
The Social, Behavioral, and Ethical Modalities of COVID-19 on HIV Care in South Africa: A Systematic Review

 ,
,
Abstract
:1. Introduction
1.1. COVID-19 and HIV
1.2. Historical Context of HIV in South Africa
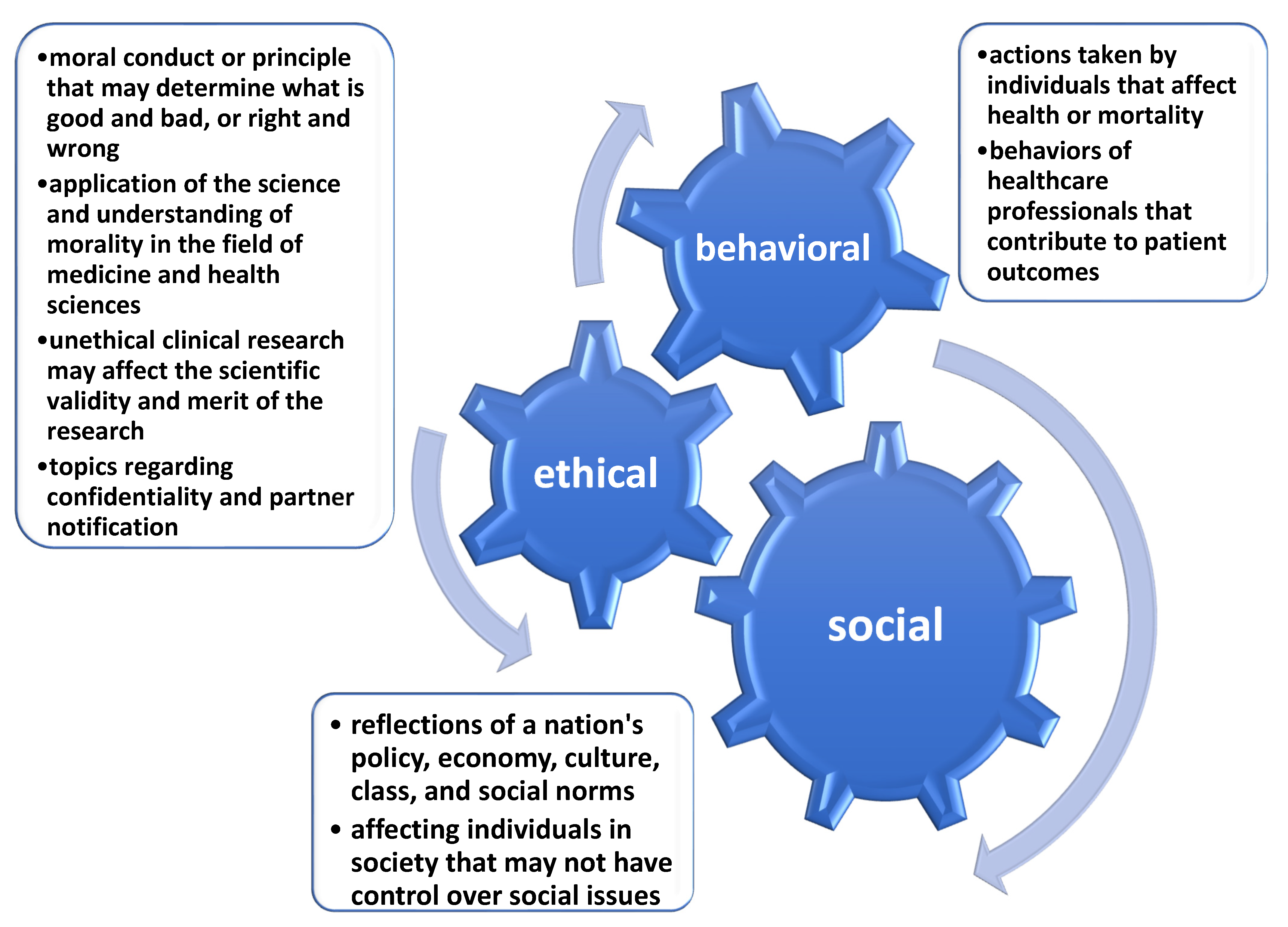
1.3. Defining Social, Behavioral, and Ethical Implications
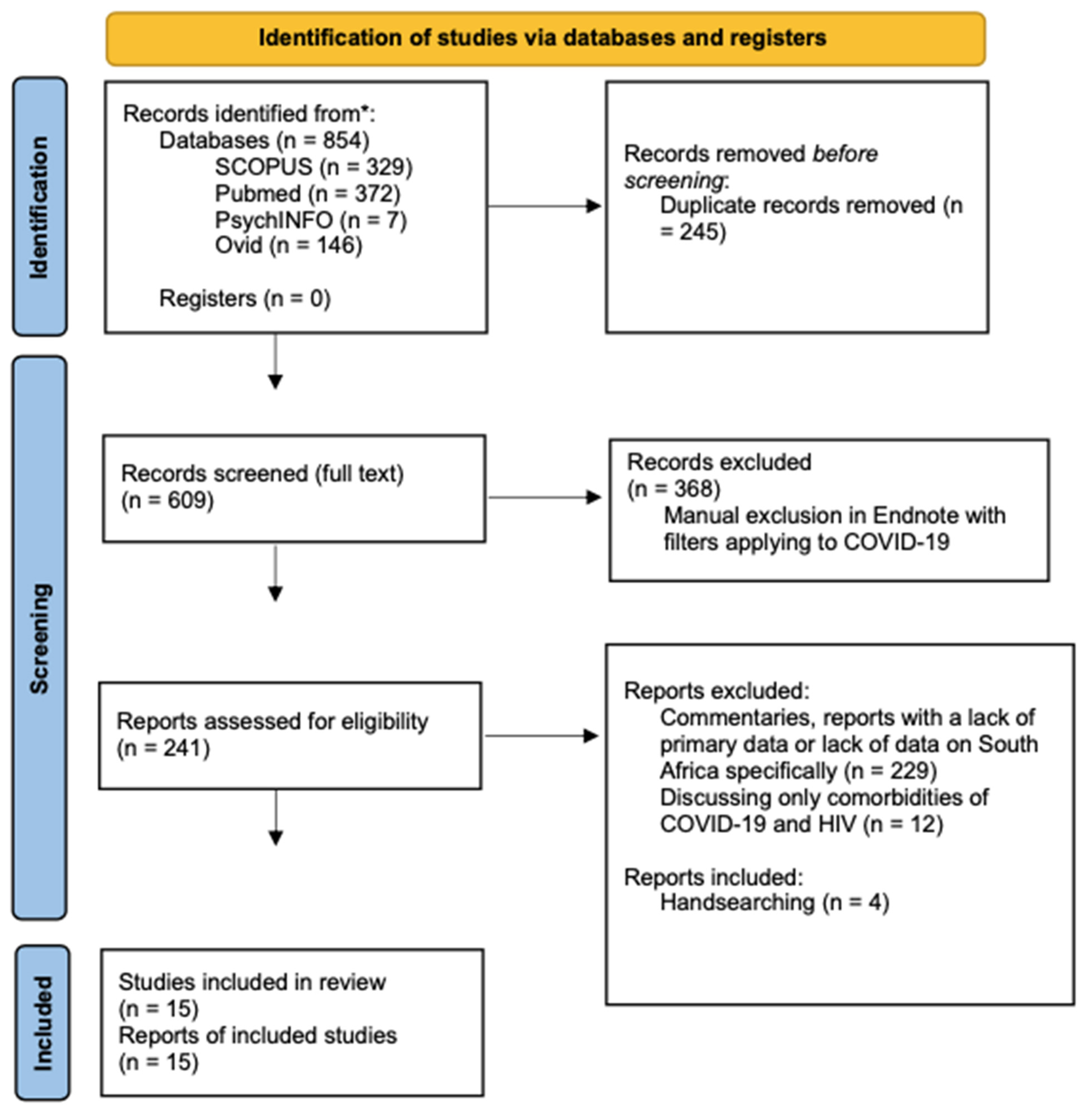
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Topic Modeling
2.5. Quality Assessment
3. Results
4. Discussion
4.1. Disruptions in Care
4.1.1. Antiretroviral Therapy (ART)
4.1.2. HIV Testing
4.1.3. Pre-Exposure Prophylaxis (PrEP)
4.2. Alternative Service Delivery
4.3. Contraceptive Access
4.4. Symptomatic Admission
4.5. Stigma
4.6. Ethical Modalities
5. Strengths
6. Limitations
7. Conclusions
8. Protocol Registration
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dorward, J. The impact of the COVID-19 lockdown on HIV care in 65 South African primary care clinics: An interrupted time series analysis. Lancet HIV 2021, 8, e158–e165. [Google Scholar] [CrossRef]
- Kruse, F.M.; Jeurissen, P.P.T. For-Profit Hospitals Out of Business? Financial Sustainability During the COVID-19 Epidemic Emergency Response. Int. J. Health Policy Manag. 2020, 9, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Simelela, N.; Venter, W.D.F.; Pillay, Y.; Barron, P. A Political and Social History of HIV in South Africa. Curr. HIV/AIDS Rep. 2015, 12, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: An interrupted time series analysis. BMJ Open 2020, 10, e043763. [Google Scholar] [CrossRef]
- Moving Towards the UNAIDS 90-90-90 Targets. Centers for Disease Control and Prevention, 2019. Available online: https://www.cdc.gov/globalhealth/stories/2019/moving-towards-unaids.html#:~:text=South%20Africa%20has%20made%20considerable,viral%20load%20suppression)%2C%20however%2C (accessed on 10 December 2021).
- Mojola, S.A.; Angotti, N.; Denardo, D.; Schatz, E.; Xavier Gómez Olivé, F. The end of AIDS? HIV and the new landscape of illness in rural South Africa. Glob. Public Health 2022, 17, 13–25. [Google Scholar] [CrossRef]
