

Stimulation of the Vascular Endothelium and Angiogenesis by Blood-Flow-Restricted Exercise
 , , and
, , and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. BFR Exercise and Control Training Protocols
2.3. Endothelial Parameters Measurements
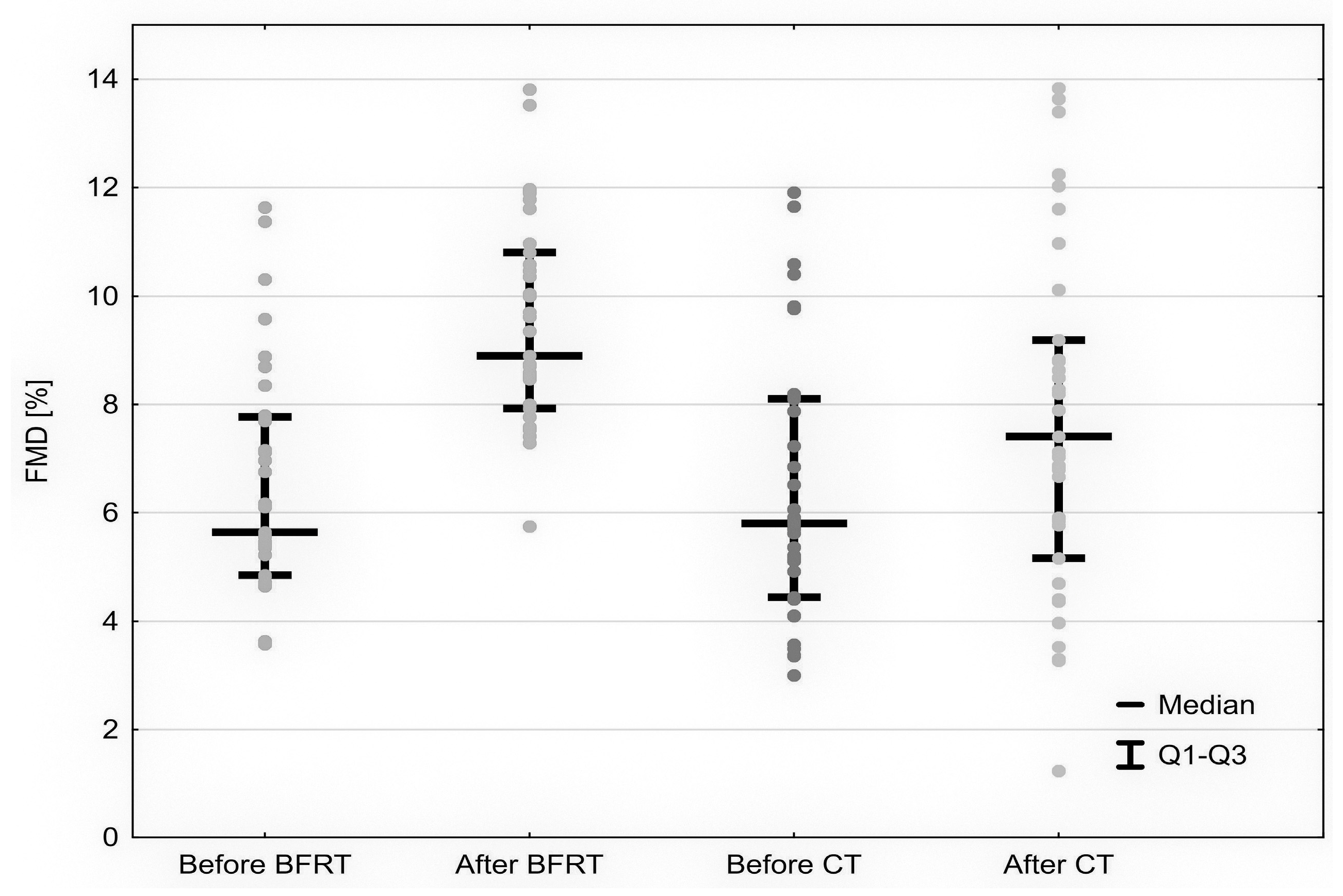
- FMD: Current guidelines for the ultrasound assessment of FMD were used in the study [20]. Before the test, the participants were resting in a supine position. FMD was measured with the Siemens Acuson S2000;
- RHI: Reactive hyperemia index (RHI) was measured using Peripheral Arterial Tone (PAT) analysis on Itamar Medical Endo-PAT 2000 device to assess digital pulse volume changes. The digital pulse amplitude was recorded continuously during the test and recorded on a laptop. A computerized algorithm provided by Itamar Medical was used to analyze and automatically calculate the RHI;
- aPWA: Arterial pulse waveform analysis (aPWA) was performed by recording 20 peripheral pressure waveforms from the radial artery at the wrist using applanation tonometry with a high-fidelity micro manometer, followed by generating the corresponding central aortic pressure waveform. The arterial stiffness evaluation enabled a commercially available SphygmoCor system (AtCor Medical). Stiffness index (SI), reflection index (RI), and corrected augmentation index (AI75) were measured to assess large, medium-sized, and small arterial stiffness variables.
