
Secondary School Athletic Trainers’ Navigation of Patient Socioeconomic Status Challenges in Care: A Qualitative Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Procedures and Instrumentation
2.3. Participants and Sampling
2.4. Data Analysis
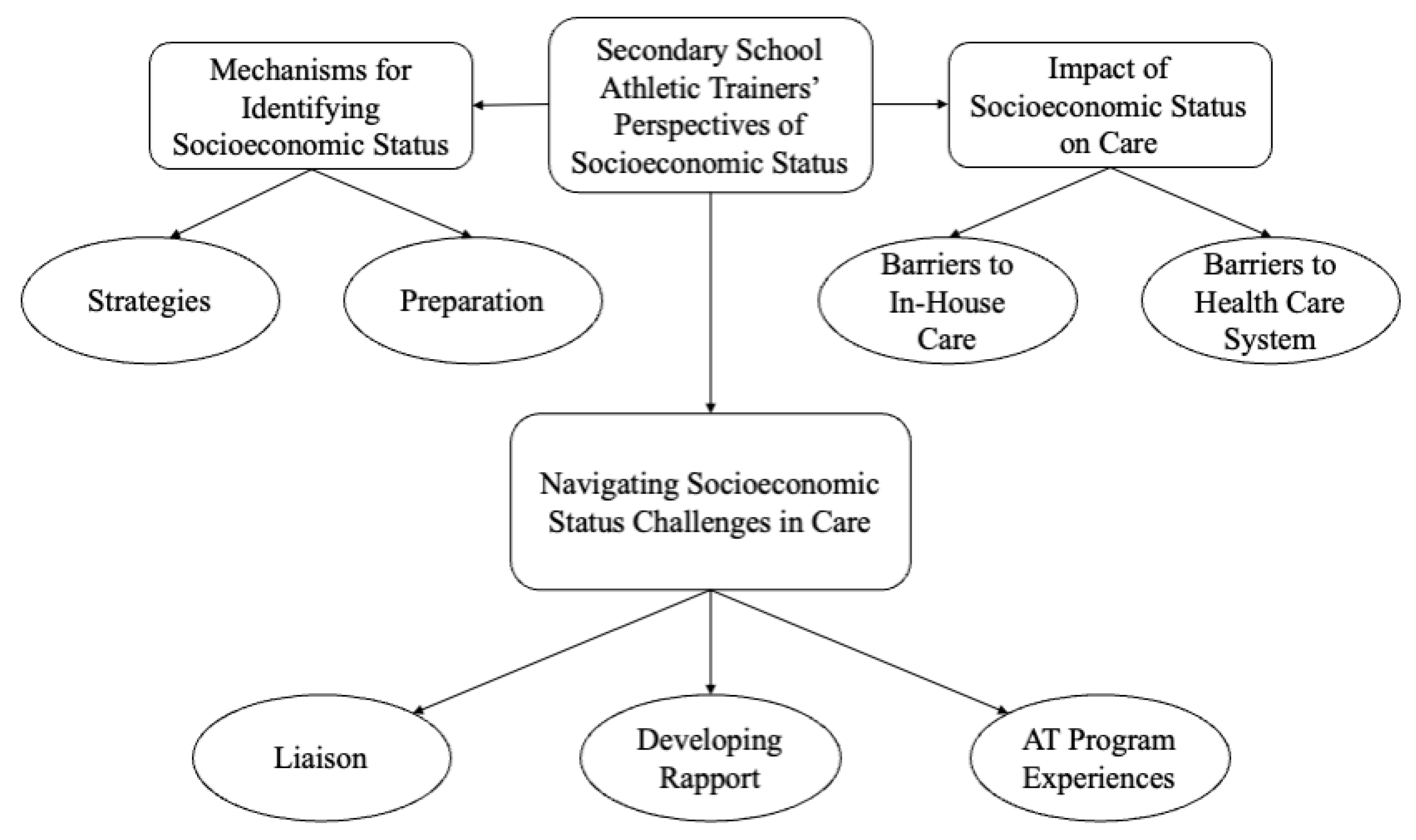
3. Results
4. Discussion
4.1. Mechanisms for Identifying Socioeconomic Status
4.2. Impact of Socioeconomic Status on Care
4.3. Navigating Socioeconomic Status Challenges in Care
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andermann, A.; Collaboration, C. Taking action on the social determinants of health in clinical practice: A framework for health professionals. CMAJ 2016, 188, E474–E483. [Google Scholar] [CrossRef] [Green Version]
- Adler, N.E.; Newman, K. Socioeconomic disparities in health: Pathways and policies. Health Aff. (Millwood) 2002, 21, 60–76. [Google Scholar] [CrossRef]
- Arpey, N.C.; Gaglioti, A.H.; Rosenbaum, M.E. How Socioeconomic Status Affects Patient Perceptions of Health Care: A Qualitative Study. J. Prim. Care Community Health 2017, 8, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Bernheim, S.M.; Ross, J.; Krumholz, H.M.; Bradley, E.H. Influence of patients’ socioeconomic status on clinical management decisions: A qualitative study. Ann. Fam. Med. 2008, 6, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Willems, S.; De Maesschalck, S.; Deveugele, M.; Derese, A.; De Maeseneer, J. Socio-economic status of the patient and doctor-patient communication: Does it make a difference? Patient Educ. Couns. 2005, 56, 139–146. [Google Scholar] [CrossRef] [Green Version]
- DeSalvo, K.B.; Wang, Y.C.; Harris, A.; Auerbach, J.; Koo, D.; O’Carroll, P. Public Health 3.0: A Call to Action for Public Health to Meet the Challenges of the 21st Century. Prev. Chronic Dis. 2017, 14, E78. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.R.; Costa, M.V.; Odunlami, A.O.; Mohammed, S.A. Moving upstream: How interventions that address the social determinants of health can improve health and reduce disparities. J. Public Health Manag. Pract. 2008, 14, S8–S17. [Google Scholar] [CrossRef]
- Naz, A.; Rosenberg, E.; Andersson, N.; Labonté, R.; Andermann, A.; CLEAR Collaboration. Health workers who ask about social determinants of health are more likely to report helping patients. Mix.-Methods Study 2016, 62, e684–e693. [Google Scholar]
- Hoffman, M.A.; Johnson, S.T.; Norcross, M.F. The Intersection of Athletic Training and Public Health. J. Athl. Train. 2019, 54, 121. [Google Scholar] [CrossRef] [Green Version]
- Turnock, B. Public Health; Jones & Bartlett Publishers: Burlington, MA, USA, 2012. [Google Scholar]
- National Center for Education Statistics. Concentration of Public School Students Eligible for Free or Reduced-Price Lunch. Condition of Education. U.S. Department of Education, Institute of Education Sciences. 2022. Available online: https://nces.ed.gov/programs/coe/indicator/clb (accessed on 13 May 2022).
- Post, E.; Winterstein, A.P.; Hetzel, S.J.; Lutes, B.; McGuine, T.A. School and Community Socioeconomic Status and Access to Athletic Trainer Services in Wisconsin Secondary Schools. J. Athl. Train. 2019, 54, 177–181. [Google Scholar] [CrossRef] [Green Version]
- Barter, E.; Post, E.; Games, K.; Eberman, L.; Rivera, M. Differences in Access to Athletic Trainers in Public Secondary Schools Based on Socioeconomic Status. J. Athl. Train. 2021. [Google Scholar] [CrossRef]
- Robison, H.J.; Simon, J.E.; Nelson, E.J.; Morris, S.N.; Wasserman, E.B.; Docherty, C.L. Secondary School Socioeconomic Status and Athletic Training Practice Characteristics. J. Athl. Train. 2021, 57, 418–424. [Google Scholar] [CrossRef]
- Smith, J.A.; Shinebourne, P. Interpretative phenomenological analysis. In APA Handbook of Research Methods in Psychology; Volume 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; American Psychological Association: Washington, DC, USA, 2012; pp. 73–82. [Google Scholar]
