
Validation of a Script to Facilitate Social Determinant of Health Conversations with Adolescent Patients
Abstract
:1. Introduction
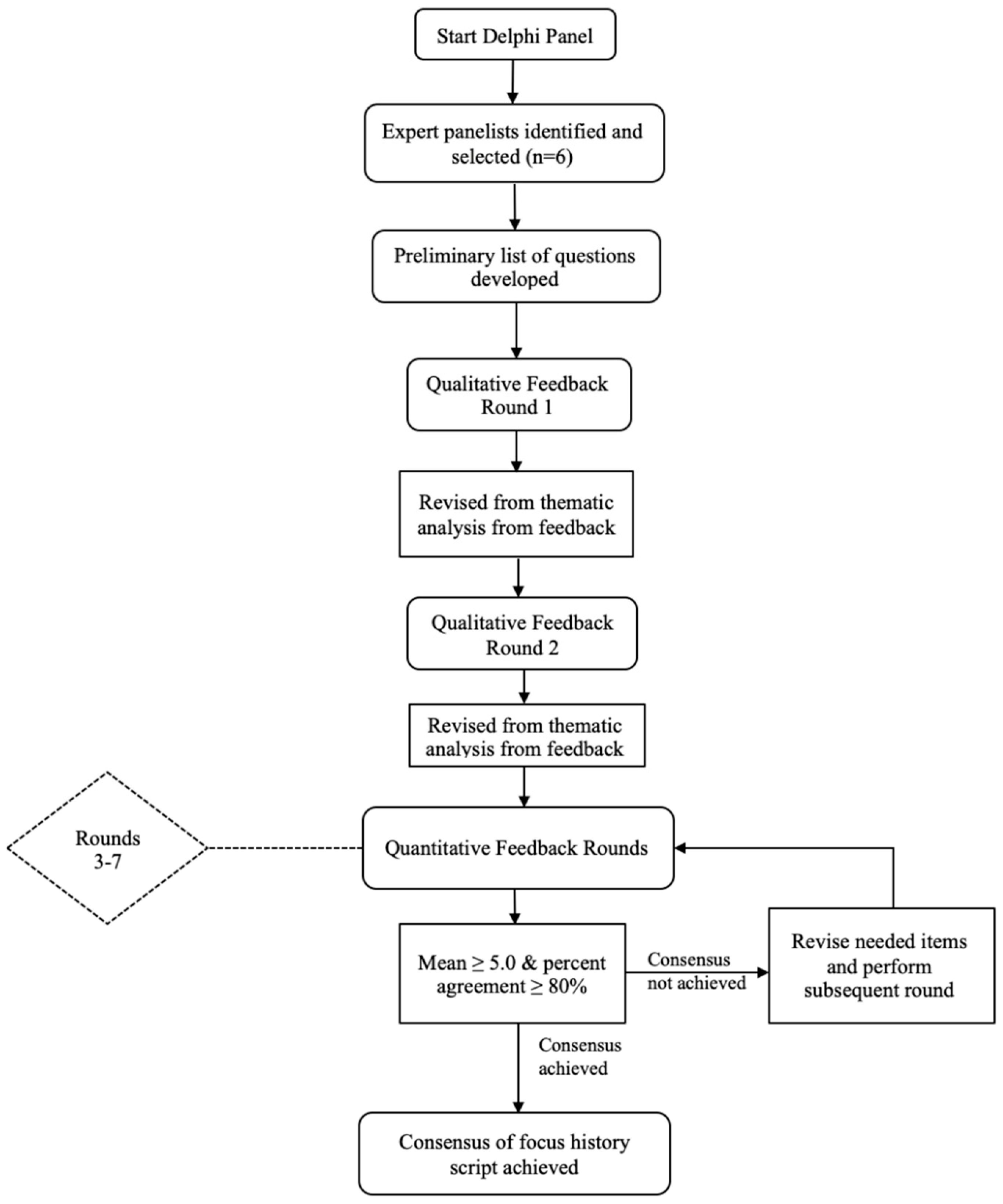
2. Materials and Methods
3. Results
3.1. Round 1
3.2. Round 2
3.3. Round 3
3.4. Round 4
3.5. Round 5
3.6. Round 6
3.7. Round 7
4. Discussion
4.1. SDOH Screening
4.2. Implications for School Health Policy, Practice, and Equity
4.3. Ensuring Script Implementation
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Reflecting Current Evidence | Script Inclusion | ||||
|---|---|---|---|---|---|
| Proposed Item | Mean ± SD | Percent Agreement | Mean ± SD | Percent Agreement | Outcome |
| Round 3 Results. | |||||
| Do you have a primary care provider, such as a family physician or nurse practitioner? (Y/N) | 6.0 ± 0.0 | 100.0% | 5.8 ± 0.8 | 100.0% | Validated. |
| What is your experience with accessing your primary care provider or other medical providers for your health and well-being? | 4.8 ± 0.8 | 66.7% | 5.0 ± 0.9 | 66.7% | Revise to address ease of access. |
| How often (annually, for illness only, etc.) do you see your primary care provider? | 5.3 ± 1.2 | 83.3% | 5.3 ± 1.2 | 83.3% | Validated. |
| What is your experience with the healthcare system beyond your primary care provider? | 4.8 ± 1.2 | 66.7% | 5.0 ± 0.6 | 83.3% | Revise to address target population. |
| Do you have health insurance? (Y/N) | 6.0 ± 0.0 | 100.0% | 5.8 ± 0.4 | 100.0% | Questionnaire error, include in following round. |
| What is your experience with your use of health insurance? | 5.0 ± 0.6 | 83.3% | 5.5 ± 0.6 | 100.0% | Questionnaire error, include in following round. |
| What are your experiences with accessing prescription medicine when needed? | 4.8 ± 1.7 | 66.7% | 4.5 ± 1.1 | 50.0% | Revise to be more direct. |
| Do you use the healthcare system on your own? (Y/N) | 5.0 ± 0.9 | 66.7% | 4.7 ± 1.2 | 50.0% | Eliminated. |
| If yes: What is your experience using the health system? | 4.7 ± 1.0 | 66.7% | 4.7 ± 1.2 | 50.0% | Eliminated. |
| What is your experience with understanding topics when discussing health issues or when given resources by healthcare professionals? | 5.0 ± 0.9 | 66.7% | 5.2 ± 1.0 | 66.7% | Revise to be more conversational. |
| Describe how language influences your interactions in healthcare settings. | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | Validated. |
| Tell me a little about your family’s education. | 4.8 ± 1.3 | 66.7% | 5.0 ± 0.6 | 83.3% | Revise to address those living with the patient. |
| What is your family’s level of education? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.8 | 83.3% | Validated. |
| What is your experience with attending school? | 4.7 ± 1.0 | 66.7% | 4.7 ± 0.8 | 50.0% | Revise to address education quality. |
| What are your thoughts and plans for any educational needs you may have for the future? | 5.2 ± 1.2 | 83.3% | 5.0 ± 0.9 | 66.7% | Revise to be more conversational. |
| Is anything preventing you from additional educational opportunities? If so, please elaborate. | 5.5 ± 0.8 | 83.3% | 5.2 ± 1.0 | 66.7% | No revisions to be made—argument: Education has a direct impact on a person’s health, so educational barriers can lead to a variety of factors decreasing health. Refer to citation. |
| Describe how language influences your interactions in school. | 5.2 ± 1.0 | 66.7% | 5.0 ± 1.3 | 66.7% | Revise to be more conversational. |
| Describe your financial situation. | 5.0 ± 1.3 | 66.7% | 5.0 ± 1.6 | 83.3% | No revisions to be made—argument: Item is intended to explore the socioeconomic status of the patient. |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Being evicted (forced out of where you live) or becoming homeless? | 5.5 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | Validated. |
| b. Having your power shut off? | 5.2 ± 1.0 | 66.7% | 5.0 ± 0.9 | 66.7% | No revisions to be made—argument: Various existing SDOH screening tools address concerns of lack of power, indicating the importance of keeping this item in the script. |
| What is your family’s experience with paying monthly bills? | 5.3 ± 0.8 | 83.3% | 5.0 ± 1.3 | 66.7% | Revise to be more conversational. |
| What is your family’s history with affording your clothes and food? | 5.3 ± 0.8 | 83.3% | 5.0 ± 1.1 | 50.0% | Revise to be more conversational. |
