, T.C.; Vlachovský, R.; Kubíček, L.; Lambert, L.; Man, V.; Novák, K.; Slažanský, M.; Burša, J.; Staffa, R. Biomechanical Indices Are More Sensitive than Diameter in Predicting Rupture of Asymptomatic Abdominal Aortic Aneurysms. J. Vasc. Surg. 2020, 71, 617–626.e6. [Google Scholar] [CrossRef] [PubMed]
- Jusko, M.; Kasprzak, P.; Majos, A.; Kuczmik, W. The Ratio of the Size of the Abdominal Aortic Aneurysm to That of the Unchanged Aorta as a Risk Factor for Its Rupture. Biomedicines 2022, 10, 1997. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H.M.; Keenan, P.S.; Brush, J.E.; Bufalino, V.J.; Chernew, M.E.; Epstein, A.J.; Heidenreich, P.A.; Ho, V.; Masoudi, F.A.; Matchar, D.B.; et al. Standards for Measures Used for Public Reporting of Efficiency in Health Care: A Scientific Statement from the American Heart Association Interdisciplinary Council on Quality of Care and Outcomes Research and the American College of Cardiology Foundation. J. Am. Coll. Cardiol. 2008, 52, 1518–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makrygiannis, G.; Labalue, P.; Erpicum, M.; Schlitz, M.; Seidel, L.; El Hachemi, M.; Gangolf, M.; Albert, A.; Defraigne, J.-O.; Lindholt, J.S.; et al. Extending Abdominal Aortic Aneurysm Detection to Older Age Groups: Preliminary Results from the Liège Screening Programme. Ann. Vasc. Surg. 2016, 36, 55–63. [Google Scholar] [CrossRef]
- Global Burden of Disease (GBD 2019). Available online: https://www.healthdata.org/gbd/2019 (accessed on 4 November 2022).
- Kniemeyer, H.W.; Kessler, T.; Reber, P.U.; Ris, H.B.; Hakki, H.; Widmer, M.K. Treatment of Ruptured Abdominal Aortic Aneurysm, a Permanent Challenge or a Waste of Resources? Prediction of Outcome Using a Multi-Organ-Dysfunction Score. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2000, 19, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Gianfagna, F.; Veronesi, G.; Tozzi, M.; Tarallo, A.; Borchini, R.; Ferrario, M.M.; Bertù, L.; Montonati, A.; Castelli, P.; RoCAV (Risk of Cardiovascular diseases and abdominal aortic Aneurysm in Varese). Project Investigators Prevalence of Abdominal Aortic Aneurysms in the General Population and in Subgroups at High Cardiovascular Risk in Italy. Results of the RoCAV Population Based Study. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2018, 55, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Bohlin, S.; Fröjd, C.; Wanhainen, A.; Björck, M. Change in Smoking Habits after Having Been Screened for Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2014, 48, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Zhang, K.; Li, T.; Zhai, S. Primary Results of Abdominal Aortic Aneurysm Screening in the At-Risk Residents in Middle China. BMC Cardiovasc. Disord. 2018, 18, 60. [Google Scholar] [CrossRef] [Green Version]
