

Polytetrafluorethylene (PTFE) vs. Polyester (Dacron®) Grafts in Critical Limb Ischemia Salvage

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Revascularization Technique
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kinlay, S. Management of Critical Limb Ischemia. Circ. Cardiovasc. Interv. 2016, 9, e001946. [Google Scholar] [CrossRef] [Green Version]
- Murabito, J.M.; Evans, J.C.; Nieto, K.; Larson, M.G.; Levy, D.; Wilson, P.W.F. Prevalence and Clinical Correlates of Peripheral Arterial Disease in the Framingham Offspring Study. Am. Heart J. 2002, 143, 961–965. [Google Scholar] [CrossRef]
- Stoyioglou, A.; Jaff, M.R. Medical Treatment of Peripheral Arterial Disease: A Comprehensive Review. J. Vasc. Interv. Radiol. 2004, 15, 1197–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Dabrh, A.M.; Steffen, M.W.; Undavalli, C.; Asi, N.; Wang, Z.; Elamin, M.B.; Conte, M.S.; Murad, M.H. The Natural History of Untreated Severe or Critical Limb Ischemia. J. Vasc. Surg. 2015, 62, 1642–1651.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steg, P.G.; Bhatt, D.L.; Wilson, P.W.F.; D’Agostino, R.; Ohman, E.M.; Röther, J.; Liau, C.-S.; Hirsch, A.T.; Mas, J.-L.; Ikeda, Y.; et al. One-Year Cardiovascular Event Rates in Outpatients With Atherothrombosis. JAMA 2007, 297, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.; Migliaccio-Walle, K.; Ishak, K.J.; Proskorovsky, I. The Morbidity and Mortality Following a Diagnosis of Peripheral Arterial Disease: Long-Term Follow-up of a Large Database. BMC Cardiovasc. Disord. 2005, 5, 14. [Google Scholar] [CrossRef] [Green Version]
- Bradbury, A.W.; Adam, D.J.; Bell, J.; Forbes, J.F.; Fowkes, F.G.R.; Gillespie, I.; Ruckley, C.V.; Raab, G.M. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) Trial: Analysis of Amputation Free and Overall Survival by Treatment Received. J. Vasc. Surg. 2010, 51, 18S–31S. [Google Scholar] [CrossRef] [Green Version]
- Romiti, M.; Albers, M.; Brochado-Neto, F.C.; Durazzo, A.E.S.; Pereira, C.A.B.; De Luccia, N. Meta-Analysis of Infrapopliteal Angioplasty for Chronic Critical Limb Ischemia. J. Vasc. Surg. 2008, 47, 975–981.e1. [Google Scholar] [CrossRef]
- Albers, M.; Romiti, M.; Brochado-Neto, F.C.; Pereira, C.A.B. Meta-Analysis of Alternate Autologous Vein Bypass Grafts to Infrapopliteal Arteries. J. Vasc. Surg. 2005, 42, 449.e1–449.e8. [Google Scholar] [CrossRef]
- Slovut, D.P.; Lipsitz, E.C. Surgical Technique and Peripheral Artery Disease. Circulation 2012, 126, 1127–1138. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.L.; Halperin, J.L.; Albert, N.; Bozkurt, B.; Brindis, R.G.; Curtis, L.H.; DeMets, D.; Guyton, R.A.; Hochman, J.S.; Kovacs, R.J.; et al. Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations). J. Am. Coll. Cardiol. 2013, 61, 1555–1570. [Google Scholar] [CrossRef] [Green Version]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109.e33. [Google Scholar] [CrossRef] [Green Version]
