
The Prevalence and Treatment Costs of Non-Melanoma Skin Cancer in Cluj-Napoca Maxillofacial Center
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Cost Analysis
2.2. Statistical Analysis
3. Results
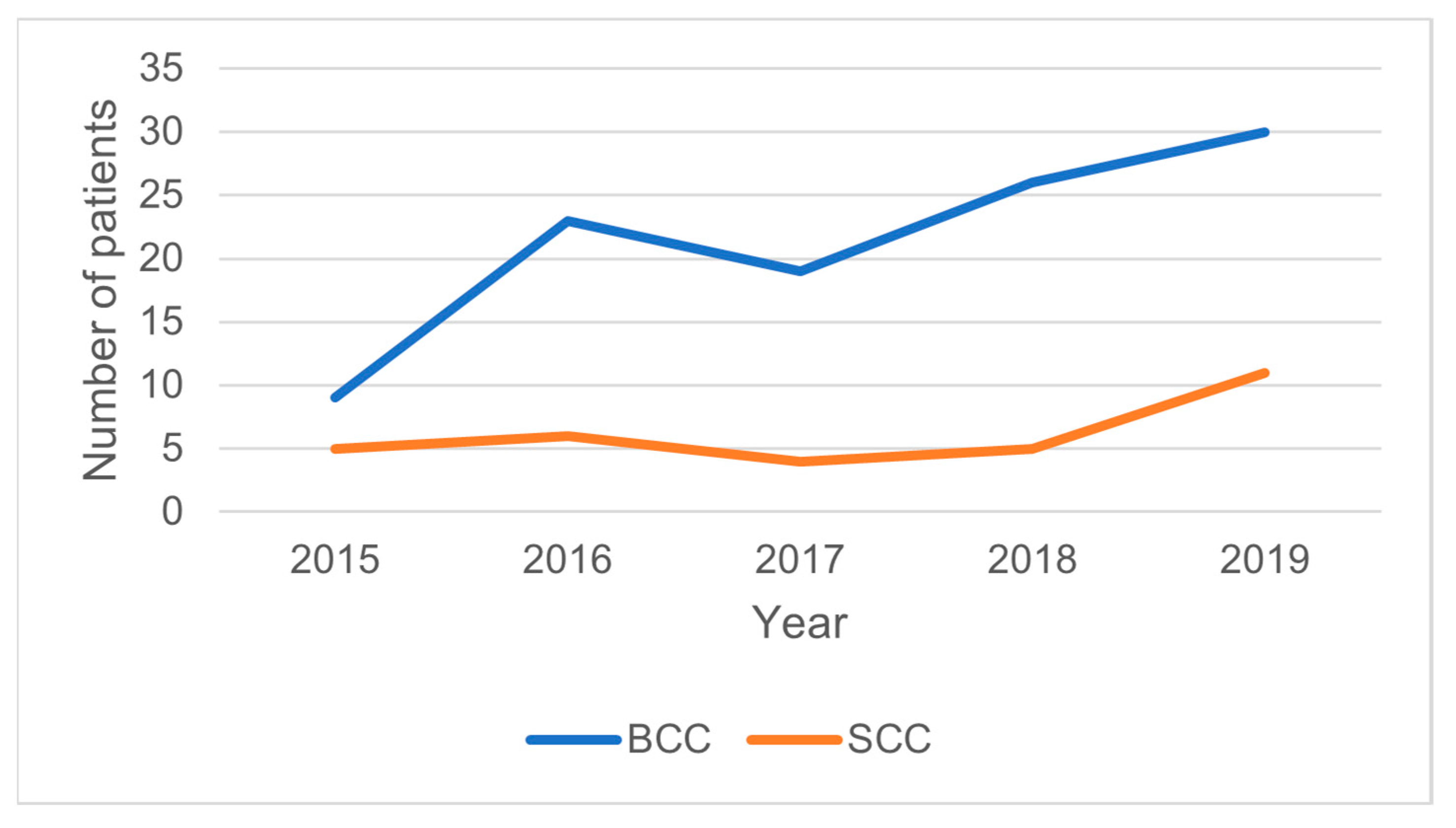
3.1. Demographical and Epidemiological Consideration of the Population
3.2. The Cost of NMSC Treatment
3.3. Cost of NMSC Treatment Related to the Demographical and Clinical Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Eisemann, N.; Waldmann, A.; Geller, A.C.; Weinstock, M.A.; Volkmer, B.; Greinert, R.; Breitbart, E.W.; Katalinic, A. Non-Melanoma Skin Cancer Incidence and Impact of Skin Cancer Screening on Incidence. J. Investig. Dermatol. 2014, 134, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Cancer.Net Editorial Board. Skin Cancer (Non-Melanoma): Statistics. Available online: https://www.cancer.net/cancer-types/skin-cancer-non-melanoma/statistics (accessed on 1 October 2022).
