
The Effects of Freshwater Clam (Corbicula fluminea) Extract on Serum Tumor Necrosis Factor-Alpha (TNF-α) in Prediabetic Patients in Taiwan

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
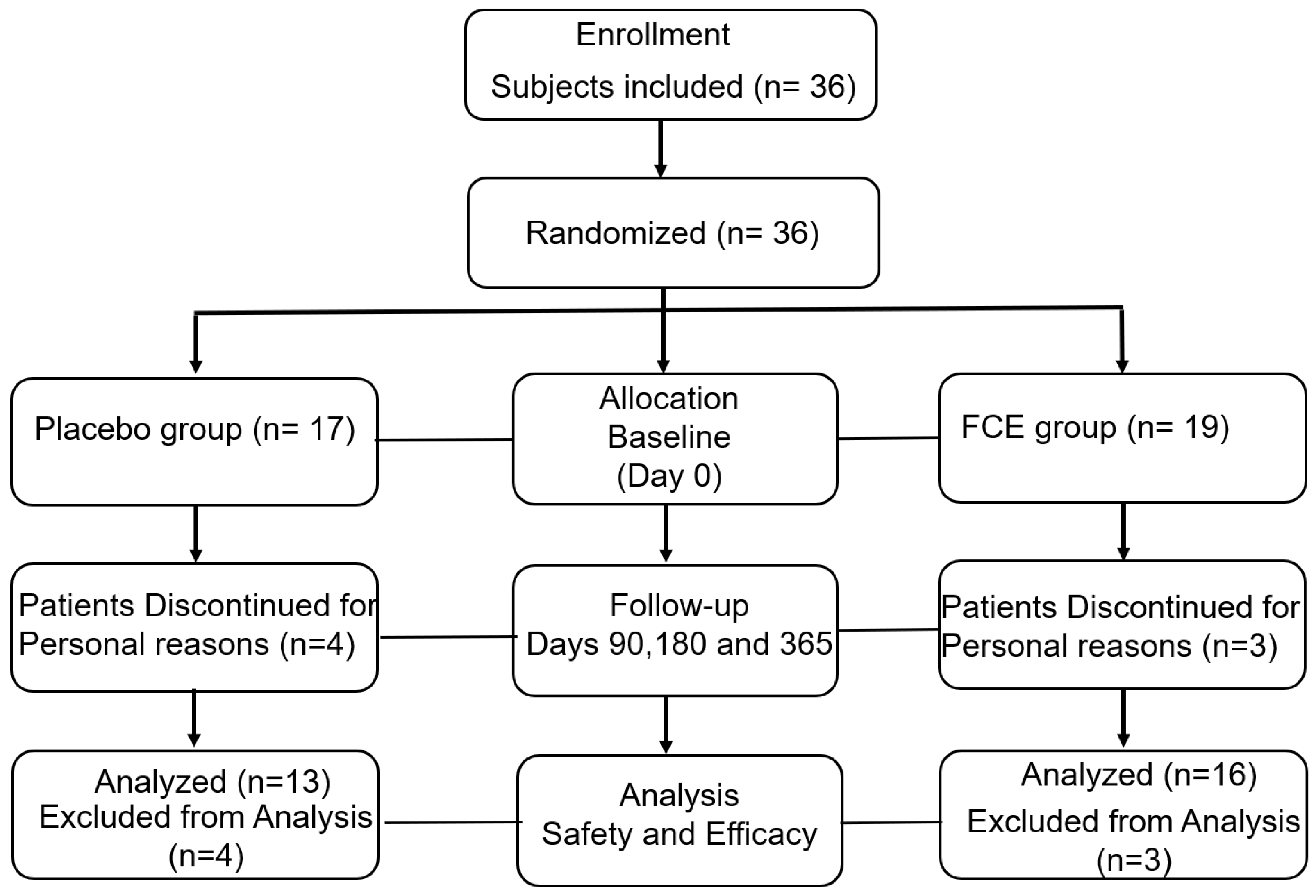
2.1. Demographics of Participants and Safety Evaluation of FCE in This Study
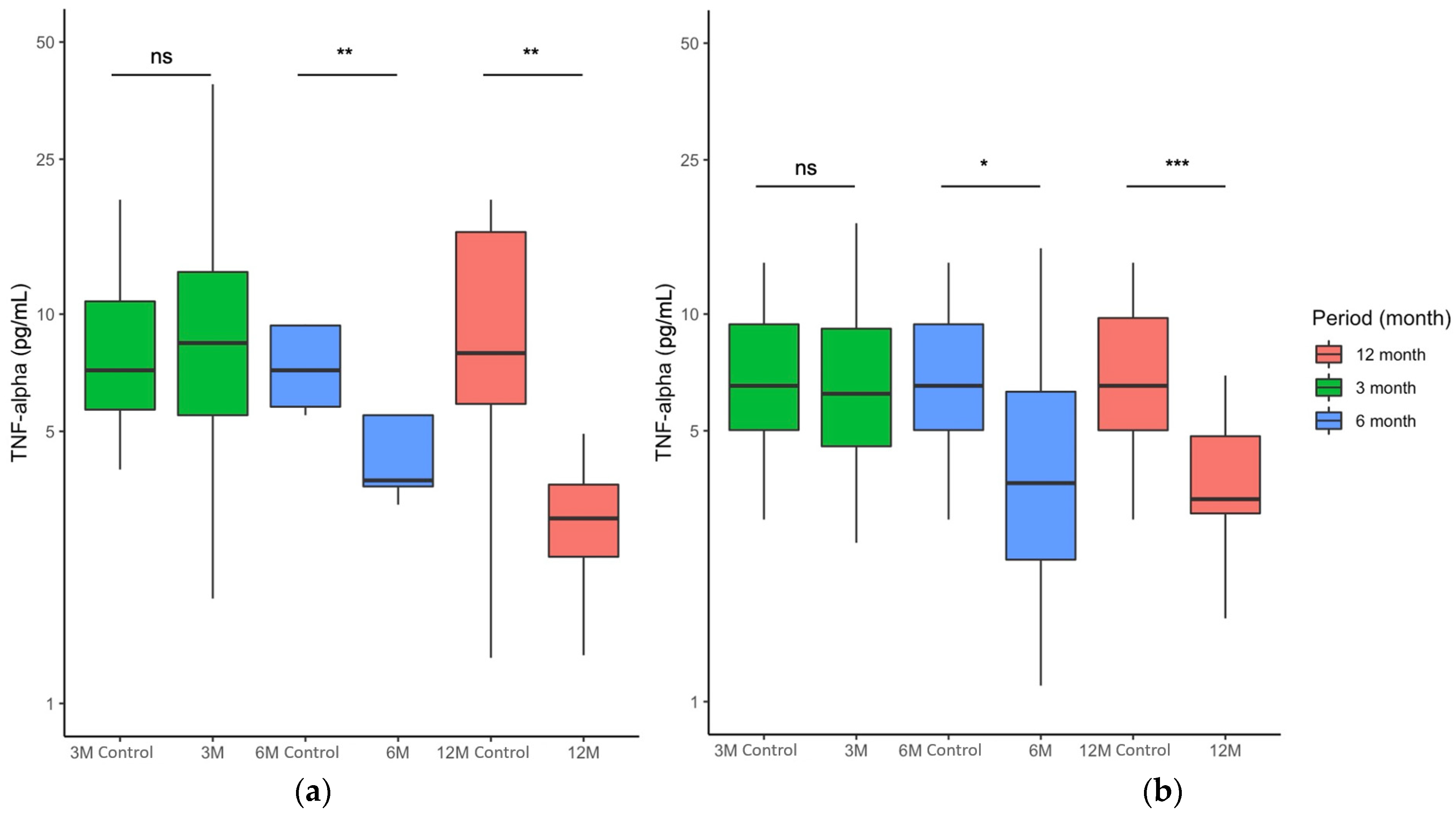
2.2. FCE Significantly Reduced Serum TNF-α Concentration of All Participants during and after Nutritional Intervention
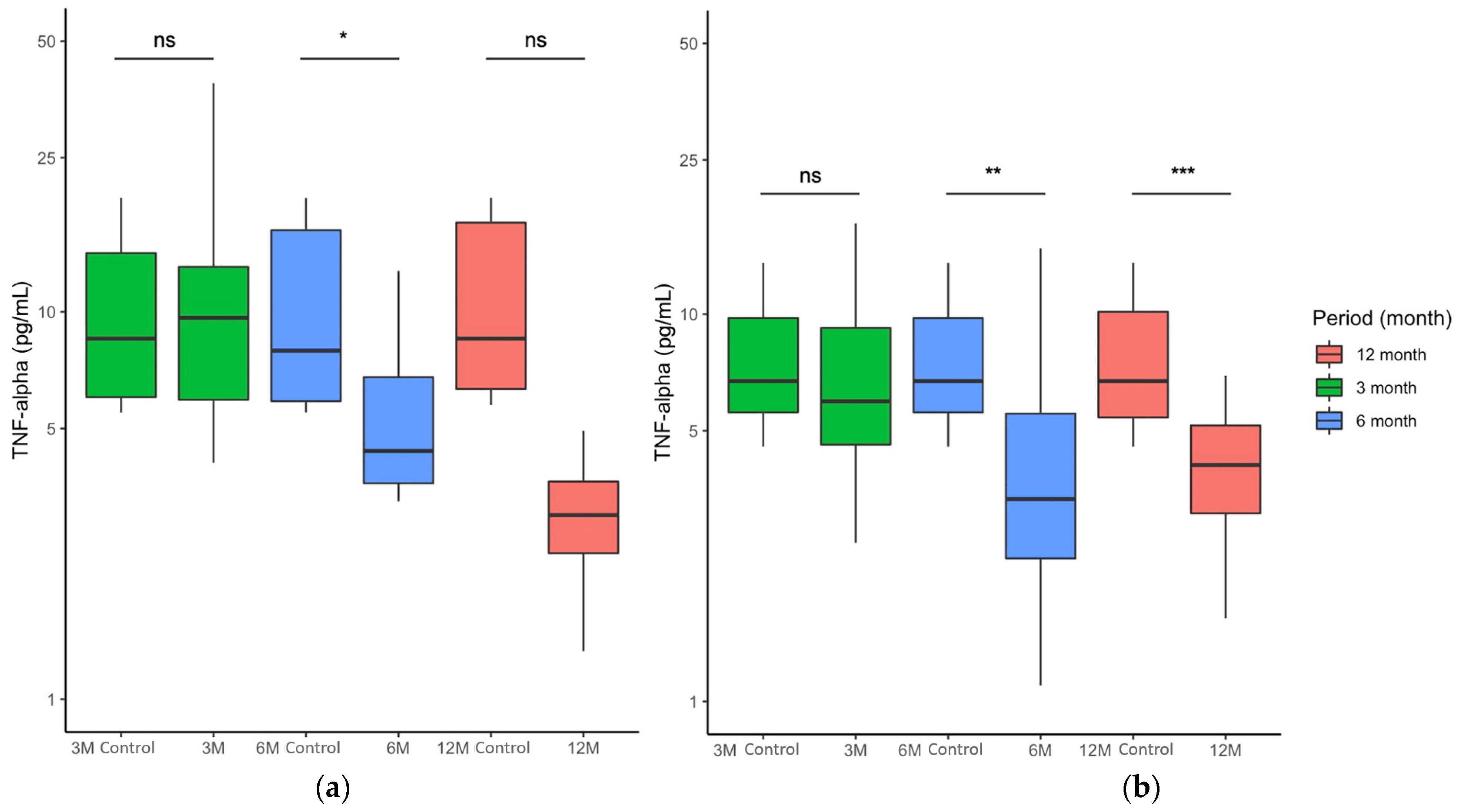
2.3. FCE Significantly Improved Patients with Elevated Serum TNF-α Concentrations during and after Nutritional Intervention
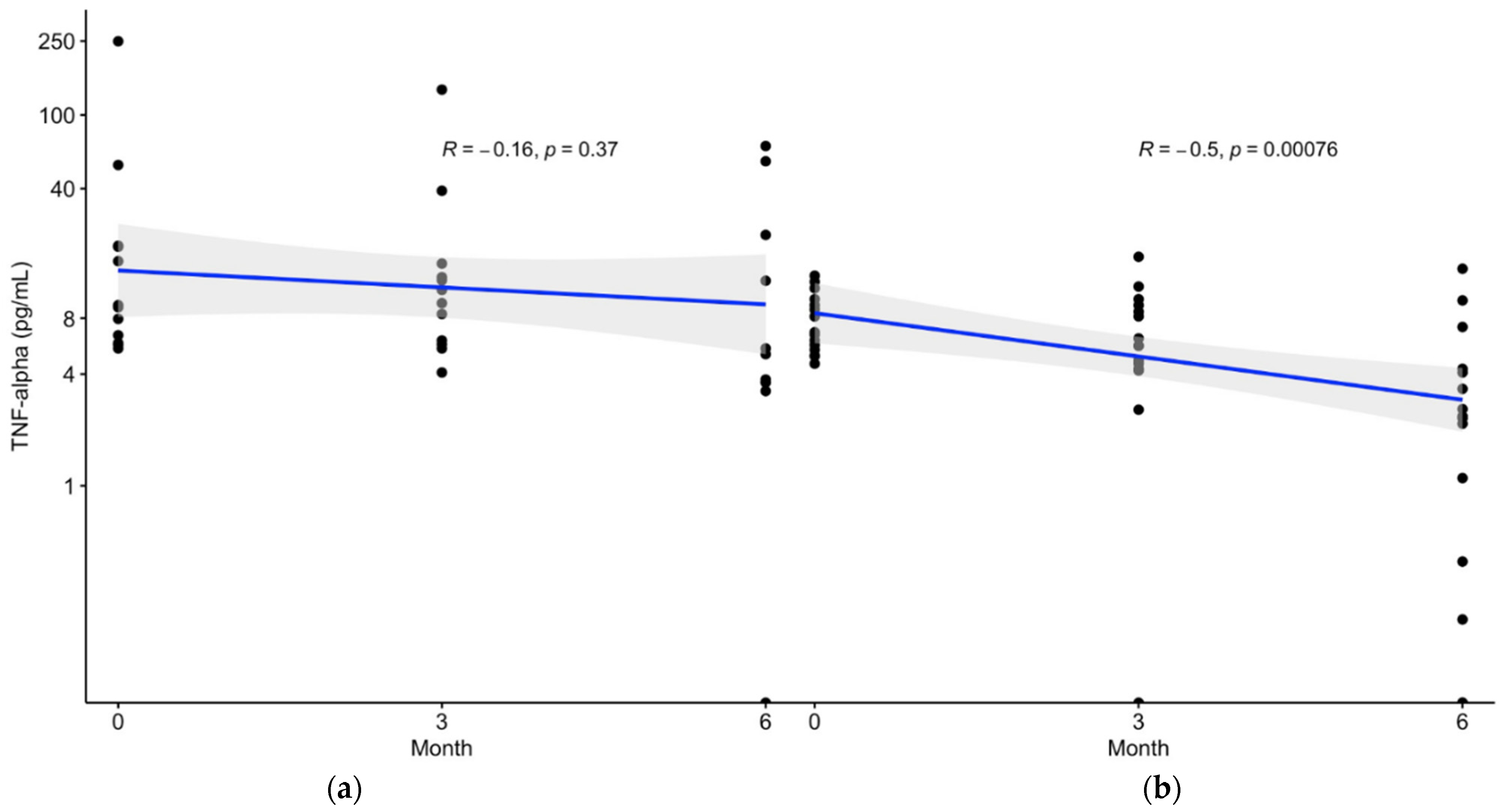
2.4. Sequential Correlation of Serum TNF-α Concentration and Time Exhibited in the Patients with Prediabetes Receiving FCE
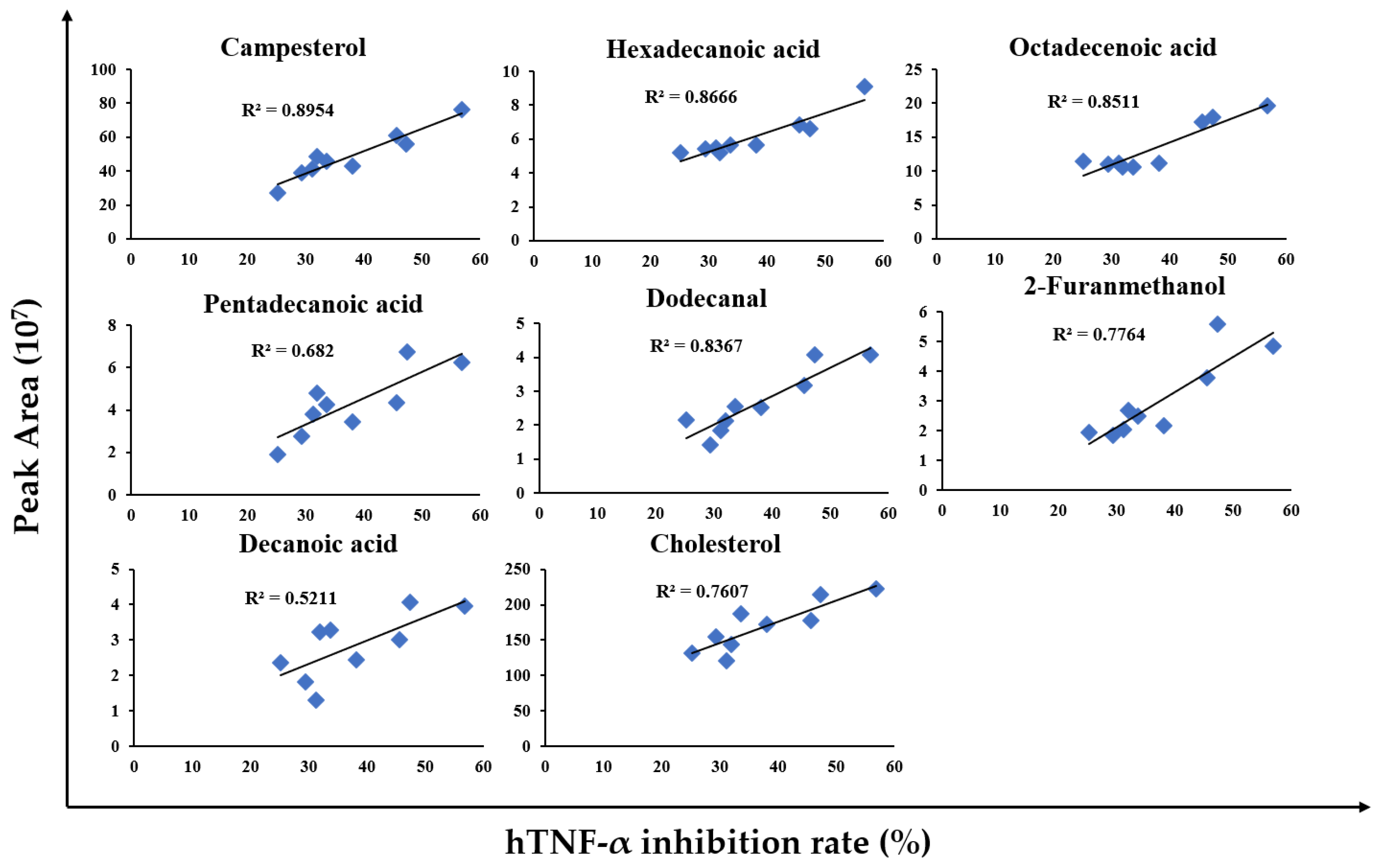
2.5. A Detailed Analysis of FCE Reveals That the Major Bioactive Compounds Derived from FCE Were Highly Associated with Anti-TNF-α Effects
3. Discussion
4. Materials and Methods
4.1. Subjects and Study Design
4.2. Preparation of Freshwater Clam Extract (FCE)
4.3. FCE Intervention
4.4. Anthropometric Parameters, Biochemistry Assays, and TNF-α Measurement
4.5. Gas Chromatography–Mass Spectrometry Analysis (GC-MS)
4.6. Cell Culture, LPS Stimulation, and Cytokine Measurement
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khetan, A.K.; Rajagopalan, S. Prediabetes. Can. J. Cardiol. 2018, 34, 615–623. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- Echouffo-Tcheugui, J.B.; Selvin, E. Prediabetes and What It Means: The Epidemiological Evidence. Annu. Rev. Public Health 2021, 42, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.K.; Bullard, K.M.; Saydah, S.; Imperatore, G.; Gregg, E.W. Cardiovascular and renal burdens of prediabetes in the USA: Analysis of data from serial cross-sectional surveys, 1988–2014. Lancet Diabetes Endocrinol. 2018, 6, 392–403. [Google Scholar] [CrossRef]