- Muresan, V.A.; Cosarca, M.C.; Russu, E.; Niculescu, R.; Zăgan, C.A. A Rare Case of Abdominal Aortic Aneurysm with Ureteral Compression. J. Interdiscip. Med. 2021, 6, 171–173. [Google Scholar] [CrossRef]
- Mocian, A.; Russu, E.; Kaller, R.; Mureșan, A. Aorto-Mesenteric Bypass for the Treatment of Chronic Mesenteric Ischemia. J. Interdiscip. Med. 2019, 4, 101–103. [Google Scholar] [CrossRef] [Green Version]
- Muresan, V.A.; Cosarca, M.C.; Russu, E.; Niculescu, R.; Soimu, M. Ilio-Deep Femoral Bypass—An Alternative Treatment Strategy to Critical Limb Ischemia (CLI). J. Interdiscip. Med. 2021, 6, 108–111. [Google Scholar] [CrossRef]
- Russu, E. Rolul By-Pass-ului extra-anatomic in managementul ischemiei membrelor inferioare. Ph.D. Thesis, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Targu Mures, Targu Mures, Romania, 2011. [Google Scholar]
- Eliza, R.; Toma, L.; Mureșan, A.; Preda, R.; Oroșan, S.; Constantinescu, F.; Grigorescu, B. Risk Scoring Systems Used in the Multidisciplinary decision of Extra-Anatomic By-passes. Acta Med. Marisiensis 2010, 56, 561–562. [Google Scholar]
- Kaller, R.; Mureșan, A.V.; Popa, D.G.; Arbănași, E.-M.; Russu, E. Fatal Aortoduodenal Fistula Caused by a Ruptured Abdominal Aortic Aneurysm—A Case Report. J. Cardiovasc. Emergencies 2021, 7, 129–132. [Google Scholar] [CrossRef]
- Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Arbănași, E.M.; Kovács, I.; Horváth, E.; Suciu, B.A.; Hosu, I.; Russu, E. Uncommon Surgical Management by AVF between the Great Saphenous Vein and Anterior Tibial Artery for Old Radiocephalic AVF Failure. Life 2022, 12, 529. [Google Scholar] [CrossRef]
- Arbanasi, E.M.; Russu, E.; Muresan, A.V.; Arbanasi, E.M.; Kaller, R. Ulnar-Basilic Arteriovenous Fistula with Multilocular Gigantic Aneurysmal Dilatation: A Case Report. Acta Marisiensis Ser. Med. 2021. [Google Scholar] [CrossRef]
- Najjar, S.F. VASCULAR SURGERY-2 VOLUME SET, 6TH EDITION. Shock 2006, 25, 209. [Google Scholar] [CrossRef]
- Russu, E.; Mureșan, A.V.; Cordoș, B.A.; Copotoiu, C.; Cotoi, O.S. Morpho-Pathological Review on the Healing of Synthetic Vascular Grafts. Acta Marisiensis Ser. Med. 2016, 62, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Eliza, R.; Vasile, M.A.; Andrei, C.B.; Simion, C.O.; Constantin, C. Tissue Integration of Synthetic Grafts and the Impact of Soft-Tissue Infection—An Experimental Model. Acta Med. Marisiensis 2015, 61, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Branchereau, A.; Rudondy, P.; Gournier, J.-P.; Espinoza, H. The Albumin-Coated Knitted Dacron Aortic Prosthesis: A Clinical Study. Ann. Vasc. Surg. 1990, 4, 138–142. [Google Scholar] [CrossRef]
