
A Need for Improvement in the Definition of Resistant Arterial Hypertension

Abstract
:1. Introduction
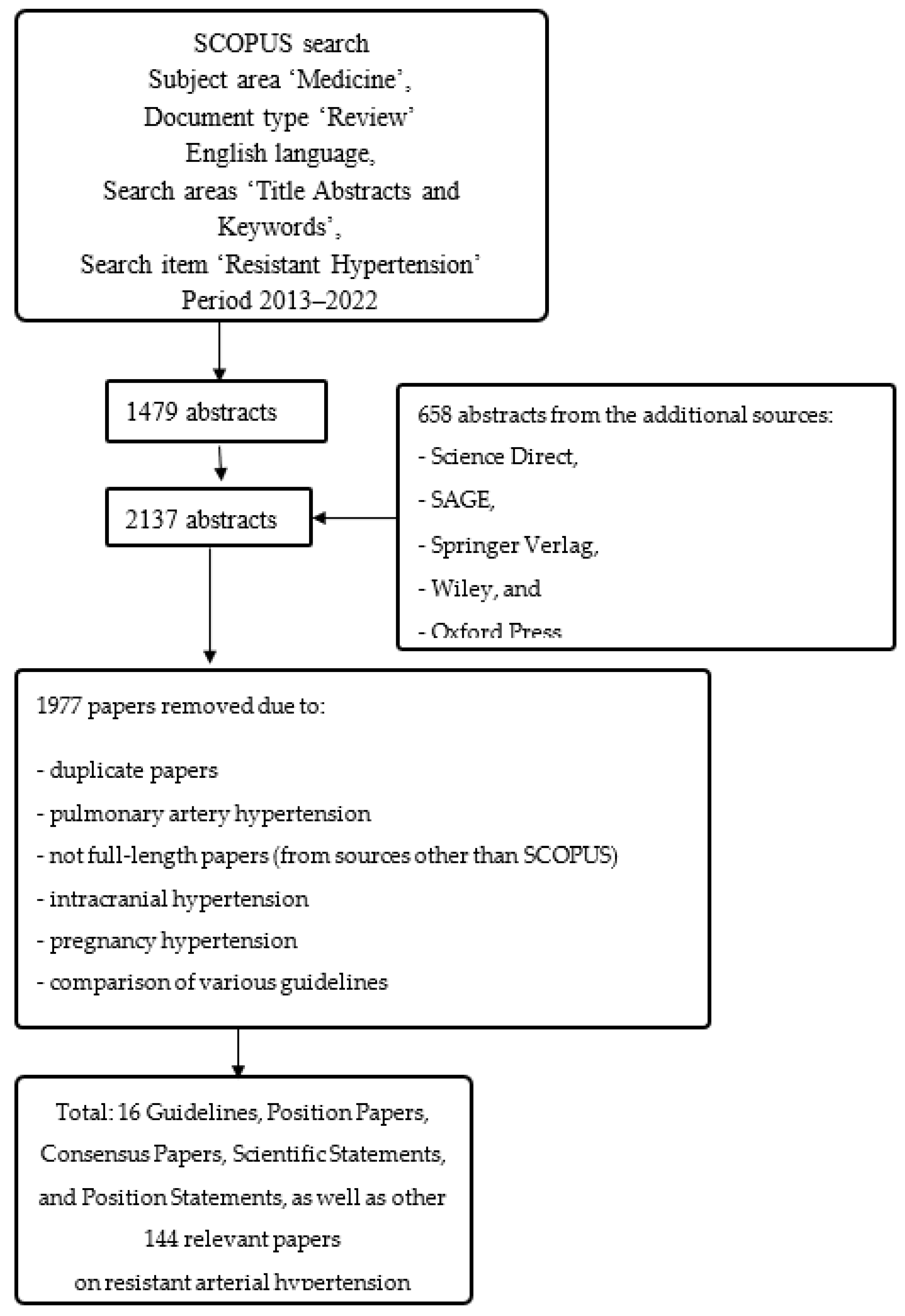
2. Materials and Methods
3. Results
- (A)
- The definitions of normal BP are geographically unequal—they are not the same in Europe and USA [6].
