
A Combination of Long-Duration Electrical Stimulation with External Shoulder Support during Routine Daily Activities in Patients with Post-Hemiplegic Shoulder Subluxation: A Randomized Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample Inclusion and Exclusion Criteria
2.3. Sample Size Estimation
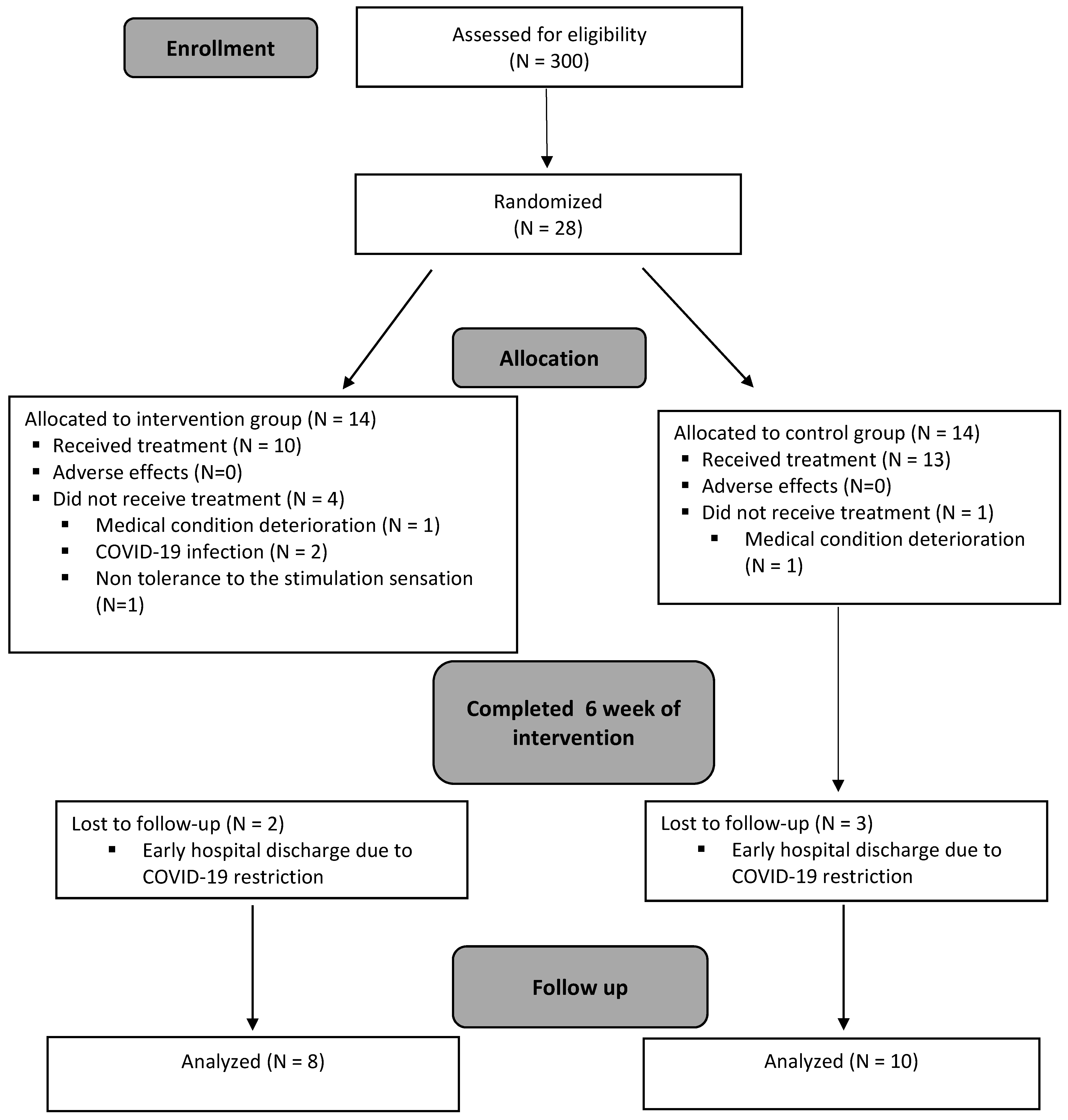
2.4. Recruitment and Randomization
2.5. Ethics Statement
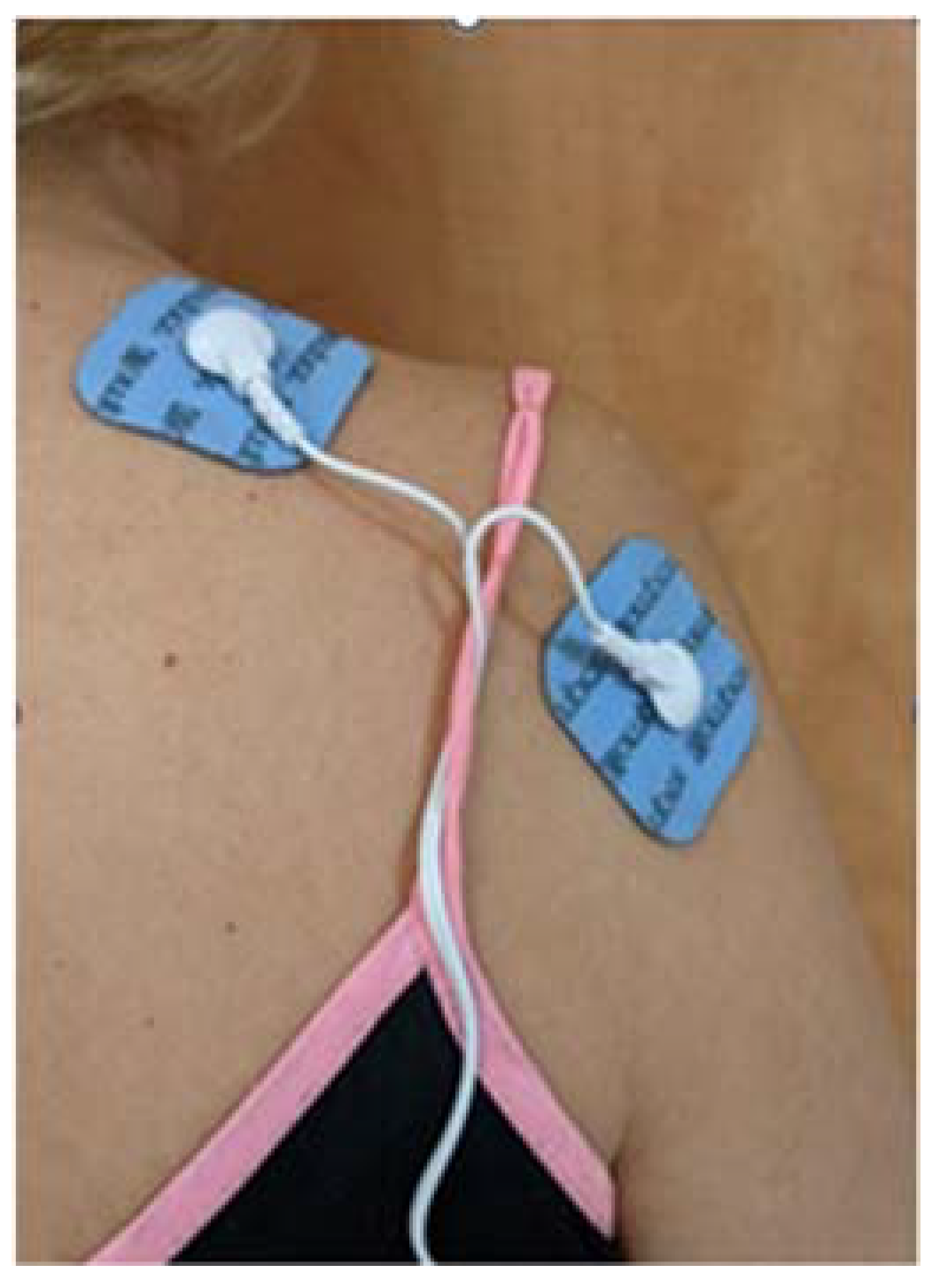
2.6. Intervention
2.7. Data Collection
2.8. Outcome Measures
2.8.1. Shoulder Subluxation Measurement
2.8.2. Upper-Extremity Motor Function
2.8.3. Distal Upper-Extremity Movement
2.8.4. Active Finger Extension
2.8.5. Pain Intensity
2.8.6. Daily Function
2.9. Statistical Analysis
3. Results
3.1. Background Characteristics of the Subjects per Group
3.2. Outcome Measures
3.2.1. Shoulder Subluxation
3.2.2. Motor Function
3.2.3. Hand Movement
3.2.4. Finger Extension
3.2.5. Pain
3.2.6. Daily Living Function
4. Discussion
4.1. Shoulder Subluxation
4.2. Motor Function
4.3. Hand Movement and Finger Extension
4.4. Pain
4.5. Daily Living Function
4.6. Follow-Up
4.7. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hong, J.; Jung, T.; Kim, A.; Choi, H.; Lee, S.; Kim, D. Effects of position-triggered electrical stimulation on poststroke hemiparetic shoulder subluxation. Eur. J. Phys. Rehabil. Med. 2021, 57, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Arya, K.N.; Pandian, S.; Puri, V. Rehabilitation methods for reducing shoulder subluxation in post-stroke hemiparesis: A systematic review. Top. Stroke Rehabil. 2017, 25, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Adey-Wakeling, Z.; Liu, E.; Crotty, M.; Leyden, J.; Kleinig, T.; Anderson, C.S.; Newbury, J. Hemiplegic Shoulder Pain Reduces Quality of Life after Acute Stroke: A Prospective Population-Based Study. Am. J. Phys. Med. Rehabil. 2016, 95, 758–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, P.; Fernando, C.; Mendoza, D.; Shah, R. Risk and associated factors for hemiplegic shoulder pain in people with stroke: A systematic literature review. Phys. Ther. Rev. 2021, 1–14. [Google Scholar] [CrossRef]
- De Sire, A.; Moggio, L.; Demeco, A.; Fortunato, F.; Spanò, R.; Aiello, V.; Marotta, N.; Ammendolia, A. Efficacy of rehabilitative techniques in reducing hemiplegic shoulder pain in stroke: Systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2021, 65, 101602. [Google Scholar] [CrossRef]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; Di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief 2020, 30, 105419. [Google Scholar] [CrossRef]