- American Diabetes Association. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S32–S36. [Google Scholar] [CrossRef] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Pan, X.R.; Li, G.W.; Hu, Y.H.; Wang, J.X.; Yang, W.Y.; An, Z.X.; Hu, Z.X.; Lin, J.; Xiao, J.Z.; Cao, H.B.; et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.D.; Vijay, V. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Knowler, W.C.; Hamman, R.F.; Edelstein, S.L.; Barrett-Connor, E.; Ehrmann, D.A.; Walker, E.A.; Fowler, S.E.; Nathan, D.M.; Kahn, S.E. Prevention of type 2 diabetes with troglitazone in the Diabetes Prevention Program. Diabetes 2005, 54, 1150–1156. [Google Scholar] [CrossRef]
- Pi-Sunyer, X.; Astrup, A.; Fujioka, K.; Greenway, F.; Halpern, A.; Krempf, M.; Lau, D.C.W.; le Roux, C.W.; Violante Ortiz, R.; Jensen, C.B.; et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N. Engl. J. Med. 2015, 373, 11–22. [Google Scholar] [CrossRef]
- Bosch, J.; Yusuf, S.; Gerstein, H.C.; Pogue, J.; Sheridan, P.; Dagenais, G.; Diaz, R.; Avezum, A.; Lanas, F.; Probstfield, J.; et al. Effect of ramipril on the incidence of diabetes. N. Engl. J. Med. 2006, 355, 1551–1562. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, K.F.; Pietrani, N.T.; Bosco, A.A.; Campos, F.M.e.F.; Sandrim, V.r.C.; Gomes, K.B. IL-6, TNF-±, and IL-10 levels/polymorphisms and their association with type 2 diabetes mellitus and obesity in Brazilian individuals. Arch. Endocrinol. Metab. 2017, 61, 438–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, N.; Julián, M.T.; Vives-Pi, M.; Puig-Domingo, M. Incretin hormones as immunomodulators of atherosclerosis. Front. Endocrinol. 2012, 3, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Feng, X.; Li, Q.; Wang, Y.; Li, Q.; Hua, M. Adiponectin, TNF-α and inflammatory cytokines and risk of type 2 diabetes: A systematic review and meta-analysis. Cytokine 2016, 86, 100–109. [Google Scholar] [CrossRef]