- Svensjö, S.; Björck, M.; Gürtelschmid, M.; Djavani Gidlund, K.; Hellberg, A.; Wanhainen, A. Low Prevalence of Abdominal Aortic Aneurysm among 65-Year-Old Swedish Men Indicates a Change in the Epidemiology of the Disease. Circulation 2011, 124, 1118–1123. [Google Scholar] [CrossRef] [Green Version]
- Smith, F.C.; Grimshaw, G.M.; Paterson, I.S.; Shearman, C.P.; Hamer, J.D. Ultrasonographic Screening for Abdominal Aortic Aneurysm in an Urban Community. Br. J. Surg. 1993, 80, 1406–1409. [Google Scholar] [CrossRef]
- Takei, H.; Ishikawa, S.; Otaki, A.; Sakata, K.; Aizaki, M.; Sato, Y.; Suzuki, M.; Ishikita, T.; Iino, Y.; Yokoe, T.; et al. Screening for Abdominal Aortic Aneurysm and Occlusive Peripheral Vascular Disease in Japanese Residents. Surg. Today 1995, 25, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Al Zahrani, H.A.; Rawas, M.; Maimani, A.; Gasab, M.; Al Khail, B.A. Screening for Abdominal Aortic Aneurysm in the Jeddah Area, Western Saudi Arabia. Cardiovasc. Surg. 1996, 4, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, E.; Rapacchietta, L.; Profeta, V.F.; Fagnano, R. Risk Factors for Abdominal Aortic Aneurysm in Population-Based Studies: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2018, 15, 2805. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.H.J.; Makaroun, M.S.; Webster, M.W.; Vorp, D.A. Effect of Intraluminal Thrombus on Wall Stress in Patient-Specific Models of Abdominal Aortic Aneurysm. J. Vasc. Surg. 2002, 36, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Inzoli, F.; Boschetti, F.; Zappa, M.; Longo, T.; Fumero, R. Biomechanical Factors in Abdominal Aortic Aneurysm Rupture. Eur. J. Vasc. Surg. 1993, 7, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Mower, W.R.; Quiñones, W.J.; Gambhir, S.S. Effect of Intraluminal Thrombus on Abdominal Aortic Aneurysm Wall Stress. J. Vasc. Surg. 1997, 26, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Martino, E.; Mantero, S.; Inzoli, F.; Melissano, G.; Astore, D.; Chiesa, R.; Fumero, R. Biomechanics of Abdominal Aortic Aneurysm in the Presence of Endoluminal Thrombus: Experimental Characterisation and Structural Static Computational Analysis. Eur. J. Vasc. Endovasc. Surg. 1998, 15, 290–299. [Google Scholar] [CrossRef] [Green Version]