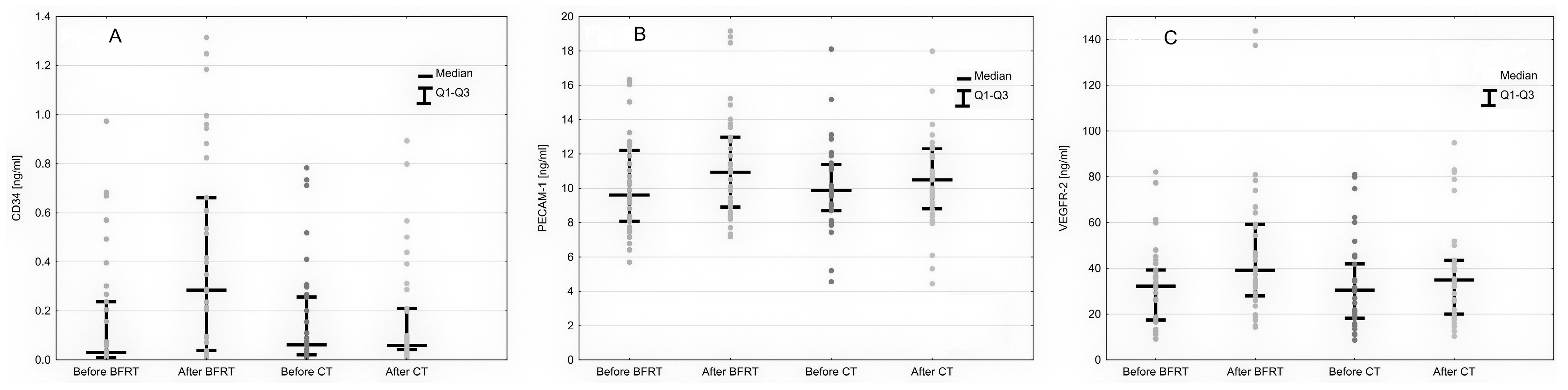
2.4. Angiogenesis Assessment
2.5. Statistical Analysis
2.6. Ethical Aspects
3. Results
3.1. Participant Population
3.2. Endothelial Response to BFR Exercise
3.3. Angiogenesis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lorenz, D.S.; Bailey, L.; Wilk, K.E.; Mangine, R.E.; Head, P.; Grindstaff, T.L.; Morrison, S. Blood Flow Restriction Training. J. Athl. Train. 2021, 56, 937–944. [Google Scholar] [CrossRef]
- Sato, Y. The History and Future of KAATSU Training. Int. J. KAATSU Train. Res. 2005, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Hunt, J.E.A.; Walton, L.A.; Ferguson, R.A. Brachial Artery Modifications to Blood Flow-Restricted Handgrip Training and Detraining. J. Appl. Physiol. 2012, 112, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R.A.; Hunt, J.E.A.; Lewis, M.P.; Martin, N.R.W.; Player, D.J.; Stangier, C.; Taylor, C.W.; Turner, M.C. The Acute Angiogenic Signalling Response to Low-Load Resistance Exercise with Blood Flow Restriction. Eur. J. Sport Sci. 2018, 18, 397–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wortman, R.J.; Brown, S.M.; Savage-Elliott, I.; Finley, Z.J.; Mulcahey, M.K. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sports Med. 2021, 49, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Wooten, S.V.; Stray-Gundersen, S.; Tanaka, H. Hemodynamic and Pressor Responses to Combination of Yoga and Blood Flow Restriction. Int. J. Sports Med. 2020, 41, 759–765. [Google Scholar] [CrossRef]
- Montgomery, R.; Paterson, A.; Williamson, C.; Florida-James, G.; Ross, M.D. Blood Flow Restriction Exercise Attenuates the Exercise-Induced Endothelial Progenitor Cell Response in Healthy, Young Men. Front. Physiol. 2019, 10, 447. [Google Scholar] [CrossRef] [Green Version]
- Centner, C.; Wiegel, P.; Gollhofer, A.; König, D. Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 95–108. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, F.A.; Pires, F.O.; Rønnestad, B.R.; Hardt, F.; Conceição, M.S.; Lixandrão, M.E.; Berton, R.; Tricoli, V. The Effect of Low-Intensity Aerobic Training Combined with Blood Flow Restriction on Maximal Strength, Muscle Mass, and Cycling Performance in a Cyclist with Knee Displacement. Int. J. Environ. Res. Public Health 2022, 19, 2993. [Google Scholar] [CrossRef] [PubMed]
- Kambič, T.; Novaković, M.; Tomažin, K.; Strojnik, V.; Jug, B. Blood Flow Restriction Resistance Exercise Improves Muscle Strength and Hemodynamics, but Not Vascular Function in Coronary Artery Disease Patients: A Pilot Randomized Controlled Trial. Front. Physiol. 2019, 10, 656. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, M.; Okita, K. Blood Flow Restricted Exercise and Vascular Function. Int. J. Vasc. Med. 2012, 2012, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Tian, G.; Wang, X. Effects of Low-Load Blood Flow Restriction Training on Hemodynamic Responses and Vascular Function in Older Adults: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6750. [Google Scholar] [CrossRef]