- den Hoed, P.T.; Veen, H.F. The Late Complications of Aorto-Ilio-Femoral Dacron Prostheses: Dilatation and Anastomotic Aneurysm Formation. Eur. J. Vasc. Surg. 1992, 6, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Greisler, H.P. Characteristics and healing of vascular grafts. Vasc. Surg. Theory Pract. 1995, 1181–1212. [Google Scholar]
- Halmaciu, I.; Arbănași, E.M.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Bacalbasa, N.; Suciu, B.A.; Cojocaru, I.I.; Runcan, A.I.; Grosu, F.; et al. Chest CT Severity Score and Systemic Inflammatory Biomarkers as Predictors of the Need for Invasive Mechanical Ventilation and of COVID-19 Patients’ Mortality. Diagnostics 2022, 12, 2089. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Halmaciu, I.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Suciu, B.A.; Coșarcă, C.M.; Cojocaru, I.I.; Melinte, R.M.; Russu, E. Systemic Inflammatory Biomarkers and Chest CT Findings as Predictors of Acute Limb Ischemia Risk, Intensive Care Unit Admission, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2379. [Google Scholar] [CrossRef]
- Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; Voidăzan, S.; Arbănași, E.M.; Horváth, E.; Suciu, B.A.; Hosu, I.; Halmaciu, I.; Brinzaniuc, K.; et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life 2022, 12, 1447. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Hălmaciu, I.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Budișcă, O.A.; Melinte, R.M.; Vunvulea, V.; Filep, R.C.; Mărginean, L.; et al. Prognostic Nutritional Index, Controlling Nutritional Status (CONUT) Score, and Inflammatory Biomarkers as Predictors of Deep Vein Thrombosis, Acute Pulmonary Embolism, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2757. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Mureșan, A.V.; Coșarcă, C.M.; Kaller, R.; Bud, T.I.; Hosu, I.; Voidăzan, S.T.; Arbănași, E.M.; Russu, E. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Impact on Predicting Outcomes in Patients with Acute Limb Ischemia. Life 2022, 12, 822. [Google Scholar] [CrossRef]
- Melinte, R.M.; Arbănași, E.M.; Blesneac, A.; Zolog, D.N.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Melinte, I.M.; Niculescu, R.; Russu, E. Inflammatory Biomarkers as Prognostic Factors of Acute Deep Vein Thrombosis Following the Total Knee Arthroplasty. Med. (Mex.) 2022, 58, 1502. [Google Scholar] [CrossRef] [PubMed]
- Russu, E.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Voidăzan, S.; Arbănași, E.M.; Coșarcă, C.M. The Predictive Role of NLR and PLR in Outcome and Patency of Lower Limb Revascularization in Patients with Femoropopliteal Disease. J. Clin. Med. 2022, 11, 2620. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Cojocaru, I.I.; Coșarcă, C.M.; Russu, E. The Neutrophil-to-Lymphocyte Ratio’s Predictive Utility in Acute Pulmonary Embolism: Systematic Review. J. Cardiovasc. Emergencies 2022, 8, 25–30. [Google Scholar] [CrossRef]
- Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public. Health 2022, 19, 13934. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk Stratification Based on Wound, Ischemia, and Foot Infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, M.P.; Blais, R.; Guidoin, E.; Prowse, M.; Marois, C.; Gosselin, H.P.; Noel. Polyethylene terephthalate (Dacron) vascular prostheses-material and fabric construction aspects. Biocompat. Clin. Implant. Mater. 1981, 2, 177–207. [Google Scholar]
- Davids, L.; Dower, T.; Zilla, P. The lack of healing in conventional vascular grafts. Tissue Eng. Prosthet. Vasc. Grafts 1999, 3–44. [Google Scholar]
- Nunn, D.B. Structural Failure of Dacron Arterial Grafts. Semin Vasc. Surg. 1999, 12, 83–91. [Google Scholar] [PubMed]
- Sottiurai, V.S.; Yao, J.S.T.; Flinn, W.R.; Batson, R.C. Intimal Hyperplasia and Neointima: An Ultrastructural Analysis of Thrombosed Grafts in Humans. Surgery 1983, 93, 809–817. [Google Scholar] [CrossRef]
- Clowes, A.W.; Gown, A.M.; Hanson, S.R.; Reidy, M.A. Mechanisms of Arterial Graft Failure. 1. Role of Cellular Proliferation in Early Healing of PTFE Prostheses. Am. J. Pathol 1985, 118, 43–54. [Google Scholar] [PubMed]
- Scott, S.M.; Gaddy, L.R.; Sahmel, R.; Hoffman, H. A Collagen Coated Vascular Prosthesis. J. Cardiovasc Surg. (Torino) 1987, 28, 498–504. [Google Scholar]
- Cziperle, D.J.; Joyce, K.A.; Tattersall, C.W.; Henderson, S.C.; Cabusao, E.B.; Garfield, J.D.; Kim, D.U.; Duhamel, R.C.; Greisler, H.P. Albumin Impregnated Vascular Grafts: Albumin Resorption and Tissue Reactions. J. Cardiovasc Surg. (Torino) 1992, 33, 407–414. [Google Scholar]
- Akers, D.L.; Du, Y.H.; Kempczinski, R.F. The Effect of Carbon Coating and Porosity on Early Patency of Expanded Polytetrafluoroethylene Grafts: An Experimental Study. J. Vasc. Surg. 1993, 18, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Prager, M.; Polterauer, P.; Böhmig, H.-J.; Wagner, O.; Fügl, A.; Kretschmer, G.; Plohner, M.; Nanobashvili, J.; Huk, I. Collagen versus Gelatin-Coated Dacron versus Stretch Polytetrafluoroethylene in Abdominal Aortic Bifurcation Graft Surgery: Results of a Seven-Year Prospective, Randomized Multicenter Trial. Surgery 2001, 130, 408–414. [Google Scholar] [CrossRef]
- Arbănași, E.-M.; Russu, E.; Mureșan, A.V.; Arbănași, E.-M. Late Rupture of a Thrombosed Aortic Abdominal Aneurysm—A Case Report. J. Cardiovasc. Emergencies 2021, 7, 84–87. [Google Scholar] [CrossRef]