- Vorp, D.A.; Lee, P.C.; Wang, D.H.J.; Makaroun, M.S.; Nemoto, E.M.; Ogawa, S.; Webster, M.W. Association of Intraluminal Thrombus in Abdominal Aortic Aneurysm with Local Hypoxia and Wall Weakening. J. Vasc. Surg. 2001, 34, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Dobrin, P.B. Pathophysiology and Pathogenesis of Aortic Aneurysms: Current Concepts. Surg. Clin. N. Am. 1989, 69, 687–703. [Google Scholar] [CrossRef]
- Schurink, G.W.H.; van Baalen, J.M.; Visser, M.J.T.; van Bockel, J.H. Thrombus within an Aortic Aneurysm Does Not Reduce Pressure on the Aneurysmal Wall. J. Vasc. Surg. 2000, 31, 501–506. [Google Scholar] [CrossRef]
- Zhu, C.; Leach, J.R.; Wang, Y.; Gasper, W.; Saloner, D.; Hope, M.D. Intraluminal Thrombus Predicts Rapid Growth of Abdominal Aortic Aneurysms. Radiology 2020, 294, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Kontopodis, N.; Koncar, I.; Tzirakis, K.; Tavlas, E.; Davidovic, L.; Ioannou, C.V. Intraluminal Thrombus Deposition Is Reduced in Ruptured Compared to Diameter-Matched Intact Abdominal Aortic Aneurysms. Ann. Vasc. Surg. 2019, 55, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Shan, Y.; Zhou, M.; Cai, L.; Li, X.; Shi, Z.; Fu, W. Amount of Intraluminal Thrombus Correlates with Severe Adverse Events in Abdominal Aortic Aneurysms after Endovascular Aneurysm Repair. Ann. Vasc. Surg. 2020, 67, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.J. Intraluminal Thrombus: Innocent Bystander or Factor in Abdominal Aortic Aneurysm Pathogenesis? JVS Vasc. Sci. 2021, 2, 159–169. [Google Scholar] [CrossRef]
- Powell, J.T.; Brown, L.C.; Forbes, J.F.; Fowkes, F.G.R.; Greenhalgh, R.M.; Ruckley, C.V.; Thompson, S.G. Final 12-Year Follow-up of Surgery versus Surveillance in the UK Small Aneurysm Trial. Br. J. Surg. 2007, 94, 702–708. [Google Scholar] [CrossRef]
- Lederle, F.A.; Wilson, S.E.; Johnson, G.R.; Reinke, D.B.; Littooy, F.N.; Acher, C.W.; Ballard, D.J.; Messina, L.M.; Gordon, I.L.; Chute, E.P.; et al. Immediate Repair Compared with Surveillance of Small Abdominal Aortic Aneurysms. N. Engl. J. Med. 2002, 346, 1437–1444. [Google Scholar] [CrossRef]
- Parkinson, F.; Ferguson, S.; Lewis, P.; Williams, I.M.; Twine, C.P. South East Wales Vascular Network Rupture Rates of Untreated Large Abdominal Aortic Aneurysms in Patients Unfit for Elective Repair. J. Vasc. Surg. 2015, 61, 1606–1612. [Google Scholar] [CrossRef] [Green Version]
- Wołoszko, T.; Skórski, M.; Kwasiborski, P.; Kmin, E.; Gałązka, Z.; Pogorzelski, R. Influence of Selective Biochemical and Morphological Agents on Natural History of Aneurysm of Abdominal Aorta Development. Med. Sci. Monit. 2016, 22, 431–437. [Google Scholar] [CrossRef] [Green Version]