- Vafadar, A.K.; Côté, J.N.; Archambault, P.S. Effectiveness of Functional Electrical Stimulation in Improving Clinical Outcomes in the Upper Arm following Stroke: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2015, 2015, 729768. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W.; Andrews, A.W. Shoulder Subluxation and Pain in Stroke Patients. Am. J. Occup. Ther. 1990, 44, 507–509. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Cao, C.; Xie, H.; Huang, Q.; Ge, M.; Yin, L.; Chen, L.; Qu, M.; Huo, M.; Onoda, K.; et al. Evaluation of supraspinatus muscle changes in the shoulder joint of stroke patients with hemiplegic and shoulder subluxation using ultrasonography: Comparison between affected and unaffected sides. J. Phys. Ther. Sci. 2022, 34, 44–48. [Google Scholar] [CrossRef]
- Ada, L.; Foongchomcheay, A. Efficacy of electrical stimulation in preventing or reducing subluxation of the shoulder after stroke: A meta-analysis. Aust. J. Physiother. 2002, 48, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Baker, L.L.; Johnson, R.E.; Tilson, J.K. Effectiveness of neuromuscular electrical stimulation for management of shoulder subluxation post-stroke: A systematic review with meta-analysis. Clin. Rehabil. 2017, 31, 1431–1444. [Google Scholar] [CrossRef] [PubMed]
- Paci, M.; Nannetti, L.; Rinaldi, L.A. Glenohumeral subluxation in hemiplegia: An overview. J. Rehabil. Res. Dev. 2005, 42, 557. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed. Eng. Online 2020, 19, 34. [Google Scholar] [CrossRef] [PubMed]
- Ada, L.; Foongchomcheay, A.; Canning, C.G. Supportive devices for preventing and treating subluxation of the shoulder after stroke. Cochrane Database Syst. Rev. 2005, 2005, CD003863. [Google Scholar] [CrossRef]
- Nadler, M.; Pauls, M. Shoulder orthoses for the prevention and reduction of hemiplegic shoulder pain and subluxation: Systematic review. Clin. Rehabil. 2016, 31, 444–453. [Google Scholar] [CrossRef]
- Baker, L.L.; Parker, K. Neuromuscular Electrical Stimulation of the Muscles Surrounding the Shoulder. Phys. Ther. 1986, 66, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Yan, T.; Lin, Z. Long-term effectiveness of neuromuscular electrical stimulation for promoting motor recovery of the upper extremity after stroke. J. Rehabil. Med. 2011, 43, 506–510. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Shin, H.; Hu, X. Muscle Fatigue Post-stroke Elicited From Kilohertz-Frequency Subthreshold Nerve Stimulation. Front. Neurol. 2018, 9, 1061. [Google Scholar] [CrossRef]