- (B)
- BP cut-offs to define normal BP have changed over time, and probably will continue to do so. If we omit exact BP cut-offs directly in the definition, it will stay the same over time (e.g., failure to obtain normal/target/controlled BP despite optimal (as suggested by the guidelines), triple antihypertensive drugs treatment, and non-medicament antihypertensive treatment) and the essence of the definition would be easier to interpret over time. The only thing that probably will change are the cut-offs for normal/target BP, which ought to be stated in the next sentence following the definition of the BP cut-off.
- (C)
- Cut-offs for resistant HTN depend on the method used for the measurement [73].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Brant, L.C.C.; Passaglia, L.G.; Pinto-Filho, M.M.; de Castilho, F.M.; Ribeiro, A.L.P.; Nascimento, B.R. The Burden of Resistant Hypertension Across the World. Curr. Hypertens. Rep. 2022, 24, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, S.; Sapir-Pichhadze, R.; Nakhla, M.; Gabor, J.Y.; Khan, N.A.; Kuyper, L.M.; Ruzicka, M.; Tobe, S.W.; Tran, K.; Rabi, D.M.; et al. Hypertension Canada’s 2020 Evidence Review and Guidelines for the Management of Resistant Hypertension. Can. J. Cardiol. 2020, 36, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.M.; Jhund, P.S.; Anand, I.S.; Düngen, H.-D.; Lam, C.S.P.; Lefkowitz, M.P.; Linssen, G.; Lund, L.H.; Maggioni, A.P.; Pfeffer, M.A.; et al. Sacubitril–valsartan as a treatment for apparent resistant hypertension in patients with heart failure and preserved ejection fraction. Eur. Heart J. 2021, 42, 3741–3752. [Google Scholar] [CrossRef] [PubMed]
- Chia, R.; Pandey, A.; Vongpatanasin, W. Resistant hypertension-defining the scope of the problem. Prog. Cardiovasc. Dis. 2019, 63, 46–50. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive Summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef]
- Vidal-Petiot, E. Editorial: Drug-resistant hypertension and primary aldosteronism. Eur. J. Prev. Cardiol. 2021, 29, e82–e84. [Google Scholar] [CrossRef]
- Sabbahi, A.; Severin, R.; Laddu, D.; Sharman, J.E.; Arena, R.; Ozemek, C. Nonpharmacological Management of Resistant Hypertension. Curr. Cardiol. Rep. 2021, 23, 166. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J.J.; Nansseu, J.R.; Nyaga, U.F.; Sime, P.S.; Francis, I.; Bigna, J.J. Global prevalence of resistant hypertension: A meta-analysis of data from 3.2 million patients. Heart 2019, 105, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Canoy, D.; Nazarzadeh, M.; Copland, E.; Bidel, Z.; Rao, S.; Li, Y.; Rahimi, K. How Much Lowering of Blood Pressure Is Required to Prevent Cardiovascular Disease in Patients with and Without Previous Cardiovascular Disease? Curr. Cardiol. Rep. 2022, 24, 851–860. [Google Scholar] [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Mondal, M.K.; Nessa, A.; Khatun, N. Study of Body Mass Index, Blood Pressure, Serum Sodium in Newly Diagnosed Hypertensive Patients. Mymensingh Med. J. 2023, 32, 355–360. [Google Scholar]
- Rukunuzzaman, M.; Khatun, N.; Nessa, A.; Wahed, F.; Sharmin, A.; Meherubin, I.; Habiba, U.; Afroz, L.; Akhter, T.; Sharmin, T.; et al. Study on Body Mass Index, Serum Total Cholesterol and Serum Triglycerides in Adult Male Hypertensive Patients. Mymensingh Med. J. 2023, 32, 44–48. [Google Scholar] [PubMed]
- Silva, B.; Pinto, F.J. Optimizing Hypertension Control Globally: WHF Roadmap. Curr. Cardiol. Rep. 2022, 24, 2057–2066. [Google Scholar] [CrossRef] [PubMed]
- Koracevic, G.; Stojanovic, M.; Lovic, D.; Zdravkovic, M.; Sakac, D. Certain beta blockers (e.g., bisoprolol) may be reevaluated in hypertension guidelines for patients with left ventricular hypertrophy to diminish the ventricular arrhythmic risk. J. Hum. Hypertens. 2021, 35, 564–576. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.D.; Perry, R.S. Definitely Life but not Definitively. Orig. Life Evol. Biosph. 2006, 36, 515–521. [Google Scholar] [CrossRef]
