
Myoepithelial Carcinoma Arising in a Salivary Duct Cyst of the Parotid Gland: Case Presentation
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
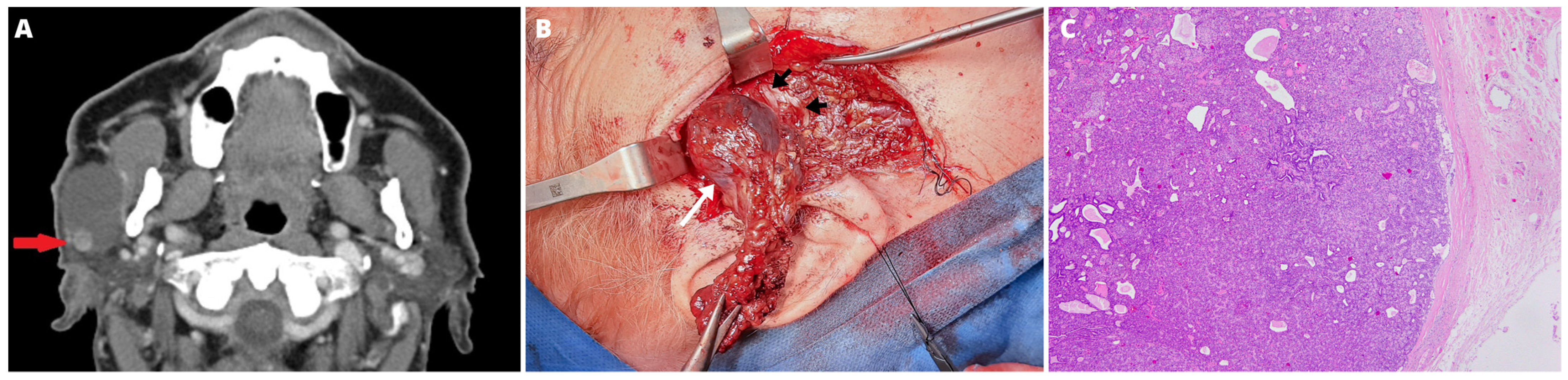
2. Case Report
2.1. Surgery
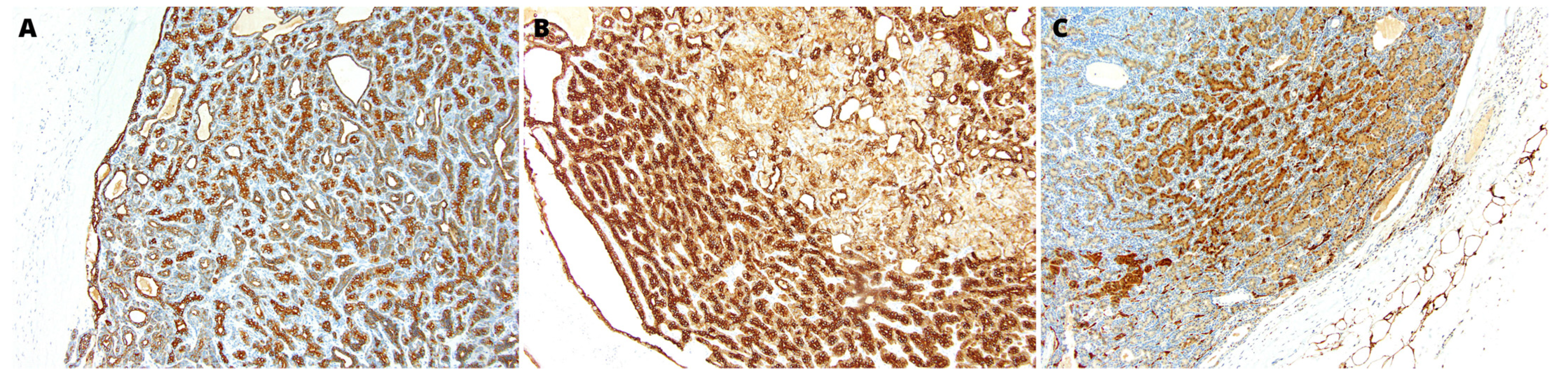
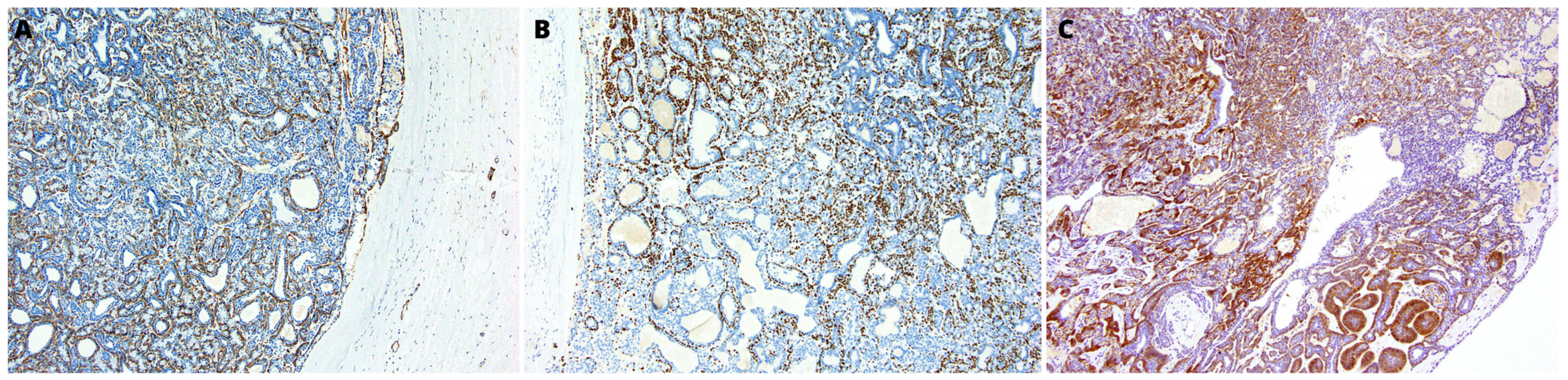
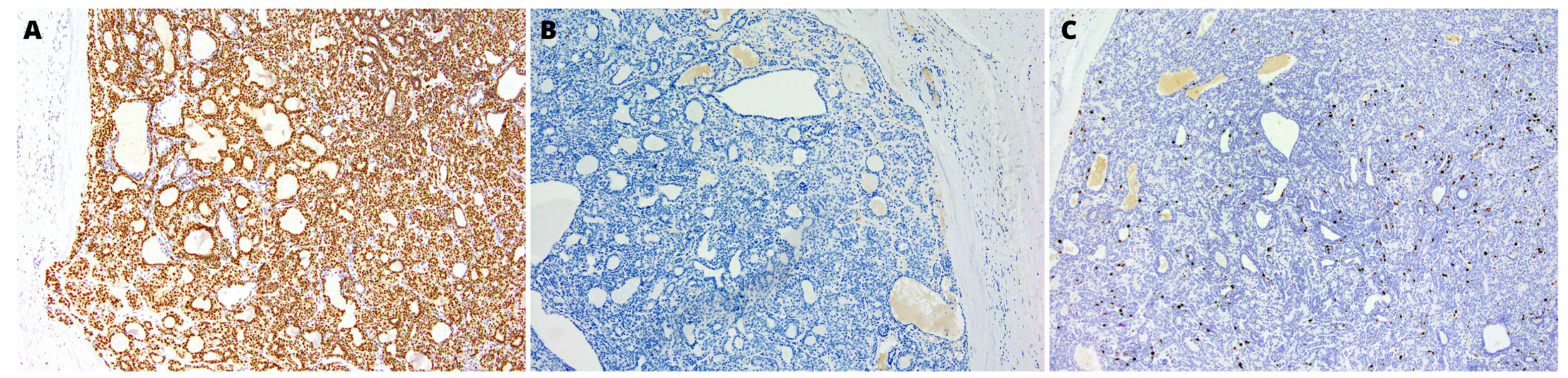
2.2. Pathology
2.3. Follow Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Classifcation of Tumours Editorial Board. Head and Neck Tumours. In WHO Classifcation of Tumours Series, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 9, Available online: https://publications.iarc.fr/ (accessed on 5 December 2022).
