
The Interference of Age and Gender on Smile Characterization Analyzed on Six Parameters: A Clinical-Photographic Pilot Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection Criteria
2.2. Criteria of Eligibility
2.3. Digital Equipment and Standardizations
2.4. Variables Analyzed
3. Statistical Analysis
4. Results
4.1. Sample Characterization
4.2. Variables Analyzed
5. Discussion
Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Oreški, N.P.; Čelebić, A.; Petričević, N. Assessment of esthetic characteristics of the teeth and surrounding anatomical structures. Acta Stomatol. Croat. 2017, 51, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Okida, R.C.; Moura, A.P.; Franco, L.M.; Salomão, F.M.; Rahal, V.; Machado, L.S.; Okida, D.S.D.S. A utilização do DSD (Digital Smile Design) para a otimização da estética dental. Rev. Odont. Araçatuba 2017, 38, 9–14. [Google Scholar]
- Gyawali, R.; Singh, V.P. Analysis of maxillary anterior teeth proportion in relationship with lower facial height and malocclusion. J. Coll. Med. Sci. Nepal 2017, 13, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Van der Geld, P.; Oosterveld, P.; Van Heck, G.; Kuijpers-Jagtman, A.M. Smile attractiveness: Self-perception and influence on personality. Angle Orthod. 2007, 77, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Soares, G.P.; Valentino, T.A.; Lima, D.A.N.L.; Paulillo, L.A.M.S.; Silva, F.A.P.; Lovadino, J.R. Esthetic analysis of the smile. Braz. J. Oral Sci. 2007, 6, 1313–1319. [Google Scholar]
- Suguino, R.; Ramos, A.L.; Terada, H.H.; Furquim, L.Z.; Maeda, L.; Silva Filho, O.G. Análise Facial. Rev. Dent. Press Ortod. Ortop. Maxilar 1996, 1, 86–107. [Google Scholar]
- Bhuvaneswaran, M. Principles of smile design. J. Conserv. Dent. JCD 2010, 13, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Hashim, P.W.; Nia, J.K.; Taliercio, M.; Goldenberg, G. Ideals of facial beauty. Cosmet. Dermatol. 2017, 100, 222–224. [Google Scholar]