- Lomas, A.; Leonardi-Bee, J.; Bath-Hextall, F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br. J. Dermatol. 2012, 166, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Fijałkowska, M.; Koziej, M.; Antoszewski, B. Detailed Head Localization and Incidence of Skin Cancers. Sci. Rep. 2021, 11, 12391. [Google Scholar] [CrossRef]
- Andrese, E.; Solovăstru, L.G.; Taranu, T.; Iancu, T.S. Epidemiological and pathological aspects of skin cancer in North East of Romania. Rev. Med. Chir. Soc. Med. Nat. 2014, 118, 457–462. [Google Scholar]
- Ciążyńska, M.; Kamińska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Sławińska, M.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ułańska, M.; et al. The Incidence and Clinical Analysis of Non-Melanoma Skin Cancer. Sci. Rep. 2021, 11, 4337. [Google Scholar] [CrossRef]
- Kasumagic-Halilovic, E.; Hasic, M.; Ovcina-Kurtovic, N. A Clinical Study of Basal Cell Carcinoma 394 A Clinical Study of Basal Cell Carcinoma. Med Arch. 2019, 73, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Marzuka, S.B. Basal cell carcinoma: Pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. Yale J. Biol. Med. 2015, 88, 167–179. [Google Scholar]
- Riihilä, P.; Nissinen, L.; Knuutila, J.; Nezhad, P.R.; Viiklepp, K.; Kähäri, V.M. Complement System in Cutaneous Squamous Cell Carcinoma. Int. J. Mol. Sci. 2019, 20, 3550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubov, J.; Labbé, M.; Sioufi, K.; Morand, G.B.; Hier, M.P.; Khanna, M.; Sultanem, K.; Mlynarek, A.M. Prognostic Factors of Head and Neck Cutaneous Squamous Cell Carcinoma: A Systematic Review. J. Otolaryngol.—Head Neck Surg. 2021, 50, 54. [Google Scholar] [CrossRef]