- Lainampetch, J.; Panprathip, P.; Phosat, C.; Chumpathat, N.; Prangthip, P.; Soonthornworasiri, N.; Puduang, S.; Wechjakwen, N.; Kwanbunjan, K. Association of Tumor Necrosis Factor Alpha, Interleukin 6, and C-Reactive Protein with the Risk of Developing Type 2 Diabetes: A Retrospective Cohort Study of Rural Thais. J. Diabetes Res. 2019, 2019, 9051929. [Google Scholar] [CrossRef] [Green Version]
- Akash, M.S.H.; Rehman, K.; Liaqat, A. Tumor Necrosis Factor-Alpha: Role in Development of Insulin Resistance and Pathogenesis of Type 2 Diabetes Mellitus. J. Cell Biochem. 2018, 119, 105–110. [Google Scholar] [CrossRef]
- Bryant, N.J.; Govers, R.; James, D.E. Regulated transport of the glucose transporter GLUT4. Nat. Rev. Mol. Cell Biol. 2002, 3, 267–277. [Google Scholar] [CrossRef]
- Gao, Z.; Hwang, D.; Bataille, F.; Lefevre, M.; York, D.; Quon, M.J.; Ye, J. Serine phosphorylation of insulin receptor substrate 1 by inhibitor kappa B kinase complex. J. Biol. Chem. 2002, 277, 48115–48121. [Google Scholar] [CrossRef] [Green Version]
- Akash, M.S.H.; Shen, Q.; Rehman, K.; Chen, S. Interleukin-1 receptor antagonist: A new therapy for type 2 diabetes mellitus. J. Pharm. Sci. 2012, 101, 1647–1658. [Google Scholar] [CrossRef]
- Rehman, K.; Akash, M.S.H. Mechanisms of inflammatory responses and development of insulin resistance: How are they interlinked? J. Biomed. Sci. 2016, 23, 87. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Ma, C.; Li, P.; Ma, C.; He, S.; Ping, F.; Zhang, H.; Li, W.; Xu, L.; Li, Y. Potential Protective Effect of Dietary Intake of Non-α-Tocopherols on Cellular Aging Markers Mediated by Tumor Necrosis Factor-α in Prediabetes: A Cross-Sectional Study of Chinese Adults. Oxid. Med. Cell. Longev. 2020, 2020, 7396801. [Google Scholar] [CrossRef] [PubMed]
- Popa, C.; Netea, M.G.; van Riel, P.L.; van der Meer, J.W.; Stalenhoef, A.F. The role of TNF-alpha in chronic inflammatory conditions, intermediary metabolism, and cardiovascular risk. J. Lipid Res. 2007, 48, 751–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.M.; Lin, Y.L.; Tsai, N.M.; Wu, H.Y.; Ho, S.Y.; Chen, C.H.; Liu, Y.K.; Chiu, Y.H.; Ho, L.P.; Lee, R.P.; et al. Inhibitory effects of chloroform extracts derived from Corbicula fluminea on the release of pro-inflammatory cytokines. J. Agric. Food Chem. 2012, 60, 4076–4082. [Google Scholar] [CrossRef] [PubMed]