- Cohn, J.; Kostova, D.; Moran, A.E.; Cobb, L.K.; Pathni, A.K.; Bisrat, D. Blood from a stone: Funding hypertension prevention, treatment, and care in low- and middle-income countries. J. Hum. Hypertens. 2021, 35, 1059–1062. [Google Scholar] [CrossRef]
- Carey, R.M.; Calhoun, D.A.; Bakris, G.L.; Brook, R.D.; Daugherty, S.L.; Dennison-Himmelfarb, C.R.; Egan, B.M.; Flack, J.M.; Gidding, S.S.; Judd, E.; et al. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement from the American Heart Association. Hypertension 2018, 72, e53–e90. [Google Scholar] [CrossRef]
- Lee, C.J.; Ha, J.; Kim, J.Y.; Kim, I.; Ryu, S.K.; Rhee, M.; Lee, J.; Lee, H.; Ihm, S.; Chung, J.W.; et al. Office blood pressure threshold of 130/80 mmHg better predicts uncontrolled out-of-office blood pressure in apparent treatment-resistant hypertension. J. Clin. Hypertens. 2020, 23, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.D.; Chiang, C.E.; Chao, T.H.; Cheng, H.M.; Wu, Y.W.; Wu, Y.J.; Lin, Y.H.; Chen, M.Y.C.; Ueng, K.C.; Chang, W.T.; et al. 2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension. Acta Cardiol. Sin. 2022, 38, 225–325. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; Rich, R.; Humphrey, L.L.; Frost, J.; Forciea, M.A.; Clinical Guidelines Committee of the American College of Physicians; the Commission on Health of the Public and Science of the American Academy of Family Physicians. Pharmacologic Treatment of Hypertension in Adults Aged 60 Years or Older to Higher Versus Lower Blood Pressure Targets: A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians. Ann. Intern. Med. 2017, 166, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Hypertension in Adults: Diagnosis and Management. NICE. Available online: https://www.guidelines.co.uk/cardiovascular/nice-hypertension-guideline/456894 (accessed on 25 April 2022).
- Schmieder, R.E.; Redon, J.; Grassi, G.; Kjeldsen, S.E.; Mancia, G.; Narkiewicz, K.; Parati, G.; Ruilope, L.; van de Borne, P.; Tsioufis, C.; et al. Updated ESH position paper on interventional therapy of resistant hypertension. EuroIntervention 2013, 9, R58–R66. [Google Scholar] [CrossRef] [PubMed]
- Judd, E.; Calhoun, D.A. Apparent and true resistant hypertension: Definition, prevalence and outcomes. J. Hum. Hypertens. 2014, 28, 463–468. [Google Scholar] [CrossRef]
- Durand, H.; Hayes, P.; Morrissey, E.C.; Newell, J.; Casey, M.; Murphy, A.W.; Molloy, G.J. Medication adherence among patients with apparent treatment-resistant hypertension: Systematic review and meta-analysis. J. Hypertens. 2017, 35, 2346–2357. [Google Scholar] [CrossRef]
- Fay, K.S.; Cohen, D.L. Resistant Hypertension in People With CKD: A Review. Am. J. Kidney Dis. 2021, 77, 110–121. [Google Scholar] [CrossRef]
- Hua, Q.; Fan, L.; Li, J. Joint Committee for Guideline Revision 2019 Chinese guideline for the management of hypertension in the elderly. J. Geriatr. Cardiol. 2019, 16, 67–99. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.N.; Munjal, Y.P.; Kamath, S.A.; Wander, G.S.; Mehta, N.; Mukherjee, S.; Kirpalani, A.; Gupta, P.; Shah, H.; Rohatgi, R.; et al. Indian guidelines on hypertension-IV (2019). J. Hum. Hypertens. 2020, 34, 745–758. [Google Scholar] [CrossRef]
- Rabi, D.M.; McBrien, K.A.; Sapir-Pichhadze, R.; Nakhla, M.; Ahmed, S.B.; Dumanski, S.M.; Butalia, S.; Leung, A.A.; Harris, K.C.; Cloutier, L.; et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2020, 36, 596–624. [Google Scholar] [CrossRef]
- Yugar-Toledo, J.C.; Moreno Junior, H.; Gus, M.; Rosito, G.B.A.; Scala, L.C.N.; Muxfeldt, E.S.; Alessi, A.; Brandao, A.A.; Moreira Filho, O.; Feitosa, A.D.D.M.; et al. Brazilian Position Statement on Resistant Hypertension—2020. Arq. Bras. Cardiol. 2020, 114, 576–596. [Google Scholar]