- Sitia, S.; Tomasoni, L.; Atzeni, F.; Ambrosio, G.; Cordiano, C.; Catapano, A.; Tramontana, S.; Perticone, F.; Naccarato, P.; Camici, P.; et al. From Endothelial Dysfunction to Atherosclerosis. Autoimmun. Rev. 2010, 9, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Norata, G.D.; Catapano, A.L. Molecular Mechanisms Responsible for the Antiinflammatory and Protective Effect of HDL on the Endothelium. Vasc. Health Risk Manag. 2005, 1, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veith, A.P.; Henderson, K.; Spencer, A.; Sligar, A.D.; Baker, A.B. Therapeutic Strategies for Enhancing Angiogenesis in Wound Healing. Adv. Drug Deliv. Rev. 2019, 146, 97–125. [Google Scholar] [CrossRef]
- Kaczmarczyk, P.; Maga, P.; Niżankowski, R.; Januszek, R.; Frołow, M.; Maga, M.; Kościelniak, J.; Belowski, A. The Relationship between Pulse Waveform Analysis Indices, Endothelial Function and Clinical Outcomes in Patients with Peripheral Artery Disease Treated Using Percutaneous Transluminal Angioplasty during a One-Year Follow-up Period. Cardiol. J. 2020, 27, 142–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaczmarczyk, P.; Frołow, M.; Januszek, R.; Belowski, A.; Gregorczyk-Maga, I.; Chlopicki, S.; Maga, P. Endothelial Function in Patients with Critical and Non-Critical Limb Ischemia Undergoing Endovascular Treatment. Kardiol. Pol. 2021, 79, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Man, A.W.C.; Li, H.; Xia, N. Impact of Lifestyles (Diet and Exercise) on Vascular Health: Oxidative Stress and Endothelial Function. Oxid. Med. Cell. Longev. 2020, 2020, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Gladden, J.; Wernecke, C.; Rector, S.; Tecson, K.; McCullough, P. Pilot Safety Study: The Use of Vasper TM, a Novel Blood Flow Restriction Exercise in Healthy Adults. J. Exerc. Physiol. 2016, 19, 99–106. [Google Scholar]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert Consensus and Evidence-Based Recommendations for the Assessment of Flow-Mediated Dilation in Humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Januszek, R.; Mika, P.; Nowobilski, R.; Maga, P.; Niżankowski, R. The Improvement of Walking Abilities and Endothelial Function after the Supervised Training Treadmill Program (STTP) in Patients with Peripheral Artery Disease (PAD) Is Not Related to Prostacyclin and Thromboxane Release. Int. J. Cardiol. 2016, 222, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Ceciliato, J.; Costa, E.C.; Azevêdo, L.; Sousa, J.C.; Fecchio, R.Y.; Brito, L.C. Effect of Resistance Training on Arterial Stiffness in Healthy Subjects: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22, 51. [Google Scholar] [CrossRef] [PubMed]
- Januszek, R.; Mika, P.; Konik, A.; Petriczek, T.; Nowobilski, R.; Niżankowski, R. The Effect of Treadmill Training on Endothelial Function and Walking Abilities in Patients with Peripheral Arterial Disease. J. Cardiol. 2014, 64, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, J.; Deng, S.; She, Q.; Wu, L. The Effects of Aerobic Endurance Exercise on Pulse Wave Velocity and Intima Media Thickness in Adults: A Systematic Review and Meta-Analysis. Scand. J. Med. Sci. Sports 2016, 26, 478–487. [Google Scholar] [CrossRef]
- Manini, T.M.; Clark, B.C. Blood Flow Restricted Exercise and Skeletal Muscle Health. Exerc. Sport Sci. Rev. 2009, 37, 78–85. [Google Scholar] [CrossRef]
- Winchester, L.J.; Blake, M.T.; Fleming, A.R.; Aguiar, E.J.; Fedewa, M.V.; Esco, M.R.; Earley, R.L. Hemodynamic Responses to Resistance Exercise with Blood Flow Restriction Using a Practical Method Versus a Traditional Cuff-Inflation System. Int. J. Environ. Res. Public Health 2022, 19, 11548. [Google Scholar] [CrossRef]