- Behr-Andersen, C.; Gammelgaard, L.; Fründ, E.T.; Dahl, M.; Lindholt, J.S. Magnetic Resonance Imaging of the Intraluminal Thrombus in Abdominal Aortic Aneurysms: A Quantitative and Qualitative Evaluation and Correlation with Growth Rate. J. Cardiovasc. Surg. 2019, 60, 221–229. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Dweck, M.R.; McBride, O.M.B.; Vesey, A.T.; Semple, S.I.; Shah, A.S.V.; Adamson, P.D.; Wallace, W.A.; Kaczynski, J.; Ho, W.; et al. 18F–Sodium Fluoride Uptake in Abdominal Aortic Aneurysms: The SoFIA3 Study. J. Am. Coll. Cardiol. 2018, 71, 513–523. [Google Scholar] [CrossRef]
- MA3RS Study Investigators Aortic Wall Inflammation Predicts Abdominal Aortic Aneurysm Expansion, Rupture, and Need for Surgical Repair. Circulation 2017, 136, 787–797. [CrossRef] [PubMed]
- Nyrønning, L.Å.; Skoog, P.; Videm, V.; Mattsson, E. Is the Aortic Size Index Relevant as a Predictor of Abdominal Aortic Aneurysm? A Population-Based Prospective Study: The Tromsø Study. Scand. Cardiovasc. J. SCJ 2020, 54, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Tzirakis, K.; Kontopodis, N.; Metaxa, E.; Ioannou, C.V.; Papaharilaou, Y. Spatial Distribution of Abdominal Aortic Aneurysm Surface Expansion and Correlation with Maximum Diameter and Volume Growth. Ann. Vasc. Surg. 2019, 58, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Nakaura, T.; Nakagawa, M.; Kidoh, M.; Oda, S.; Utsunomiya, D.; Yamashita, Y. Machine Learning to Predict the Rapid Growth of Small Abdominal Aortic Aneurysm. J. Comput. Assist. Tomogr. 2020, 44, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Verzini, F.; Herzeele, I.V.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choksy, S.A.; Wilmink, A.B.; Quick, C.R. Ruptured Abdominal Aortic Aneurysm in the Huntingdon District: A 10-Year Experience. Ann. R. Coll. Surg. Engl. 1999, 81, 27–31. [Google Scholar]
- Hall, A.J.; Busse, E.F.; McCarville, D.J.; Burgess, J.J. Aortic Wall Tension as a Predictive Factor for Abdominal Aortic Aneurysm Rupture: Improving the Selection of Patients for Abdominal Aortic Aneurysm Repair. Ann. Vasc. Surg. 2000, 14, 152–157. [Google Scholar] [CrossRef]
- Siika, A.; Lindquist Liljeqvist, M.; Hultgren, R.; Gasser, T.C.; Roy, J. Aortic Lumen Area Is Increased in Ruptured Abdominal Aortic Aneurysms and Correlates to Biomechanical Rupture Risk. J. Endovasc. Ther. 2018, 25, 750–756. [Google Scholar] [CrossRef]
- Fillinger, M.F.; Marra, S.P.; Raghavan, M.L.; Kennedy, F.E. Prediction of Rupture Risk in Abdominal Aortic Aneurysm during Observation: Wall Stress versus Diameter. J. Vasc. Surg. 2003, 37, 724–732. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, E.S.; Bohra, A.; Vande Geest, J.P.; Gupta, N.; Makaroun, M.S.; Vorp, D.A. Biomechanical Properties of Ruptured versus Electively Repaired Abdominal Aortic Aneurysm Wall Tissue. J. Vasc. Surg. 2006, 43, 570–576; discussion 576. [Google Scholar] [CrossRef] [Green Version]