- Pietkiewicz, I.; Smith, J. A practical guide to using Interpretative Phenomenological Analysis in qualitative research psychology. CPPJ 2014, 20, 7–14. [Google Scholar]
- Smith, J.A.; Jarman, M.; Osborn, M. Doing interpretative phenomenological analysis. Qual. Health Psychol. Theor. Methods 1999, 1, 218–240. [Google Scholar]
- Hernandez, M.; Miller, E.; Biese, K.; Columna, L.; Andreae, S.; McGuine, T.; Snedden, T.; Eberman, L.; Bell, D. Secondary School Athletic Trainers’ Clinical Management Decisions toward Low Socioeconomic Status Patients; Sam Houston State University: Huntsville, TX, USA, 2022; unpublished. [Google Scholar]
- McConnell-Henry, T.; Chapman, Y.; Francis, K. Member checking and Heideggerian phenomenology: A redundant component. Nurse Res. 2011, 18, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 2nd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2007; p. xvii, 395. [Google Scholar]
- Smith, B.; McGannon, K.R. Developing rigor in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport Exerc. Psychol. 2018, 11, 101–121. [Google Scholar] [CrossRef]
- Christensen, A.-D.; Jensen, S.Q. Doing intersectional analysis: Methodological implications for qualitative research. NORA-Nord. J. Fem. Gend. Res. 2012, 20, 109–125. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Yardley, L. Dilemmas in qualitative health research. Psychol. Health 2000, 15, 215–228. [Google Scholar] [CrossRef]
- Hill, C.E.; Knox, S.; Thompson, B.J.; Williams, E.N.; Hess, S.A.; Ladany, N. Consensual qualitative research: An update. J. Couns. Psychol. 2005, 52, 196–205. [Google Scholar] [CrossRef] [Green Version]
- McLeod, T.C.V.; Snyder, A.R.; Parsons, J.T.; Bay, R.C.; Michener, L.A.; Sauers, E.L. Using disablement models and clinical outcomes assessment to enable evidence-based athletic training practice, part II: Clinical outcomes assessment. J. Athl. Train. 2008, 43, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Haegele, J.A.; Hodge, S.R.; Filho, P.G.; Ribeiro, N.; Martínez-Rivera, C. A Phenomenological Inquiry into the Meaning Ascribed to Physical Activity by Brazilian Men with Visual Impairments. J. Vis. Impair. Blind. 2018, 112, 519–531. [Google Scholar] [CrossRef] [Green Version]
- Wynia, M.K.; VanGeest, J.B.; Cummins, D.S.; Wilson, I.B. Do physicians not offer useful services because of coverage restrictions? Health Aff. (Millwood) 2003, 22, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Bharmal, N.; Derose, K.P.; Felician, M.; Weden, M.M. Understanding the Upstream Social Determinants of Health; RAND: Santa Monica, CA, USA, 2015; pp. 1–18. [Google Scholar]
- Sharma, M.; Pinto, A.D.; Kumagai, A.K. Teaching the Social Determinants of Health: A Path to Equity or a Road to Nowhere? Acad. Med. 2018, 93, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Community Health 2003, 57, 254–258. [Google Scholar] [CrossRef]
- Picha, K.J.; Welch Bacon, C.E.; Normore, C.; Snyder Valier, A.R. Social Determinants of Health: Considerations for Athletic Health Care. J. Athl. Train. 2021, 57, 521–531. [Google Scholar] [CrossRef]
- Manchanda, R.; Gottlieb, L. Upstream Risks Screening Tool and Guide V2; HealthBegins: Los Angeles, CA, USA, 2015. [Google Scholar]
- Bigrigg, A.; Nandwani, R.; Ilett, R.; Thow, C.; Lamont, M.; Bankowska, U.; Brechin, S. Use of a staff administered structured questionnaire to identify relevant life-style issues and social-health determinants in a sexual and reproductive health service. Eur. J. Contracept. Reprod. Health Care 2005, 10, 66–72. [Google Scholar] [CrossRef]
- Behforouz, H.L.; Drain, P.K.; Rhatigan, J.J. Rethinking the social history. N. Engl. J. Med. 2014, 371, 1277–1279. [Google Scholar] [CrossRef]
- Brcic, V.; Eberdt, C.; Kaczorowski, J. Development of a tool to identify poverty in a family practice setting: A pilot study. Int. J. Fam. Med. 2011, 2011, 812182. [Google Scholar] [CrossRef] [Green Version]