- Fassin, D.; Schneider, H. The politics of AIDS in South Africa: Beyond the controversies. BMJ 2003, 326, 495–497. [Google Scholar] [CrossRef] [Green Version]
- Kenyon, C. Cognitive dissonance as an explanation of the genesis, evolution and persistence of Thabo Mbeki’s HIV denialism. Afr. J. AIDS Res. 2008, 7, 29–35. [Google Scholar] [CrossRef]
- Saguy, A. Chapter 11: The social and cultural meanings of illness. In The Sociology of Health & Illness, 9th ed.; Conrad, P., Leiter, V., Eds.; Worth Publisher: New York, NY, USA, 2013. [Google Scholar]
- Vawda, Y.A.; Shozi, B. Eighteen years after Doha: An analysis of the use of public health TRIPS flexibilities in Africa. SSRN Electron. J. EconBiz. 2020, 103, 3559478. [Google Scholar] [CrossRef]
- Heywood, M. South Africa’s Treatment Action Campaign: Combining Law and Social Mobilization to Realize the Right to Health. J. Hum. Rights Pract. 2009, 1, 14–36. [Google Scholar] [CrossRef]
- Venkatesh, K.K.; Mayer, K.H.; Carpenter, C.C. Low-cost generic drugs under the President’s Emergency Plan for AIDS Relief drove down treatment cost; more are needed. Health Aff. 2012, 31, 1429–1438. [Google Scholar] [CrossRef] [Green Version]
- McKinlay, J. Chapter 1: The social nature of disease. In The Sociology of Health & Illness, 9th ed.; Conrad, P., Leiter, V., McKinlay, S., Eds.; Worth Publishers: New York, NY, USA, 2013; Volume 7–9. [Google Scholar]
- Mastroianni, A.C. Women and Health Research. In Institute of Medicine; Faden, R., Federmana, D., Eds.; National Academy Press: Washington, DC, USA, 1994; Volume 108–127. [Google Scholar]
- Nandi, P.L. Ethical aspects of clinical practice. Arch. Surg. 2000, 135, 22–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, S.E.; Mollborn, S. Social Determinants and Health Behaviors: Conceptual Frames and Empirical Advances. Curr. Opin. Psychol. 2015, 5, 78–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benade, M.; Long, L.; Rosen, S.; Meyer-Rath, G.; Tucker, J.M.; Miot, J. Reduction in initiations of HIV treatment in South Africa during the COVID pandemic. BMC Health Serv. Res. 2022, 22, 428. [Google Scholar] [CrossRef] [PubMed]