- Gustafsson, T.; Ameln, H.; Fischer, H.; Sundberg, C.J.; Timmons, J.A.; Jansson, E. VEGF-A Splice Variants and Related Receptor Expression in Human Skeletal Muscle Following Submaximal Exercise. J. Appl. Physiol. 2005, 98, 2137–2146. [Google Scholar] [CrossRef] [Green Version]
- Spranger, M.D.; Krishnan, A.C.; Levy, P.D.; O’Leary, D.S.; Smith, S.A. Blood Flow Restriction Training and the Exercise Pressor Reflex: A Call for Concern. Am. J. Physiol. Circ. Physiol. 2015, 309, H1440–H1452. [Google Scholar] [CrossRef]
- Ramis, T.R.; Muller, C.H.d.L.; Boeno, F.P.; Teixeira, B.C.; Rech, A.; Pompermayer, M.G.; Medeiros, N.d.S.; de Oliveira, Á.R.; Pinto, R.S.; Ribeiro, J.L. Effects of Traditional and Vascular Restricted Strength Training Program With Equalized Volume on Isometric and Dynamic Strength, Muscle Thickness, Electromyographic Activity, and Endothelial Function Adaptations in Young Adults. J. Strength Cond. Res. 2020, 34, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Paiva, F.M.; Vianna, L.C.; Fernandes, I.A.; Nóbrega, A.C.; Lima, R.M. Effects of Disturbed Blood Flow during Exercise on Endothelial Function: A Time Course Analysis. Braz. J. Med. Biol. Res. = Rev. Bras. Pesqui. Med. Biol. 2016, 49, e5100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Credeur, D.P.; Hollis, B.C.; Welsch, M.A. Effects of Handgrip Training with Venous Restriction on Brachial Artery Vasodilation. Med. Sci. Sports Exerc. 2010, 42, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Starzak, M.; Stanek, A.; Jakubiak, G.K.; Cholewka, A.; Cieślar, G. Arterial Stiffness Assessment by Pulse Wave Velocity in Patients with Metabolic Syndrome and Its Components: Is It a Useful Tool in Clinical Practice? Int. J. Environ. Res. Public Health 2022, 19, 10368. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, U.; Karabulut, M.; James, E.G. Small Arteries Stay Stiff for a Longer Period Following Vibration Exercises in Combination with Blood Flow Restriction. Clin. Physiol. Funct. Imaging 2018, 38, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Fahs, C.A.; Rossow, L.M.; Seo, D.-I.; Loenneke, J.P.; Sherk, V.D.; Kim, E.; Bemben, D.A.; Bemben, M.G. Effect of Different Types of Resistance Exercise on Arterial Compliance and Calf Blood Flow. Eur. J. Appl. Physiol. 2011, 111, 2969–2975. [Google Scholar] [CrossRef]
- Poredoš, P.; Bešič, H.; Jeraj, L. Relationship between Endothelial Function of Micro-and Macrocirculation in Patients with Peripheral Arterial Disease. Vasa Eur. J. Vasc. Med. 2017, 46, 19–22. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-Intensity Resistance Training with Blood Flow Restriction Improves Vascular Endothelial Function and Peripheral Blood Circulation in Healthy Elderly People. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Christiansen, D.; Eibye, K.H.; Hostrup, M.; Bangsbo, J. Blood Flow-Restricted Training Enhances Thigh Glucose Uptake during Exercise and Muscle Antioxidant Function in Humans. Metabolism 2019, 98, 1–15. [Google Scholar] [CrossRef]