- Kimura, M.; Hoshina, K.; Miyahara, K.; Nitta, J.; Kobayashi, M.; Yamamoto, S.; Ohshima, M. Geometric Analysis of Ruptured and Nonruptured Abdominal Aortic Aneurysms. J. Vasc. Surg. 2019, 69, 86–91. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Markers | Definition |
|---|---|
| DAmax | maximum diameter of the AAA |
| DArenal | diameter of the aorta at renal level |
| DACT | diameter of the aorta at celiac trunk level |
| DAfemoral | diameter of the femoral artery |
| SAmax | surface of the AAA at maximum diameter |
| SArenal | surface of the aorta at renal level |
| SACT | surface of the aorta at celiac trunk level |
| SAfemoral | surface of the femoral artery |
| SLumenmax | surface of the lumen at maximum diameter of the AAA |
| SThrombusmax | surface of the thrombus at maximum diameter of the AAA |
| DAmax/Arenal | |
| DAmax/ACT | |
| SAmax/Arenal | |
| SAmax/ACT | |
| SAmax/Lumenmax | |
| SLumenmax/Thrombusmax |
| Variables | All Patients n = 220 | uAAA n = 173 | rAAA n = 47 | p Value (OR; CI 95%) |
|---|---|---|---|---|
| Age mean ± SD (min–max) | 71.68 ± 9.78 (47–95) | 71.58 ± 10.13 (47–95) | 72.06 ± 8.44 (55–88) | 0.74 |
| Male/Female sex no. (%) | 123 (55.91%) 97 (44.09%) | 95 (54.91%) 78 (45.09%) | 28 (59.57%) 19 (40.43%) | 0.14 (1.45; 0.87–2.42) |
| Comorbidities and Risk factors, no. (%) | ||||
| AH, no. (%) | 175 (79.54%) | 134 (77.45%) | 41 (87.23%) | 0.006 (2.30; 1.26–4.19) |
| IHD, no. (%) | 159 (72.27%) | 120 (69.36%) | 39 (82.97%) | 0.001 (2.32; 1.38–3.89) |
| AF, no. (%) | 62 (28.18%) | 48 (27.74%) | 14 (29.78%) | <0.0001 (3.23; 1.90–5.48) |
| CHF, no. (%) | 73 (33.18%) | 57 (32.94%) | 16 (34.04%) | 0.77 (1.09; 0.60–1.98) |
| MI, no. (%) | 44 (20%) | 27 (15.6%) | 17 (36.17%) | <0.0001 (3.16; 1.83–5.44) |
| DM, no. (%) | 66 (30%) | 52 (30.05%) | 14 (29.78%) | 0.25 (1.37; 0.79–2.35) |
| CKD, no. (%) | 33 (15%) | 25 (14.45%) | 8 (17.02%) | 0.74 (1.11; 0.58–2.10) |
| COPD, no. (%) | 24 (10.9%) | 17 (9.82%) | 7 (14.89%) | 0.74 (1.11; 0.58–2.10) |
| PAD, no. (%) | 103 (46.81%) | 71 (41.04%) | 32 (68.08%) | 0.64 (1.14; 0.63–2.06) |
| CVA, no. (%) | 64 (29.09%) | 46 (26.58%) | 18 (38.29%) | 0.74 (1.11; 0.58–2.10) |
| Tobacco, no. (%) | 58 (26.36%) | 41 (23.69%) | 17 (36.17%) | 0.001 (2.55; 1.46–4.46) |
| Obesity, no. (%) | 50 (22.72%) | 31 (17.91%) | 19 (40.42%) | 0.02 (1.90; 1.10–3.28) |
| Dyslipidemia, no. (%) | 39 (17.72%) | 30 (17.34%) | 9 (19.14%) | <0.0001 (5.27; 3.07–9.02) |