- Nussbaum, E.L.; Houghton, P.; Anthony, J.; Rennie, S.; Shay, B.L.; Hoens, A.M. Neuromuscular Electrical Stimulation for Treatment of Muscle Impairment: Critical Review and Recommendations for Clinical Practice. Physiother. Can. 2017, 69, 1–76. [Google Scholar] [CrossRef]
- Shepherd, R.B.; Carr, J.H. The Shoulder following Stroke: Preserving Musculoskeletal Integrity for Function. Top. Stroke Rehabil. 1998, 4, 35–53. [Google Scholar] [CrossRef]
- Boyd, E.A.; Torrance, G.M. Clinical measures of shoulder subluxation: Their reliability. Can. J. Public Health 1992, 83, S24–S28. [Google Scholar] [PubMed]
- Hall, J.; Dudgeon, B.; Guthrie, M. Validity of clinical measures of shoulder subluxation in adults with poststroke hemiplegia. Am. J. Occup. Ther. 1995, 49, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladstone, D.; Danells, C.J.; Black, S. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Rozevink, S.G.; van der Sluis, C.K.; Garzo, A.; Keller, T.; Hijmans, J.M. HoMEcare aRm rehabiLItatioN (MERLIN): Telerehabilitation using an unactuated device based on serious games improves the upper limb function in chronic stroke. J. Neuroeng. Rehabil. 2021, 18, 48. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patients. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Page, S.J.; Levine, P.; Hade, E. Psychometric Properties and Administration of the Wrist/Hand Subscales of the Fugl-Meyer Assessment in Minimally Impaired Upper Extremity Hemiparesis in Stroke. Arch. Phys. Med. Rehabil. 2012, 93, 2373–2376.e5. [Google Scholar] [CrossRef] [Green Version]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies Comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the Numeric Pain Rating Scale in Patients with Shoulder Pain and the Effect of Surgical Status. J. Sport Rehabil. 2011, 20, 115–128. [Google Scholar] [CrossRef]
- Sato, K.; Inoue, T.; Maeda, K.; Shimizu, A.; Murotani, K.; Ueshima, J.; Ishida, Y.; Ogawa, T.; Suenaga, M. Early Wearing of Knee-Ankle-Foot Orthosis Improves Functional Prognosis in Patients after Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106261. [Google Scholar] [CrossRef]
- Dutta, D.; Sen, S.; Aruchamy, S.; Mandal, S. Prevalence of post-stroke upper extremity paresis in developing countries and significance of m-Health for rehabilitation after stroke—A review. Smart Health 2022, 23, 100264. [Google Scholar] [CrossRef]