- Pollack, R.M.; Donath, M.Y.; LeRoith, D.; Leibowitz, G. Anti-inflammatory Agents in the Treatment of Diabetes and Its Vascular Complications. Diabetes Care 2016, 39, S244–S252. [Google Scholar] [CrossRef] [Green Version]
- Evans, L.P., Jr.; Murphy, C.E.; Britton, J.C.; Newland, L.W. Salinity Relationships in Corbicula fluminea (Müller). In Proceedings of the First International Corbicula Symposium; Texas Christian University Research Foundation: Texas, TX, USA, 1979; pp. 194–214. [Google Scholar]
- Nedeau, E.S.A.; Stone, J. Freshwater Mussels of the Pacific Northwest; United States Fish and Wildlife Service: Vancouver, WA, USA, 1985; p. 48.
- Huang, K.-C.; Wu, W.-T.; Yang, F.-L.; Chiu, Y.-H.; Peng, T.-C.; Hsu, B.-G.; Liao, K.-W.; Lee, R.-P. Effects of freshwater clam extract supplementation on time to exhaustion, muscle damage, pro/anti-inflammatory cytokines, and liver injury in rats after exhaustive exercise. Molecules 2013, 18, 3825–3838. [Google Scholar] [CrossRef] [Green Version]
- Peng, T.C.; Subeq, Y.M.; Lee, C.J.; Lee, C.C.; Tsai, C.J.; Chang, F.M.; Lee, R.P. Freshwater clam extract ameliorates acute liver injury induced by hemorrhage in rats. Am. J. Chin. Med. 2008, 36, 1121–1133. [Google Scholar] [CrossRef]
- Huang, Y.-T.; Huang, Y.-H.; Hour, T.-C.; Pan, B.S.; Liu, Y.-C.; Pan, M.-H. Apoptosis-inducing active components from Corbicula fluminea through activation of caspase-2 and production of reactive oxygen species in human leukemia HL-60 cells. Food Chem. Toxicol. 2006, 44, 1261–1272. [Google Scholar] [CrossRef]
- Song, E.-J.; Chan, M.W.Y.; Shin, J.-W.; Chen, C.-C. Hard clam extracts induce atypical apoptosis in human gastric cancer cells. Exp. Ther. Med. 2017, 14, 1409–1418. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.L.; Hsu, C.C.; Yen, G.C. Hepatoprotection by freshwater clam extract against CCl4-induced hepatic damage in rats. Am. J. Chin. Med. 2010, 38, 881–894. [Google Scholar] [CrossRef]