- Barjaste, A.; Mirzaei, B.; Rahmani-nia, F.; Haghniyaz, R.; Brocherie, F. Concomitant Aerobic- and Hypertrophy-Related Skeletal Muscle Cell Signaling Following Blood Flow-Restricted Walking. Sci. Sports 2020, 36, e51–e58. [Google Scholar] [CrossRef]
- Barili, A.; Corralo, V.d.S.; Cardoso, A.M.; Mânica, A.; Bonadiman, B.d.S.R.; Bagatini, M.D.; Da Silva-Grigoletto, M.E.; de Oliveira, G.G.; De Sá, C.A. Acute Responses of Hemodynamic and Oxidative Stress Parameters to Aerobic Exercise with Blood Flow Restriction in Hypertensive Elderly Women. Mol. Biol. Rep. 2018, 45, 1099–1109. [Google Scholar] [CrossRef]
- Ivy, S.P.; Wick, J.Y.; Kaufman, B.M. An Overview of Small-Molecule Inhibitors of VEGFR Signaling. Nat. Rev. Clin. Oncol. 2009, 6, 569–579. [Google Scholar] [CrossRef]
- Jiang, L.; Chen, T.; Sun, S.; Wang, R.; Deng, J.; Lyu, L.; Wu, H.; Yang, M.; Pu, X.; Du, L.; et al. Nonbone Marrow CD34+Cells Are Crucial for Endothelial Repair of Injured Artery. Circ. Res. 2021, 129, e146–e165. [Google Scholar] [CrossRef] [PubMed]
- Boeno, F.P.; Ramis, T.R.; Farinha, J.B.; de Lemos, L.S.; Medeiros, N.D.S.; Ribeiro, J.L. Efeito Agudo Do Exercício de Força Com Restrição Do Fluxo Sanguíneo Sobre Parâmetros Antioxidantes Em Indivíduos Jovens Saudáveis. J. Vasc. Bras. 2018, 17, 122–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonorino, S.L.; Corralo, V.D.S.; Copatti, S.L.; Da Matta, E.S.; Dornelles, A.L.; De Sá, C.A. Acute Effects of Strength Exercise with Blood Flow Restriction on the Arterial Resistance Index. J. Phys. Educ. 2020, 31, 24482455. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M.; Hoffman, R.L.; Williams, P.S.; Guiler, M.K.; Knutson, M.J.; McGLynn, M.L.; Kushnick, M.R. Relative Safety of 4 Weeks of Blood Flow-Restricted Resistance Exercise in Young, Healthy Adults. Scand. J. Med. Sci. Sports 2011, 21, 653–662. [Google Scholar] [CrossRef]
- Korkmaz, H.; Akbulut, M.; Özbay, Y.; Ko, M. A New Noninvasive Method in Evaluating the Endothelial Function: The Measurement of the Resistive Index after Reactive Hyperemia of the Brachial Artery. Echocardiography 2010, 27, 873–877. [Google Scholar] [CrossRef]
- Stoner, L.; Faulkner, J.; Lowe, A.; Lambrick, D.M.; Young, J.M.; Love, R.; Rowlands, D.S. Should the Augmentation Index Be Normalized to Heart Rate? J. Atheroscler. Thromb. 2014, 21, 11–16. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maga, M.; Schönborn, M.; Wachsmann-Maga, A.; Śliwka, A.; Krężel, J.; Włodarczyk, A.; Olszewska, M.; Nowobilski, R. Stimulation of the Vascular Endothelium and Angiogenesis by Blood-Flow-Restricted Exercise. Int. J. Environ. Res. Public Health 2022, 19, 15859. https://doi.org/10.3390/ijerph192315859
Maga M, Schönborn M, Wachsmann-Maga A, Śliwka A, Krężel J, Włodarczyk A, Olszewska M, Nowobilski R. Stimulation of the Vascular Endothelium and Angiogenesis by Blood-Flow-Restricted Exercise. International Journal of Environmental Research and Public Health. 2022; 19(23):15859. https://doi.org/10.3390/ijerph192315859
Chicago/Turabian StyleMaga, Mikołaj, Martyna Schönborn, Agnieszka Wachsmann-Maga, Agnieszka Śliwka, Jakub Krężel, Aleksandra Włodarczyk, Marta Olszewska, and Roman Nowobilski. 2022. "Stimulation of the Vascular Endothelium and Angiogenesis by Blood-Flow-Restricted Exercise" International Journal of Environmental Research and Public Health 19, no. 23: 15859. https://doi.org/10.3390/ijerph192315859