| What is your family’s experience with affording recreational activities? (i.e., Sports outside of school teams, musical instrument lessons, etc.). | 5.2 ± 1.0 | 66.7% | 5.2 ± 1.2 | 83.3% | Revise to be more conversational. |
| Describe your living situation. | 5.2 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | Validated. |
| What is your experience with accessing a grocery store or other markets where you live to get nutritious food? | 5.3 ± 0.8 | 83.3% | 5.2 ± 1.0 | 66.7% | Revise to be more conversational. |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Having clean running water? | 5.5 ± 0.8 | 83.3% | 5.7 ± 0.5 | 100.0% | Validated. |
| b. Being exposed to mold or pests where you live? | 5.7 ± 0.5 | 100.0% | 5.5 ± 0.6 | 100.0% | Validated. |
| c. Feeling safe in your neighborhood? | 5.7 ± 0.5 | 100.0% | 5.7 ± 0.5 | 100.0% | Validated. |
| What type(s) of transportation do you use most often (car, bus, metro, biking, walking, etc.)? | 5.3 ± 0.8 | 83.3% | 5.2 ± 0.8 | 83.3% | Validated. |
| If you had an appointment or needed to get somewhere, can you describe how you might get there? | 5.7 ± 0.5 | 100.0% | 5.5 ± 0.8 | 83.3% | Validated. |
| Tell me about the parks, sidewalks, and other green spaces that are in your neighborhood. | 5.5 ± 0.6 | 100% | 5.3 ± 0.8 | 83.3% | Validated. |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Abuse in the home (physical, verbal, emotional)? | 5.5 ± 0.8 | 83.0% | 5.3 ± 0.5 | 100.0% | Validated. |
| b. Family members getting arrested? | 5.7 ± 0.5 | 100.0% | 5.3 ± 0.5 | 100.0% | Validated. |
| c. Feeling lonely and isolated from your friends and family? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.6 | 100.0% | Validated. |
| d. Being discriminated against for any reason? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.6 | 100.0% | Validated. |
| How would you describe your faith, spirituality, or religious beliefs? | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.5 | 100.0% | Validated. |
| Describe how language influences your interactions in social settings. | 5.3 ± 1.0 | 66.7% | 5.3 ± 0.8 | 83.3% | Revise to be more conversational. |
| Branch Question for following sub questions: For the following questions, think about your experiences with support systems: | |||||
| a. Describe how your relationship is with your family members/guardians. | 5.5 ± 0.8 | 83.3% | 5.7 ± 0.5 | 100.0% | Revise to improve question flow and structure. |
| b. Describe your relationship with your peers. | 5.3 ± 0.8 | 83.3% | 5.5 ± 0.6 | 100.0% | Validated* |
| c. Describe your relationship with your neighbors. | 5.3 ± 0.8 | 83.3% | 5.2 ± 1.0 | 66.7% | Revise to improve question flow and structure. |
| d. Describe your relationship with your teachers/coaches/other adult figures. | 5.2 ± 1.0 | 66.67% | 5.2 ± 1.0 | 66.7% | Revise to improve question flow and structure, and to be more conversational. |
| e. Describe your relationship with healthcare professionals. | 4.5 ± 1.6 | 50.0% | 4.7 ± 1.2 | 50.0% | Revise to improve question flow and structure, and to be more conversational. |
| Round 4 Results. | |||||
| How easy is it to access your primary care provider or other medical professionals for your health and well-being? | 5.5 ± 0.8 | 83.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| How easy is it to navigate the healthcare system? On your own? | 4.7 ± 0.8 | 83.0% | 5.2 ± 1.0 | 67.0% | Revise to a singular question. |
| Do you have health insurance? (Y/N) | 6.0 ± 0.4 | 100.0% | 6.0 ± 0.4 | 100.0% | Validated. |
| What is your experience with your use of health insurance? | 4.8 ± 1.2 | 67.0% | 5.3 ± 1.0 | 67.0% | Revise to a sub-question of previous item. |
| Have you ever gone without medication or medical care due to concerns of cost? | 5.3 ± 1.0 | 67.0% | 5.7 ± 0.5 | 100.0% | Revise to be more open-ended, with a follow up sub-question. |
| How well do you understand topics when discussing health issues or when given resources by healthcare professionals? | 5.2 ± 1.0 | 67.0% | 5.5 ± 0.8 | 83.0% | Revise to be more conversational. |
| Tell me a little about the education of relatives or those who live with you. | 5.0 ± 1.3 | 67.0% | 5.2 ± 1.0 | 67.0% | Eliminated. |
| How do you feel about the quality of schooling you have received? | 5.4 ± 1.0 | 67.0% | 5.4 ± 1.0 | 67.0% | Revise to be more conversational. |