- Hua, K.F.; Chen, G.M.; Ho, C.L.; Chen, M.C.; Chen, Y.L.; Chen, W.J.; Huang, J.F.; Perng, Y.S.; Lin, C.C. Freshwater clam extract inhibits inflammatory responses in LPS-activated macrophages by reducing the activation of mitogen-activated protein kinases and NF-kappaB. Nat. Prod. Commun. 2012, 7, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.P.; Subeq, Y.M.; Lee, C.J.; Hsu, B.G.; Peng, T.C. Freshwater clam extract decreased hemorrhagic shock-induced liver injury by attenuating TNF-α production. Biol. Res. Nurs. 2012, 14, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.T.; Lee, P.F.; Lii, C.K.; Liu, Y.T.; Chen, S.H. Freshwater clam extract reduces liver injury by lowering cholesterol accumulation, improving dysregulated cholesterol synthesis and alleviating inflammation in high-fat, high-cholesterol and cholic acid diet-induced steatohepatitis in mice. Food Funct. 2018, 9, 4876–4887. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Xie, F.; Yan, S.; Hu, X.; Jin, B.; Wang, J.; Wu, J.; Yin, D.; Xie, Q. Subhealth: Definition, criteria for diagnosis and potential prevalence in the central region of China. BMC Public Health 2013, 13, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Liu, W.; Zuo, S.; Xie, T.; Deng, H.; Zhang, Q.; Zhong, B. Impaired function of the intestinal barrier in a novel sub-health rat model. Mol. Med. Rep. 2016, 13, 3459–3465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Belwal, T.; Li, L.; Limwachiranon, J.; Liu, X.; Luo, Z. Phytosterols and their derivatives: Potential health-promoting uses against lipid metabolism and associated diseases, mechanism, and safety issues. Compr. Rev. Food Sci. Food Saf. 2020, 19, 1243–1267. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, S.; Ellegård, L.; Johansson, I.; Hallmans, G.; Weinehall, L.; Andersson, H.; Winkvist, A. Inverse relation between dietary intake of naturally occurring plant sterols and serum cholesterol in northern Sweden. Am. J. Clin. Nutr. 2008, 87, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Navarro, A.; De las Heras, B.; Villar, A. Anti-inflammatory and immunomodulating properties of a sterol fraction from Sideritis foetens Clem. Biol. Pharm. Bull. 2001, 24, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Carluccio, M.A.; Massaro, M.; Bonfrate, C.; Siculella, L.; Maffia, M.; Nicolardi, G.; Distante, A.; Storelli, C.; De Caterina, R. Oleic acid inhibits endothelial activation: A direct vascular antiatherogenic mechanism of a nutritional component in the mediterranean diet. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Oh, Y.T.; Lee, J.Y.; Lee, J.; Kim, H.; Yoon, K.S.; Choe, W.; Kang, I. Oleic acid reduces lipopolysaccharide-induced expression of iNOS and COX-2 in BV2 murine microglial cells: Possible involvement of reactive oxygen species, p38 MAPK, and IKK/NF-kappaB signaling pathways. Neurosci. Lett. 2009, 464, 93–97. [Google Scholar] [CrossRef]
- Ogbe, R. A Review of Dietary Phytosterols: Their occurences, metabolism and health benefits. Asian J. Plant Sci. Res. 2015, 5, 10–21. [Google Scholar]
- Salehi, B.; Quispe, C.; Sharifi-Rad, J.; Cruz-Martins, N.; Nigam, M.; Mishra, A.P.; Konovalov, D.A.; Orobinskaya, V.; Abu-Reidah, I.M.; Zam, W.; et al. Phytosterols: From Preclinical Evidence to Potential Clinical Applications. Front. Pharmacol. 2021, 11, 599959. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.J.; Liu, Y.C.; Chang, C.J.; Pan, M.H.; Lee, M.F.; Pan, B.S. Hepatoprotective mechanism of freshwater clam extract alleviates non-alcoholic fatty liver disease: Elucidated in vitro and in vivo models. Food Funct. 2018, 9, 6315–6325. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.S.; Lin, T.C.; Chen, J.L.; Pan, B.S. The inhibitory effects of freshwater clam (Corbicula fluminea, Muller) muscle protein hydrolysates on angiotensin I converting enzyme. Process Biochem. 2006, 41, 2276–2281. [Google Scholar] [CrossRef]
