
Establishment of an Individual-Specific Nomogram for Predicting the Risk of Left Ventricular Hypertrophy in Chinese Postmenopausal Hypertensive Women
Abstract
:1. Introduction
2. Methods
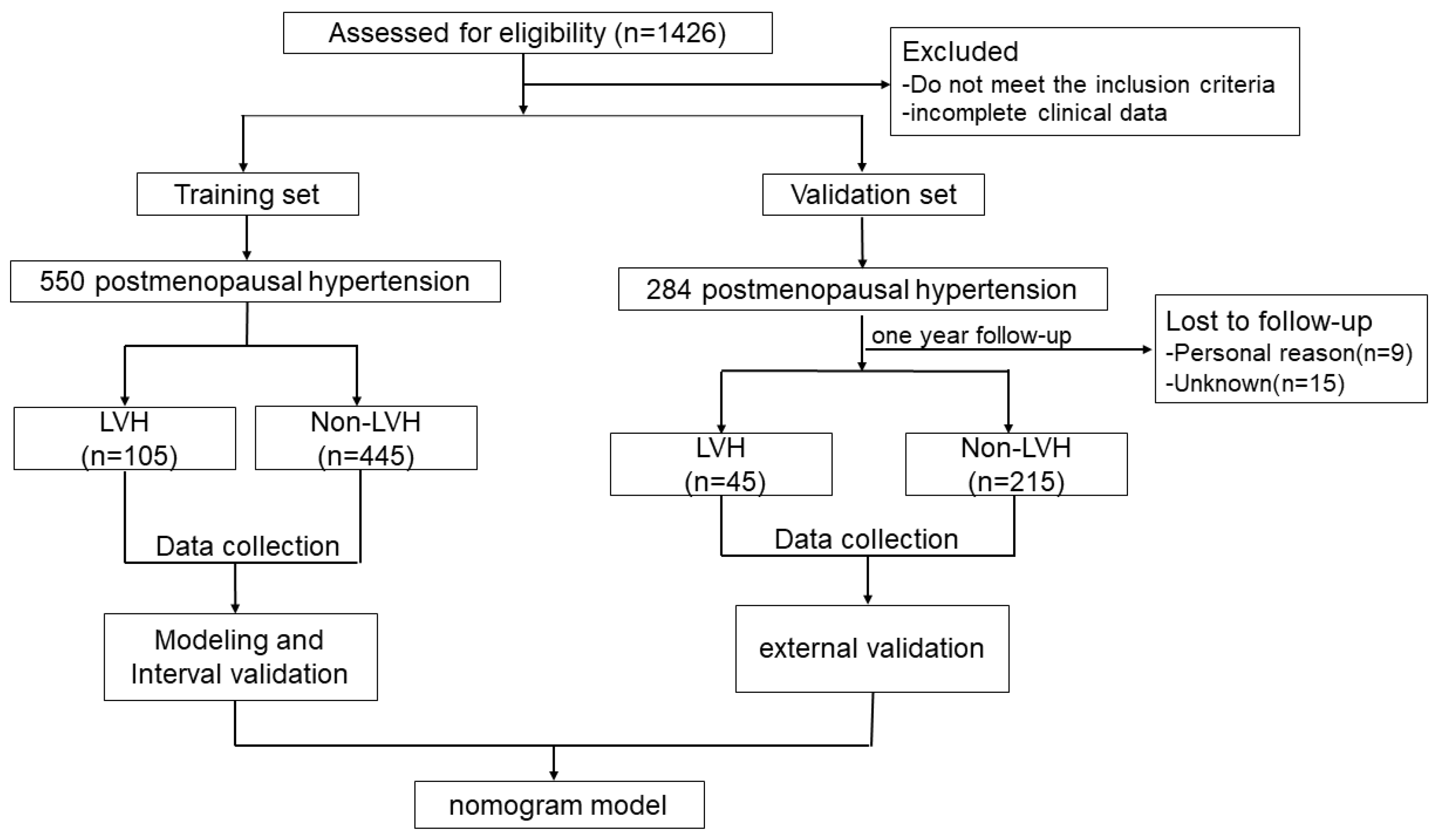
2.1. Trial Design and Participants
2.2. Clinical Data Collection
2.3. Echocardiography
2.4. Laboratory Testing
2.5. Vascular Function
2.6. Questionnaire Survey
2.7. Follow-Up
3. Statistical Analysis
4. Results
4.1. Baseline Characteristics and Risk Factors of LVH Women with Postmenopausal Hypertension
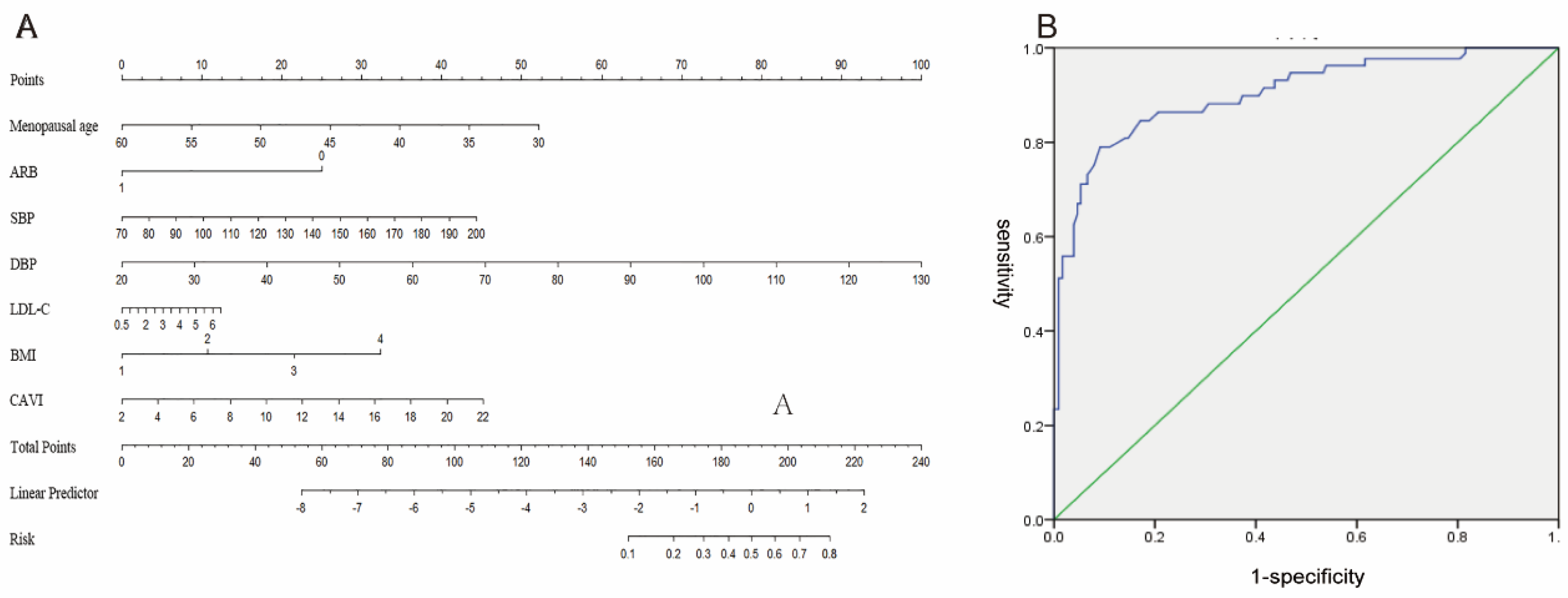
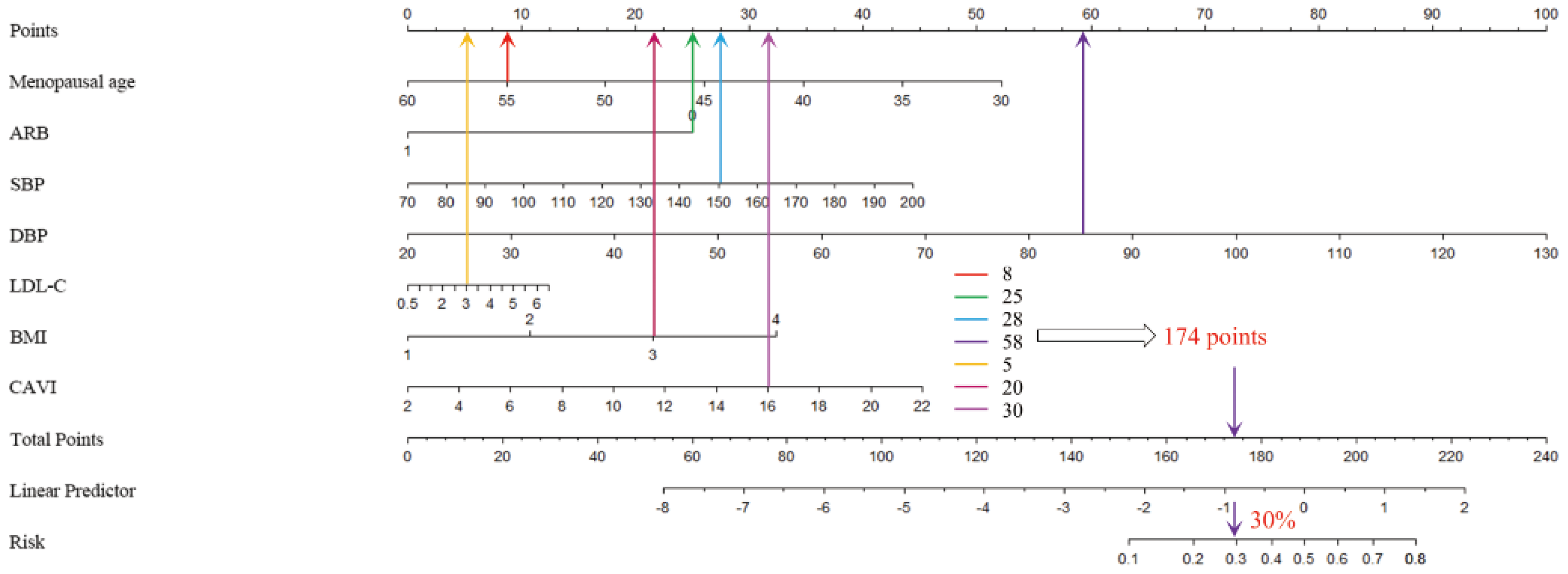
4.2. Establishment and Internal Validation of LVH-Predictive Nomogram
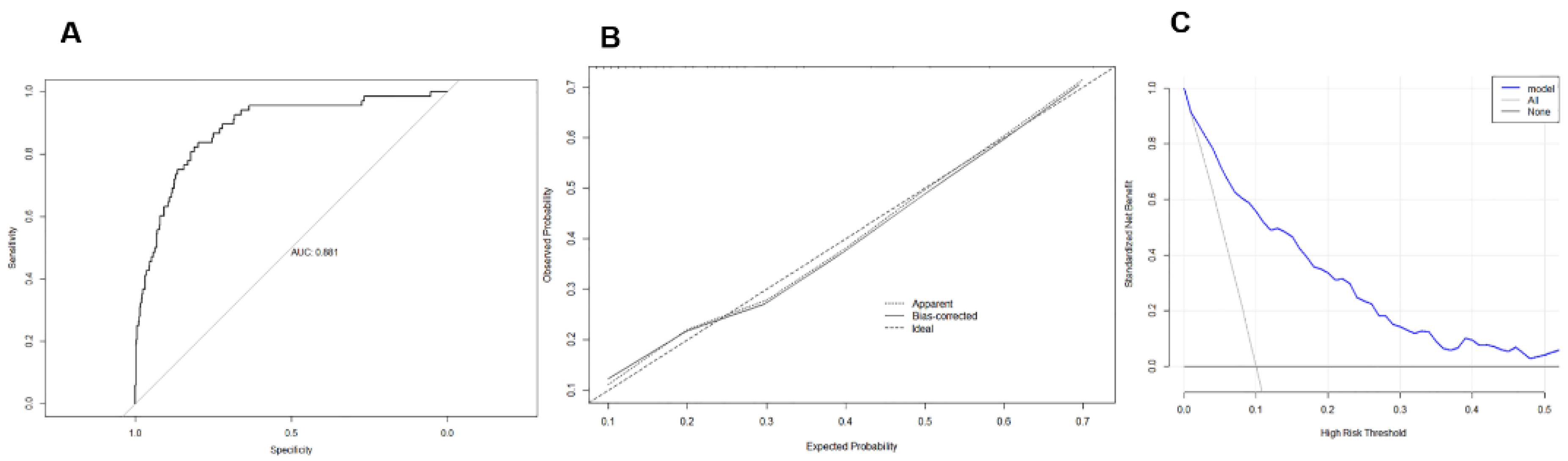
4.3. External Validation of LVH-Predictive Nomogram
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buford, T.W. Hypertension and aging. Ageing Res. Rev. 2016, 26, 96–111. [Google Scholar] [CrossRef] [Green Version]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Executive Summary: Heart Disease and Stroke Statistics--2016 Update: A Report From the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, M.; Oktay, A.A.; Stewart, M.H.; Milani, R.V.; Ventura, H.O.; Lavie, C.J. Left ventricular hypertrophy and hypertension. Prog. Cardiovasc. Dis. 2020, 63, 10–21. [Google Scholar] [CrossRef]
- Maugeri, A.; Hruskova, J.; Jakubik, J.; Barchitta, M.; Lo Re, O.; Kunzova, S.; Medina-Inojosa, J.R.; Agodi, A.; Sciacca, S.; Vinciguerra, M. Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study. J. Clin. Med. 2019, 8, 370. [Google Scholar] [CrossRef] [Green Version]
- Luczak, E.D.; Leinwand, L.A. Sex-based cardiac physiology. Annu. Rev. Physiol. 2009, 71, 1–18. [Google Scholar] [CrossRef]
- Thomopoulos, C.; Parati, G.; Zanchetti, A. Effects of blood pressure lowering on outcome incidence in hypertension: 2. Effects at different baseline and achieved blood pressure levels--overview and meta-analyses of randomized trials. J. Hypertens. 2014, 32, 2296–2304. [Google Scholar] [CrossRef]