- Western Cape Department of Health. Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef]
- Grimsrud, A.; Wilkinson, L. Acceleration of differentiated service delivery for HIV treatment in sub-Saharan Africa during COVID-19. J. Int. AIDS Soc. 2021, 24, e25704. [Google Scholar] [CrossRef]
- El-Krab, R.; Kalichman, S.; Govindasamy, D.; Banas, E.; Kalichman, M.; Mathews, C. Subjective well-being and COVID-19 prevention practices among people living with HIV in Cape Town, South Africa. Glob. Public Health 2022, 17, 1–12. [Google Scholar] [CrossRef]
- Jensen, C.; McKerrow, N.H. Child health services during a COVID-19 outbreak in KwaZulu-Natal Province, South Africa. S. Afr. Med. J. 2020, 111, 13185. [Google Scholar] [CrossRef]
- Mutyambizi, C.; Dunlop, J.; Maluleke, C.; Ranoto, L.; Chetty, T.; Ndou, R.; Struthers, H.; McIntyre, J.A.; Rees, K. Effect of COVID-19 on HIV, tuberculosis, and prevention of mother-to-child transmission of HIV indicators in Mopani district, South Africa. S. Afr. Med. J. 2021, 111, 1181–1189. [Google Scholar] [CrossRef]
- Rees, K.; Dunlop, J.L.; Patel-Abrahams, S.; Struthers, H.; McIntyre, J.A. Primary healthcare workers at risk during COVID-19: An analysis of infections in HIV service providers in five districts of South Africa. S. Afr. Med. J. 2021, 111, 309–314. [Google Scholar] [CrossRef]
- Davey, D.L.J.; Bekker, L.G.; Mashele, N.; Gorbach, P.; Coates, T.J.; Myer, L. PrEP retention and prescriptions for pregnant women during COVID-19 lockdown in South Africa. Lancet HIV 2020, 7, e735. [Google Scholar] [CrossRef]
- Mash, R.; Christian, C.; Chigwanda, R.V. Alternative mechanisms for delivery of medication in South Africa: A scoping review. S. Afr. Fam. Pract. 2021, 63, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Bolarinwa, O.A. Factors associated with access to condoms and sources of condoms during the COVID-19 pandemic in South Africa. Arch. Public Health 2021, 79, 186. [Google Scholar] [CrossRef] [PubMed]