- Steding-Jessen, M.; Birch-Johansen, F.; Jensen, A.; Schüz, J.; Kjær, S.K.; Dalton, S.O. Socioeconomic Status and Non-Melanoma Skin Cancer: A Nationwide Cohort Study of Incidence and Survival in Denmark. Cancer Epidemiol. 2010, 34, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, A.B.; Robin Yabroff, K.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the Cost of Cancer Care in the United States: 2010–2020. JNCI J. Natl. Cancer Inst. 2011, 103, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newlands, C.; Currie, R.; Memon, A.; Whitaker, S.; Woolford, T. Non-Melanoma Skin Cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S125. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.T.; Kempton, S.J.; Rao, V.K. The Economics of Skin Cancer: An Analysis of Medicare Payment Data. Plast. Reconstr. Surg.—Glob. Open 2016, 4, 9. [Google Scholar] [CrossRef]
- Duarte, A.F.; Sousa-Pinto, B.; Freitas, A.; Delgado, L.; Costa-Pereira, A.; Correia, O. Skin Cancer Healthcare Impact: A Nation-Wide Assessment of an Administrative Database. Cancer Epidemiol. 2018, 56, 154–160. [Google Scholar] [CrossRef]
- Ruiz, E.S.; Morgan, F.C.; Zigler, C.M.; Besaw, R.J.; Schmults, C.D. Analysis of National Skin Cancer Expenditures in the United States Medicare Population, 2013. J. Am. Acad. Dermatol. 2019, 80, 275–278. [Google Scholar] [CrossRef] [Green Version]
- Guy, G.P.; Machlin, S.R.; Ekwueme, D.U.; Yabroff, K.R. Prevalence and Costs of Skin Cancer Treatment in the U.S., 2002−2006 and 2007–2011. Am. J. Prev. Med. 2015, 48, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Tran, D.A.; Coronado, A.C.; Sarker, S.; Alvi, R. Estimating the Health Care Costs of Non-Melanoma Skin Cancer in Saskatchewan Using Physician Billing Data. Curr. Oncol. 2019, 26, 114. [Google Scholar] [CrossRef] [Green Version]