- Olszanecka, A.; Kawecka-Jaszcz, K.; Czarnecka, D. Association of free testosterone and sex hormone binding globulin with metabolic syndrome and subclinical atherosclerosis but not blood pressure in hypertensive perimenopausal women. Arch. Med. Sci. AMS 2016, 12, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Guallar, E.; Ouyang, P.; Subramanya, V.; Vaidya, D.; Ndumele, C.E.; Lima, J.A.; Allison, M.A.; Shah, S.J.; Bertoni, A.G.; et al. Endogenous Sex Hormones and Incident Cardiovascular Disease in Post-Menopausal Women. J. Am. Coll. Cardiol. 2018, 71, 2555–2566. [Google Scholar] [CrossRef]
- Yu, S.; Yang, H.; Guo, X.; Zheng, L.; Sun, Y. Hyperuricemia is independently associated with left ventricular hypertrophy in post-menopausal women but not in pre-menopausal women in rural Northeast China. Gynecol. Endocrinol. 2015, 31, 736–741. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [Green Version]
- Brahmbhatt, Y.; Gupta, M.; Hamrahian, S. Hypertension in Premenopausal and Postmenopausal Women. Curr. Hypertens. Rep. 2019, 21, 74. [Google Scholar] [CrossRef]
- Jianshu, C.; Qiongying, W.; Ying, P.; Ningyin, L.; Junchen, H.; Jing, Y. Association of free androgen index and sex hormone-binding globulin and left ventricular hypertrophy in postmenopausal hypertensive women. J. Clin. Hypertens. 2021, 23, 1413–1419. [Google Scholar] [CrossRef]
- Kokkinos, P.; Faselis, C.; Myers, J.; Pittaras, A.; Sui, X.; Zhang, J.; McAuley, P.; Kokkinos, J.P. Cardiorespiratory fitness and the paradoxical BMI-mortality risk association in male veterans. Mayo Clin. Proc. 2014, 89, 754–762. [Google Scholar] [CrossRef]
- Kario, K.; Park, S.; Buranakitjaroen, P.; Chia, Y.C.; Chen, C.H.; Divinagracia, R.; Hoshide, S.; Shin, J.; Siddique, S.; Sison, J.; et al. Guidance on home blood pressure monitoring: A statement of the HOPE Asia Network. J. Clin. Hypertens. 2018, 20, 456–461. [Google Scholar] [CrossRef] [Green Version]