- Sarver, D.M.; Ackerman, M.B. Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 116–127. [Google Scholar] [CrossRef]
- Van der Geld, P.; Oosterveld, P.; Kuijpers-Jagtman, A.M. Age-related changes of the dental aesthetic zone at rest and during spontaneous smiling and speech. Eur. J. Orthod. 2008, 30, 366–373. [Google Scholar] [CrossRef]
- Singh, B.; Ahluwalia, R.; Verma, D.; Grewal, S.B.; Goel, R.; Kumar, P.S. Perioral age-related changes in smile dynamics along the vertical plane: A videographic crosssectional study. Angle Orthod. 2013, 83, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Correia, L.N.; Reis, S.A.; Conti, A.C.; Capelozza Filho, L.; Almeida-Pedrin, R.R. Age-related changes in the Brazilian woman’s smile. Braz. Oral Res. 2016, 30, e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chetan, P.; Tandon, P.; Singh, G.K.; Nagar, A.; Prasad, V.; Chugh, V.K. Dynamics of a smile in different age groups. Angle Orthod. 2013, 83, 90–96. [Google Scholar] [CrossRef]
- Drummond, S.; Capelli, J. Incisor display during speech and smile: Age and gender correlations. Angle Orthod. 2017, 86, 631–637. [Google Scholar] [CrossRef]
- Filho, P.F.M.; Barros, C.H.O.; Noronha, J.A.A.; Júnior, P.C.M.; Cardoso, R. Avaliação crítica do sorriso. Int. J. Dent. 2006, 1, 14–19. [Google Scholar]
- Nold, S.L.; Horvath, S.D.; Stampf, S.; Blatz, M.B. Analysis of select facial and dental esthetic parameters. Int. J. Periodontics Restor. Dent. 2014, 34, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Tjan, A.; Miller, G.; The, J.G. Some esthetic factors in a smile. J. Prosthet. Dent. 1984, 51, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Bini, V. Aesthetic Digital Smile Design: Software-aided aesthetic dentistry—Part I. CAD/CAM Int. Mag. Digit. Dent. 2014, 2, 12–17. [Google Scholar]
- Snow, S.R. Application of the golden percentage in smile design and esthetic treatment success. Contemp. Esthet. 2006, 10, 30–37. [Google Scholar]