- Nerenberg, K.A.; Zarnke, K.B.; Leung, A.A.; Dasgupta, K.; Butalia, S.; McBrien, K.; Harris, K.C.; Nakhla, M.; Cloutier, L.; Gelfer, M.; et al. Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2018, 34, 506–525. [Google Scholar] [CrossRef]
- Soh, Y.C.; Yap, K.H.; McGrattan, A.; Yasin, S.; Reidpath, D.; Siervo, M.; Mohan, D. Protocol for a systematic review assessing the measurement of dietary sodium intake among adults with elevated blood pressure. BMJ Open 2022, 12, e052175. [Google Scholar] [CrossRef]
- Kurtz, T.W.; Pravenec, M.; DiCarlo, S.E. Will Food and Drug Administration Guidance to Reduce the Salt Content of Processed Foods Reduce Salt Intake and Save Lives? Hypertension 2022, 79, 809–812. [Google Scholar] [CrossRef]
- Cooper, M.; Simpson, J.R.; Klutka, R. Development and validation of a sodium AnaLysis tool (SALT). Nutr. J. 2020, 19, 55. [Google Scholar] [CrossRef]
- Tsioufis, C.; Kasiakogias, A.; Kordalis, A.; Dimitriadis, K.; Thomopoulos, C.; Tsiachris, D.; Vasileiou, P.; Doumas, M.; Makris, T.; Papademetriou, V.; et al. Dynamic resistant hypertension patterns as predictors of cardiovascular morbidity: A 4-year prospective study. J. Hypertens. 2014, 32, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Mohammadifard, N.; Grau, N.; Khosravi, A.; Esmaillzadeh, A.; Feizi, A.; Abdollahi, Z.; Sarrafzadegan, N. Validation and reproducibility of a semi-qualitative food frequency questionnaire for assessment of sodium intake in Iranian population. Nutr. J. 2022, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Almeida, V.; Seto, T.; Banna, J. Considerations for Measurement of Sodium Intake. Am. J. Lifestyle Med. 2020, 14, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Perin, M.S.; Gallani, M.C.B.J.; Andrechuk, C.R.S.; João, T.M.S.; Rhéaume, C.; Cornélio, M.E. What methods have been used to estimate salt intake? A systematic review. Int. J. Food Sci. Nutr. 2019, 71, 22–35. [Google Scholar] [CrossRef]
- Usman, S.; Masyitha, A.; Arafat, I.R. Efficacy of the behavior of low-salt diets in people with high blood pressure: A Literature review. Int. J. Caring Sci. 2019, 12, 542–552. [Google Scholar]
- Xie, H.; Li, J.; Zhu, X.; Li, J.; Yin, J.; Ma, T.; Luo, Y.; He, L.; Bai, Y.; Zhang, G.; et al. Association between healthy lifestyle and the occurrence of cardiometabolic multimorbidity in hypertensive patients: A prospective cohort study of UK Biobank. Cardiovasc. Diabetol. 2022, 21, 199. [Google Scholar] [CrossRef]
- Lopes, S.; Félix, G.; Mesquita-Bastos, J.; Figueiredo, D.; Oliveira, J.; Ribeiro, F. Determinants of exercise adherence and maintenance among patients with hypertension: A narrative review. Rev. Cardiovasc. Med. 2021, 22, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Wakjira, H.; Gobena, T.; Shore, H. Lifestyle modification practice and associated factors among diagnosed hypertensive patients in selected Hospitals in West Arsi Zone, Oromia Regional State, Ethiopia. J. Cardiol. Cardiovasc. Med. 2022, 7, 6–12. [Google Scholar] [CrossRef]
- Smachew, M.; Melak, M.F.; Atenafu, A.; Belew, A.K. Lifestyle Modification Practice and Associated Factors Among Diagnosed Hypertensive Patients in Selected Hospitals in Central Gondar Zone. Nutr. Metab. Insights 2022, 23, 15. [Google Scholar] [CrossRef] [PubMed]
- Kebede, T.; Taddese, Z.; Girma, A. Knowledge, attitude and practices of lifestyle modification and associated factors among hypertensive patients on-treatment follow up at Yekatit 12 General Hospital in the largest city of East Africa: A prospective cross-sectional study. PLoS ONE 2022, 17, e0262780. [Google Scholar] [CrossRef] [PubMed]
- Toft, B.S.; Hörberg, U.; Rasmussen, B. The ups and downs of lifestyle modification: An existential journey among persons with severe obesity. Scand. J. Caring Sci. 2021, 36, 265–274. [Google Scholar] [CrossRef]