- Hayakawa, M.; Yano, Y.; Kuroki, K.; Inoue, R.; Nakanishi, C.; Sagara, S.; Koga, M.; Kubo, H.; Imakiire, S.; Aoyagi, Z.; et al. Independent association of cognitive dysfunction with cardiac hypertrophy irrespective of 24-h or sleep blood pressure in older hypertensives. Am. J. Hypertens. 2012, 25, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, J.M.; Houman, J.; Caron, A.T.; Patel, D.N.; Baskin, A.S.; Ackerman, A.L.; Eilber, K.S.; Anger, J.T. Female Sexual Dysfunction and the Placebo Effect: A Meta-analysis. Obstet. Gynecol. 2018, 132, 453–458. [Google Scholar] [CrossRef]
- Hsieh, B.P.; Pham, M.X.; Froelicher, V.F. Prognostic value of electrocardiographic criteria for left ventricular hypertrophy. Am. Heart J. 2005, 150, 161–167. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Ke, Y.; Bertin, J.; Gonthier, R.; Simard, J.N.; Labrie, F. A sensitive, simple and robust LC-MS/MS method for the simultaneous quantification of seven androgen- and estrogen-related steroids in postmenopausal serum. J. Steroid Biochem. Mol. Biol. 2014, 144 Pt B, 523–534. [Google Scholar] [CrossRef]
- Rothman, M.S.; Carlson, N.E.; Xu, M.; Wang, C.; Swerdloff, R.; Lee, P.; Goh, V.H.; Ridgway, E.C.; Wierman, M.E. Reexamination of testosterone, dihydrotestosterone, estradiol and estrone levels across the menstrual cycle and in postmenopausal women measured by liquid chromatography-tandem mass spectrometry. Steroids 2011, 76, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Lobo, R.A.; Davis, S.R.; De Villiers, T.J.; Gompel, A.; Henderson, V.W.; Hodis, H.N.; Lumsden, M.A.; Mack, W.J.; Shapiro, S.; Baber, R.J. Prevention of diseases after menopause. Climacteric J. Int. Menopause Soc. 2014, 17, 540–556. [Google Scholar] [CrossRef]