- Pillay, Y.; Pienaar, S.; Barron, P.; Zondi, T. Impact of COVID-19 on routine primary healthcare services in South Africa. S. Afr. Med. J. 2021, 111, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.; Koegelenberg, C.F.N.; Moolla, M.S.; Louw, E.H.; Mowlana, A.; Nortjé, A.; Ahmed, R.; Brittain, N.; Lalla, U.; Allwood, B.W.; et al. High HIV prevalence in an early cohort of hospital admissions with COVID-19 in Cape Town, South Africa. S. Afr. Med. J. 2020, 110, 982–987. [Google Scholar] [CrossRef]
- Jarolimova, J.; Yan, J.; Govere, S.; Ngobese, N.; Shazi, Z.M.; Khumalo, A.R.; Bunda, B.A.; Wara, N.J.; Zionts, D.; Thulare, H.; et al. Medical Mistrust and Stigma Associated with COVID-19 Among People Living with HIV in South Africa. AIDS Behav. 2021, 25, 3967–3977. [Google Scholar] [CrossRef] [PubMed]
- Committee on Behavioral and Social Sciences in Medical School Curricula. Enhancing the Behavioral and Social Science Content of Medical School Curricula. In Improving Medical Education; National Academies Press: Washington, DC, USA, 2004; Volume 52–86. [Google Scholar]
- Jiamsakul, A.; Kerr, S.J.; Ng, O.T.; Lee, M.P.; Chaiwarith, R.; Yunihastuti, E.; van Nguyen, K.; Pham, T.T.; Kiertiburanakul, S.; Ditangco, R.; et al. Effects of unplanned treatment interruptions on HIV treatment failure—Results from TAHOD. Trop. Med. Int. Health 2016, 21, 662–674. [Google Scholar] [CrossRef] [Green Version]
- Danel, C.; Moh, R.; Gabillard, D.; Badje, A.; le Carrou, J.; Ouassa, T.; Ouattara, E.; Anzian, A.; Ntakpé, J.B.; Minga, A.; et al. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N. Engl. J. Med. 2015, 373, 808–822. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. The Impact of the COVID-19 Response on the Supply Chain, Availability and Cost of Generic Antiretroviral Medicines for HIV in Low- and Middle-Income Countries. 2020. Available online: https://www.unaids.org/en/resources/documents/2020/covid19-supply-chain-availability-cost-generic-arv (accessed on 5 June 2022).