- Seixas, A.; Connors, C.; Chung, A.; Donley, T.; Jean-Louis, G. A Pantheoretical Framework to Optimize Adherence to Healthy Lifestyle Behaviors and Medication Adherence: The Use of Personalized Approaches to Overcome Barriers and Optimize Facilitators to Achieve Adherence. JMIR mHealth uHealth 2020, 8, e16429. [Google Scholar] [CrossRef] [PubMed]
- Viana, S.; Salvador, R.; Morouço, P.; Rebelo-Gonçalves, R. The Contribution of Exercise in Telemedicine Monitoring in Reducing the Modifiable Factors of Hypertension—A Multidisciplinary Approach. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; Shah, S.M.; Aburawi, E.H. Medication Adherence and Treatment-Resistant Hypertension in Newly Treated Hypertensive Patients in the United Arab Emirates. J. Clin. Med. 2021, 10, 5036. [Google Scholar] [CrossRef]
- Lamirault, G.; Artifoni, M.; Daniel, M.; Barber-Chamoux, N. Nantes University Hospital working group on hypertension Resistant Hypertension: Novel Insights. Curr. Hypertens. Rev. 2020, 16, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Şahinarslan, A.; Gazi, E.; Aktoz, M.; Özkan, Ç.; Okyay, G.U.; Elalmış, Ö.U.; Belen, E.; Bitigen, A.; Derici, Ü.; Tütüncü, N.B.; et al. Consensus paper on the evaluation and treatment of resistant hypertension by the Turkish Society of Cardiology. Anatol. J. Cardiol. 2020, 24, 137–152. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Petersen, K.S.; Després, J.-P.; Anderson, C.A.; Deedwania, P.; Furie, K.L.; Lear, S.; Lichtenstein, A.H.; Lobelo, F.; Morris, P.B.; et al. Strategies for Promotion of a Healthy Lifestyle in Clinical Settings: Pillars of Ideal Cardiovascular Health: A Science Advisory from the American Heart Association. Circulation 2021, 144, e495–e514. [Google Scholar] [CrossRef]
- Sevild, C.H.; Niemiec, C.P.; Bru, L.E.; Dyrstad, S.M.; Husebø, A.M.L. Initiation and maintenance of lifestyle changes among participants in a healthy life centre: A qualitative study. BMC Public Health 2020, 20, 1006. [Google Scholar] [CrossRef]
- Jones, D.W.; Whelton, P.K.; Allen, N.; Clark, D., III; Gidding, S.S.; Muntner, P.; Nesbitt, S.; Mitchell, N.S.; Townsend, R.; Falkner, B.; et al. Management of Stage 1 Hypertension in Adults with a Low 10-Year Risk for Cardiovascular Disease: Filling a Guidance Gap: A Scientific Statement from the American Heart Association. Hypertension 2021, 77, e58–e67. [Google Scholar] [CrossRef]
- Sohlberg, T.; Bergmark, K.H. Lifestyle and Long-Term Smoking Cessation. Tob. Use Insights 2020, 13, 1–7. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.-Y.; Li, N.; Li, W.A.; Khan, H. Association between psychosocial stress and hypertension: A systematic review and meta-analysis. Neurol. Res. 2017, 39, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Ostroumova, O.D.; Kochetkov, A.I. Worksite hypertension as a model of stress-induced arterial hypertension. Ter. Arkhiv 2018, 90, 123–132. [Google Scholar] [CrossRef]
- Munakata, M. Clinical significance of stress-related increase in blood pressure: Current evidence in office and out-of-office settings. Hypertens. Res. 2018, 41, 553–569. [Google Scholar] [CrossRef]
- Nagele, E.; Jeitler, K.; Horvath, K.; Semlitsch, T.; Posch, N.; Herrmann, K.H.; Grouven, U.; Hermanns, T.; Hemkens, L.; Siebenhofer, A. Clinical effectiveness of stress-reduction techniques in patients with hypertension: Systematic review and meta-analysis. J. Hypertens. 2014, 32, 1936–1944; discussion 1944. [Google Scholar] [CrossRef]
- Koracevic, G.; Lovic, D.; Zdravkovic, M.; Stojanovic, M. Long-lasting, resistant hypertension should be a part of the aortic dissection risk score. Hypertens. Res. 2019, 42, 1836–1838. [Google Scholar] [CrossRef] [PubMed]