- Dindaroğlu, F.; Doğan, S.; Ertan Erdinç, A. Smile esthetics: Age related changes, and objective differences between social and spontaneous smiles. J. Clin. Pediatr. Dent. 2011, 36, 99–106. [Google Scholar] [CrossRef]
- Jain, A.R. Coincidence of facial midline with dental midline in Chennai population. Drug Invent. Today 2018, 10, 99–106. [Google Scholar]
- Mavani, S.; Ramesh, T.R.; Patel, N.; Patel, V. Evaluation of coincidence of facial midline to dental midline and maxillary midline to mandibular midline in undergraduate students. Int. J. Adv. Res. 2017, 5, 2364–2369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.F.; Qamar, K.; Naeem, S. Coincidence of facial midline with dental midline. Pak. Oral Dent. J. 2014, 34, 555–557. [Google Scholar]
- Ahmad, I. Anterior dental aesthetics: Dentofacial perspective. Br. Dent. J. 2005, 199, 195–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J. The role of cosmetic dentistry in restoring a youthful appearance. J. Am. Dent. Assoc. 1999, 130, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.-Z.; Hu, W.-J.; Zhang, Y.-L.; Chung, K.-H. Analysis of dynamic smile and upper lip curvature in young Chinese. Int. J. Oral Sci. 2013, 5, 49–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, J.K.; Jin, T.H.; Cho, H.W.; Oh, S.C. The esthetics of smile of some recent studies. Int. J. Prosthodont. 1999, 12, 9–19. [Google Scholar]
- Hinderer, U.T. Aging of the upper lip: A new treatment technique. Aesthetic Plast. Surg. 1995, 19, 519–526. [Google Scholar] [CrossRef]
- Bugiga, F.B.; Colpo, F.L.; Anzolin, D.; Kreve, S. Restabelecimento da dimensão vertical em paciente com desgastes dentais severos-relato de caso clínico. J. Oral Investig. 2016, 5, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Sabri, R. The eight components of a balanced smile. J. Clin. Orthod. 2005, 39, 155–167. [Google Scholar]