| What are your thoughts and plans for your education in the future? | 4.8 ± 1.2 | 67.0% | 4.8 ± 1.2 | 67.0% | Revise to be more inclusive of all career paths post-secondary school completion. |
| Is anything preventing you from additional educational opportunities? If so, please elaborate. | 5.3 ± 1.0 | 67.0% | 5.3 ± 1.0 | 67.0% | Revise to be more conversational. |
| How does language influence your interactions in school? | 5.2 ± 1.2 | 83.0% | 5.2 ± 1.2 | 83.0% | Validated. |
| Describe your financial situation. | 4.8 ± 1.3 | 50.0% | 4.8 ± 1.1 | 33.0% | Eliminated. |
| Branch Question for following sub question: Recently, or in the past, what concerns, if any, have you had about: | |||||
| b. Having your power shut off? | 5.3 ± 0.8 | 83.0% | 5.5 ± 0.6 | 100.00% | Validated. |
| Has your family had any experience worrying about paying monthly bills? | 5.7 ± 0.5 | 100.0% | 5.8 ± 0.4 | 100.00% | Validated. |
| Has your family had any experience with difficulty affording your clothes and food? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| Has your family had any experience with difficulty affording recreational activities? (i.e., Sports outside of school teams, musical instrument lessons, etc.) | 5.3 ± 1.0 | 67.0% | 5.2 ± 1.0 | 67.0% | No revisions to be made—argument: Recreation/sport activity contributes to enhancement of quality of life. |
| Has your family had trouble accessing a grocery store or other markets where you live to get nutritious food? | 5.5 ± 0.8 | 83.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| How does language influence your interactions in social settings? | 5.5 ± 0.8 | 83.0% | 5.3 ± 1.0 | 67.0% | Revise to be more conversational and more reflective of question intention. |
| Branch Question for following sub questions: For the following questions, think about your experiences with support systems. How is your relationship with the following people: | |||||
| a. Your family members/guardians? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | Validated. |
| b. Your peers? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | Validated. |
| c. Your neighbors? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | Validated. |
| d. Your teachers/coaches/other adult figures? | 5.3 ± 0.8 | 83.0% | 5.2 ± 1.1 | 50.0% | Revise to be more conversational. |
| e. Your athletic trainer? | 5.3 ± 0.8 | 83.0% | 5.2 ± 1.0 | 83.0% | Revise to be more quality improvement focused. |
| Round 5 Results. | |||||
| How easy is it to navigate the healthcare system on your own? | 5.2 ± 1.0 | 67.0% | 5.2 ± 1.0 | 67.0% | Revise to be more conversational and address target population. |
| If not, does that impact whether you go to the doctor or not? | 5.0 ± 0.0 | 100.0% | 5.2 ± 0.4 | 100.0% | Validated. |
| Have you ever felt like you’ve gone without medical care? | 5.0 ± 0.8 | 67.0% | 5.3 ± 0.8 | 83.0% | No revisions made— argument: avoidance of healthcare can be an indicator of lack of access. |
| If so, why do you think that has happened? | 5.2 ± 0.4 | 100.0% | 5.0 ± 0.6 | 100.0% | Validated. |
| How easy is it to talk about your health with healthcare providers? | 5.0 ± 0.9 | 67.0% | 5.3 ± 0.8 | 83.0% | Revise to be more direct, with a follow up sub-question. |
| Are you satisfied with the quality of schooling you’ve had? If not, can you explain? | 4.7 ± 1.2 | 50.0% | 5.0 ± 0.9 | 67.0% | Eliminated. |
| Do you have thoughts and plans for any future education? If so, can you explain? | 4.8 ± 1.2 | 67.0% | 5.0 ± 0.9 | 67.0% | Revise to be more conversational. |
| Is anything preventing you from achieving your future education? If so, can you tell me more? | 5.3 ± 1.0 | 67.0% | 5.3 ± 1.0 | 67.0% | No revisions made— argument: higher education has a direct impact on health. |
| Has your family had any experience with difficulty affording recreational activities (i.e., sports outside of school teams, musical instrument lessons, etc.)? | 5.3 ± 1.2 | 83.0% | 5.2 ± 1.0 | 67.0% | Revise to be more conversational. |
| How does language influence your interactions in different social support systems? | 4.7 ± 1.0 | 67.0% | 5.0 ± 0.9 | 67.0% | Revise to be more specific. |
| Branch Question for following sub question: For the following questions, think about your experiences with support systems. How is your relationship with the following people: | |||||