- Nattrass, N. Understanding the origins and prevalence of AIDS conspiracy beliefs in the United States and South Africa. Sociol. Health Illn. 2013, 35, 113–129. [Google Scholar] [CrossRef]
- WHO. WHO Recommends HIV Self Testing—Evidence Update and Considerations for Success. 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/329968/WHO-CDS-HIV-19.36-eng.pdf (accessed on 5 June 2022).
- Naicker, C.L.; Mansoor, L.E.; Dawood, H.; Naidoo, K.; Singo, D.; Matten, D.; Williamson, C.; Abdool Karim, Q. Importance of early identification of PrEP breakthrough infections in a generalized HIV epidemic: A case report from a PrEP demonstration project in South Africa. BMC Infect. Dis. 2020, 20, 532. [Google Scholar] [CrossRef]
- Baeten, J.M.; Donnell, D.; Ndase, P.; Mugo, N.R.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; Katabira, E.; et al. Antiretroviral Prophylaxis for HIV Prevention in Heterosexual Men and Women. N. Engl. J. Med. 2012, 367, 399–410. [Google Scholar] [CrossRef] [Green Version]
- Thurlow, J.; Gow, J.; George, G. HIV/AIDS, growth and poverty in KwaZulu-Natal and South Africa: An integrated survey, demographic and economy-wide analysis. J. Int. AIDS Soc. 2009, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogart, L.M.; Chetty, S.; Giddy, J.; Sypek, A.; Sticklor, L.; Walensky, R.P.; Losina, E.; Katz, J.N.; Bassett, I.V. Barriers to care among people living with HIV in South Africa: Contrasts between patient and healthcare provider perspectives. AIDS Care 2013, 25, 843–853. [Google Scholar] [CrossRef]
- Beksinska, M.; Nkosi, P.; Mabude, Z.; Mantell, J.E.; Zulu, B.; Milford, C.; Smit, J.A. Lessons from the evaluation of the South African National Female Condom Programme. PLoS ONE 2020, 15, e0236984. [Google Scholar] [CrossRef]
- Kharsany, A.B.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Earnshaw, V.A.; Bogart, L.M.; Laurenceau, J.P.; Chan, B.T.; Maughan-Brown, B.G.; Dietrich, J.J.; Courtney, I.; Tshabalala, G.; Orrell, C.; Gray, G.E.; et al. Internalized HIV stigma, ART initiation and HIV-1 RNA suppression in South Africa: Exploring avoidant coping as a longitudinal mediator. J. Int. AIDS Soc. 2018, 21, e25198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watkins, A.J. Community health workers’ efforts to build health system trust in marginalised communities: A qualitative study from South Africa. BMJ Open 2021, 11, e044065. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, T.M.; Nienaber, A.G.; Boswell, M.T.; Moodley, K. Comorbidity in context: Part 2. Ethicolegal considerations around HIV and tuberculosis during the COVID-19 pandemic in South Africa. S. Afr. Med. J. 2020, 110, 625–628. [Google Scholar]



{kind=link}
{kind=link}
| Section A: Are the Results of the Study Valid? | |||||||
|---|---|---|---|---|---|---|---|
| Author | Did the Study Address a Clearly Focused Issue? | Was the Cohort Recruited in an Acceptable Way? | Was the Exposure Accurately Measured to Minimize Bias? | Was the Outcome Accurately Measured to Minimize Bias? | 5. (a) Have the Authors Identified all Important Confounding Factors? | 5. (b) Have they Taken Account of the Confounding Factors in the Design and/or Analysis? | 6. (a) Was the Follow Up of Subjects Complete Enough? |
| Dorward | yes | yes | yes | yes | no | no | no |
| Siedner | yes | yes | yes | yes | yes | yes | yes |
| Benade | yes | yes | yes | yes | yes | no | NA |
| Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa | yes | yes | yes | yes | yes | yes | NA |
| El-Krab | yes | yes | yes | yes | yes | yes | Cannot tell |
| Jensen | yes | yes | yes | yes | yes | no | Cannot tell |
| Mutyambizi | yes | yes | yes | yes | yes | no | NA |
| Rees | yes | yes | yes | yes | yes | yes | Cannot tell |
| Davey | yes | yes | yes | yes | no | no | NA |
| Boralinwa | yes | yes | yes | yes | yes | yes | NA |
| Pillay | yes | yes | yes | yes | yes | yes | NA |
| Parker | yes | yes | yes | yes | yes | yes | NA |
| Jarolimova | yes | yes | yes | yes | yes | yes | no |
| Section B: What are the Results? | Section C: Will the Results Help Locally? | ||||||