- Massa, S.T.; Osazuwa-Peters, N.; Adjei Boakye, E.; Walker, R.J.; Ward, G.M. Comparison of the Financial Burden of Survivors of Head and Neck Cancer with Other Cancer Survivors. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 239–249. [Google Scholar] [CrossRef]
- Doran, C.M.; Ling, R.; Byrnes, J.; Crane, M.; Searles, A.; Perez, D.; Shakeshaft, A. Estimating the Economic Costs of Skin Cancer in New South Wales, Australia. BMC Public Health 2015, 15, 952. [Google Scholar] [CrossRef] [Green Version]
- Zanoni, D.K.; Patel, S.G.; Shah, J.P. Changes in the 8th Edition of the American Joint Committee on Cancer (AJCC) Staging of Head and Neck Cancer: Rationale and Implications. Curr. Oncol. Rep. 2019, 21, 52. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Schilsky, R.L.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual; American Joint Committee on Cancer (AJCC): Chicago, IL, USA, 2017; ISBN 9783319406176. [Google Scholar]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A Review of ASA Physical Status—Historical Perspectives and Modern Developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.; Crawford, K.; Faraji, F.; Ramsey, C.; Kemp, A.; Califano, J.A. An Analysis of 1-Year Charges for Head and Neck Cancer: Targets for Value-Based Interventions. Otolaryngol.