- Iezzoni, L.I.; Barreto, E.A.; Wint, A.J.; Hong, C.S.K.; Donelan, K. Development and preliminary testing of the health in community survey. J. Health Care Poor Underserved 2015, 26, 134–153. [Google Scholar] [CrossRef]
- Patel, A.R.; Sarkisova, N.; Smith, R.; Gupta, K.; VandenBerg, C.D. Socioeconomic status impacts outcomes following pediatric anterior cruciate ligament reconstruction. Medicine 2019, 98, e15361. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Browne, A.J.; Varcoe, C.M.; Wong, S.T.; Smye, V.L.; Lavoie, J.; Littlejohn, D.; Tu, D.; Godwin, O.; Krause, M.; Khan, K.B.; et al. Closing the health equity gap: Evidence-based strategies for primary health care organizations. Int. J. Equity Health 2012, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Tompsett, J.; Knoester, C. The Making of a College Athlete: High School Experiences, Socioeconomic Advantages, and the Likelihood of Playing College Sports. Sociol. Sport J. 2021, 39, 129–140. [Google Scholar] [CrossRef]
- Pryor, R.R.; Casa, D.J.; Vandermark, L.W.; Stearns, R.L.; Attanasio, S.M.; Fontaine, G.J.; Wafer, A.M. Athletic training services in public secondary schools: A benchmark study. J. Athl. Train. 2015, 50, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Noel-London, K.C.; Grimsley, C.; Porter, J.; Breitbach, A.P. “The Tip of the Iceberg”: Commentary on Sports, Health Inequity, and Trauma Exacerbated by COVID-19. J. Athl. Train. 2020, 56, 5–10. [Google Scholar] [CrossRef]


{kind=link}
| 1. To begin, tell me about your background as an AT. |
| 2. What is your definition of a low SES person? |
| 3. Have you ever found yourself making assumptions about your patients because of their SES? Tell me more about that. |
| 4. In your secondary school of employment, how do you know which student athletes are of low SES? At what time point do you know their SES? How did you learn about that information? |
| 5. What experience, if any, do you have in providing care to patients who are of low SES? In what ways, in any, have those experiences changed how you view low SES patients? |
| 6. In what ways, if any, does your experience in providing care to low SES patients affect your clinical decisions as an AT? Further probe with how this changes once the patient needs advanced care/AT needs to work alongside physician |
| 7. In what ways, if any, does your experience in providing care to low SES patients affect your workload? Further probe: Does this mean more in house-care or a more conservative care plan? |
| 8. What are, if any, the challenges you have faced in providing care to low SES student athletes? Further probe: How do these challenges make you feel? |
| 9. When providing health care to low SES student athletes, what strategies do you feel have worked best for providing a high standard of care? Further probe: Why do you feel those strategies are successful? |
| 10. What are the biggest barriers, if any, your low SES student athletes face when in the health care system? |
| 11. In what ways, if any, did your ATP prepare you to provide care for low SES patient population? |
| 12. Is there anything else you would like to share about providing care to low SES student athletes in the secondary school setting? |
| Pseudonym | Sex | School Location | School Setting | Title 1 School | Highest Level of Education | Years of Clinical Experience | Race/Ethnicity |
|---|---|---|---|---|---|---|---|
| 1 | Male | Illinois | Private | No | Master’s | 30 | White |
| 2 | Male | Pennsylvania | Public | Yes | Master’s | 3 | White |
| 3 | Male | Pennsylvania | Private | No | Master’s | 6 | Hispanic, Latino, or Spanish Origin |
| 4 | Female | California | Public | No | Master’s | 19 | Hispanic, Latino, or Spanish Origin |
| 5 | Female | Kansas | Public | Yes | Master’s | 11 | White |
| 6 | Female | Arizona | Public | Yes | Master’s | 28 | White |