- Ren, J.; Kelley, R.O. Cardiac health in women with metabolic syndrome: Clinical aspects and pathophysiology. Obesity 2009, 17, 1114–1123. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; Zhao, G.; Tsai, J. Trends in obesity and abdominal obesity among adults in the United States from 1999–2008. Int. J. Obes. 2011, 35, 736–743. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M.H.; Lavie, C.J.; Shah, S.; Englert, J.; Gilliland, Y.; Qamruddin, S.; Dinshaw, H.; Cash, M.; Ventura, H.; Milani, R. Prognostic Implications of Left Ventricular Hypertrophy. Prog. Cardiovasc. Dis. 2018, 61, 446–455. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O.; Cardenas, G.A.; Mehra, M.R.; Messerli, F.H. Disparate effects of left ventricular geometry and obesity on mortality in patients with preserved left ventricular ejection fraction. Am. J. Cardiol. 2007, 100, 1460–1464. [Google Scholar] [CrossRef]
- Gosse, P.; Lasserre, R.; Minifié, C.; Lemetayer, P.; Clementy, J. Blood pressure surge on rising. J. Hypertens. 2004, 22, 1113–1118. [Google Scholar] [CrossRef]
- Ikeda, T.; Gomi, T.; Shibuya, Y.; Matsuo, K.; Kosugi, T.; Oku, N.; Uetake, Y.; Kinugasa, S.; Furutera, R. Morning rise in blood pressure is a predictor of left ventricular hypertrophy in treated hypertensive patients. Hypertens. Res. 2004, 27, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Shibamiya, T.; Obara, T.; Ohkubo, T.; Shinki, T.; Ishikura, K.; Yoshida, M.; Satoh, M.; Hashimoto, T.; Hara, A.; Metoki, H.; et al. Electrocardiographic abnormalities and home blood pressure in treated elderly hypertensive patients: Japan home versus office blood pressure measurement evaluation in the elderly (J-HOME-Elderly) study. Hypertens. Res. 2010, 33, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Mirabito Colafella, K.M.; Bovée, D.M.; Danser, A.H.J. The renin-angiotensin-aldosterone system and its therapeutic targets. Exp. Eye Res. 2019, 186, 107680. [Google Scholar] [CrossRef]