—Head Neck Surg. 2020, 163, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, A.; Tompa, E.; Spencer, J.; Kalcevich, C.; Peters, C.E.; Kim, J.; Song, C.; Mortazavi, S.B.; Demers, P.A. The Economic Burden of Occupational Non-Melanoma Skin Cancer Due to Solar Radiation. J. Occup. Environ. Hyg. 2018, 15, 481–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangka, F.K.; Trogdon, J.G.; Richardson, L.C.; Howard, D.; Sabatino, S.A.; Finkelstein, E.A. Cancer Treatment Cost in the United States. Cancer 2010, 116, 3477–3484. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, M.E.; Santesteban, R.; Larumbe, A. Oncologic Surgery of the Eyelid and Orbital Region. Actas Dermo-Sifiliogr. (Engl. Ed.) 2015, 106, 365–375. [Google Scholar] [CrossRef]
- Yüce, S.; Demir, Z.; Selçuk, C.T.; Çelebioğlu, S. Reconstruction of Periorbital Region Defects: A Retrospective Study. Ann. Maxillofac. Surg. 2014, 4, 45. [Google Scholar] [CrossRef] [Green Version]
- Dacosta Byfield, S.; Chen, D.; Yim, Y.M.; Reyes, C. Age Distribution of Patients with Advanced Non-Melanoma Skin Cancer in the United States. Arch. Dermatol. Res. 2013, 305, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Whitney, R.L.; Bell, J.F.; Tancredi, D.J.; Romano, P.S.; Bold, R.J.; Joseph, J.G. Hospitalization Rates and Predictors of Rehospitalization among Individuals with Advanced Cancer in the Year After Diagnosis. J. Clin. Oncol. 2017, 35, 3610. [Google Scholar] [CrossRef] [Green Version]
- Brambullo, T.; Azzena, G.P.; Toninello, P.; Masciopinto, G.; De Lazzari, A.; Biffoli, B.; Vindigni, V.; Bassetto, F. Current Surgical Therapy of Locally Advanced CSCC: From Patient Selection to Microsurgical Tissue Transplant. Review. Front. Oncol. 2021, 11, 5185. [Google Scholar] [CrossRef]