| d. Adult figures at school? | 4.5 ± 0.9 | 67.0% | 4.45 ± 0.9 | 67.0% | Revise to provide examples. |
| Is there anything I could do to make managing your health easier? | 5.3 ± 0.8 | 83.0% | 5.3 ± 0.8 | 83.0% | Validated. |
| Round 6 Results. | |||||
| Have you ever felt like you’ve gone without medical care? | 5.2 ± 1.6 | 83.3% | 5.2 ± 1.3 | 66.7% | Revise to be more specific. |
| (If not addressed in the above response) Was cost an issue? Was quality of care an issue? | 5.6 ± 0.6 | 83.3% | 5.0 ± 1.3 | 66.7% | Revise to multiple sub-questions. |
| Is it easy to discuss your health with healthcare providers? If not, why? | 5.0 ± 1.6 | 83.3% | 5.0 ± 1.6 | 83.3% | Validated. |
| What are you thinking of doing after you finish high school? | 5.0 ± 1.7 | 66.7% | 5.0 ± 1.7 | 66.7% | Revise to provide examples. |
| Is anything preventing you from achieving any future education plans? If so, can you tell me more? | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | Validated. |
| Has your family had difficulty affording recreational activities? (i.e., sports outside of school teams, musical instrument lessons, etc.) | 5.3 ± 1.0 | 66.7% | 5.3 ± 1.0 | 66.7% | Revise to be more specific, with follow up sub-questions addressing specific reasons. |
| Do language barriers affect your ability to talk to people who support you? | 5.3 ± 1.2 | 83.3% | 5.7 ± 0.8 | 83.3% | Validated. |
| Branch Question for following sub question: For the following questions, think about your experiences with support systems. How is your relationship with the following people: | |||||
| d. Adults at school, like teachers or coaches? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.8 | 83.3% | Validated. |
| Round 7 Results. | |||||
| Was there ever a time where you needed medical care but did not get it? | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | Validated. |
| (If not addressed in the above response) Was cost an issue? | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | Validated. |
| (If not addressed in the above response) Was quality of care an issue? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| What do you expect your next step to be after you finish high school (school, job, military, etc.)? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| Was there ever a recreational activity (i.e., sports outside of school teams, musical instrument lessons, etc.) that you wanted to do but couldn’t? | 5.7 ± 0.5 | 100.0% | 5.8 ± 0.4 | 100.0% | Validated. |
| If yes, was it due to any of the following? (Explain/choose all that apply.) (Cost, Transportation, Scheduling, Other.) | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | Validated. |
References
- Prevention CfDCa. About Social Determinants of Health US Department of Health and Human Services. Available online: https://www.cdc.gov/socialdeterminants/about.html (accessed on 26 October 2022).
- Services UDoHaH. Social Determinants of Health. Office of Disease Prevention and Health Promotion. Healthy People 2030 Web Site. Available online: https://health.gov/healthypeople/objectives-and-data/social-determinants-health (accessed on 20 August 2021).
- Picha, K.J.; Welch Bacon, C.E.; Normore, C.; Snyder Valier, A.R. Social determinants of health: Considerations for athletic health care. J. Athl. Train. 2022, 57, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Freiburger, R.; Picha, K.; Bacon, C.E.W.; Valier, A.R.S. Educational technique: Incorporating social determinants of health into athletic training education. Athl. Train. Ed. J. 2020, 15, 321–330. [Google Scholar] [CrossRef]
- Nair, L.; Adetayo, O.A. Cultural competence and ethnic diveristy in healthcare. J. Am. Soc. Plast. Surg. 2019, 7, e2219. [Google Scholar]
- Flaskerud, J.H.; DeLilly, C.R. Social determinants of health status. Issues Ment. Health Nurs. 2012, 33, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Schoenthaler, A.; Hassan, I.; Fiscella, K. The time is now: Fostering relationship-centered discussions about patients’ social determinants of health. Patient Educ. Couns. 2019, 102, 810–814. [Google Scholar] [CrossRef]
- World Health Organization. A Conceptual Framework for Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2010; pp. 1–76.