- Jang, Y.Y.; Kim, T.H.; Lee, B.H. Effects of Brain-Computer Interface-controlled Functional Electrical Stimulation Training on Shoulder Subluxation for Patients with Stroke: A Randomized Controlled Trial. Occup. Ther. Int. 2016, 23, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiragami, S.; Inoue, Y.; Harada, K. Minimal clinically important difference for the Fugl-Meyer assessment of the upper extremity in convalescent stroke patients with moderate to severe hemiparesis. J. Phys. Ther. Sci. 2019, 31, 917–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollà-Casanova, S.; Llorens, R.; Borrego, A.; Salinas-Martínez, B.; Serra-Añó, P. Validity, reliability, and sensitivity to motor impairment severity of a multi-touch app designed to assess hand mobility, coordination, and function after stroke. J. Neuroeng. Rehabil. 2021, 18, 70. [Google Scholar] [CrossRef] [PubMed]
- Pandyan, A.D.; Cameron, M.; Powell, J.; Stott, D.J.; Granat, M.H. Contractures in the post-stroke wrist: A pilot study of its time course of development and its association with upper limb recovery. Clin. Rehabil. 2003, 17, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.; Crome, P. Hand function and stroke. Rev. Clin. Gerontol. 2002, 12, 68–81. [Google Scholar] [CrossRef]
- Hao, N.; Zhang, M.; Li, Y.; Guo, Y. Risk factors for shoulder pain after stroke: A clinical study. Pak. J. Med Sci. 2021, 38, 145. [Google Scholar] [CrossRef] [PubMed]
- Beninato, M.; Gill-Body, K.M.; Salles, S.; Stark, P.C.; Black-Schaffer, R.M.; Stein, J. Determination of the minimal clinically im-portant difference in the FIM instrument in patients with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 32–39. [Google Scholar] [CrossRef]
- Faghri, P.D.; Rodgers, M.M.; Glaser, R.M.; Bors, J.G.; Ho, C.; Akuthota, P. The effects of functional electrical stimulation on shoulder subluxation, arm function recovery, and shoulder pain in hemiplegic stroke patients. Arch. Phys. Med. Rehabil. 1994, 75, 73–79. [Google Scholar] [CrossRef]
- Linn, S.L.; Granat, M.H.; Lees, K.R. Prevention of shoulder subluxation after stroke with electrical stimulation. Stroke 1999, 30, 963–968. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.-Y.; Yang, Y.-R.; Tsai, M.-W.; Wang, W.T.J.; Chan, R.-C. Effects of Functional Electric Stimulation on Upper Limb Motor Function and Shoulder Range of Motion in Hemiplegic Patients. Am. J. Phys. Med. Rehabil. 2002, 81, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Corbellini, C.; Rossino, E.; Massaccesi, R.; Battaglino, A.; Pedersini, P.; Sanchez-Romero, E.A.; Villafañe, J.H. Improvements in Perimeter Thoracic Mobility on Patients with COPD after Pulmonary Rehabilitation: A Case Series. Electron. J. Gen. Med. 2022, 19, em361. [Google Scholar]