- Pang, T.; Wang, J.; Benicky, J.; Sánchez-Lemus, E.; Saavedra, J.M. Telmisartan directly ameliorates the neuronal inflammatory response to IL-1β partly through the JNK/c-Jun and NADPH oxidase pathways. J. Neuroinflamm. 2012, 9, 102. [Google Scholar] [CrossRef] [Green Version]
- CF, I. Corbicula and Neocorbicula (Bivalvia: Corbiculidae) in the Parana, Uruguay, and Rio de La Plata Basins. Nautilus 1994, 107, 129–135. [Google Scholar]
- Barbour, J.; McMenamin, S.; Dick, J.; Alexander, M.; Caffrey, J. Biosecurity measures to reduce secondary spread of the invasive freshwater Asian clam, Corbicula fluminea (Müller, 1774). Manag. Biol. Invasions 2013, 4, 219–230. [Google Scholar] [CrossRef] [Green Version]
- Matheson, F.E.; Dugdale, A.M.; Wells, R.D.S.; Taumoepeau, A.; Smith, J.P. Efficacy of Saltwater Solutions to Kill Introduced Freshwater Species and Sterilise Freshwater Fishing Nets; Science & Technical Publishing, Department of Conservation: Wellington, New Zealand, 2007.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Placebo Group | Freshwater Clam Extract Group | p Value | ||
|---|---|---|---|---|---|
| (n = 17) | (n = 19) | ||||
| n | % | n | % | ||
| Sex | 0.1052 | ||||
| Female | 12 | 70.59 | 12 | 63.16 | |
| Male | 5 | 29.41 | 7 | 36.84 | |
| Age, years (SD) | 54.47 (10.61) | 52.95 (8.78) | 0.6405 | ||
| 25–45 | 2 | 11.76 | 5 | 26.32 | |
| 45–65 | 13 | 76.47 | 12 | 63.16 | |
| over 65 | 2 | 11.76 | 2 | 10.53 | |
| Height, cm (SD) | 157.81 (8.51) | 159.47 (6.88) | 0.5231 | ||
| Weight, kg (SD) | 61.90 (11.19) | 66.60 (13.54) | 0.2731 | ||
| BMI, kg/m2 (SD) | 24.80 (3.84) | 26.01 (3.85) | 0.3545 | ||
| <18.5 | 0 | 0 | 0 | 0 | |
| 18.5–23.9 | 7 | 41.18 | 7 | 36.84 | |
| 24–26.9 | 5 | 29.41 | 5 | 26.32 | |
| 27–29.9 | 3 | 17.65 | 4 | 21.05 | |
| 30–34.9 | 2 | 11.76 | 3 | 15.79 | |
| ≥35 | 0 | 0 | 0 | 0 | |
| Placebo Group | Freshwater Clam Extract Powder Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 Months | 3 Months | 6 Months | 12 Months | p Value | 0 Months | 3 Months | 6 Months | 12 Months | p Value | |