- Robinson, B.I.; Fletcher, J.P.; Tomlinson, P.; Allen, R.D.M.; Hazelton, S.J.; Richardson, A.J.; Stuchbery, K. A Prospective Randomized Multicentre Comparison of Expanded Polytetrafluoroethylene and Gelatin-Sealed Knitted Dacron Grafts for Femoropopliteal Bypass. Cardiovasc. Surg. 1999, 7, 214–218. [Google Scholar] [CrossRef]
- Devine, C.; McCollum, C. Heparin-Bonded Dacron or Polytetrafluorethylene for Femoropopliteal Bypass: Five-Year Results of a Prospective Randomized Multicenter Clinical Trial. J. Vasc. Surg. 2004, 40, 924–931. [Google Scholar] [CrossRef]
- Post, S.; Kraus, T.; Müller-Reinartz, U.; Weiss, C.; Kortmann, H.; Quentmeier, A.; Winkler, M.; Husfeldt, K.J.; Allenberg, J.R. Dacron vs Polytetrafluoroethylene Grafts for Femoropopliteal Bypass:A Prospective Randomised Multicentre Trial. Eur. J. Vasc. Endovasc. Surg. 2001, 22, 226–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, R.M.; Abbott, W.M.; Matsumoto, T.; Wheeler, J.R.; Miller, N.; Veith, F.J.; Money, S.; Garrett, H.E. Prosthetic Above-Knee Femoropopliteal Bypass Grafting: Five-Year Results of a Randomized Trial. J. Vasc. Surg. 2000, 31, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.I.; Fletcher, J.P. The Australian and New Zealand Femoropopliteal Graft Trial Participants Fluoropolymer Coated Dacron or Polytetrafluoroethylene for Femoropopliteal Bypass Grafting: A Multicentre Trial. ANZ J. Surg. 2003, 73, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.P.; Lepäntalo, M.; Fossdal, J.E.; Røder, O.C.; Jensen, B.S.; Madsen, M.S.; Grenager, O.; Fasting, H.; Myhre, H.O.; Bækgaard, N.; et al. Dacron or PTFE for Above-Knee Femoropopliteal Bypass. A Multicenter Randomised Study. Eur. J. Vasc. Endovasc. Surg. 2007, 34, 44–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | All Patients (n = 183) | PTFE Group (n = 98) | Dacron Group (n = 85) | p Value |
|---|---|---|---|---|
| Age (years) mean ± SD | 69.2 ± 8.54 | 69.79 ± 8.38 | 68.52 ± 8.71 | 0.31 |
| Sex (M) (%, no) | 75.41% (138) | 79.59% (78) | 70.53% (60) | 0.16 (0.61; 0.31–1.21) |
| Leriche–Fontaine Classification | ||||
| Stage III LF (%, no) | 63.38% (116) | 70.41% (69) | 55.29% (47) | 0.03 (0.51; 0.28–0.95) |
| Stage IV LF (%, no) | 36.61% (67) | 29.59% (29) | 44.71% (38) | 0.03 (1.92; 1.04–3.53) |
| Wifi Classification | ||||
| Wound grade | ||||
| 0 | 63.38% (116) | 70.41% (69) | 55.29% (47) | 0.03 |
| 1 | 21.86% (40) | 18.37% (18) | 25.88% (22) | 0.22 |
| 2 | 10.93% (20) | 9.18% (9) | 12.94% (11) | 0.41 |
| 3 | 2.04% (7) | 2.04% (2) | 5.88% (5) | 0.19 |
| Ischemia severity | ||||
| 0 | 18.58% (34) | 14.29% (14) | 23.53% (20) | 0.11 |
| 1 | 31.15% (57) | 31.63% (31) | 30.59% (26) | 0.87 |
| 2 | 37.16% (68) | 35.71% (35) | 35.71% (33) | 0.66 |
| 3 | 13.11% (24) | 18.37% (18) | 7.06% (6) | 0.02 |
| Foot infection grade | ||||
| 0 | 63.38% (116) | 70.41% (69) | 55.29% (47) | 0.03 |
| 1 | 82.51% (151) | 83.67% (82) | 81.18% (69) | 0.07 |