- Egeler, S.A.; Huang, A.; Johnson, A.R.; Ibrahim, A.; Bucknor, A.; Peymani, A.; Mureau, M.A.M.; Lin, S.J. Regional Incidence of and Reconstructive Management Patterns in Melanoma and Nonmelanoma Skin Cancer of the Head and Neck: A 3-Year Analysis in the Inpatient Setting. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Asai, Y.; Nguyen, P.; Hanna, T.P. Impact of the COVID-19 Pandemic on Skin Cancer Diagnosis: A Population-Based Study. PLoS ONE 2021, 16, e0248492. [Google Scholar] [CrossRef] [PubMed]
- Jambusaria-Pahlajani, A.; Kanetsky, P.A.; Karia, P.S.; Hwang, W.T.; Gelfand, J.M.; Whalen, F.M.; Elenitsas, R.; Xu, X.; Schmults, C.D. Evaluation of AJCC Tumor Staging for Cutaneous Squamous Cell Carcinoma and a Proposed Alternative Tumor Staging System. JAMA Dermatol. 2013, 149, 402–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Malignant Skin Cancer Episodes | NMSC Treatment Cost Per Episode | |||||
|---|---|---|---|---|---|---|
| NMSC n = episodes (n%) | BCC n = episodes (n%) | SCC n = episodes (n%) | p value (BCC vs. SCC among subsets) * | Mean ± standard deviation (Euro) ** | p Value (costs comparison among subsets) *** | |
| Age decade distribution | ||||||
| 20–30 | 2 (1.31%) | 1 (0.83%) | 1 (3.13%) | 0.31 | 110 ± 9 | 0.04 |
| 30–40 | 5 (3.27%) | 4 (3.33%) | 1 (3.13%) | 177 ± 67 | ||
| 40–50 | 18 (11.76%) | 15 (12.5%) | 3 (9.38%) | 205 ± 90 | ||
| 50–60 | 5 (3.27%) | 4 (3.33%) | 1 (3.13%) | 226 ± 42 | ||
| 60–70 | 37 (24.18%) | 33 (27.5%) | 4 (12.5%) | 248 ± 150 | ||
| 70–80 | 54 (35.29%) | 41 (34.17%) | 13 (40.63%) | 281 ± 224 | ||
| 80–90 | 30 (19.61%) | 22 (18.33%) | 8 (25%) | 352 ± 210 | ||
| 90–100 | 1 (0.65%) | - | 1 (3.13%) | - | ||
| Sex | ||||||
| Female | 64 (42.1%) | 49 (40.83%) | 15 (46.85%) | 0.53 | 323 ± 271 | 0.17 |