- Alsharari, R.; Shantsila, E.; Lip, G.Y.H.; Shantsila, A. Revisiting the diagnosis of ‘resistant hypertension’: What should we do nowadays’. J. Hum. Hypertens. 2021, 36, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Bourque, G.; Hiremath, S. Rethinking Resistant Hypertension. J. Clin. Med. 2022, 11, 1455. [Google Scholar] [CrossRef]
- Clozel, M. Aprocitentan and the endothelin system in resistant hypertension. Can. J. Physiol. Pharmacol. 2022, 100, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Pappaccogli, M.; Di Monaco, S.; Georges, C.M.; Petit, G.; Eula, E.; Ritscher, S.; Lengelé, J.-P.; Fanelli, E.; Severino, F.; Renkin, J.; et al. Predictors of blood pressure control in patients with resistant hypertension after intensive management in two expert centres: The Brussels-Torino experience. Blood Press. 2019, 28, 336–344. [Google Scholar] [CrossRef]
- Koracevic, G.; Micic, S.; Stojanovic, M.; Lovic, D.; Simic, D.; Colic, M.; Koracevic, M.; Stojkovic, A.; Paunovic, M. Compelling Indications Should be Listed for Individual Beta-Blockers (Due to Diversity), Not for the Whole Class. Curr. Vasc. Pharmacol. 2021, 19, 343–346. [Google Scholar] [CrossRef]
- Li, D.; Huo, Z.; Liu, D.; Gong, N.; Zhang, F.; Kong, Y.; Zhang, Y.; Su, X.; Xu, Q.; Feng, J.; et al. Current apparent treatment-resistant hypertension in patients undergoing peritoneal dialysis: A multi-center cross-sectional study. J. Clin. Hypertens. 2022, 24, 493–501. [Google Scholar] [CrossRef]
- Petersen, J.; Malyutina, S.; Ryabikov, A.; Kontsevaya, A.; Kudryavtsev, A.V.; Eggen, A.E.; McKee, M.; Cook, S.; Hopstock, L.A.; Schirmer, H.; et al. Uncontrolled and apparent treatment resistant hypertension: A cross-sectional study of Russian and Norwegian 40–69 year olds. BMC Cardiovasc. Disord. 2020, 20, 135. [Google Scholar] [CrossRef]
- Sarzani, R.; Laureti, G.; Gezzi, A.; Spannella, F.; Giulietti, F. Single-pill fixed-dose drug combinations to reduce blood pressure: The right pill for the right patient. Ther. Adv. Chronic Dis. 2022, 13, 1–19. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef]
- Nugroho, P.; Andrew, H.; Kohar, K.; Noor, C.A.; Sutranto, A.L. Comparison between the world health organization (WHO) and international society of hypertension (ISH) guidelines for hypertension. Ann. Med. 2022, 54, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Chernova, I.; Krishnan, N. Resistant Hypertension Updated Guidelines. Curr. Cardiol. Rep. 2019, 21, 117. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.A.; Williams, J.V.A.; Tran, K.C.; Padwal, R.S. Epidemiology of Resistant Hypertension in Canada. Can. J. Cardiol. 2022, 38, 681–687. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Remarks (Insufficiencies in the Definition of Resistant HTN) | References |
|---|---|
| 1. Different BP cut-offs to diagnose resistant HTN are used. | [1,3,4,18,19,20] |
| 2. sBP values normal-for-the-age for 61 and 81 year old patients in some guidelines fulfill the criterion for resistant HTN. | [6,21,22,23,24,25,26] |
| 3. The number of BP measurements is not specified. | [22,27] |
| 4. The time-frame for the definition is not obtained. | [27,28] |
| 5. Normal or target or controlled BP values have not been provided. | [2,3,6,22,23,29,30,31,32] |
| 6. To what degree do healthy lifestyle measures need to be fulfilled to consider it as sufficient to change the diagnosis from “apparent treatment-resistant HTN” to “resistant HTN”? | [33,34,35] |
| 7. Is there a need to introduce a category of recovered resistant HTN? | [36] |
| 8. Stress is not included in the exclusion strategy for resistant HTN. | [2] |
| 9. It probably ought to read “In the absence of contraindications and compelling indications…”. | n/a |
| 10. The definition usually directly incorporates BP cut-offs for sBP and dBP (which is not an ideal solution from a practical viewpoint). | [1] |