| What are the Results of the Study? | How Precise are the Results? | Do you Believe the Results? | Will the Results Help Locally? | Do the Results of this Study Fit with Other Available Evidence? All Important Confounding Factors? | What are the Implications of this Study for Practice? | ||
| Dorward | ART treatments were generally maintained during 2020 lockdown, but HIV testing and ART initiation was impacted. | Yes, CI intervals and significance levels were reported. | yes, the statistical analysis holds. | yes | Yes and no, other studies show some drop-off in treatment continuance and maintenance, whereas this study shows a steady maintenance of ART tx. Could depend on specific pop examined. | Meaning that during a community lockdown, strategies need to be implemented to maintain or increase testing and initiation of treatments to further prevention efforts. | |
| Siedner | No changes were found in total clinic visits/clinic/day at the time of starting the level 5 lockdown. | Statistical significance and CI were stated | yes | yes | Does not fit with other studies in the same province that do suggest reductions in visit during this time. | This would implicate a lesser impact of the COVID-19 pandemic on HIV care in the KZN Province. | |
| Benade | Initiations of ART were 20% fewer in 2020 compared to 2019, with large declines in all provinces between April and June 2020. These numbers remained low for the remainder of 2020, other than short periods of recovery between COVID-19 waves and possible improvement starting in March 2021 | CI not reported | Yes, to some degree. Authors mentioned a lack of validation of the data from the DHIS database. | yes | yes | Lack of data validation may reduce support for the paper’s argument | |
| Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa | Among 601 hospitalized PLWH, 33% had their CD4 count measured during the COVID-19 episode, of which 35% had CD4 count <200 cells/µL, which was associated with COVID-19 death. HIV and previous tuberculosis infection was associated with death but not current TB. | HRs and CIs are reported | Yes, the statistical analysis holds. | yes | yes | Provides context on TB/HIV coinfection and comorbidities for HIV | |
| El-Krab | Food access was limited among the majority of the sample. Over half of the sample could not work or attend school due to lockdown policies. More than one in three participants revealed interruptions in their HIV care, specifically in medication access. | Yes, chi-square tests and t-tests were used to assess correlations, with statistical significance noted. | yes, the statistical analysis holds. | yes | Yes, authors discussed similar results with other primary literature sources | Supports focus on psychological well-being with adherence of ART associated with COVID-19 protections | |
| Jensen | Reductions in hospital visits were recorded with less recovery than PHC clinic attendance. Access to service was reduced further for young children than for adults and adolescents. | Yes, CI intervals and significance levels were reported. | yes, the statistical analysis holds. | yes | Cannot tell | Confirmation of the anticipated impact of the COVID-19 pandemic on child health services, with a pattern of disruption across multiple data elements and indicators covering service access, service delivery and child wellbeing. | |
| Mutyambizi | Study showed statistically significant declines in ART initiation, both at the beginning of the first wave in April and at the move to lockdown level 1 in September. | single-group ITSA regression model was used | yes, the statistical analysis holds. | yes | Yes and no, authors mentioned finding data similar to another study covering DHIS data in all of SA but in contrast to a DHIS data set in the KZN Province | Comprehensive data analysis that can help prepare for breaks in treatment in future waves | |
| Rees | Rates of COVID-19 infection were as high in frontline support staff as those in clinical HCWs. | Cumulative incidence was noted, but CI or p values were not stated | somewhat, could use some more statistical data validation | yes | Cannot tell | CHW of HIV facilities who test positive for COVID-19 pose infectious risk to PLHIV, potentially affecting the prognosis | |