- Plamondon, K.M.; Bottorff, J.L.; Caxaj, C.S.; Graham, I.D. The integration of evidence from the comission on social determinants of health in the field of health equity: A scoping review. Crit. Public Health 2020, 30, 415–428. [Google Scholar] [CrossRef]
- Clayton, S.; Chin, T.; Blackburn, S.; Echeverria, C. Different setting, different care: Integrating prevention and clincial care in school-based health centers. Am. J. Public Health 2010, 100, 1592–1597. [Google Scholar] [CrossRef]
- Friedman, N.L.; Banegas, M.P. Towards addressing social determinants of health: A health care system strategy. Perm. J. 2018, 22, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.J.; Wade, T.J.; Pan, W.; Keller, K.N. School-based health centers: Cost-benefit analysis and impact on health care disparities. Am. J. Public Health 2010, 100, 1617–1625. [Google Scholar] [CrossRef]
- World Health Organization. How Health Systems Can Address Health Inequities Linked to Migration and Ethnicity. WHO Regional Office for Europe: Geneva, Switzerland, 2010; pp. 1–35. [Google Scholar]
- O’Brien, K.H. Social determinants of health: The how, who, and where screenings are occurring; a systematic review. Soc. Work Health Care 2019, 58, 719–745. [Google Scholar] [CrossRef]
- Marra, J.; Covassin, T.; Shingles, R.R.; Canady, R.B.; Mackowiak, T. Assessment of certified athletic trainers’ levels of cultural competence in the delivery of health care. J. Athl. Train. 2010, 45, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Canter, D.S.; Randolph, S.; Molloy, M.A.; Carter, B.; Cary, M.P. Student-developed simulations: Enhancing cultural awareness and understanding social determinants of health. J. Nurs. Educ. 2017, 56, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Nynas, S.M. The assessment of athletic training students’ knowledge and behavior to provide culturally competent care. Athl. Train. Educ. J. 2015, 10, 82–90. [Google Scholar] [CrossRef] [Green Version]
- Seeleman, C.; Hermans, J.; Lamkaddem, M.; Suurmond, J.; Stronks, K.; Essink-Bot, M.L. A students’ survey of cultural competence as a basis for identifying gaps in the medical cirriculum. BMC Med. Educ. 2014, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, S.M.; Willis-Esqueda, C.; Newton, D.; Sivasubramaniam, D.; Paradies, Y. The challenge of cultural competence in the workplace: Perspectives of healthcare providers. BMC Health Serv. Res. 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.M.; de Saxe Zerden, L. Prevention, health promotion, and social work: Aligning healht and human service systems through a workforce for health. AJPH 2020, 110. [Google Scholar] [CrossRef]
- Drevdahl, D.J.; Canales, M.K.; Dorcy, K.S. Of goldfish tanks and moonlight tricks. Adv. Nurs. Sci. 2008, 13, 13–27. [Google Scholar] [CrossRef]
- Brach, C.; Fraserirector, I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med. Care Res. Rev. 2000, 57, 181–217. [Google Scholar] [CrossRef]
- Loudon, R.F.; Anderson, P.; Gill, P.S.; Greenfield, S.M. Educating medical students for work in culturally diverse societies. J. Am. Med. Assoc. 1999, 282, 875–880. [Google Scholar] [CrossRef]
- Downs, K.C.; Eberman, L.; Liscombe, B.C.; Correll, C.B.; Winkelmann, Z.K. Continuing education using infographics improves the knowledge and practice of the social determinants of health. Athl. Train. Educ. J. 2021, 56, S38. [Google Scholar]
- Downs, K.C.; Liscombe, B.C.; Eberman, L.E.; Winkelmann, Z.K. The athletic trainer’s role in screening for the social determinants of health in secondary school student-athlete patient populations. J. Athl. Train. 2021, in press. [Google Scholar]
- Drescher, M.J.; Winkelmann, Z.; Downs, K.C.; Lisombe, B.C.; Eberman, L.E. Incorporating the social determinants of health in healthcare delivery among secondary school athletic trainers. J. Athl. Train. 2021, 56, S209. [Google Scholar]
- Klein, M.D.; Kahn, R.S.; Baker, R.C.; Fink, E.E.; Parrish, D.S.; White, D.C. Training in social determinants of health in primary care: Does it change resident behavior? Acad. Pediatr. 2011, 11, 387–393. [Google Scholar] [CrossRef]
- Lax, Y.; Bathory, E.; Braganza, S. Pediatric primary care and subspecialist providers’ comfort, attitudes, and practices screening and referring for social determinants of health. BMC Health Serv. Res. 2021, 21, 956. [Google Scholar] [CrossRef]
- The Accountable Health Communities Health-Related Social Needs Screening Tool. Available online: https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf (accessed on 9 January 2022).
- Foundation, A. Social Needs Screening Tool. American Academy of Family Physicians 2018, the EveryONE Project. Available online: https://www.aafp.org/dam/AAFP/documents/patient_care/everyone_project/hops19-physician-form-sdoh.pdf (accessed on 13 August 2022).
- Chung, E.K.; Siegel, B.S.; Garg, A.; Conroy, K.; Gross, R.S.; Long, D.A.; Lewis, G.; Osman, C.J.; Jo Messito, M.; Wade, R., Jr.; et al. Screening for social determinants of health among children and families living in poverty: A guide for clinicians. Curr. Probl. Pediatr. Adolesc. Health Care 2016, 46, 135–153. [Google Scholar] [CrossRef] [PubMed]
- O’Gurek, D.T.; Henke, C. A practical approach to screening for social determinants of health. Fam. Pr. Manag. 2018, 25, 7–12. [Google Scholar]
- Garg, A.; Boynton-Jarrett, R.; Dworkin, P.H. Avoiding the unintended consequences of screening for social determinants of health. J. Am. Med. Assoc. 2016, 316, 813–814. [Google Scholar] [CrossRef]
- Naz, A.; Rosenberg, E.; Andersson, N.; Labonte, R.; Andermann, A. Health workers who ask about social determinants of health are more likely to report helping patients. Can. Fam. Physician 2016, 62, 474–484. [Google Scholar]
- Garg, A.; Butz, A.; Dworkin, P.H.; Lewis, R.A.; Thompson, R.E.; Serwint, J.R. Improving the management of family psychosocial problems at low-income children’s well-child care visits: The WE CARE project. Pediatrics 2007, 120, 547–558. [Google Scholar] [CrossRef]
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J. Adv. Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef] [PubMed]
- McMillan, S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Keeney, S.; Hasson, F.; McKenna, H. A critical review of the Delphi technique as a research methodology for nursing. Int. J. Nurs. Stud. 2001, 38, 195–200. [Google Scholar] [CrossRef]
- Almanasreh, E.; Moles, R.; Chen, T.F. Evaluation of methods for estimating content validity. RSAP 2019, 15, 214–221. [Google Scholar]
- Taylor, E. We agree don’t we? The delphi method for health environments research. Methodology 2020, 13, 11–23. [Google Scholar] [CrossRef]
- Services UDoHH. Social Determinants of Health: Know What Affects Health. Published 2021. Updated 9 March 2021. Available online: https://www.cdc.gov/socialdeterminants/index.htm (accessed on 16 December 2021).