| 2 | 25.68% (47) | 24.49% (24) | 27.06% (23) | 0.24 |
| 3 | 85.25% (156) | 83.67% (82) | 87.06% (74) | 0.55 |
| Comorbidities | ||||
| AH (%, no) | 85.25% (156) | 83.67% (82) | 87.06% (74) | 0.52 (1.31; 0.57–3.008) |
| IHD (%, no) | 82.51% (151) | 83.67% (82) | 81.18% (69) | 0.65 (0.84; 0.39–1.80) |
| AF (%, no) | 25.68% (47) | 24.49% (24) | 27.06% (23) | 0.69 (1.14; 0.58–2.22) |
| MI (%, no) | 33.88% (62) | 33.67% (33) | 34.12% (29) | 0.94 (1.02; 0.55–1.88) |
| CHF (%, no) | 63.93% (117) | 61.22% (60) | 67.06% (57) | 0.41 (1.28; 0.70–2.36) |
| COPD (%, no) | 22.95% (42) | 29.59% (29) | 15.29% (13) | 0.02 (0.42; 0.20–0.89) |
| CKD (%, no) | 21.86% (40) | 23.47% (23) | 20% (17) | 0.57 (0.81; 0.40–1.65) |
| CVA (%, no) | 24.59% (45) | 23.47% (23) | 25.88% (22) | 0.70 (1.13; 0.58–2.23) |
| T2D (%, no) | 48.63% (89) | 51.02% (50) | 45.88% (39) | 0.48 (0.81; 0.45–1.45) |
| CVI (%, no) | 27.87% (51) | 22.45% (22) | 34.12% (29) | 0.08 (1.78; 0.93–3.43) |
| Risk Factors | ||||
| Obesity (%, no) | 40.44% (74) | 40.82% (40) | 40% (34) | 0.91 (0.96; 0.53–1.74) |
| Hyperlipidemia (%, no) | 65.03% (119) | 61.22% (60) | 69.41% (59) | 0.24 (1.43; 0.77–2.65) |
| Tobacco (%, no) | 77.05% (141) | 78.57% (77) | 75.29% (64) | 0.59 (0.83; 0.41–1.65) |
| Variables (Mean ± SD) | All Patients (n = 183) | PTFE Group (n = 98) | Dacron Group (n = 85) | p Value |
|---|---|---|---|---|
| Hemoglobin g/dL | 13.67 + 1.72 | 13.55 + 1.62 | 13.8 + 1.84 | 0.28 |
| Hematocrit % | 41.68 + 5.11 | 41.25 + 4.68 | 42.18 + 5.55 | 0.20 |
| Glucose mg/dL | 119.55 + 46.02 | 119.08 + 49.68 | 120.09 + 41.7 | 0.17 |
| ALT u/L | 29.99 + 3.47 | 31.54 + 4.29 | 28.19 + 2.25 | 0.27 |
| AST u/L | 35.91 + 4.33 | 38.28 + 4.97 | 33.17 + 3.45 | 0.34 |
| Total bilirubin mg/dL | 0.48 + 0.24 | 0.47 + 0.25 | 0.49 + 0.22 | 0.07 |
| BUN mg/dL | 42.39 + 20.16 | 40.73 + 17.31 | 44.3 + 22.97 | 0.30 |
| Creatinine mg/dL | 1.03 + 071 | 1.08 + 0.90 | 0.96 + 0.38 | 0.07 |
| GFR (mL/min/1.73 m2) | 77.28 + 23.56 | 76.85 + 22.6 | 77.78 + 24.74 | 0.46 |
| K mmol\L | 4.13 + 0.5 | 4.15 + 0.51 | 4.1 + 0.48 | 0.32 |
| Na mmol\L | 140.16 + 3.87 | 139.9 + 3.72 | 140.47 + 4.03 | 0.09 |
| INR | 1.11 + 0.17 | 1.08 + 0.16 | 1.14 + 0.19 | 0.03 |
| APTT (sec) | 30.66 + 5.82 | 30.7 + 5.87 | 30.62 + 5.84 | 0.48 |
| Monocyte × 103/uL | 2.19 + 0.73 | 2.24 + 0.65 | 2.14 + 0.81 | 0.11 |
| Lymphocytes × 103/uL | 0.58 + 0.15 | 0.58 + 0.12 | 0.59 + 0.18 | 0.46 |
| Monocyte × 103/uL | 5.59 + 1.82 | 5.49 + 1.71 | 5.72 + 1.94 | 0.26 |
| Neutrophils × 103/uL | 194.29 + 49.59 | 194.27 + 49.28 | 194.32 + 50.24 | 0.48 |
| PLT × 103/uL | 0.30 + 0.13 | 0.28 + 0.10 | 0.32 + 0.15 | 0.10 |
| MLR | 2.90 + 1.53 | 2.66 + 1.13 | 3.17 + 1.86 | 0.07 |
| NLR | 100.11 + 46.31 | 93.59 + 34.29 | 107.61 + 56.42 | 0.18 |
| PLR | 13.67 + 1.72 | 13.55 + 1.62 | 13.8 + 1.84 | 0.28 |