- Serfozo, P.; Wysocki, J.; Gulua, G.; Schulze, A.; Ye, M.; Liu, P.; Jin, J.; Bader, M.; Myöhänen, T.; García-Horsman, J.A.; et al. Ang II (Angiotensin II) Conversion to Angiotensin-(1-7) in the Circulation Is POP (Prolyloligopeptidase)-Dependent and ACE2 (Angiotensin-Converting Enzyme 2)-Independent. Hypertension 2020, 75, 173–182. [Google Scholar] [CrossRef]
- Restrepo, C.; Patel, S.K.; Rethnam, V.; Werden, E.; Ramchand, J.; Churilov, L.; Burrell, L.M.; Brodtmann, A. Left ventricular hypertrophy and cognitive function: A systematic review. J. Hum. Hypertens. 2018, 32, 171–179. [Google Scholar] [CrossRef]
- Vernooij, J.W.; van der Graaf, Y.; Nathoe, H.M.; Bemelmans, R.H.; Visseren, F.L.; Spiering, W. Hypertensive target organ damage and the risk for vascular events and all-cause mortality in patients with vascular disease. J. Hypertens. 2013, 31, 492–499. [Google Scholar] [CrossRef]
- Olaya, B.; Moneta, M.V.; Bobak, M.; Haro, J.M.; Demakakos, P. Cardiovascular risk factors and memory decline in middle-aged and older adults: The English Longitudinal Study of Ageing. BMC Geriatr. 2019, 19, 337. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set (n = 550) | Validation Set (n = 260) | |||||
|---|---|---|---|---|---|---|
| LVH (n = 105) | non-LVH (n = 445) | p Value | LVH (n = 45) | Non-LVH (n = 215) | p Value | |
| menopausal age | 47.69 ± 4.03 | 48.62 ± 3.26 | 0.012 * | 57.1 ± 4.28 | 59.00 ± 3.38 | 0.001 * |
| BMI ≥ 24 (kg/m2) | 64 (61) | 129 (29) | <0.001 | 20 (44) | 60 (28) | 0.029 * |
| WHR | 0.83 ± 0.07 | 0.84 ± 0.06 | 0.141 | 1 ± 0.001 | 1 ± 0.007 | 0.648 |
| SBP (mmHg) | 151.85 ± 15.03 | 141.58 ± 20.91 | <0.001 * | 154.56 ± 13.42 | 143.31 ± 18.74 | <0.001 |
| DBP (mmHg) | 91.73 ± 13.24 | 82.86 ± 13.48 | <0.001 * | 94.96 ± 10.58 | 85.59 ± 13.58 | <0.001 |
| HR (beats/min) | 81.95 ± 12.04 | 78.90 ± 11.48 | 0.016 * | 82.40 ± 12.59 | 80.84 ± 11.89 | 0.430 |
| Educational level (college degree or above), n (%) | 38 (36) | 176 (40) | 0.348 | 18 (40) | 95 (44) | 0.606 |