- Abd, A.T.; Singh, R.E.; Iqbal, K.; White, G. Investigation of Power Specific Motor Primitives in an Upper Limb Rotational Motion. J. Mot. Behav. 2022, 54, 80–91. [Google Scholar] [CrossRef]
- Roh, J.; Rymer, W.Z.; Perreault, E.J.; Yoo, S.B.; Beer, R.F. Alterations in upper limb muscle synergy structure in chronic stroke survivors. J. Neurophysiol. 2013, 109, 768–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Control Group n = 13 (Mean ± SD) | Experimental Group n = 10 (Mean ± SD) | Mann-Whitney (U, p-Value) |
|---|---|---|---|
| Age (years) | 67.54 ± 15.54 | 73.30 ± 9.81 | U = 48, p = 0.306 |
| Weight (kg) | 70.97 ± 12.02 | 65.75 ± 11.01 | U = 50, p = 0.352 |
| BMI (kg/m2) | 25.72 ± 4.87 | 25.23 ± 3.26 | U = 47, p = 0.849 |
| Time since stroke (months) | 1.38 ± 1.61 | 0.50 ± 0.97 | U = 45, p = 0.169 |
| Variables | Control Group | Experimental Group | Chi-Square χ2 (p-Value) |
| Sex | Male 61.5% Female 38.5% | Male 60% Female 40% | Fisher, p = 1 |
| Background disease | Yes 69.2% No 30.8% | Yes 70% No 30% | Fisher, p = 1 |
| Type of stroke | Ischemic 76.9% Hemorrhagic 23.1% | Ischemic 80% Hemorrhagic 20% | Fisher, p = 1 |
| Affected side | Right 53.8% Left 46.2% | Right 50% Left 50% | Fisher, p = 1 |
| Pre-Intervention (T0) | Post-Intervention Following 6 Weeks of Treatment (T1) | Follow-Up 2 Weeks Later (T2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Experimental n = 10 | Control n = 13 | p-Value | Experimental n = 10 | Control n = 13 | p-Value | Experimental n = 8 | Control n = 10 | p-Value | |
| Shoulder subluxation (cm) | 1.60 ± 0.84 (2.00) | 2.23 ± 0.93 (2.00) | 0.148 | 0.70 ± 0.82 (0.50) | 2.00 ± 1.08 (2.00) | 0.0058 | 0.38 ± 0.74 (0.00) | 2.00 ± 1.20 (2.10) | 0.0045 |
| * FMA-UE (0–66) | 24.70 ± 17.98 (30.00) | 13.00 ± 11.80 (4.00) | 0.099 | 44.70 ± 21.92 (53.50) | 17.46 ± 16.00 (15.00) | 0.005 | 51.00 ± 19.82 (55.00) | 23.20 ± 17.55 (22.50) | 0.016 |
| Hand, FMA-UE (0–14) | 5.20 ± 4.83 (5.00) | 2.00 ± 3.08 (0.00) | 0.094 | 9.90 ± 5.32 (11.50) | 3.15 ± 4.34 (0.00) | 0.006 | 11.13 ± 4.73 (13.00) | 4.40 ± 5.13 (3.00) | 0.03 |
| Finger Extension (0–2) | 0.90 ± 0.99 (0.50) | 0.46 ± 0.78 (0.00) | 0.285 | 1.70 ± 0.67 (2.00) | 0.62 ± 0.87 (0.00) | 0.007 | 1.75 ± 0.71 (2.00) | 0.90 ± 0.88 (1.00) | 0.038 |
| NPRS (0–10) | 4.30 ± 3.80 (4.00) | 3.92 ± 3.28 (4.00) | 0.825 | 4.00 ± 3.20 (5.00) | 3.46 ± 2.54 (4.00) | 0.639 | 2.88 ± 2.75 (2.00) | 3.60 ± 3.24 (4.00) | 0.786 |
| FIM (18–126) | 58.30 ± 15.46 (57.50) | 52.00 ± 22.35 (44.00) | 0.456 | 81.20 ± 21.16 (83.00) | 63.00 ± 27.40 (59.00) | 0.172 | 89.50 ± 22.33 (94.50) | 69.90 ± 27.10 (60.00) | 0.168 |