| Computed Tomography Angiography Markers, median [Q1–Q3] | ||||
| DAmax | 6.75 [5.71–8.15] | 6.42 [5.64–8.1] | 7.63 [6.31–8.41] | 0.003 |
| DArenal | 2.15 [1.64–2.50] | 2.26 [1.88–2.56] | 1.59 [1.27–2.04] | <0.0001 |
| DACT | 2.38 [1.83–2.86] | 2.56 [2.13–2.95] | 1.78 [1.53–2.04] | <0.0001 |
| DAfemoral | 0.93 [0.78–1.12] | 0.95 [0.80–1.13] | 0.84 [0.72–0.98] | 0.005 |
| SAmax | 53.7 [39.51–74.26] | 48.3 [36.01–69.94] | 75.73 [57.83–91.78] | <0.0001 |
| SArenal | 4.95 [3.89–5.91] | 5.29 [4.34–6.31] | 3.89 [3.53–4.79] | <0.0001 |
| SACT | 5.33 [4.44–6.69] | 5.55 [4.69–6.95] | 4.59 [4.01–5.42] | <0.0001 |
| SAfemoral | 1.19 [0.87–1.61] | 1.24 [0.89–1.59] | 1.15 [0.81–1.98] | 0.12 |
| SLumenmax | 28.98 [13.01–44.77] | 23.47 [10.42 = 35.31] | 55.31 [42.79–65.64] | <0.0001 |
| SThrombusmax | 21.81 [13.38–34.23] | 22.9 [14.21–34.42] | 16.41 [11.72–29.09] | 0.052 |
| DAmax/Arenal | 3.29 [2.49–4.37] | 3.04 [2.34–3.92] | 4.60 [3.86–5.41] | <0.0001 |
| DAmax/ACT | 2.92 [2.26–3.97] | 2.71 [2.03–3.39] | 4.29 [3.45–5.15] | <0.0001 |
| DAmax/Afemoral | 7.40 [5.83–9.06] | 7.10 [5.46–8.81] | 8.81 [6.89–10.36] | 0.01 |
| SAmax/Arenal | 10.65 [7.47–16.12] | 8.89 [7.03–12.98] | 18.9 [15.9–21.05] | <0.0001 |
| SAmax/ACT | 9.41 [6.8–14.66] | 7.79 [6.38–12.02] | 15.6 [12.89–20.76] | <0.0001 |
| SAmax/Afemoral | 42.44 [26.79–72.19] | 38.61 [25.73–57.67] | 82.22 [32.17–106.3] | <0.0001 |
| SAmax/Lumenmax | 1.72 [1.35–2.89] | 2.06 [1.49–3.89] | 1.32 [1.20–1.56] | <0.0001 |
| SAmax/Thrombusmax | 2.37 [1.52–3.80] | 1.94 [1.34–3.007] | 4.04 [2.75–5.89] | <0.0001 |
| SLumenmax/Thrombusmax | 1.37 [0.52–2.80] | 0.94 [0.34–2.007] | 3.04 [1.75–4.89] | <0.0001 |
| Intraluminal Thrombus Morphology, no. (%) | ||||
| Posterior-Eccentric | 77 (35%) | 61 (35.26%) | 16 (34.04%) | 0.87 (0.94; 0.48–1.86) |
| Anterior-Eccentric | 49 (22.27%) | 31 (17.92%) | 18 (38.3%) | 0.003 (2.84; 1.40–5.75) |
| Lateral-Eccentric | 62 (28.18%) | 49 (28.32%) | 13 (27.66%) | 0.92 (0.96; 0.47–1.98) |
| Concentric | 32 (14.55%) | 30 (17.34%) | 2 (4.26%) | 0.03 (0.21; 0.04–0.92) |
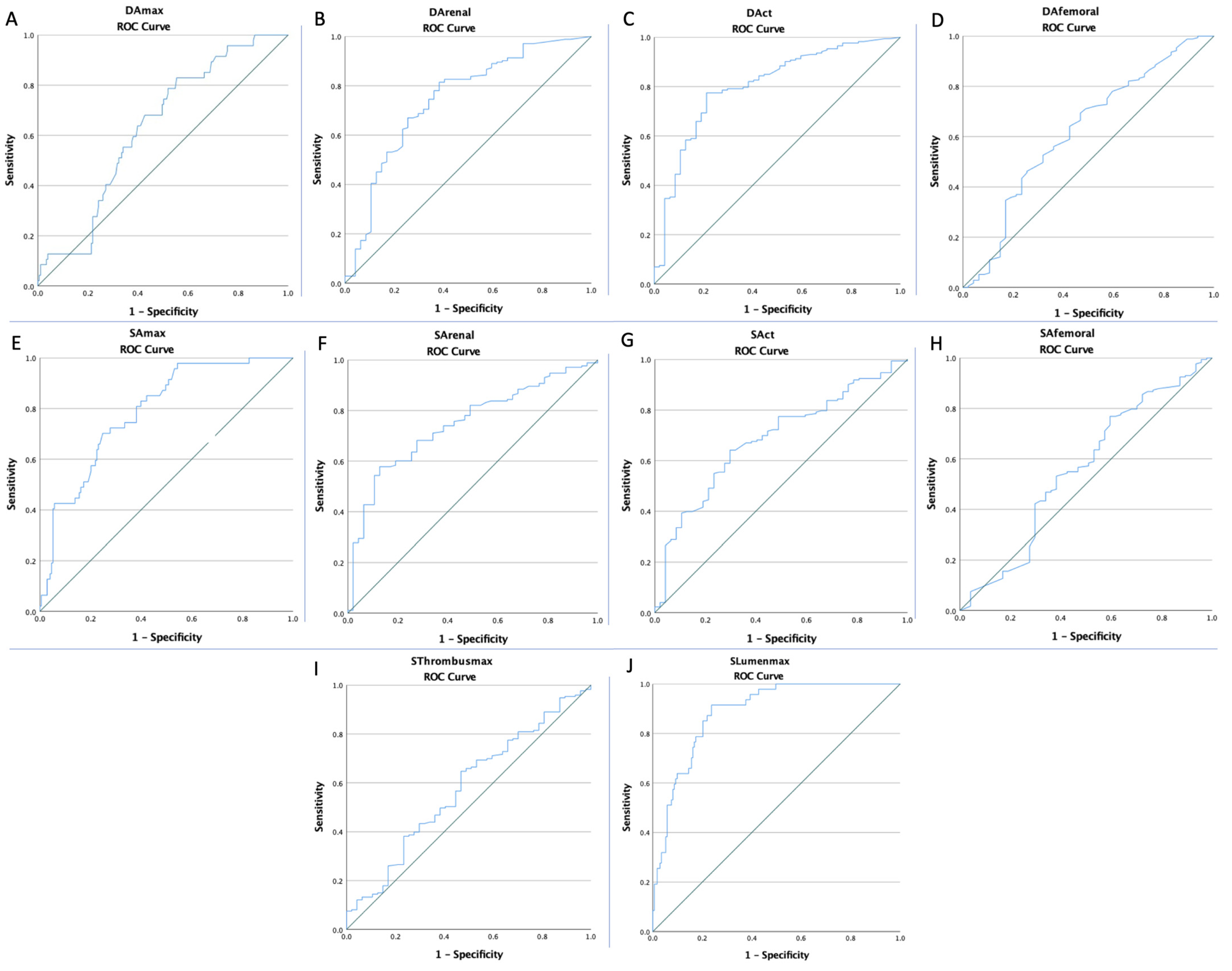
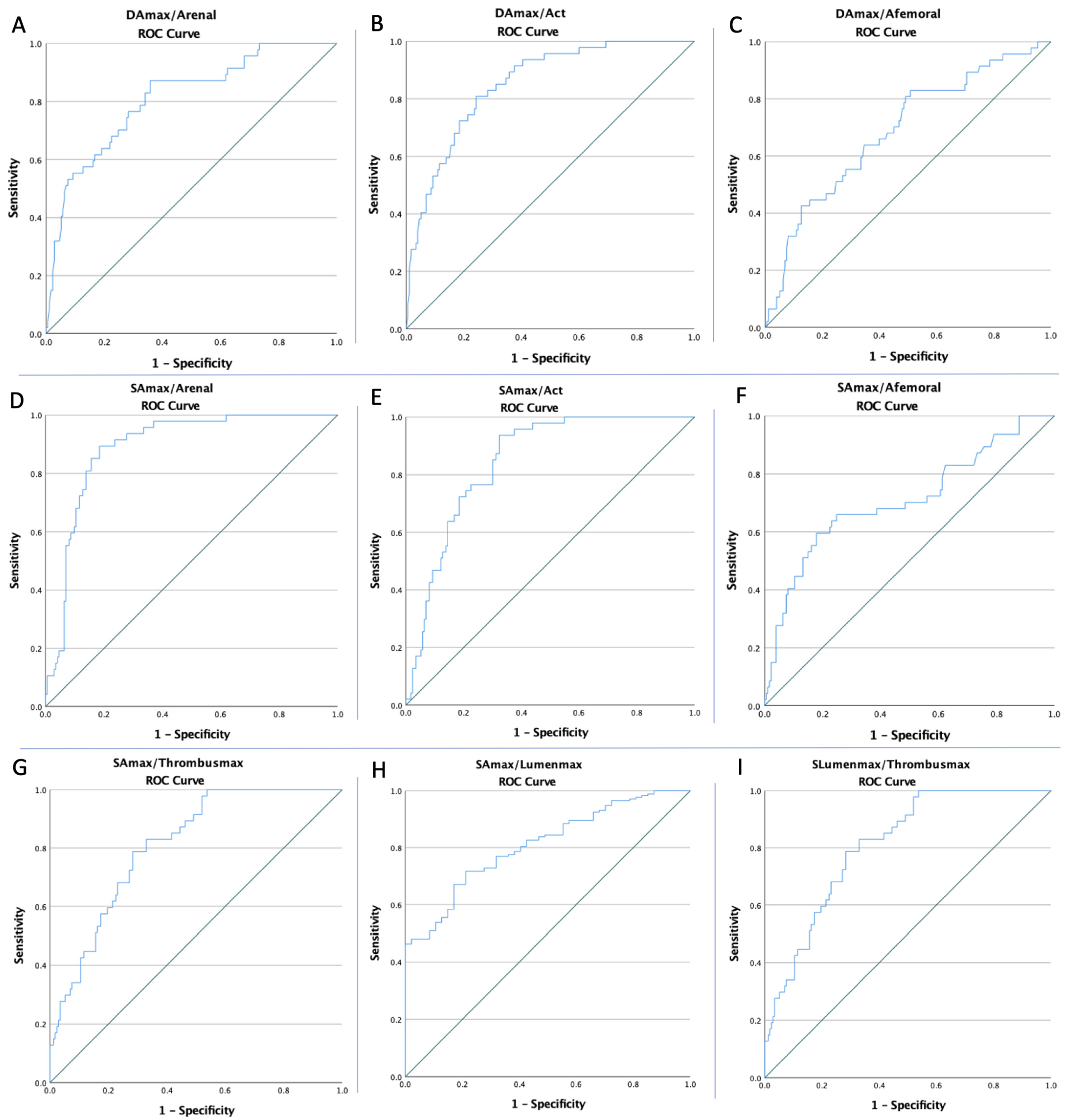
| Variables | Cut-Off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p Value |
|---|---|---|---|---|---|---|---|
| AAA Rupture | |||||||
| DAmax | 6.11 | 0.630 | 0.041 | 0.549–0.711 | 83% | 44.5% | 0.006 |
| DArenal | 1.73 | 0.744 | 0.043 | 0.660–0.828 | 81.5% | 61.7% | <0.0001 |
| DACT | 2.08 | 0.802 | 0.037 | 0.730–0.875 | 77.5% | 78.7% | <0.0001 |
| DAFemoral | 0.84 | 0.620 | 0.049 | 0.524–0.716 | 71.1% | 51.1% | 0.01 |
| SAmax | 65.16 | 0.789 | 0.034 | 0.723–0.856 | 70.2% | 75.1% | <0.0001 |