| 11. Secondary HTN is not currently defined as true resistant HTN, but instead as treatment-resistant HTN. | [1] |
| Remarks (Insufficiencies in the Definition of Resistant HTN) | Suggestions for Improvement |
|---|---|
| 1. Different BP cut-offs to diagnose resistant HTN are used. | An international consensus could solve this by setting the sBP cut-off ought to either 130 or 140 mmHg. |
| 2. sBP values considered normal-for-the-age for 61 and 81 year old patients fulfill the criterion for resistant HTN in some guidelines. | This shortcoming may be improved by paying more attention to not mix normal and abnormal BP ranges; it may be stated in the national guidelines that (in the case of differences) international guidelines should have priority in clinical consideration. |
| 3. The number of BP measurements is not specified. | A single BP measurement following the introduction of triple antihypertensive treatment is clearly not enough; dose up-titration needs to be applied. Therefore, at least 3 additional doctor’s office BP measurements are likely needed. |
| 4. The time-frame for the definition is not obtained. | This is clearly a point where consensus is needed; but it depends on several factors. Possibly, for most patients, this time-frame might be a month. |
| 5. Normal, target, and controlled BP values are not provided. | It seems that a failure to achieve target rather than normal BP values can be considered treatment-resistant HTN, because the aim of treatment is to provide target BP. |
| 6. What is the degree to which healthy lifestyle measures need to be fulfilled to consider it as sufficient to change the diagnosis from “apparent treatment-resistant HTN” to “resistant HTN”? | This is important, but difficult to define and it obviously needs scientific work and consensus. |
| 7. Is there a need to introduce a category for recovered resistant HTN? | Although this category is rarely mentioned, the answer seems to be positive. |
| 8. Stress is not included in the exclusion strategy for resistant HTN. | Stress is not easy to predict and measure in routine clinical practice, but it should be considered in each patient, prevented/treated within the limits of reality, and evaluated similarly as other risk factors, e.g., increased salt intake. |
| 9. It probably ought to read “In the absence of contraindications and compelling indications…”. | The answer is positive, because of the high number of various comorbidities in patients with resistant HTN; they represent contraindications for some and compelling indications for the other antihypertensive drugs. |
| 10. The definition usually directly incorporates BP cut-offs for sBP and dBP (which is not an ideal solution from a practical viewpoint for a long time). | This can be solved by using the phrase “above the target BP” possibly with the additional explanation “currently above this cut-off”. |
| 11. Secondary HTN is not currently defined as true resistant HTN, but as apparently treatment-resistant HTN. | Secondary HTN might be considered true resistant HTN, because it usually cannot be controlled by adopting a healthy lifestyle and following other recommended measures. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koracevic, G.; Micic, S.; Stojanovic, M.; Zdravkovic, M. A Need for Improvement in the Definition of Resistant Arterial Hypertension. Medicina 2023, 59, 803. https://doi.org/10.3390/medicina59040803
Koracevic G, Micic S, Stojanovic M, Zdravkovic M. A Need for Improvement in the Definition of Resistant Arterial Hypertension. Medicina. 2023; 59(4):803. https://doi.org/10.3390/medicina59040803
Chicago/Turabian StyleKoracevic, Goran, Sladjana Micic, Milovan Stojanovic, and Marija Zdravkovic. 2023. "A Need for Improvement in the Definition of Resistant Arterial Hypertension" Medicina 59, no. 4: 803. https://doi.org/10.3390/medicina59040803