- Peck, S.; Peck, L.; Kataja, M. The gingival smile line. Angle Orthod. 1992, 62, 91–100. [Google Scholar]
- Miron, H.; Calderon, S.; Allon, D. Upper lip changes and gingival exposure on smiling: Vertical dimension analysis. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Sarver, D.M. The importance of incisor positioning in the esthetic smile: The smile arc. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 98–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frush, J.O.; Fisher, R.D. The dysesthetic interpretation of the dentogenic concept. J. Prosthet. Dent. 1958, 8, 558–581. [Google Scholar] [CrossRef]
- Desai, S.; Upadhyay, M.; Nanda, R. Dynamic smile analysis: Changes with age. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 310.e1–310.e10. [Google Scholar] [CrossRef]
- Rodrigues, C.d.D.T.; Loffredo, L.d.C.M.; Candido, M.S.M.; Oliveira Júnior, O.B.d. Influência de variações das normas estéticas na atratividade do sorriso. Rev. Gaúch. Odontol. 2010, 58, 307–311. [Google Scholar]
- Carlsson, G.E.; Wagner, I.V.; Odman, P.; Ekstrand, K.; MacEntee, M.; Marinello, C.; Nanami, T.; Ow, R.K.; Sato, H.; Speer, C.; et al. An international comparative multicenter study of assessment of dental appearance using computer—Aided image manipulation. Int. J. Prosthod. 1998, 11, 246–254. [Google Scholar]
- Goldstein, R.E. Change Your Smile, 3rd ed.; Quintessence Publishing: Carol Stream, IL, USA, 1997. [Google Scholar]
- Machado, A.W. 10 commandments of smile esthetics. Dent. Press J. Orthod. 2014, 19, 136–157. [Google Scholar] [CrossRef] [Green Version]
- Al-Habahbeh, R.; Al-Shammout, R.; Algananem, M.; Al-Jabrah, O.; Al Habahbeh, N. Tooth and Gingival Display in the Anterior Region at Rest and during Smiling of Different Age Groups: A Comparative Study. J. R. Med. Serv. 2013, 20, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Paranhos, L.R.; Jóias, R.P.; Velascob, L.G.; Bérzin, F.; Júnior, E.D. Prevalence of the different maxillary central incisor shapes in individuals with natural normal occlusion. Braz. J. Oral Sci. 2010, 9, 104–107. [Google Scholar]