- Takita, H.; Takeshita, T.; Shimono, T.; Tanaka, H.; Iguchi, H.; Hashimoto, S.; Kuwae, Y.; Ohsawa, M.; Miki, Y. Cystic lesions of the parotid gland: Radiologic-pathologic correlation according to the latest World Health Organization 2017 Classification of Head and Neck Tumours. Jpn. J. Radiol. 2017, 35, 629–647. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Kawaguchi, M.; Ando, T.; Aoki, M.; Kuze, B.; Matsuo, M. CT and MR imaging findings of non-neoplastic cystic lesions of the parotid gland. Jpn. J. Radiol. 2019, 37, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Stojanov, I.J.; Malik, U.A.; Woo, S.B. Intraoral Salivary Duct Cyst: Clinical and Histopathologic Features of 177 Cases. Head Neck Pathol. 2017, 11, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, Y.; Yamamoto, H. Salivary duct cyst: Its frequency in a certain Japanese population group (Tohoku districts), with special reference to adenomatous proliferation of the epithelial lining. J. Oral. Sci. 2001, 43, 9–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minocha, V.R.; Verma, K.; Kapur, B.M. Malignant parotid cyst. Aust. New Zealand J. Surg. 1975, 45, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Schwetschke, O.; Zimmerer, A.; Bosch, F.X.; Maier, H. Salivary duct cyst of the parotid gland and adenocarcinoma. HNO 1994, 42, 441–445. [Google Scholar]
- Seifert, G. Mucoepidermoid carcinoma in a salivary duct cyst of the parotid gland. Contribution to the development of tumours in salivary gland cysts. Pathol. Res. Pract. 1996, 192, 1211–1217. [Google Scholar] [CrossRef]
- Myers, E.N.; Ferris, R.L. Salivary Gland Disorders; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Xu, B.; Mneimneh, W.; Torrence, D.E.; Higgins, K.; Klimstra, D.; Ghossein, R.; Katabi, N. Misinterpreted Myoepithelial Carcinoma of Salivary Gland: A Challenging and Potentially Significant Pitfall. Am. J. Surg. Pathol. 2019, 43, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y. Myoepithelial carcinoma of major salivary glands: Analysis of population-based clinicopathologic and prognostic features. Transl. Oncol. 2022, 20, 101410. [Google Scholar] [CrossRef]
- Giridhar, P.; Gupta, P.; Mallick, S.; Upadhyay, A.D.; Rath, G.K. Impact of adjuvant therapy on survival in patients with myoepithelial carcinoma: A systematic review and individual patient data analysis of 691 patients. Radiother. Oncol. 2019, 140, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Cormier, C.; Agarwal, S. Myoepithelial Carcinoma Ex-Pleomorphic Adenoma: A Rare Pathology Misdiagnosed as Pleomorphic Adenoma; With a Novel TERT Promoter Mutation and High PD-L1 Expression. Head Neck Pathol. 2022, 16, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Gontarz, M.; Bargiel, J.; Gąsiorowski, K.; Marecik, T.; Szczurowski, P.; Zapała, J.; Wyszyńska-Pawelec, G. Epidemiology of Primary Epithelial Salivary Gland Tumors in Southern Poland-A 26-Year, Clinicopathologic, Retrospective Analysis. J. Clin. Med. 2021, 10, 1663. [Google Scholar] [CrossRef] [PubMed]
- Savera, A.T.; Sloman, A.; Huvos, A.G.; Klimstra, D.S. Myoepithelial carcinoma of the salivary glands: A clinicopathologic study of 25 patients. Am. J. Surg. Pathol. 2000, 24, 761–774. [Google Scholar] [CrossRef] [PubMed]
- Nagao, T.; Sugano, I.; Ishida, Y.; Tajima, Y.; Matsuzaki, O.; Konno, A.; Kondo, Y.; Nagao, K. Salivary gland malignant myoepithelioma: A clinicopathologic and immunohistochemical study of ten cases. Cancer 1998, 83, 1292–1299. [Google Scholar] [CrossRef]
- Kane, S.V.; Bagwan, I.N. Myoepithelial carcinoma of the salivary glands: A clinicopathologic study of 51 cases in a tertiary cancer center. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.T.; Watermann, C.; Dreyer, T.; Ergün, S.; Karnati, S. 2021 Update on Diagnostic Markers and Translocation in Salivary Gland Tumors. Int. J. Mol. Sci. 2021, 22, 6771. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.B.; Law, M.L.; Vasquez, R.V.; Fernandez, O.C. Parotid Myoepithelial Carcinoma in a Pediatric Patient with Multiple Recurrences: Case Report. Case Rep. Oncol. 2021, 24, 989–997. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guidelines. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1437 (accessed on 14 December 2022).
- Xiao, C.C.; Baker, A.B.; White-Gilbertson, S.J.; Day, T.A. Prognostic Factors in Myoepithelial Carcinoma of the Major Salivary Glands. Otolaryngol. Head Neck Surg. 2016, 154, 1047–1053. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gontarz, M.; Orłowska-Heitzman, J.; Gąsiorowski, K.; Bargiel, J.; Marecik, T.; Szczurowski, P.; Zapała, J.; Wyszyńska-Pawelec, G. Myoepithelial Carcinoma Arising in a Salivary Duct Cyst of the Parotid Gland: Case Presentation. Medicina 2023, 59, 184. https://doi.org/10.3390/medicina59020184
Gontarz M, Orłowska-Heitzman J, Gąsiorowski K, Bargiel J, Marecik T, Szczurowski P, Zapała J, Wyszyńska-Pawelec G. Myoepithelial Carcinoma Arising in a Salivary Duct Cyst of the Parotid Gland: Case Presentation. Medicina. 2023; 59(2):184. https://doi.org/10.3390/medicina59020184
Chicago/Turabian StyleGontarz, Michał, Jolanta Orłowska-Heitzman, Krzysztof Gąsiorowski, Jakub Bargiel, Tomasz Marecik, Paweł Szczurowski, Jan Zapała, and Grażyna Wyszyńska-Pawelec. 2023. "Myoepithelial Carcinoma Arising in a Salivary Duct Cyst of the Parotid Gland: Case Presentation" Medicina 59, no. 2: 184. https://doi.org/10.3390/medicina59020184