- Holey, E.A.; Feeley, J.; Dixon, J.; Whittaker, V.J. An exploration of the use of simple statistics to measure consensus and stability in Delphi studies. BMC Med. Res. Methodol. 2007, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Santaguida, P.; Dolovich, L.; Oliver, D.; Lamarche, L.; Gilsing, A.; Griffith, L.E.; Richardson, J.; Mangin, D.; Kastner, M.; Raina, P. Protocol for a Delphi consensus exercise to identify a core set of criteria for selecting health related outcome measures (HROM) to be used in primary health care. BMC Fam. Pract. 2018, 19, 1–14. [Google Scholar] [CrossRef]
- Von der Gracht, H.A. Consensus measurement in Delphi studies review and implications for future quality assurance. Technol. Forecast. Soc. Change 2012, 79, 1525–1536. [Google Scholar] [CrossRef]
- Centers NAoCH. PRAPARE: Protocol for Responding to and Assessing Aptient Assets, Risks, and Experiences; National Association of Community Health Centers: OR, USA, 2016; Available online: https://www.molinahealthcare.com/-/media/Molina/PublicWebsite/PDF/Providers/ky/medicaid/PRAPARE-Protocol-for-Responding-to-and-Assessing-Patient-Assets-Risks-and-Experiences.pdf (accessed on 24 August 2021).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Morgenlander, M.A.; Tyrrell, H.; Garfunkel, L.C.; Serwint, J.R.; Steiner, M.J.; Schilling, S. Screening for social determinants of health in pediatric resident continuity clinic. Am. Ped. 2019, 19, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Gurewich, D.; Garg, A.; Kressin, N.R. Addressing social determinants of health within healthcare delivery systems: A framework to ground and inform health outcomes. J. Gen. Intern. Med. 2020, 35, 1571–1575. [Google Scholar] [CrossRef] [PubMed]
- Riley, M.; Laurie, A.R.; Plegue, M.A.; Richardson, C.R. The adolscent “expanded medical home”: School-based health centers partner with a primary care clinic to improve population health and mitigate social determinants of health. J. Am. Board Fam. Med. 2016, 29, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokol, R.L.; Ammer, J.; Stein, S.F.; Trout, P.; Mohammed, L.; Miller, A.L. Provider perspectives on screening for social determinants of health in pediatric settings: A qualitative study. J. Pediatr. Health Care 2021, 35, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, N.; Adib-Hajbaghery, M.; Najafi, M. Cultural competence in nursing: A concept analysis. Int. J. Nurs. Stud. 2019, 99, 1–8. [Google Scholar] [CrossRef]
- Garg, A.; Toy, S.; Tripodis, Y.; Silverstein, M.; Freemen, E. Addressing social determinants of health at well child care visits: A cluster RCT. Pediatrics 2015, 135, e296–e304. [Google Scholar] [CrossRef] [Green Version]
- Byhoff, E.; Garg, A.; Pellicer, M.; Diaz, Y.; Yoon, G.H.; Charns, M.P.; Drainoni, M.L. Provider and staff feedback on screening for social and behavioral deterinants of health for pediatric patients. J. Am. Board Fam. Med. 2019, 32, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Morone, J. An integrative review of social determinants of health assessment and screening tools used in pediatrics. J. Pediatr. Nurs. 2017, 37, 22–28. [Google Scholar] [CrossRef]
- LaForge, K.; Gold, R.; Cottrell, E.; Bunce, A.E.; Proser, M.; Hollombe, C.; Dambrun, K.; Cohen, D.J.; Clark, K.D. How 6 organizations developed tools and processes for social determinants of health screening in primary care. J. Ambul. Care Manag. 2018, 41, 2–14. [Google Scholar] [CrossRef]
- California University of San Francisco. WE CARE Survey. San Francisco., United States. Published 2022. Available online: https://sirenetwork.ucsf.edu/sites/default/files/HL%20BMC%20Screening%20Tool%20final%20%28English%29.pdf (accessed on 28 May 2022).