| n = 17 | n = 17 | n = 16 | n = 13 | n = 19 | n = 19 | n = 19 | n = 16 | |||
| TNF-α, pg/mL | 8.56 (12.85) | 9.04 (7.63) | 4.43 (11.67) | 2.99 (2.35) | 0.784 | 6.31 (4.28) | 5.96 (4.71) | 2.48 (2.91) | 3.06 (3.71) | <0.001 |
| ALT, U/L | 24.1 (10.4) | 23.2 (10.4) | 23.2 (10.2) | 28.8 (18.0) | 0.587 | 34.5 (32.7) | 33.6 (28.7) | 32.8 (23.4) | 32.1 (41.4) | 0.996 |
| AST, U/L | 22.1 (4.79) | 20.0 (3.91) | 20.8 (4.97) | 22.9 (7.62) | 0.443 | 23.7 (8.44) | 24.2 (9.10) | 22.7 (7.99) | 21.1 (9.49) | 0.744 |
| UA, mg/dL | 5.18 (1.54) | 5.23 (1.56) | 5.40 (1.75) | 5.48 (1.88) | 0.955 | 5.88 (1.70) | 6.00 (1.69) | 5.69 (1.60) | 5.47 (1.40) | 0.790 |
| CRE, mg/dL | 0.74 (0.15) | 0.73 (0.15) | 0.76 (0.18) | 0.72 (0.16) | 0.942 | 0.81 (0.23) | 0.84 (0.24) | 0.82 (0.21) | 0.80 (0.22) | 0.957 |
| BUN, mg/dL | 15.1 (3.81) | 14.5 (4.32) | 14.7 (3.24) | 14.9 (3.45) | 0.972 | 14.2 (3.66) | 14.5 (2.93) | 15.0 (3.07) | 14.5 (2.95) | 0.893 |
| ALB, g/dL | 4.47 (0.30) | 4.41 (0.27) | 4.54 (0.28) | 4.44 (0.41) | 0.669 | 4.56 (0.22) | 4.60 (0.24) | 4.55 (0.24) | 4.48 (0.32) | 0.526 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, T.-H.; Ke, C.-H.; Chen, C.-C.; Chuang, C.-H.; Liao, K.-W.; Shiao, Y.-H.; Lin, C.-S. The Effects of Freshwater Clam (Corbicula fluminea) Extract on Serum Tumor Necrosis Factor-Alpha (TNF-α) in Prediabetic Patients in Taiwan. Mar. Drugs 2022, 20, 261. https://doi.org/10.3390/md20040261
Huang T-H, Ke C-H, Chen C-C, Chuang C-H, Liao K-W, Shiao Y-H, Lin C-S. The Effects of Freshwater Clam (Corbicula fluminea) Extract on Serum Tumor Necrosis Factor-Alpha (TNF-α) in Prediabetic Patients in Taiwan. Marine Drugs. 2022; 20(4):261. https://doi.org/10.3390/md20040261
Chicago/Turabian StyleHuang, Tse-Hung, Chiao-Hsu Ke, Chin-Chang Chen, Cheng-Hsun Chuang, Kuang-Wen Liao, Yi-Hsien Shiao, and Chen-Si Lin. 2022. "The Effects of Freshwater Clam (Corbicula fluminea) Extract on Serum Tumor Necrosis Factor-Alpha (TNF-α) in Prediabetic Patients in Taiwan" Marine Drugs 20, no. 4: 261. https://doi.org/10.3390/md20040261