| Davey | During the initial lockdown, women’s missed PrEP visits increased from 34% (pre-lockdown) to 57% (during lockdown). | Yes, IQR intervals and CI levels reported | yes, the statistical analysis holds. | yes | Cannot tell | Clinical implications for missed visits are great for maternal and infant health. Pregnant and post-partum women who were on PrEP cited their reasoning for missed appts. to fear of contracting the virus. Making it essential for different delivery of care in the community to address these barriers and continue prevention efforts. | |
| Boralinwa | One-fourth of South Africans couldn’t access condoms during the pandemic; individuals in lower wealth groups had less public access to condoms; ppl w/lower educational attainment, between 25 and 34 were less likely to prefer public source of condoms | CI levels, agency levels, and sig. levels reported | yes, the statistical analysis holds. | yes | yes | Study shines light on access to condoms that was limited during the pandemic and the preferred method of obtaining condoms, which was skewed across the public and age cohorts. Strategies on community distribution of free condoms should be implemented in the future. | |
| Pillay | Confirmed decrease in use of primary healthcare facilities within all South African provinces | CI or p values were not stated | somewhat, could use some more statistical data validation | yes | Yes, described similar findings from a review by the Global Fund | ||
| Parker | PLHIV with COVID-19 may have a high probability of admission to hospital, but had similar presentations, comorbidities and outcomes when compared with the HIV-negative study population. | Statistical significance and CI were stated | Mostly, although the sample size was small | yes | Cannot tell | The presentation and outcome of patients with HIV did not differ significantly from those of patients without HIV | |
| Jarolimova | High stigma of COVID-19 was associated more with the female gender and previous HIV stigma. Lower stigma of COVID-19 was associated with television broadcast as an information source. Further efforts should focus on stigma and mistrust, as well as its effects on protective health behaviors and vaccine hesitancy. | Descriptive statistics with univariate logistic regression models | yes, the statistical analysis holds. | yes | Cannot tell | Sheds light on the prevalence of medical mistrust and conspiracy beliefs related to COVID-19 among PLWH in South Africa | |
| Author | Section A: Are the Results of the Review Valid? | |||||
|---|---|---|---|---|---|---|
| 1. Did the Review Address a Clearly Focused Question? | 2. Did the Authors Look for the Right Type of Papers? | 3. Do You Think all the Important, Relevant Studies were Included? | 4. Did the Review’s Authors do Enough to Assess Quality of the Included Studies? | 5. If the Results of the Review have been Combined, was it Reasonable to do so? | 6. Apart from the Experimental Intervention, did Each Study Group Receive the Same Level of Care (that is, Were They Treated Equally)? | |
| Mash | yes | yes | yes | yes | yes | NA |
| Section B: What are the Results? | Section C: Will the Results Help Locally? | |||||
| 6. What are the Overall Results of the Review? | 7. How Precise are the Results? | 8. Can the Results be Applied to the Local Population? | 9. Were all Important Outcomes Considered? | 10. Are the Benefits Worth the Harms and Costs? | ||
| The study suggests the implementation of a hybrid system that allows alternatives to heed to the needs of each patient. | Precise, studies were adequately analyzed and reviewed | Yes, promotes the hybrid approach in South Africa | yes | yes | ||
| Author | Section A: Are the Results of the Review Valid? | ||||||
|---|---|---|---|---|---|---|---|
| 1. Was There a Clear Statement of the Aims of the Research? | 2. Is a Qualitative Methodology Appropriate? | 3. Was the Research Design Appropriate to Address the Aims of the Research? | 4. Was the Recruitment Strategy Appropriate to the aims of the Research? | 5. Was the Data Collected in a Way that Addressed the Research Issue? | 6. Has the Relationship between Researcher and Participants been Adequately Considered? | 7. Have Ethical Issues been Taken into Consideration? | |