- Coulombe, B.J.; Games, K.; Eberman, L.E. The use of patient-reported outcome measures in secondary school athletic trainers’ perceptions, practices, and barriers. J. Athl. Train. 2019, 54, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Bacon, C.E.W.; Eppelheimer, B.L.; Kasamatsu, T.M.; Lam, K.C.; Nottingham, S.L. Athletic trainers’ perceptions of and barriers to patient care documentation: A report from the athletic training practice-based research network. J. Athl. Train. 2017, 52, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Adermann, A. Taking action on the social determinants of health in clinical practice: A framework for health professionals. CMAJ 2016, 188, E474–E483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.C.; Harrington, K.M.; Cameron, K.L.; Valier, A.R.S. Use of patient-reported outcome measures in athletic training: Common measures, selection considerations, and practical barriers. J. Athl. Train. 2019, 54, 449–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjerdingen, D.K.; Yawn, B.P. Postpartum depression screening: Importance, methods, barriers, and recommendations for practice. J. Am. Board Fam. Med. 2007, 20, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeely, J.; Kumar, P.C.; Rieckmann, T.; Sedlander, E.; Farkas, S.; Chollak, C.; Kannry, J.L.; Vega, A.; Waite, E.A.; Peccoralo, L.A.; et al. Barriers and facilitators affecting the implementation of substance use screening in primary care clinics: A qualitative study of patients, providers, and staff. Addict. Sci. Clin. Pr. 2018, 13, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahan, S.; Manson, J. Nutrition counseling in clinical practice: How clinicans can do better. JAMA 2017, 318, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.; Persaud, S. Preparing today’s nurses: Social determinants of health and nursing education. OJIN 2018, 23. [Google Scholar] [CrossRef]
- Denizard-Thompson, N.; Palakshappa, D.; Vellevand, A.; Kundu, D.; Brooks, A.; DiGiacobbe, G. Association of a health equity cirriculum with medical students’ knowledge of social determinants of health and confidence in working with underserved populations. JAMA New Open 2021, 4, 1–11. [Google Scholar]
- Peer, K.S.; McClendon, R.C. Sociocultural learning theory in practice: Implications for athletic training educators. J. Athl. Train. 2002, 37, S136–S140. [Google Scholar]
- Issenberg, S.B.; McGaghie, W.C.; Petrusa, E.R.; Gordon, D.L.; Scalese, R.J. Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med. Teach. 2005, 27, 10–28. [Google Scholar] [CrossRef]
- May, W.; Park, J.H.; Lee, J.P. A ten-year review of the literature on the use of standardized patients in teaching and learning: 1996–2005. Med. Teach. 2009, 31, 487–492. [Google Scholar] [CrossRef]
- Committee, I.S. INACSL standards of best practice: Simulation. Clin. Simul. Nurs. 2016, 12, S16–S20. [Google Scholar]
- Stegeman, C.A.; Zydney, J. Effectiveness of multimedia instruction in health professions education compared to traditional instruction in health professions education compared to traditional instruction. J. Dent. Hyg. 2010, 84, 130–136. [Google Scholar] [PubMed]

| Panelist | Years of Experience | Contemporary Qualifications in SDOH | Work Area(s) | Patient Care Setting |
|---|---|---|---|---|
| A | 4.5 | College of public health Master’s degree Research in Healthcare and Social Justice, cultural competency Presenter at various professional conferences | Athletic Trainer | Secondary-Level School-Based Sports Medicine Collegiate-Level School-Based Sports Medicine |
| B | 14 | Research in rural & minority health populations, psychosocial determinants of health Recipient of National Institute of Health (NIH) funding for Minority Health and Health Disparities (HHD) HHD grant reviewer | Neurosurgical ICU/Stroke Rehabilitation Unit RN Professor | Hospital (In-patient) |
| C | 18 | Research in rural health, SDOH, health policy, health equity Case managing and community organizing focused on housing/mental health | Social services Outpatient psychiatry Professor Rural health research center | Hospital (Outpatient) |
| D | 23 | Health Care Alliance Board Member Access to Care Workgroup member for 8+ years Resilience Leader Medical/Dental Sector for New Mexico Part of Adverse Childhood Experiences (ACEs) initiative 2+ years SDOH PPE Event 11+ years | Athletic Trainer PT/AT/OT private practice CEO | Professional Sports Secondary-Level School-Based Sports Medicine Collegiate- Level School-Based Sports Medicine |
| E | 9 | Post-doctoral fellowship completing extensive SDOH research New Investigator Grant recipient for SDOH in athletic healthcare Presenter at various professional conferences | Athletic Trainer Professor | Secondary-Level School-Based Sports Medicine Collegiate-Level School-Based Sports Medicine PT clinic |
| F | 26 | 13+ years of community based coalition work within urban health disparities/obesity initiatives Worksite/university campus wellness Diversity, equity, and inclusion coalition work | Athletic Trainer Community outreach educator Professor | Secondary-Level School-Based Sports Medicine Collegiate-Level School-Based Sports Medicine |
| Reflecting Current Evidence | Script Inclusion | ||||
|---|---|---|---|---|---|
| Item | Mean ± SD | Percent Agreement | Mean ± SD | Percent Agreement | Round Validated: |
| Do you have a primary care provider, such as a family physician or nurse practitioner? (Y/N) | 6.0 ± 0.0 | 100.0% | 5.8 ± 0.8 | 100.0% | 3 |
| How easy is it to access your primary care provider or other medical professionals for your health and well-being? | 5.5 ± 0.8 | 83.0% | 5.8 ± 0.4 | 100.0% | 4 |
| How often (annually, for illness only, etc.) do you see your primary care provider? | 5.3 ± 1.2 | 83.3% | 5.3 ± 1.2 | 83.3% | 3 |