| 7 | Female | Pennsylvania | Public | Yes | Master’s | 7 | White |
| 8 | Female | Idaho | Public | Yes | Master’s | 6 | White |
| 9 | Female | Arizona | Public | Yes | Bachelor’s | 3 | White |
| 10 | Female | Indiana | Public | Yes | Bachelor’s | 8 | White |
| 11 | Female | Indiana | Public | Yes | Master’s | 29 | White |
| 12 | Female | Virginia | Public | No | Master’s | 4 | White |
| Category | Supporting Quotation |
|---|---|
| Strategies | “Because you got a kid that’s got a $50,000 souped out Jeep Cherokee driving in and you got another one, that’s got a small convertible that you can hear the muffler rattling or the kids that are walking home. And it’s not walking because it’s close, they’re just walking because that’s the transportation.”—P1 |
| “My biggest thing is when I can look at their physicals and I see that their insurance is either Medicaid or no insurance, or the parents will sometimes disclose to me, “we don’t have insurance, we can’t afford to go to physical therapy, can we do our rehab with you?” So, it’s a combination of that. Either seeing it on the documents or the parents of the kids disclosing it to me.”—P10 | |
| “I have conversations with coaches, teachers, my athletic director, et cetera, at the beginning of the school year, particularly for the incoming students, because the ones who are sophomores, juniors, seniors, I usually have had before, and I know them. So, I usually have conversations with those other adults about the students, and that’s typically where I get my information on their socioeconomic status.”—P8 | |
| “Most of the time the kids are forthcoming. “Like, yeah, I live in Chula Vista, which is really far away or yeah, my parents are working two jobs, or I have five siblings and my parents are working two jobs.” So, it’s kind of what other information I can gather from them without directly asking.”—P4 | |
| Preparation | “I probably got a better eye opener in my teaching education program because I was assigned to a low-income elementary school. I still remember the teacher that I went with had a lot of years of experience. She said, “This is the best meal they’re going to get.” It really explained to me that we have like 60% of our students here are very low income that come in. So, I actually got more from my student teaching part than I ever got from my athletic training part. I think that’s because you don’t have those real experiences....”—P1 |
| “I think it was more so our clinical education that allowed me to get that understanding because my very first clinical site was actually at a very rural high school. So that was kind of my first eye-opening experience of, these kids aren’t coming from a lot. These kids are getting a free and reduced lunch and sometimes that’s their only means of a meal for that day.”—P12 | |
| “Oh, it’s a rude awakening for me. I would have been prepared if I had one of my clinical rotations at this low SES site or at a similar site. I would have been like, “Okay, I can recognize which athletes are low SES and which athletes aren’t.”—P2 |
| Category | Supporting Quotation |
|---|---|
| Barriers to in-house care | “We don’t have that specialty store that some places have. Rehab stuff we’re kind of bare on. We don’t have a lot of the fancy stuff. The STIM machine came, so that helped, but it’s still kind of just getting creative with what we have.”—P12 |
| “Cross country training shoes costs $80 and $180 per pair these kids can’t afford it, but they still want to be a part of the team. I’ve seen cross country kids that have come in with holes in their shoes and that’s the only pair of shoes that they have. So, they wear them to school all day long and then they try to go do a five-mile run and they come in and you wonder why their body is hurting.”—P5 | |