| Grimsrud | yes | yes | yes | yes | Yes | yes | yes |
| Section B: What are the Results? | Section C: Will the Results Help Locally? | ||||||
| 7. Have Ethical Issues been Taken into Consideration? | 8. Was the Data Analysis Sufficiently Rigorous? | 9. Is There a Clear Statement of Findings? | 10. How Valuable is the Research? | ||||
| yes | yes | yes | The authors review and promote the use of differentiated service delivery for HIV, which extends access to treatment services | ||||
| Ref | Author | Study Type | Study Population | N | Analytical Method |
|---|---|---|---|---|---|
| [1] | Dorward | Interrupted time series analysis | People testing for HIV, initiating ART, and collecting ART at participating clinics recorded on the DHIS | 3,706,543 | multivariable |
| [4] | Siedner | Interrupted time series analysis | Patients from 11 primary healthcare clinic in KwaZulu-Natal Province with data recorded on the Africa Health Research Institute (AHRI) surveillance system | 46,523 | multivariable |
| [17] | Benade | Retrospective cohort | Facilities providing ART initiations in SA District Health Information System (DHIS) | 2471 | multivariable |
| [18] | Western Cape Department of Health | Population cohort | Adults attending public sector health facilities in Western Cape | 3,460,932 | Univariable and multivariable HRs |
| [19] | Grimsrud | Qualitative study | ART receiving patients in sub-Saharan Africa | NA | univariable |
| [20] | El-Krab | Observational cohort | Patients receiving services for HIV treatment at a public health clinic in an established formal township of Cape Town | 272 | univariable |
| [21] | Jensen | Retrospective cohort | Health facilities recorded in the DHIS data set for KwaZulu-Natal Province | 681 | multivariable |
| [22] | Mutyambizi | Retrospective cohort | Health facilities of the Mopani District in the Limpopo Province registered on DHIS | NA | multivariable |
| [23] | Rees | Retrospective cohort | Anova Health Institute employees of primary healthcare facilities in Cape Town, Capricorn, Sedibeng, Johannesburg and Mopani districts in South Africa | 562 | univariable |
| [24] | Davey | Population cohort | Pregnant and post-partum women with HIV-negative status in antenatal care at a primary care clinic that was operational during the COVID-19 lockdown in a Cape Town community with high antenatal HIV prevalence | 455 | univariable |
| [25] | Mash | Systematic review | Reviews of alternative mechanisms for delivery of medication to South African primary health clinic patients | 4253 | univariable |
| [26] | Bolarinwa | Observational cohort | Respondents of National Income Dynamics Study-COVID Rapid Mobile Survey | 5304 | univariable |
| [27] | Pillay | Observational cohort | Patients making visits for primary healthcare, reproductive, maternity, and HIV care within all African provinces recorded on DHIS | NA | multivariable |
| [28] | Parker | Retrospective cohort | Patients admitted to the Tyberg hospital in Cape Town | 116 | multivariable |
| [29] | Jarolimova | Observational cohort | Patients receiving HIV care in 9 DOH primary health clinics that enroll in the Central Chronic Medicines Dispensing and Distribution program (CCMDD) in the urban Umlazi township | 303 | multivariable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, K.; Himelfarb, A.; Karrah, K.; Porterfield, L.; Paremoer, L.; Serag, H.; Lee, W.-C. The Social, Behavioral, and Ethical Modalities of COVID-19 on HIV Care in South Africa: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9766. https://doi.org/10.3390/ijerph19159766
Roy K, Himelfarb A, Karrah K, Porterfield L, Paremoer L, Serag H, Lee W-C. The Social, Behavioral, and Ethical Modalities of COVID-19 on HIV Care in South Africa: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9766. https://doi.org/10.3390/ijerph19159766
Chicago/Turabian StyleRoy, Khushali, Aliayah Himelfarb, Kapil Karrah, Laura Porterfield, Lauren Paremoer, Hani Serag, and Wei-Chen Lee. 2022. "The Social, Behavioral, and Ethical Modalities of COVID-19 on HIV Care in South Africa: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 15: 9766. https://doi.org/10.3390/ijerph19159766