| Family history of hypertension, n (%) | 67 (64) | 258 (58) | 0.250 | 30 (67) | 135 (63) | 0.623 |
| ACEI, n (%) | 36 (34) | 114 (26) | 0.122 | 6 (13) | 67 (31) | 0.016 * |
| ARB, n (%) | 45 (43) | 328 (74) | <0.001 * | 19 (42) | 140 (65) | 0.004 * |
| BB, n (%) | 24 (23) | 91 (20) | 0.585 | 10 (22) | 55 (26) | 0.636 |
| CCB, n (%) | 75 (71) | 305 (69) | 0.564 | 33 (73) | 152 (71) | 0.723 |
| DIU, n (%) | 25 (24) | 128 (29) | 0.308 | 9 (20) | 57 (27) | 0.316 |
| FSFI score | 17.45 ± 6.95 | 18.23 ± 7.78 | 0.347 | 16.84 ± 8.13 | 17.78 ± 7.11 | 0.434 |
| MMSE score | 26.26 ± 2.10 | 26.92 ± 2.22 | 0.006 * | 25.84 ± 2.40 | 26.88 ± 1.95 | 0.002 * |
| Laboratory | ||||||
| BUN (mmol/L) | 4.85 ± 1.58 | 4.66 ± 1.30 | 0.195 | 4.78 ± 1.24 | 4.67 ± 1.24 | 0.596 |
| CR (μmol/L) | 60.27 ± 9.17 | 61.15 ± 9.78 | 0.400 | 59.44 ± 7.82 | 60.75 ± 9.58 | 0.391 |
| TC (mmol/L) | 4.69 ± 0.73 | 4.71 ± 0.88 | 0.825 | 4.62 ± 0.78 | 4.70 ± 0.83 | 0.590 |
| TG (mmol/L) | 1.74 ± 1.32 | 1.69 ± 0.95 | 0.698 | 3.00 ± 1.78 | 1.68 ± 1.03 | 0.530 |
| LDL-C (mmol/L) | 2.75 ± 0.75 | 2.56 ± 0.69 | 0.010 * | 2.81 ± 0.82 | 2.54 ± 0.68 | 0.019 * |
| proteinuria, n (%) | 5 (5) | 13 (3) | 0.340 | 5 (11) | 13 (6) | 0.224 |
| Echocardiography | ||||||
| LVEDD (mm) | 43.74 ± 3.88 | 40.44 ± 2.93 | <0.001 | 43.07 ± 2.98 | 41.15 ± 1.96 | <0.001 |
| IVST (mm) | 11.58 ± 1.03 | 9.83 ± 0.78 | <0.001 | 11.93 ± 1.00 | 10.44 ± 0.73 | <0.001 |
| LVPWT (mm) | 11.63 ± 1.05 | 9.85 ± 0.77 | <0.001 | 11.89 ± 0.82 | 10.50 ± 0.87 | <0.001 |
| LVMI (g/m2) | 104.94 ± 9.71 | 73.13 ± 7.08 | <0.001 | 108.78 ± 10.39 | 81.81 ± 5.57 | <0.001 |
| Vascular function | ||||||
| CAVI (Right) | 8.28 ± 0.98 | 7.99 ± 1.35 | 0.040 * | 8.60 ± 0.81 | 8.14 ± 1.38 | 0.031 * |
| CAVI (Left) | 8.23 ± 0.99 | 7.89 ± 1.22 | 0.008 * | 8.44 ± 0.78 | 8.01 ± 1.12 | 0.015 * |
| LVH (n = 69) | Non-LVH (n = 678) | p Value | |
|---|---|---|---|