| SArenal | 4.72 | 0.746 | 0.037 | 0.673–0.819 | 63.6% | 72.3% | <0.0001 |
| SACT | 5.09 | 0.684 | 0.042 | 0.603–0.766 | 64.2% | 68.1% | <0.0001 |
| SAfemoral | 0.91 | 0.556 | 0.051 | 0.457–0.655 | 73.4% | 40.4% | 0.24 |
| SLumenmax | 35.94 | 0.887 | 0.023 | 0.842–0.932 | 91.5% | 76.3% | <0.0001 |
| SThrombusmax | 17.48 | 0.577 | 0.047 | 0.485–0.669 | 64.7% | 51.1% | 0.10 |
| DAmax/Arenal | 3.27 | 0.810 | 0.036 | 0.740–0.880 | 87.2% | 64.2% | <0.0001 |
| DAmax/ACT | 3.07 | 0.850 | 0.029 | 0.794–0.907 | 80.9% | 75.7% | <0.0001 |
| DAmax/Afemoral | 6.78 | 0.687 | 0.044 | 0.600–0.773 | 83% | 49.1% | <0.0001 |
| SAmax/Arenal | 14.27 | 0.890 | 0.023 | 0.844–0.935 | 89.4% | 81.5% | <0.0001 |
| SAmax/ACT | 9.85 | 0.846 | 0.027 | 0.793–0.898 | 93.6% | 67.6% | <0.0001 |
| SAmax/Afemoral | 58.19 | 0.709 | 0.047 | 0.618–0.800 | 66% | 75.1% | <0.0001 |
| SAmax/Lumenmax | 1.57 | 0.809 | 0.031 | 0.749–0.870 | 71.7% | 78.7% | <0.0001 |
| SAmax/Thrombusmax | 2.75 | 0.809 | 0.031 | 0.749–0.870 | 78.7% | 71.7% | <0.0001 |
| SLumenmax/Thrombusmax | 1.75 | 0.809 | 0.031 | 0.749–0.870 | 78.7% | 71.7% | <0.0001 |
| rAAA | rAAA | ||
|---|---|---|---|
| Low-DAmax vs. High-DAmax | 14/144 (9.72%) vs. 33/76 (43.42%) p < 0.0001 | Low-DAmax/Arenal vs. High-DAmax/Arenal | 6/117 (5.13%) vs. 41/103 (39.81%) p < 0.0001 |
| High-DArenal vs. Low-DArenal | 18/159 (11.32%) vs. 29/61 (47.5%) p < 0.0001 | Low-DAmax/ACT vs. High-DAmax/ACT | 3/120 (2.5%) vs. 44/100 (44%) p < 0.0001 |
| High-DACT vs. Low-DACT | 10/144 (6.94%) vs. 37/76 (48.68%) p < 0.0001 | Low-DAmax/AFemoral vs. High-DAmax/AFemoral | 3/120 (2.5%) vs. 44/100 (44%) p < 0.0001 |
| Low-DAFemoral vs. High-DAFemoral | 23/146 (15.7%) vs. 24/74 (32.43%) p = 0.005 | Low-SAmax/Arenal vs. High-SAmax/Arenal | 10/134 (7.46%) vs. 37/86 (43.02%) p < 0.0001 |
| Low-SAmax vs. High-SAmax | 14/144 (9.72%) vs. 33/76 (43.42%) p < 0.0001 | Low-SAmax/ACT vs. High-SAmax/ACT | 3/120 (2.5%) vs. 44/100 (44%) p < 0.0001 |
| High-SArenal vs. Low-SArenal | 13/123 (10.5%) vs. 34/97 (35.05%) p < 0.0001 | Low-SAmax/AFemoral vs. High-SAmax/AFemoral | 16/146 (10.96%) vs. 31/74 (41.9%) p < 0.0001 |
| Low-SACT vs. High-SACT | 3/120 (2.5%) vs. 44/100 (44%) p < 0.0001 | Low-SAmax/SLumenmax vs. High-SAmax/SLumenmax | 35/84 (41.67%) vs. 12/136 (8.82%) p < 0.0001 |
| Low-SLumenmax vs. High-SLumenmax | 4/136 (2.94%) vs. 43/84 (51.19%) p < 0.0001 | Low-SLumenmax/Thrombusmax vs. High-SLumenmax/Thrombusmax | 10/134 (7.46%) vs. 37/86 (43.02%) p < 0.0001 |
| Low-SAmax/Thrombusmax vs. High-SAmax/Thrombusmax | 10/134 (7.46%) vs. 37/86 (43.02%) p < 0.0001 | ||
| rAAA | |||
|---|---|---|---|