| All (n = 183) | PTFE Group (n = 98) | Dacron Group (n = 85) | p Value | |
|---|---|---|---|---|
| Type of surgery | ||||
| AK FP bypass, (no, %) | 114 (62.29%) | 77 (78.57%) | 37 (43.53%) | <0.0001 (0.21; 0.11–0.40) |
| BK FP bypass, (no, %) | 42 (22.95%) | 19 (19.39%) | 23 (27.06%) | 0.22 (1.54; 0.77–3.08) |
| FF bypass, (no, %) | 27 (14.75%) | 2 (2.04%) | 25 (29.41%) | 0.0001 (20.01; 4.57–87.5) |
| Patency of bypass | ||||
| 1 month, (%, no) | 90.16% (165) | 90.82% (89) | 89.41% (76) | 0.75 (0.85; 0.32–2.26) |
| 6 months, (%, no) | 73.77% (135) | 80.61% (79) | 65.88% (56) | 0.02 (0.46; 0.23–0.90) |
| 12 months, (%, no) | 57.38% (105) | 64.29% (63) | 49.41% (42) | 0.04 (0.54; 0.29–0.98) |
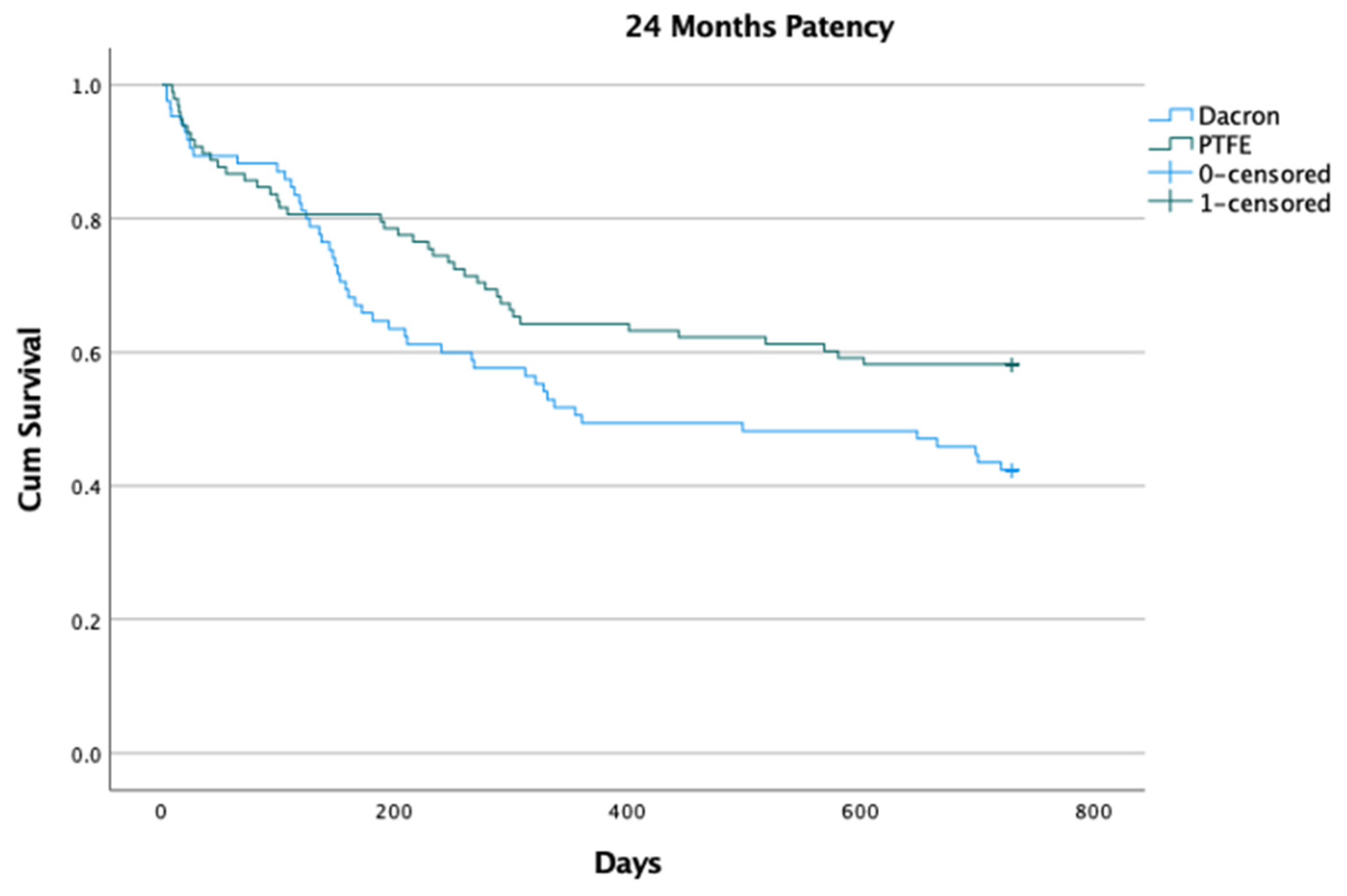
| 24 months, (%, no) | 50.82% (93) | 58.16% (57) | 42.35% (36) | 0.03 (0.52; 0.29–0.95) |
| Outcomes | ||||
| Bypass thrombosis (%, no) | 36.61% (67) | 29.59% (29) | 44.71% (38) | 0.03 (1.92; 1.04–3.53) |
| Graft infection (%, no) | 14.75% (27) | 9.18% (9) | 21.18% (18) | 0.02 (2.65; 1.12–6.28) |
| Bleeding (%, no) | 7.65% (14) | 9.18% (9) | 5.85% (5) | 0.40 (0.61; 0.19–1.92) |
| Above-the-knee amputation, (%, no) | 17.49% (32) | 11.22% (11) | 24.71% (21) | 0.01 (2.59; 1.16–5.76) |
| Below-the-knee amputation, (%, no) | 8.74% (16) | 7.14% (7) | 10.59% (9) | 0.41 (1.53; 0.54–4.32) |
| Death, (%, no) | 11.47% (21) | 8.16% (8) | 14.11% (13) | 0.13 (2.03; 0.79–5.16) |
| PTFE Group (n = 77) | Dacron Group (n = 37) | p Value | |
|---|---|---|---|
| Stage III LF (%, no) | 74.03% (57) | 64.86% (24) | 0.31 (0.64; 0.27–1.50) |
| Stage IV LF (%, no) | 25.97% (20) | 35.14% (13) | 0.31 (1.54; 0.66–3.59) |
| Patency of bypass | |||
| 1 month (%, no) | 90.91% (70) | 97.29% (36) | 0.23 (3.60; 0.42–30.41) |
| 6 months (%, no) | 79.22% (61) | 72.97% (27) | 0.45 (0.70; 0.28–1.76) |
| 12 months (%, no) | 63.64% (49) | 56.76% (21) | 0.48 (0.75; 0.33–1.66) |
| 24 months (%, no) | 57.14% (44) | 54.05% (20) | 0.75 (0.88; 0.40–1.94) |
| Outcomes | |||
| Bypass thrombosis (%, no) | 31.17% (24) | 35.14% (13) | 0.67 (1.19; 0.52–2.74) |
| Graft infection (%, no) | 10.39% (8) | 21.62% (8) | 0.11 (2.37; 0.81–6.94) |
| Bleeding (%, no) | 6.49% (5) | 5.41% (2) | 0.82 (0.82; 0.15–4.45) |
| Above-the-knee amputation (%, no) | 11.69% (9) | 27.03% (10) | 0.04 (2.79; 1.02–7.64) |
| Below-the-knee amputation (%, no) | 3.9% (3) | 5.41% (2) | 0.71 (1.40; 0.22–8.82) |
| Deaths (%, no) | 3.9% (3) | 13.51% (5) | 0.07 (3.85; 0.86–17.10) |
| PTFE Group (n = 19) | Dacron Group (n = 23) | p Value | |
|---|---|---|---|
| Stage III LF (%, no) | 57.89% (11) | 26.09% (6) | 0.04 (0.25; 0.06–0.94) |
| Stage IV LF (%, no) | 42.11% (8) | 73.91% (17) | 0.04 (3.89; 1.05–14.32) |
| Patency of bypass | |||
| 1 month (%, no) | 89.47% (17) | 82.62% (19) | 0.53 (0.55; 0.09–3.44) |