| LVEF (%) | 63.10 ± 5.49 | 64.10 ± 2.58 | 0.008 * |
| LVDd (mm) | 43.70 ± 4.25 | 39.82 ± 2.74 | 0.000 * |
| IVSTd (mm) | 11.65 ± 1.15 | 9.54 ± 1.01 | 0.000 * |
| LVPWTd (mm) | 11.64 ± 1.18 | 9.55 ± 0.99 | 0.000 * |
| RVWT (mm) | 0.54 ± 0.09 | 0.48 ± 0.06 | 0.000 * |
| LAD (mm) | 35.09 ± 5.55 | 29.75 ± 2.80 | 0.000 * |
| LAVi (mL/m2) | 21.46 ± 6.93 | 19.96 ± 3.28 | 0.002 * |
| LVMI (kg/m2) | 106.19 ± 10.05 | 68.63 ± 11.91 | 0.000 * |
| E/e′ | 9.22 ± 3.42 | 7.91 ± 1.64 | 0.000 * |
| PASP (mmHg) | 20.80 ± 8.96 | 19.94 ± 5.13 | 0.224 |
| Risk Factors | Partial Regression Coefficient | SE | OR | 95% CI | p Value |
|---|---|---|---|---|---|
| menopausal age | −0.073 | 0.036 | 0.929 | 0.866–0.998 | 0.044 * |
| BMI | 0.065 | 0.023 | 1.067 | 1.019–1.116 | 0.005 * |
| ARB | −1.521 | 0.262 | 0.219 | 0.131–0.365 | 0.000 * |
| morning SBP | 0.049 | 0.009 | 1.050 | 1.032–1.069 | 0.000 * |
| morning DBP | 0.054 | 0.013 | 1.055 | 1.028–1.083 | 0.003 * |
| LDL-C | 0.378 | 0.149 | 1.460 | 1.090–1.945 | 0.011 * |
| CAVI | 0.347 | 0.111 | 1.415 | 1.139–1.757 | 0.028 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, R.; Chen, J.; Zhang, S.; Zhang, X.; Yu, J. Establishment of an Individual-Specific Nomogram for Predicting the Risk of Left Ventricular Hypertrophy in Chinese Postmenopausal Hypertensive Women. Medicina 2023, 59, 598. https://doi.org/10.3390/medicina59030598
Yuan R, Chen J, Zhang S, Zhang X, Yu J. Establishment of an Individual-Specific Nomogram for Predicting the Risk of Left Ventricular Hypertrophy in Chinese Postmenopausal Hypertensive Women. Medicina. 2023; 59(3):598. https://doi.org/10.3390/medicina59030598
Chicago/Turabian StyleYuan, Ruowen, Jianshu Chen, Shangyun Zhang, Xiaowei Zhang, and Jing Yu. 2023. "Establishment of an Individual-Specific Nomogram for Predicting the Risk of Left Ventricular Hypertrophy in Chinese Postmenopausal Hypertensive Women" Medicina 59, no. 3: 598. https://doi.org/10.3390/medicina59030598