- Goldstein, R.E.; Niessen, L.C. Issues in esthetic dentistry for older adults. J. Esthet. Restor. Dent. 1998, 10, 235–242. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Description | Pictures (Examples) |
|---|---|---|
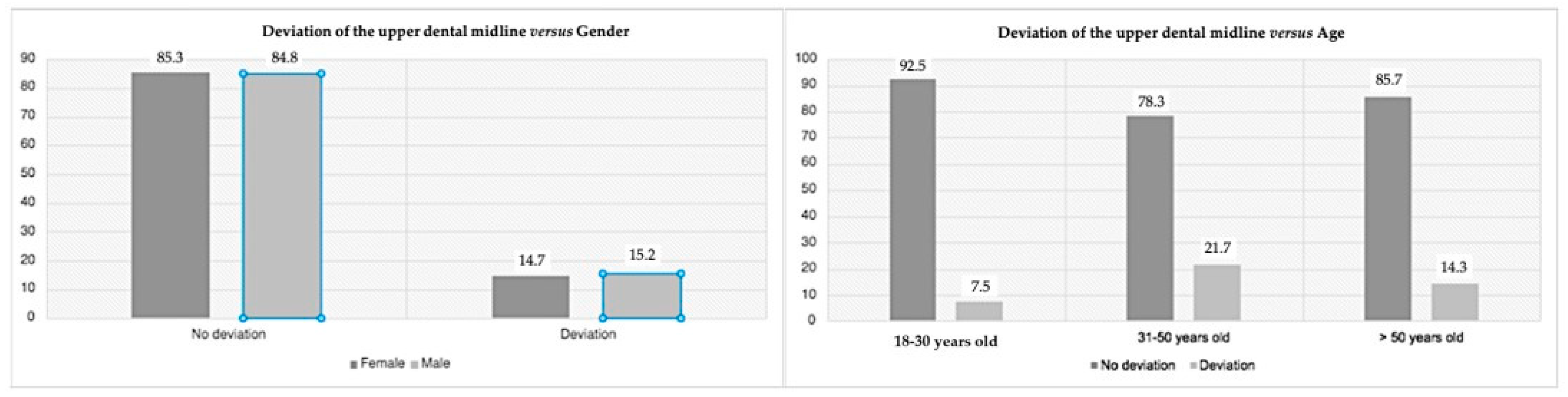
| Deviation of the upper dental midline from the facial midline | To analyze whether there is a coincidence between the upper dental midline and the facial midline in all frontal smile photographs, by tracing the facial midline through the union of anatomical points: glabella, sub nasal, and cutaneous pogonion. To analyze the coincidence of this with the upper dental midline |  A—absence of upper dental midline deviation; B—presence of upper dental midline deviation. |
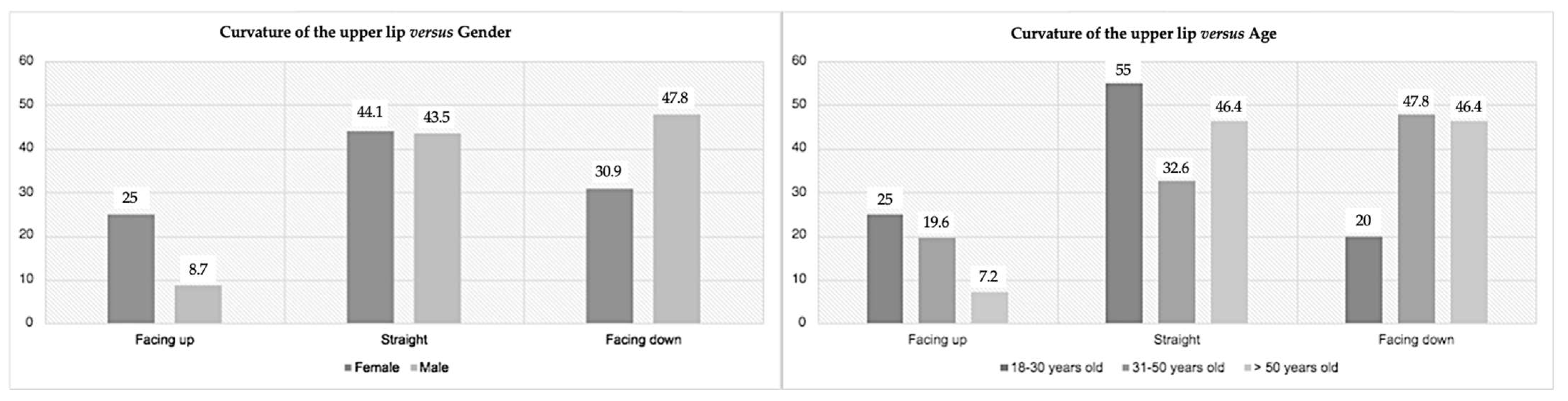
| Upper lip curvature | To analyze, in all smiles, if the curvature of the upper lip is facing up, if it is straight, or if it is facing down, by marking three points: one in the right commissure, one in the left commissure, and another in the central area of the lower edge of the upper lip. |  A—lip facing up; B—straight lip; C—lip facing down. |
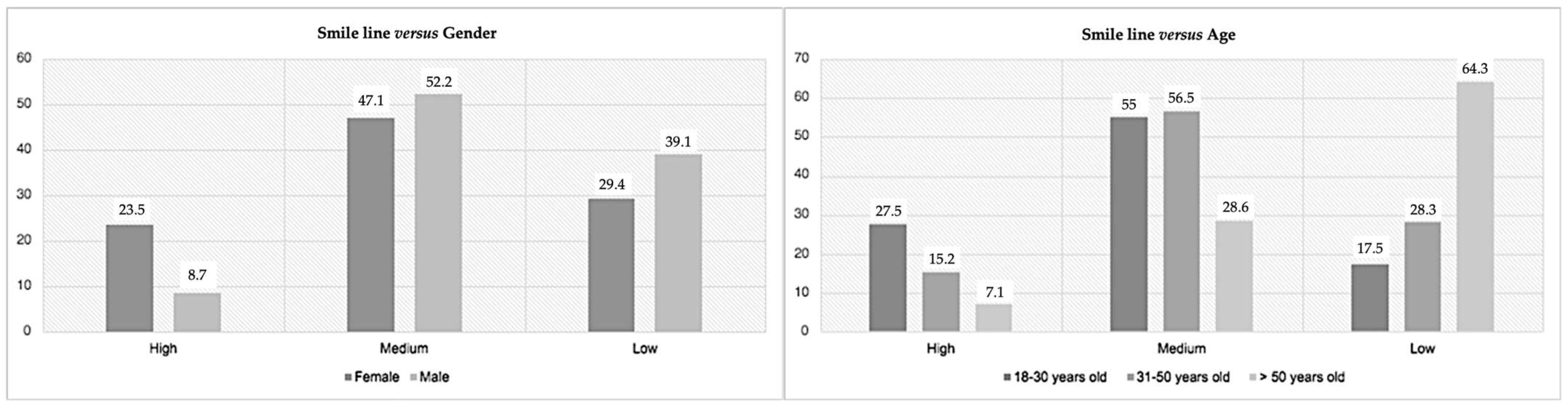
| Smile line | To classify the smile line as high, medium, or low by evaluating the exposure of the anterior teeth during the smile. The high smile line is characterized by the exposure of the entire clinical crown of the maxillary anterior teeth together with a gingival band with approximately 3 mm of gingival tissue. The medium smile line occurs when there is exposure of 75% to 100% of the clinical crown of the anterior maxillary teeth as well as the interproximal gingival papillae. The low smile line presents less than 75% of the clinical crown of the maxillary anterior teeth without gingival exposure. |  A—high smile line; B—medium smile line; C—low smile line. |