| 6 months (%, no) | 84.21% (16) | 65.22% (15) | 0.17 (0.35; 0.07–1.57) |
| 12 months (%, no) | 63.16% (12) | 39.13% (9) | 0.12 (0.37; 0.10–1.31) |
| 24 months (%, no) | 57.89% (11) | 26.09% (6) | 0.04 (0.25; 0.06–0.94) |
| Outcomes | |||
| Bypass thrombosis (%, no) | 52.63% (9) | 47.83% (11) | 0.98 (1.01; 0.25–4.02) |
| Graft infection (%, no) | 31.57% (6) | 30.43% (7) | 0.93 (0.94; 0.25–3.52) |
| Bleeding (%, no) | 26.31% (5) | 8.7% (2) | 0.14 (0.26; 0.04–1.57) |
| Above-the-knee amputation (%, no) | 31.57% (6) | 21.74% (5) | 0.60 (0.60; 0.15–2.40) |
| Below-the-knee amputation (%, no) | 21.05% (4) | 26.09% (6) | 0.70 (1.32; 0.31–5.60) |
| Death (%, no) | 15.78% (3) | 17.39% (4) | 0.88 (1.12; 0.21–5.70) |
| Primary Patency | Dacron Group | PTFE Group | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| 1 month | 0.85 | 0.32–2.26 | 0.75 | 1.17 | 0.44–3.09 | 0.75 |
| 6 months | 0.46 | 0.23–0.91 | 0.02 | 2.15 | 1.09–4.21 | 0.02 |
| 12 months | 0.54 | 0.30–0.98 | 0.04 | 1.84 | 1.01–3.33 | 0.04 |
| 24 months | 0.52 | 0.29–0.95 | 0.03 | 1.89 | 1.05–3.40 | 0.03 |
| Complications | OR | 95% CI | p Value | OR | 95% CI | p Value |
| Bypass thrombosis | 1.92 | 1.04–3.53 | 0.03 | 0.52 | 0.28–0.95 | 0.03 |
| Graft infection | 2.65 | 1.12–6.28 | 0.02 | 0.37 | 0.15–0.89 | 0.02 |
| Bleeding | 0.61 | 0.19–1.92 | 0.40 | 1.61 | 0.52–5.03 | 0.40 |
| Above-the-knee amputation | 2.59 | 1.16–5.76 | 0.01 | 0.38 | 0.17–0.85 | 0.01 |
| Below-the-knee amputation | 1.53 | 0.54–4.32 | 0.41 | 0.65 | 0.23–1.82 | 0.41 |
| Death | 0.37 | 0.03–3.69 | 0.40 | 2.65 | 0.27–25.89 | 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russu, E.; Mureșan, A.V.; Ivănescu, A.D.; Kaller, R.; Nedelea, D.E.; Niculescu, R.; Cordoș, B.A.; Budișcă, O.A.; Arbănași, E.M.; Arbănași, E.M. Polytetrafluorethylene (PTFE) vs. Polyester (Dacron®) Grafts in Critical Limb Ischemia Salvage. Int. J. Environ. Res. Public Health 2023, 20, 1235. https://doi.org/10.3390/ijerph20021235
Russu E, Mureșan AV, Ivănescu AD, Kaller R, Nedelea DE, Niculescu R, Cordoș BA, Budișcă OA, Arbănași EM, Arbănași EM. Polytetrafluorethylene (PTFE) vs. Polyester (Dacron®) Grafts in Critical Limb Ischemia Salvage. International Journal of Environmental Research and Public Health. 2023; 20(2):1235. https://doi.org/10.3390/ijerph20021235
Chicago/Turabian StyleRussu, Eliza, Adrian Vasile Mureșan, Adrian Dumitru Ivănescu, Réka Kaller, Daniela Elena Nedelea, Raluca Niculescu, Bogdan Andrei Cordoș, Ovidiu Aurelian Budișcă, Eliza Mihaela Arbănași, and Emil Marian Arbănași. 2023. "Polytetrafluorethylene (PTFE) vs. Polyester (Dacron®) Grafts in Critical Limb Ischemia Salvage" International Journal of Environmental Research and Public Health 20, no. 2: 1235. https://doi.org/10.3390/ijerph20021235