| Post-Intervention Minus Pre Intervention | Follow-Up Minus Post Intervention | Follow-Up Minus Pre Intervention | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Experimental n = 10 | Control n = 13 | p-Value | Experimental n = 8 | Control n = 10 | p-Value | Experimental n = 8 | Control n = 10 | p-Value | |
| Shoulder subluxation | −0.90 ± 1.20 (−1.00) | −0.23 ± 0.60 (0.00) | 0.0964 | −0.13 ± 0.35 (0.00) | 0.30 ± 0.67 (0.00) | 0.1158 | −1.38 ± 0.92 (−1.00) | 0.00 ± 1.05 (0.00) | 0.0107 |
| * FMA-UE | 20.00 ± 20.09 (15.50) | 4.46 ± 12.31 (0.00) | 0.006 | 0.75 ± 1.67 (0.50) | 1.50 ± 3.21 (0.00) | 1.0000 | 24.88 ± 20.51 (23.50) | 7.50 ± 16.30 (0.50) | 0.035 |
| Hand, FMA-UE (0–14) | 4.70 ± 4.95 (2.00) | 1.15 ± 3.34 (0.00) | 0.014 | 0.00 ± 0.53 (0.00) | 0.30 ± 1.25 (0.00) | 0.49 | 5.50 ± 5.21 (4.50) | 1.80 ± 4.89 (0.50) | 0.1040 |
| Finger extension (0–2) | 0.80 ± 0.92 (0.50) | 0.15 ± 0.55 (0.00) | 0.036 | 0.00 ± 0.00 (0.00) | 0.10 ± 0.32 (0.00) | 0.434 | 0.88 ± 0.99 (0.50) | 0.30 ± 0.67 (0.00) | 0.182 |
| NPRS (0–10) | −0.30 ± 4.11 (0.00) | −0.46 ± 4.03 (0.00) | 0.826 | −0.25 ± 1.39 (0.00) | 0.10 ± 3.54 (0.00) | 0.854 | −1.38 ± 4.07 (−0.50) | −1.30 ± 4.92 (−1.00) | 0.964 |
| FIM (18–126) | 22.90 ± 17.50 (21.00) | 11.00 ± 11.02 (6.00) | 0.099 | 8.63 ± 8.58 (5.50) | 1.70 ± 2.54 (0.00) | 0.062 | 31.88 ± 16.48 (34.00) | 14.90 ± 13.22 (14.00 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavi, C.; Elboim-Gabyzon, M.; Naveh, Y.; Kalichman, L. A Combination of Long-Duration Electrical Stimulation with External Shoulder Support during Routine Daily Activities in Patients with Post-Hemiplegic Shoulder Subluxation: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2022, 19, 9765. https://doi.org/10.3390/ijerph19159765
Lavi C, Elboim-Gabyzon M, Naveh Y, Kalichman L. A Combination of Long-Duration Electrical Stimulation with External Shoulder Support during Routine Daily Activities in Patients with Post-Hemiplegic Shoulder Subluxation: A Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9765. https://doi.org/10.3390/ijerph19159765
Chicago/Turabian StyleLavi, Chen, Michal Elboim-Gabyzon, Yuval Naveh, and Leonid Kalichman. 2022. "A Combination of Long-Duration Electrical Stimulation with External Shoulder Support during Routine Daily Activities in Patients with Post-Hemiplegic Shoulder Subluxation: A Randomized Controlled Study" International Journal of Environmental Research and Public Health 19, no. 15: 9765. https://doi.org/10.3390/ijerph19159765