| Variables | OR | 95% CI | p Value |
| Comorbidities and Risk Factors | |||
| AH | 3.33 | 1.13–9.86 | 0.02 |
| MI | 3.06 | 1.48–6.31 | 0.002 |
| PAD | 2.71 | 1.38–5.33 | 0.004 |
| Tobacco | 1.41 | 0.70–2.86 | 0.33 |
| Obesity | 0.52 | 0.22–1.26 | 0.15 |
| Intraluminal Thrombus Morphology | |||
| Anterior-Eccentric | 2.84 | 1.40–5.75 | 0.004 |
| Concentric | 0.21 | 0.04–0.92 | 0.03 |
| Computed Tomography Angiography Markers | |||
| High-DAmax | 3.91 | 1.72–8.85 | 0.001 |
| Low-DArenal | 7.09 | 3.51–14.32 | <0.001 |
| Low-DACT | 12.71 | 5.80–27.85 | <0.001 |
| Low-DAfemoral | 2.56 | 1.32–4.95 | 0.005 |
| High-SAmax | 7.12 | 3.49–14.55 | <0.001 |
| Low-SArenal | 4.56 | 2.24–9.29 | <0.001 |
| Low-SACT | 3.81 | 1.92–7.59 | <0.001 |
| High-SLumenmax | 34.61 | 11.72–102.20 | <0.001 |
| Low-SThrombusmax | 5.27 | 3.07–9.02 | <0.001 |
| High-DAmax/Arenal | 12.23 | 4.91–30.43 | <0.001 |
| High-DAmax/ACT | 11.93 | 5.03–28.32 | <0.001 |
| High-DAmax/Afemoral | 4.60 | 2.03–10.41 | <0.001 |
| High-SAmax/Arenal | 37.01 | 13.56–100.96 | <0.001 |
| High-SAmax/ACT | 30.64 | 9.11–102.97 | <0.001 |
| High-SAmax/Afemoral | 5.85 | 2.92–11.73 | <0.001 |
| High-SAmax/Lumenmax | 0.13 | 0.06–0.28 | <0.001 |
| High-SAmax/Thrombusmax | 9.36 | 4.32–20.28 | <0.001 |
| High-SLumenmax/Thrombusmax | 9.36 | 4.32–20.28 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbănași, E.M.; Mureșan, A.V.; Coșarcă, C.M.; Arbănași, E.M.; Niculescu, R.; Voidăzan, S.T.; Ivănescu, A.D.; Hălmaciu, I.; Filep, R.C.; Mărginean, L.; et al. Computed Tomography Angiography Markers and Intraluminal Thrombus Morphology as Predictors of Abdominal Aortic Aneurysm Rupture. Int. J. Environ. Res. Public Health 2022, 19, 15961. https://doi.org/10.3390/ijerph192315961
Arbănași EM, Mureșan AV, Coșarcă CM, Arbănași EM, Niculescu R, Voidăzan ST, Ivănescu AD, Hălmaciu I, Filep RC, Mărginean L, et al. Computed Tomography Angiography Markers and Intraluminal Thrombus Morphology as Predictors of Abdominal Aortic Aneurysm Rupture. International Journal of Environmental Research and Public Health. 2022; 19(23):15961. https://doi.org/10.3390/ijerph192315961
Chicago/Turabian StyleArbănași, Emil Marian, Adrian Vasile Mureșan, Cătălin Mircea Coșarcă, Eliza Mihaela Arbănași, Raluca Niculescu, Septimiu Toader Voidăzan, Adrian Dumitru Ivănescu, Ioana Hălmaciu, Rareș Cristian Filep, Lucian Mărginean, and et al. 2022. "Computed Tomography Angiography Markers and Intraluminal Thrombus Morphology as Predictors of Abdominal Aortic Aneurysm Rupture" International Journal of Environmental Research and Public Health 19, no. 23: 15961. https://doi.org/10.3390/ijerph192315961