| Male | 88 (57.9%) | 71 (59.17%) | 17 (53.13%) | 271 ± 245 | ||
| Place of living | ||||||
| Rural | 60 (39.47%) | 45 (37.5%) | 15 (46.88%) | 0.33 | 331 ± 327 | 0.44 |
| Urban | 92 (60.53%) | 75 (62.5%) | 17 (53.13%) | 266 ± 190 | ||
| Educational formation | ||||||
| Elementary school | 5 (3.76%) | 2 (1.87%) | 3 (9.68%) | 0.13 | 331 ± 329 | 0.16 |
| Medium school | 24 (18.05%) | 21 (19.63%) | 3 (9.68%) | 242 ± 159 | ||
| Technical school | 9 (6.77%) | 8 (7.48%) | 1 (3.23%) | 523 ± 622 | ||
| High School | 19 (14.29%) | 16 (14.95%) | 3 (9.68%) | 258 ± 293 | ||
| College | 15 (11.28%) | 11 (10.28%) | 4 (12.9%) | 214 ± 163 | ||
| Economic status | ||||||
| Low income | 42 (27.45%) | 23 (19.17%) | 10 (31.25%) | 0.66 | 300 ± 331 | <0.01 |
| Medium income | 26 (16.99%) | 47 (39.16%) | 3 (9.38%) | 283 ± 282 | ||
| Upper income | 4 (2.61%) | 3 (2.5%) | 1 (3.13%) | 103 ± 4 | ||
| Immunosuppression | ||||||
| Yes | 6 (3.95%) | 3 (2.5%) | 3 (9.38%) | 0.07 | 419 ± 212 | 0.04 |
| No | 146(96.05%) | 117 (97.5%) | 29 (90.63%) | 277 ± 213 | ||
| ASA risk classification | ||||||
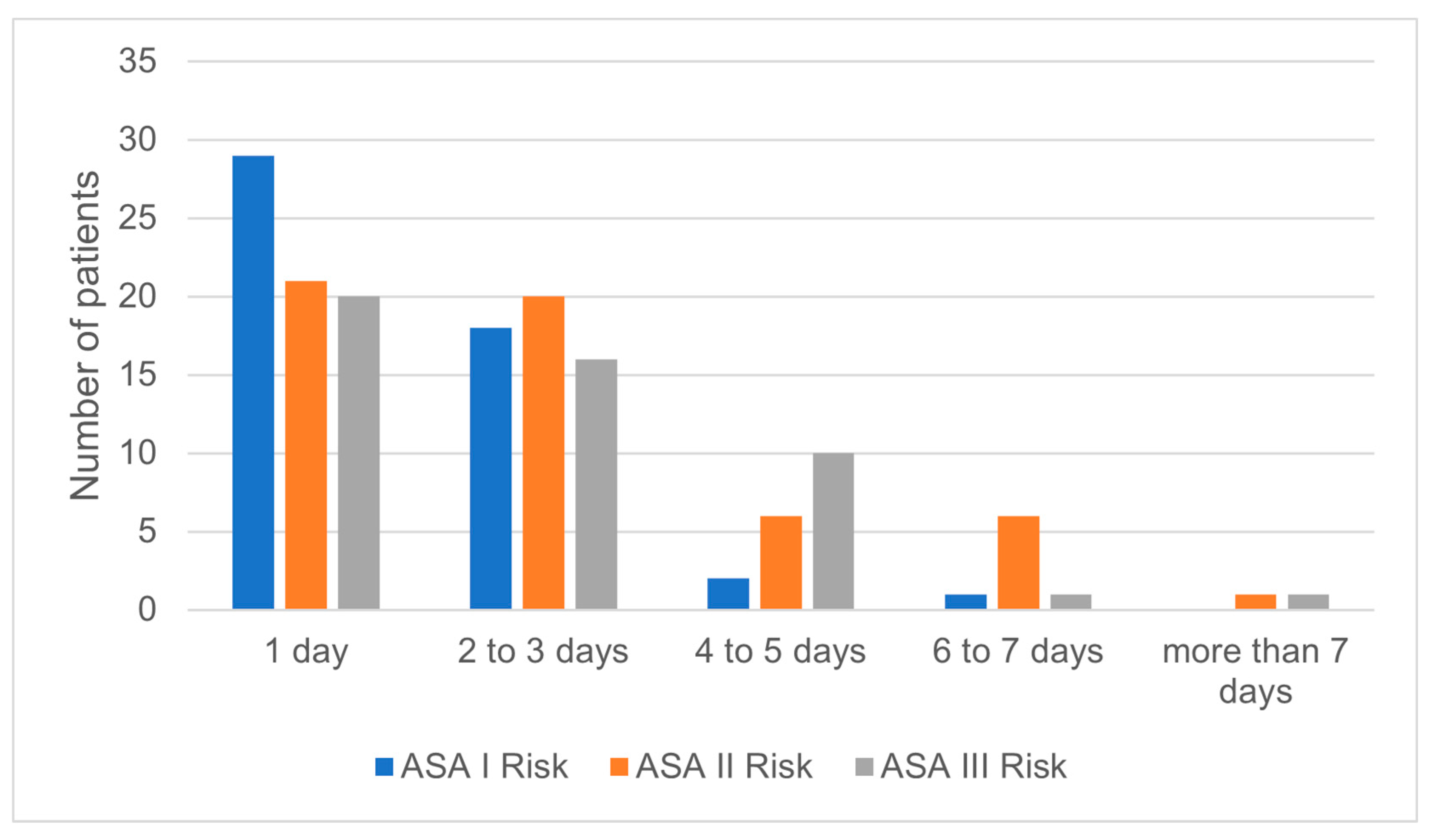
| I | 50 (32.89%) | 40 (33.33%) | 10 (31.25%) | 0.91 | 242 ± 219 | 0.03 |
| II | 54 (35.53%) | 42 (35%) | 12 (37.5%) | 333 ± 106 | ||
| III | 48 (31.58%) | 38 (31.67%) | 10 (31.25%) | 339 ± 142 | ||
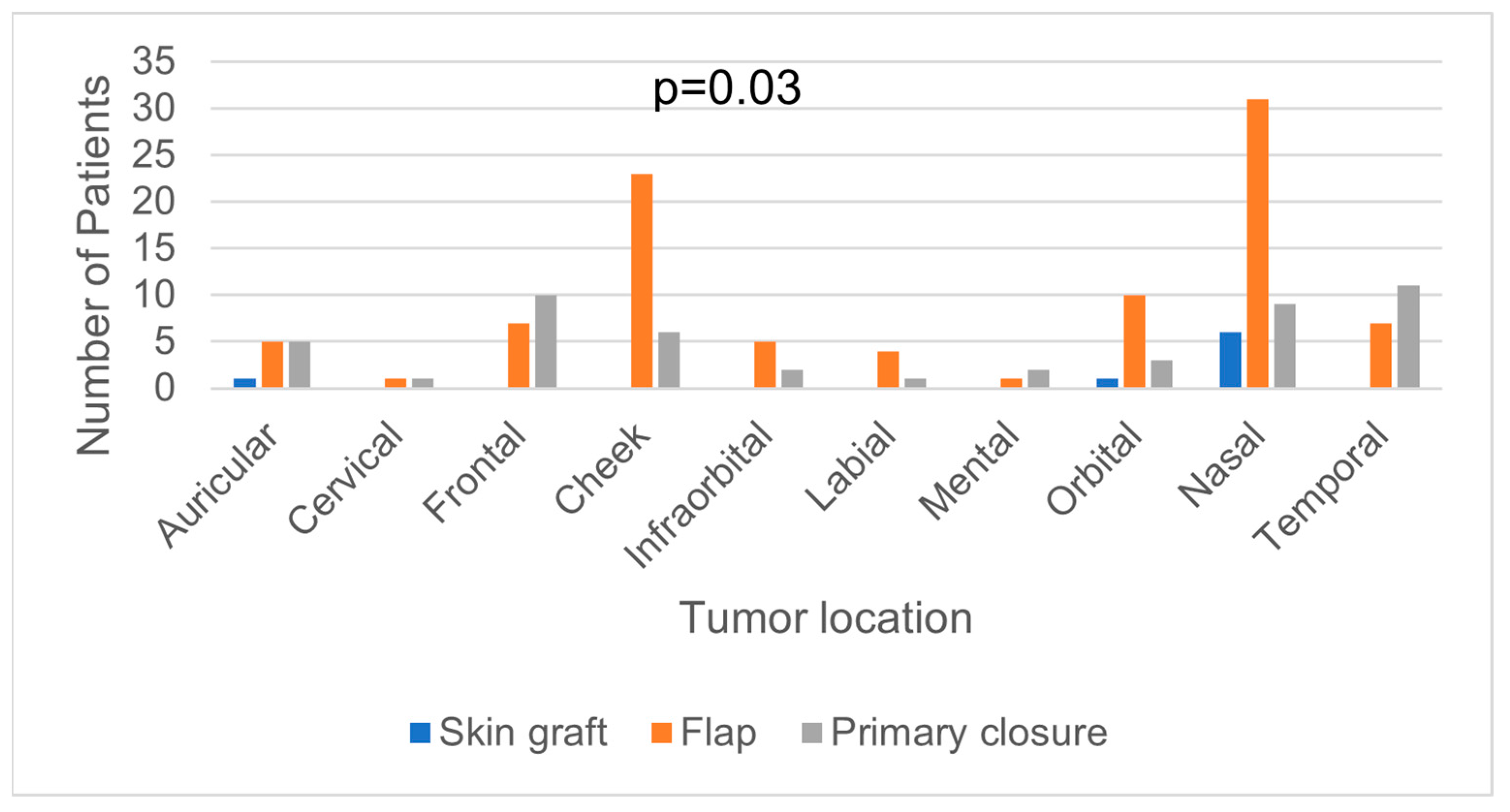
| Tumor’s location (head and neck regions) | ||||||
| Auricular | 11 (7.24%) | 6 (5%) | 5 (15.63%) | 0.14 | 214 ± 113 | 0.14 |
| Cervical | 2 (1.32%) | 1 (0.83%) | 1 (3.13%) | 215 ± 49 | ||
| Frontal | 17 (11.18%) | 11 (9.17%) | 6 (18.75%) | 332 ± 303 | ||
| Cheek | 29 (19.08%) | 24 (20%) | 5 (15.63%) | 329 ± 225 | ||