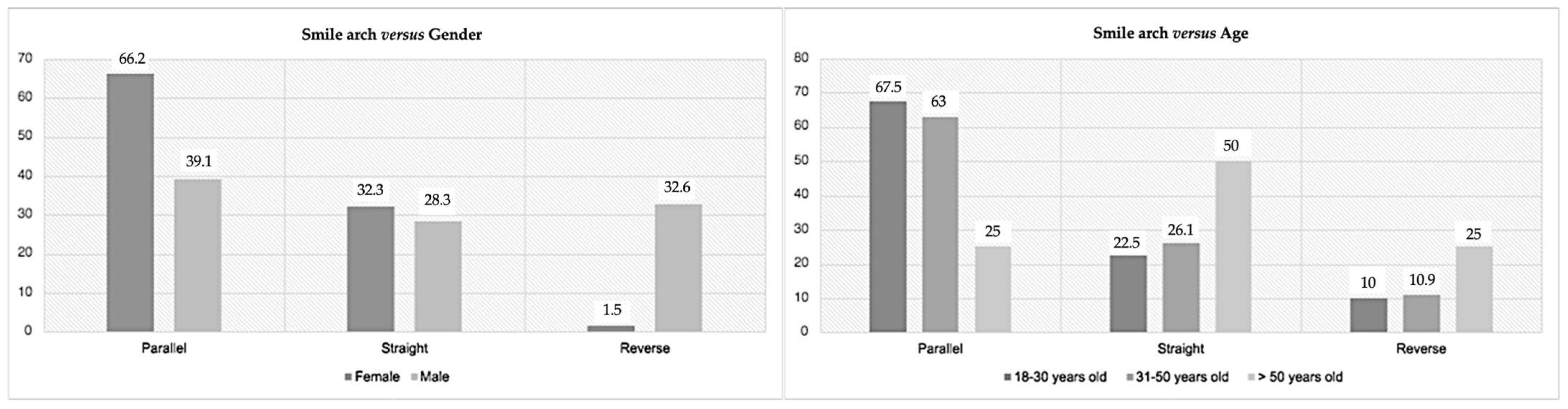
| Smile arch | To evaluate in all frontal photographs the existence of parallelism between the smile line and the upper edge of the lower lip by tracing of two curves, one formed from the union of the incisal edges of the anterior-maxillary teeth, and the other formed by the upper edge of the lower lip. After the tracing has been carried out, the classification of the relationship between the curves as parallel, straight, or reverse can be made. |  A—consonant smile arch; B—straight smile arch; C—reverse smile arch. |
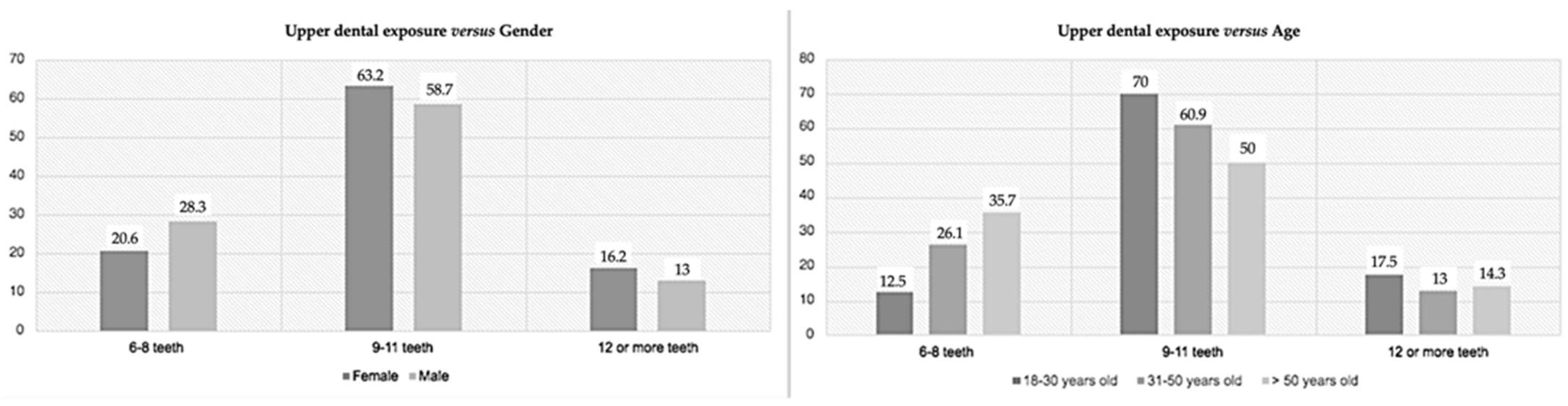
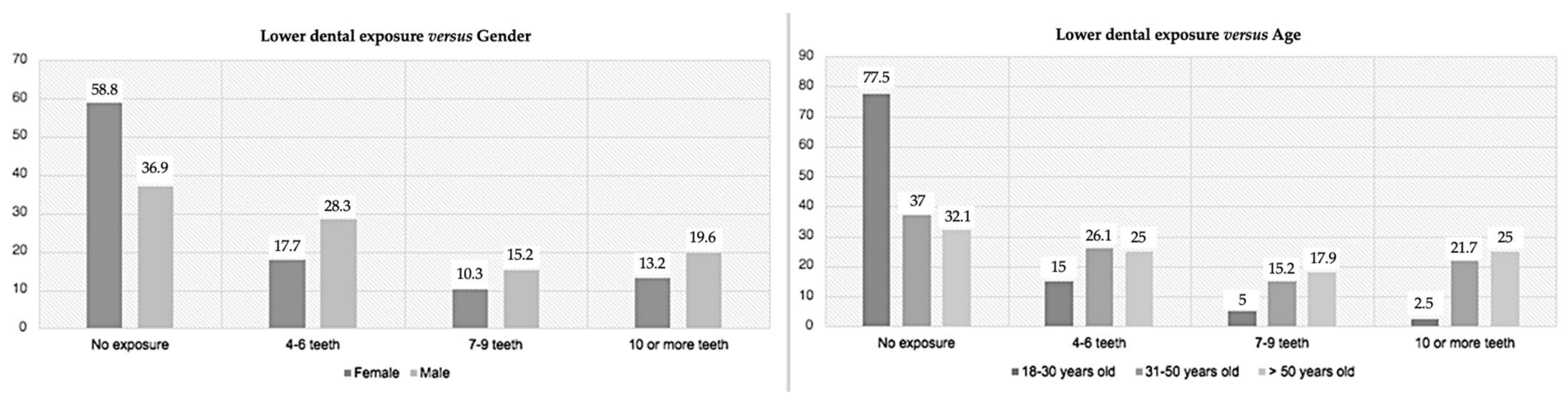
| Smile width–upper and lower teeth exposure | The smile width corresponds to the number of teeth that are exposed in a smile, and is achieved by counting the number of teeth that each participant has exposed through the frontal photographs in smile. |  A—exposure of upper teeth; B—exposure of upper and lower teeth. |
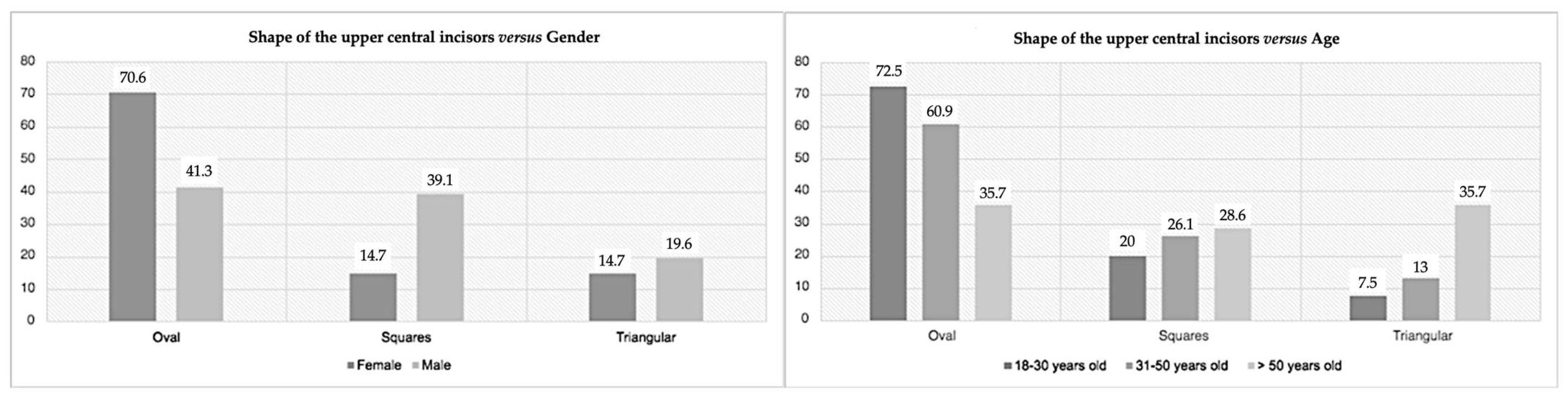
| Shape of the maxillary central incisors | To classify the maxillary central incisors by observing the intraoral photographs according to their shape. Thus, these can be square (straight and parallel external limits forming a larger cervical area than the other shapes, with the incisal edge also being large), ovoid (more curved and rounded limits either incisal or cervical, accompanied by a decrease gradual from the incisal edge and the cervical zone), or triangular (lateral limits of the labial surface diverge towards the incisal, with the cervical area being narrower). |  A—ovoid; B—square; C—triangular. |
| Gender | Age | ||||||
|---|---|---|---|---|---|---|---|
| Variables | M (n = 46) | F (n = 68) | p-Value | 18–30 y (n = 40) | 31–50 y (n = 46) | >50 y (n = 28) | p-Value |