| “We have a couple of kids whose parents speak very little English or are only Spanish speaking. So, I have to use the child as a translator, which I’ve learned now is not best practice. When I’m trying to convey information to the parent on how to best care for their child and using the child who we’re talking about as the translator, to me, doesn’t feel like it’s the right thing to do because you shouldn’t be using children to translate medical things. They may not understand how to appropriately translate what’s going on. My fear is that what I’m saying isn’t making it to the parents in a way that they can comprehend and understand and make an appropriate decision.”—P10 | |
| “Sometimes it’s the kids just being non-compliant with daily screenings and rehab. Sometimes it’s the families being non-compliant. “If little Bobby has a head injury and can’t practice, well he’s going to come home and babysit his siblings. So, he doesn’t need to see you. He’ll come in eventually when he feels better.”—P6 | |
| Barriers to health care system | “I think they tend to not get as good of care just based on where they geographically lived. The hospitals and clinics there are not as good as where a lot of my highest SES students live.”—P3 |
| “It’s about 20 plus miles to the nearest hospital, the nearest specialist, really the nearest health clinic essentially. So, that’s a struggle that I have to deal with where I can’t just necessarily go, “I think this person should be referred. Okay, great. I’m going to refer them.” Do they have the ability to go see this doctor if I was to refer them?”—P8 | |
| “I may need to explain to the parents that their kid may not get the MRI in two days like another kid on the team did. You know, kids talk amongst themselves. Obviously, I’m not going to share information, but I let them know that it may not be tomorrow that you get your MRI. It may be another week or so. We can help you, but the process may be a little bit different for you.”—P10 | |
| “My gut says he probably broke his scaphoid. I would’ve loved to have him get X-rayed, but the mother fought me tooth and nail. Undocumented immigrant, didn’t want to be in the system, didn’t want all that.”—P6 |
| Category | Supporting Quotation |
|---|---|
| Liaison | “There was one physician practice in town, and I had an amazing relationship with her. It was really easy to say, “Hey, so-and-so got hurt”, and she would be like, “I know that family, tell him that I’ll see them in a week if I need to see him”, or she’d be like, “I can go see him.” Sometimes it’d be like, “You know what, I’ll stop by their house tonight”, and she’d do it for free.”—P7 |
| “In many instances I play the gatekeeper for medical care. Meaning, if it was something we could take care of in house I would communicate with the parents, and they were happy with it. If it was something that I knew was out of my hands, then I would go through the resources I had available, work with our dropout prevention coordinator, refugee services on campus to get these kids seen. In a lot of instances, if the parents bought into it, you could get them the access, the state health insurance.”—P6 | |
| “My orthopedist is awesome, and I can send my kids to him if I really need it. But there are certain places and there are certain doctors that I just won’t send my kids to, because I know that first of all, they will be discriminated against because of what they look like and where they live, and they won’t take them because they wouldn’t be able to afford it.”—P9 | |
| “I’m more prepared to be able to help them with braces or crutches or things that they need. I have former athletes whose parents are cleaning out when they go away to college. And they say, “can you use this cryo cuffs? Yes. Can you use these crutches? Yes. Can you use these ankle braces? Yes.” Because I always know I have kids that can’t afford them, and we’ll be grateful for them. Especially if they’ve had previous injuries and stuff like that. I just have never turned down a hand.”—P11 | |