| Do you have health insurance? (Y/N) | 6.0 ± 0.4 | 100.0% | 6.0 ± 0.4 | 100.0% | 4 |
| If not, does that impact whether you go to the doctor or not? | 5.0 ± 0.0 | 100.0% | 5.2 ± 0.4 | 100.0% | 5 |
| Was there ever a time where you needed medical care but did not get it? | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | 7 |
| If so, why do you think that has happened? | 5.2 ± 0.4 | 100.0% | 5.0 ± 0.6 | 100.0% | 5 |
| (If not addressed in the above response) Was cost an issue? | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | 7 |
| (If not addressed in the above response) Was quality of care an issue? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | 7 |
| Is it easy to discuss your health with healthcare providers? If not, why? | 5.0 ± 1.6 | 83.3% | 5.0 ± 1.6 | 83.3% | 6 |
| Describe how language influences your interactions in healthcare settings. | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | 3 |
| What is your family’s level of education? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.8 | 83.3% | 3 |
| What do you expect your next step to be after you finish high school (school, job, military, etc.)? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | 7 |
| Is anything preventing you from achieving any future education plans? If so, can you tell me more? | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | 6 |
| How does language influence your interactions in school? | 5.2 ± 1.2 | 83.0% | 5.2 ± 1.2 | 83.0% | 4 |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Being evicted (forced out of where you live) or becoming homeless? | 5.5 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | 3 |
| b. Having your power shut off? | 5.3 ± 0.8 | 83.0% | 5.5 ± 0.6 | 100.0% | 4 |
| Has your family had any experience worrying about paying monthly bills? | 5.7 ± 0.5 | 100.0% | 5.8 ± 0.4 | 100.0% | 4 |
| Has your family had any experience with difficulty affording your clothes and food? | 5.8 ± 0.4 | 100.0% | 5.8 ± 0.4 | 100.0% | 4 |
| Was there ever a recreational activity (i.e., sports outside of school teams, musical instrument lessons, etc.) that you wanted to do but couldn’t? | 5.7 ± 0.5 | 100.0% | 5.8 ± 0.4 | 100.0% | 7 |
| If yes, was it due to any of the following? (Explain/choose all that apply.) (Cost, Transportation, Scheduling, Other.) | 6.0 ± 0.0 | 100.0% | 6.0 ± 0.0 | 100.0% | 7 |
| Describe your living situation. | 5.2 ± 0.8 | 83.3% | 5.3 ± 0.8 | 83.3% | 3 |
| Has your family had trouble accessing a grocery store or other markets where you live to get nutritious food? | 5.5 ± 0.8 | 83.0% | 5.8 ± 0.4 | 100.0% | 4 |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Having clean running water? | 5.5 ± 0.8 | 83.3% | 5.7 ± 0.5 | 100.0% | 3 |
| b. Being exposed to mold or pests where you live? | 5.7 ± 0.5 | 100.0% | 5.5 ± 0.6 | 100.0% | 3 |
| c. Feeling safe in your neighborhood? | 5.7 ± 0.5 | 100.0% | 5.7 ± 0.5 | 100.0% | 3 |
| What type(s) of transportation do you use most often (car, bus, metro, biking, walking, etc.)? | 5.3 ± 0.8 | 83.3% | 5.2 ± 0.8 | 83.3% | 3 |
| If you had an appointment or needed to get somewhere, can you describe how you might get there? | 5.7± 0.5 | 100.0% | 5.5 ± 0.8 | 83.3% | 3 |
| Tell me about the parks, sidewalks, and other green spaces that are in your neighborhood. | 5.5 ± 0.6 | 100.0% | 5.3 ± 0.8 | 83.3% | 3 |
| Branch Question for following sub questions: Recently, or in the past, what concerns, if any, have you had about: | |||||
| a. Abuse in the home (physical, verbal, emotional)? | 5.5 ± 0.8 | 83.0% | 5.3 ± 0.5 | 100.0% | 3 |
| b. Family members getting arrested? | 5.7 ± 0.5 | 100.0% | 5.3 ± 0.5 | 100.0% | 3 |
| c. Feeling lonely and isolated from your friends and family? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.6 | 100.0% | 3 |
| d. Being discriminated against for any reason? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.6 | 100.0% | 3 |
| Do language barriers affect your ability to talk to people who support you? | 5.3 ± 1.2 | 83.3% | 5.7 ± 0.8 | 83.3% | 6 |
| How would you describe your faith, spirituality, or religious beliefs? | 5.3 ± 0.8 | 83.3% | 5.3 ± 0.5 | 100.0% | 3 |
| Branch Question for following sub question: For the following questions, think about your experiences with support systems. How is your relationship with the following people: | |||||
| a. Your family members/guardians? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | 4 |
| b. Your peers? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | 4 |
| c. Your neighbors? | 5.7 ± 0.8 | 83.0% | 5.7 ± 0.8 | 83.0% | 4 |
| d. Adult at school, like teachers or coaches? | 5.5 ± 0.8 | 83.3% | 5.5 ± 0.8 | 83.3% | 6 |
| Is there anything I could do to make managing your health easier? | 5.3 ± 0.8 | 83.0% | 5.3 ± 0.8 | 83.0% | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giorgi, E.M.; Drescher, M.J.; Winkelmann, Z.K.; Eberman, L.E. Validation of a Script to Facilitate Social Determinant of Health Conversations with Adolescent Patients. Int. J. Environ. Res. Public Health 2022, 19, 14810. https://doi.org/10.3390/ijerph192214810
Giorgi EM, Drescher MJ, Winkelmann ZK, Eberman LE. Validation of a Script to Facilitate Social Determinant of Health Conversations with Adolescent Patients. International Journal of Environmental Research and Public Health. 2022; 19(22):14810. https://doi.org/10.3390/ijerph192214810
Chicago/Turabian StyleGiorgi, Emily M., Matthew J. Drescher, Zachary K. Winkelmann, and Lindsey E. Eberman. 2022. "Validation of a Script to Facilitate Social Determinant of Health Conversations with Adolescent Patients" International Journal of Environmental Research and Public Health 19, no. 22: 14810. https://doi.org/10.3390/ijerph192214810