| Deviation of the upper dental midline (with deviation) | 15.2% | 14.7% | 0.049 | 7.5% | 21.7% | 14.3% | 0.032 |
| The curvature of the upper lip (most common) | 47.8% downward curve | 44.1% straight lip | 0.113 | 55% straight-line | 47.8% downward curve | 46.4% for straight lip and downward curve | 0.001 |
| Smile line | 52.2% medium | 47.1% medium | 0.001 | 55.0% medium | 56.5% medium | 64.3% low | 0.007 |
| Smile arch | 39.1% parallel | 66.2% parallel | 0.620 | 67.5% parallel | 63.0% parallel | 50.0% straight | 0.257 |
| Smile width—upper teeth exposure | 58.7% 9–11 teeth | 63.2% 9–11 teeth | 0.153 | 70.0% 9–11 teeth | 60.9% 9–11 teeth | 60.0% 9–11 teeth | 0.002 |
| Lower teeth exposure | 36.9% did not expose | 58.8% did not expose | 0.004 | 77.5% did not expose | 37.0% did not expose | 32.1% did not expose | 0.012 |
| The shape of the upper central incisors | 41.3% oval shaped 39.1% square shaped | 70.6% oval shaped | 0.049 | 72.5% oval shape | 60.9% oval shape | 35.7% oval shape 35.7% triangular shape | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunha, J.; Fernandes, G.V.O.; Fernandes, J.C.H.; Lopes, P.C.; Rio, R. The Interference of Age and Gender on Smile Characterization Analyzed on Six Parameters: A Clinical-Photographic Pilot Study. Medicina 2023, 59, 595. https://doi.org/10.3390/medicina59030595
Cunha J, Fernandes GVO, Fernandes JCH, Lopes PC, Rio R. The Interference of Age and Gender on Smile Characterization Analyzed on Six Parameters: A Clinical-Photographic Pilot Study. Medicina. 2023; 59(3):595. https://doi.org/10.3390/medicina59030595
Chicago/Turabian StyleCunha, Joana, Gustavo Vicentis Oliveira Fernandes, Juliana Campos Hasse Fernandes, Pedro C. Lopes, and Rute Rio. 2023. "The Interference of Age and Gender on Smile Characterization Analyzed on Six Parameters: A Clinical-Photographic Pilot Study" Medicina 59, no. 3: 595. https://doi.org/10.3390/medicina59030595