| Developing Rapport | “They need to understand that as an athletic trainer and a teacher that I’m not going to go running around town to tell them what you tell me. I’m a resource that you can use. I can help you. I don’t have all the answers, but at least I think being in a community long enough, I know where I can tell them to go to get the answers, to help them.”—P1 |
| “I don’t think you ever really realize a situation or what a kid is going through until you actually sit down and have that conversation with them. Being able to build that trust is huge, but it takes time. They’re not just going to automatically trust you right off the bat because of the situations that these kids come from or go through.”—P12 | |
| “I don’t think they get follow up care or personalized medical care or they get charged a bill and they get stressed about it. Instead, I say, “let’s try to avoid that. And then if we need to, we’ll do it, but I’m still going to follow up with you regardless of how this case turns out.”—P10 | |
| “I try talk to them about what I do, what I can do for their kids as an athletic trainer, and I really stress that I’m there to take care of their kids. There’s no ulterior motive or anything like that. Some of them, especially with my African American athletes and parents, have disclosed to me that they really just don’t trust doctors, or just healthcare in general, because they have been mistreated in the past.”– P9 | |
| ATP Experiences | “I think we just assumed people had the resources available to them to just do the gold standard of care, which is not the real world. Most of my experiences were in the college setting so everything was kind of in-house and taken care of. What I remember from my first rotation at that high school and what I’ve even seen now is that there are so many factors that come into the care people actually get. I don’t think we ever talked about the fear undocumented people might have going to a doctor’s office or language barriers, access to interpreters, things like that.”—P3 |
| “My only exposure to diverse populations was at this one site and I think that’s what drew me in. There wasn’t really a lot of education on certain populations or how to go about if the lower SES student can’t afford to go to get an x-ray or something like that. So, it was very eye-opening once I got to that one rotation and then once I was an independent clinician at my school.”—P9 | |
| “The collegiate level for my undergrad just focused on the athletes who were on our campus. So, every athlete is almost equal at that point because they’re living on campus or nearby campus. So, we never really explored or dove into any differences. Everybody can see doctor so-and-so. All had free reign to student health. So there never was an issue of socioeconomic status.”—P4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez, M.I.; Miller, E.C.; Biese, K.M.; Columna, L.; Andreae, S.J.; McGuine, T.; Snedden, T.; Eberman, L.; Bell, D.R. Secondary School Athletic Trainers’ Navigation of Patient Socioeconomic Status Challenges in Care: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 16709. https://doi.org/10.3390/ijerph192416709
Hernandez MI, Miller EC, Biese KM, Columna L, Andreae SJ, McGuine T, Snedden T, Eberman L, Bell DR. Secondary School Athletic Trainers’ Navigation of Patient Socioeconomic Status Challenges in Care: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(24):16709. https://doi.org/10.3390/ijerph192416709
Chicago/Turabian StyleHernandez, Mayrena Isamar, Elena Catherine Miller, Kevin Mark Biese, Luis Columna, Susan J. Andreae, Timothy McGuine, Traci Snedden, Lindsey Eberman, and David Robert Bell. 2022. "Secondary School Athletic Trainers’ Navigation of Patient Socioeconomic Status Challenges in Care: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 24: 16709. https://doi.org/10.3390/ijerph192416709