| Infraorbital | 7 (4.61%) | 6 (5%) | 1 (3.13%) | 203 ± 61 | ||
| Labial | 5 (3.29%) | 4 (3.33%) | 1 (3.13%) | 376 ± 225 | ||
| Mental | 3 (1.97%) | 3 (2.5%) | - | 143 ± 33 | ||
| Orbital | 14 (9.21%) | 13 (10.83%) | 1 (3.13%) | 421 ± 340 | ||
| Nasal | 46 (30.26%) | 40 (33.33%) | 6 (18.75%) | 256 ± 154 | ||
| Temporal | 18 (11.84%) | 12 (10%) | 6 (18.75%) | 301 ± 456 | ||
| Stage of the disease | ||||||
| I | 97 (63.82%) | 83 (69.17%) | 14 (43.75%) | 0.002 | 253 ± 151 | 0.65 |
| II | 31 (20.39%) | 25 (20.83%) | 6 (18.75%) | 307 ± 184 | ||
| III | 21 (13.82%) | 11 (9.17%) | 10 (31.25%) | 371 ± 446 | ||
| IV | 3 (1.97%) | 1 (0.83%) | 2 (6.25%) | 974 ± 715 | ||
| Type of reconstruction | ||||||
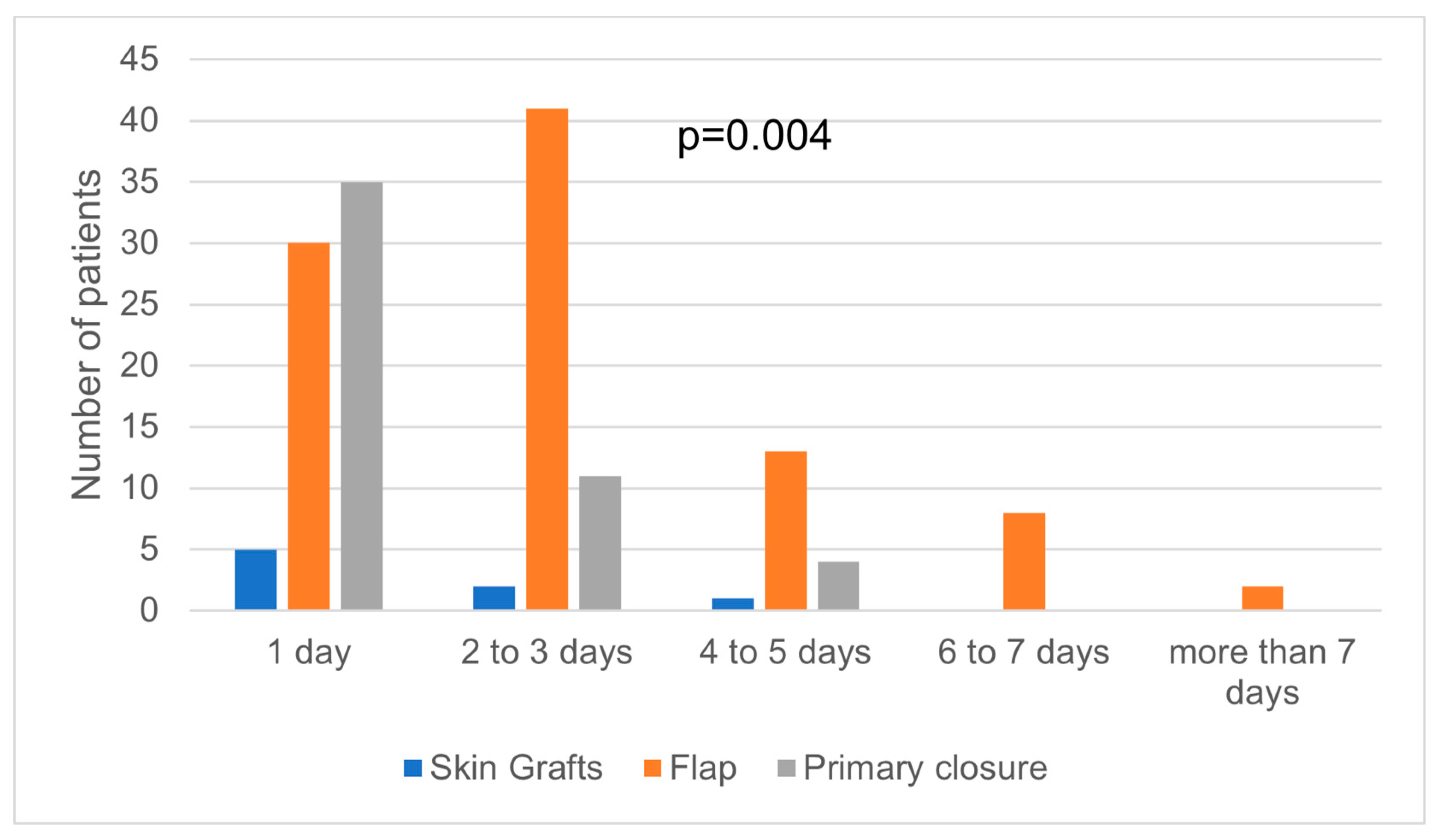
| Primary closure | 50 (32.68%) | 37 (30.83%) | 13 (40.63%) | 0.52 | 198 ± 116 | <0.01 |
| Skin graft | 8 (5.23%) | 6 (5%) | 2 (6.25%) | 220 ± 134 | ||
| Local flap | 94 (61.44%) | 77 (64.17%) | 17 (53.13%) | 352 ± 315 | ||
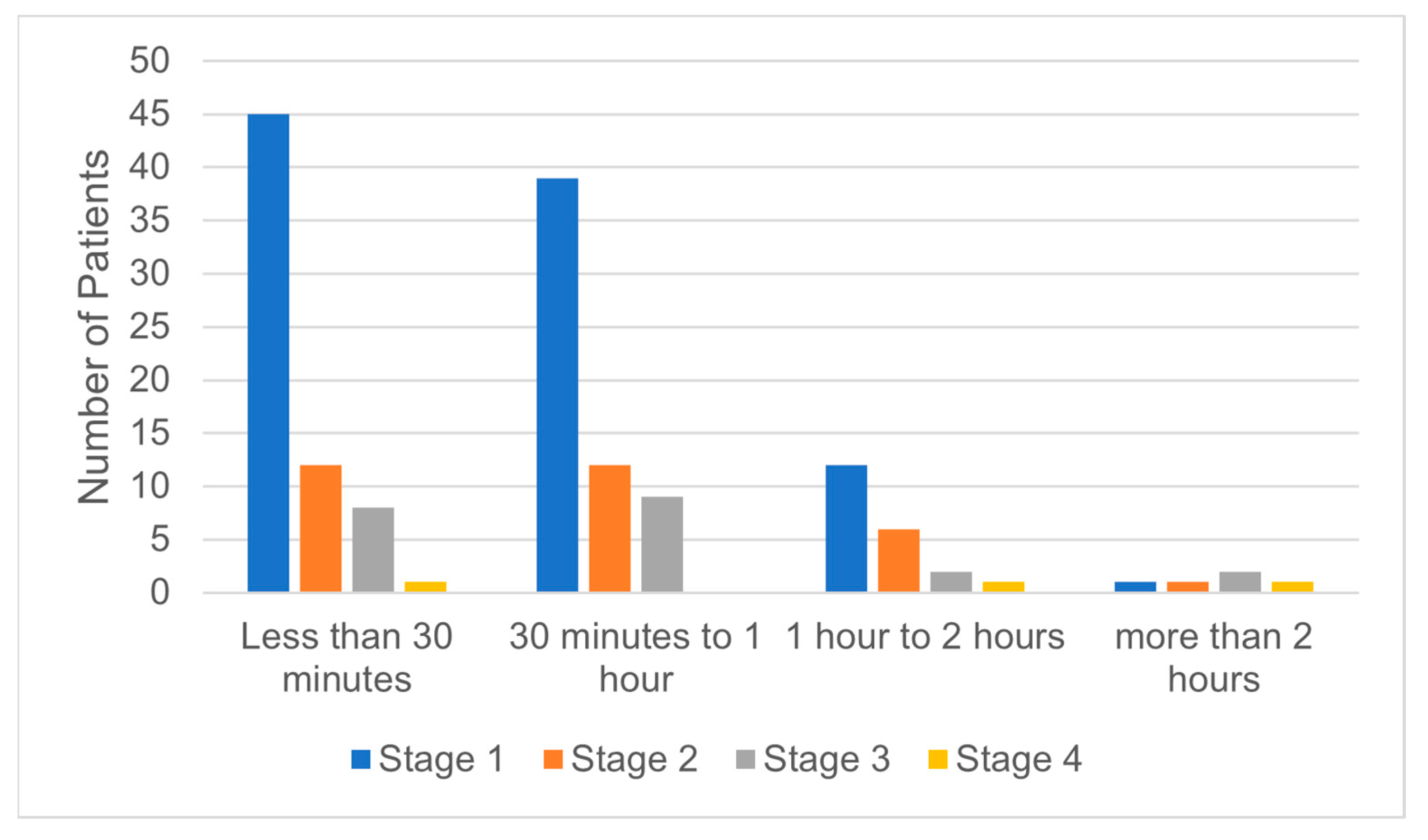
| Time needed for surgical procedure | ||||||
| <1 h | 66 (43.42%) | 53 (44.16%) | 13 (40.62%) | - | 257 ± 177 | <0.01 |
| 1–2 h | 66 (43.42%) | 52 (43.33%) | 14 (43.75%) | 340 ± 155 | ||
| >2 h | 20 (13.16%) | 15 (12.5%) | 5 (15.62%) | 647 ± 581 | ||
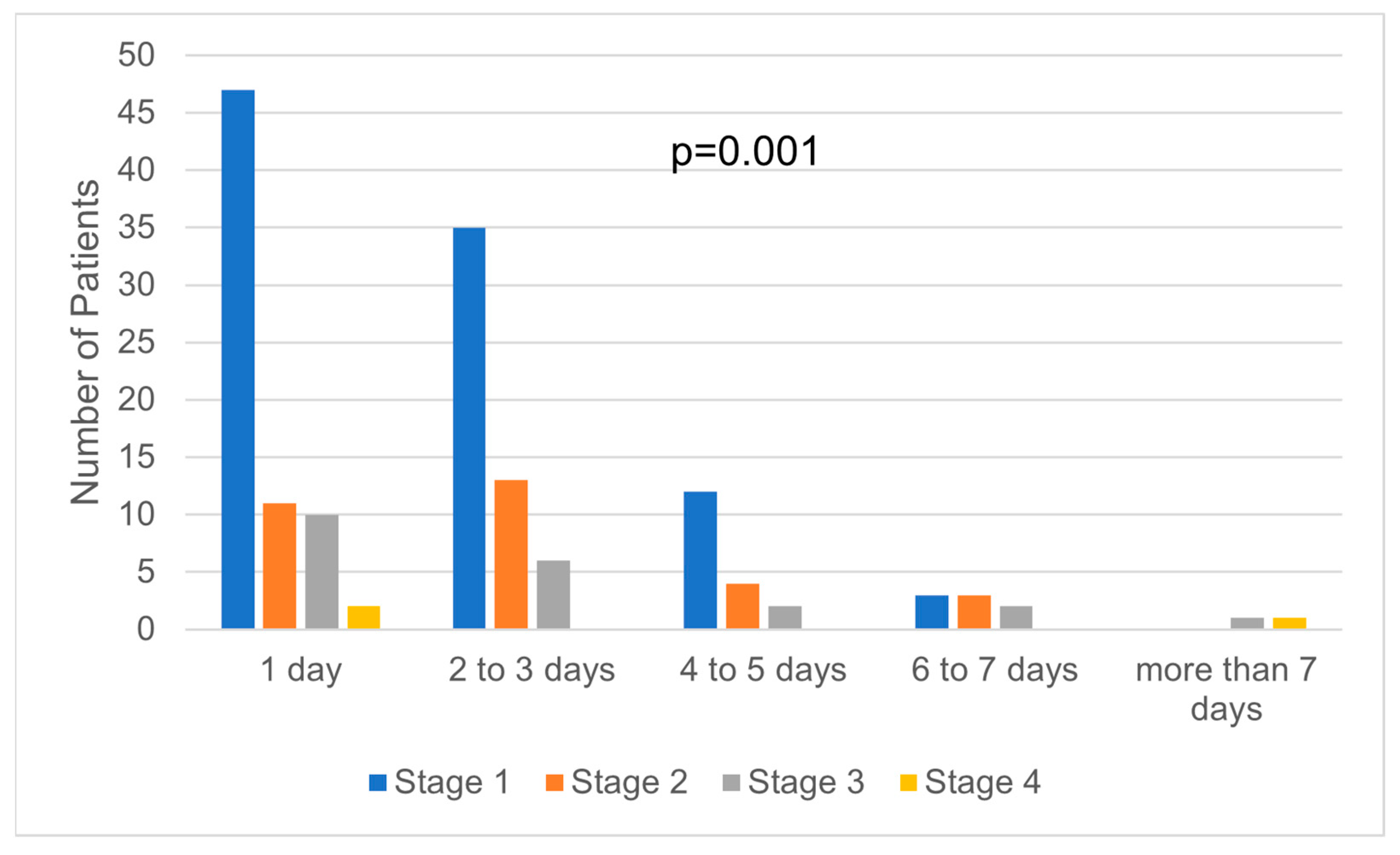
| Days of hospitalization | ||||||
| 1 | 69 (45.39%) | 56 (46.66%) | 13 (40.62%) | 0.53 | 139 ± 31 | <0.01 |
| 2 | 36 (23,68%) | 31 (25.83%) | 5 (15.62%) | 281 ± 190 | ||
| 3 | 18 (11,84%) | 13 (10.83) | 5 (15.62%) | 357 ± 46 | ||
| 4 | 14 (9,21%) | 9 (7,5%) | 5 (15.62%) | 475 ± 58 | ||
| 5 | 4 (2,63%) | 3 (2.5%) | 1 (3.12%) | 596 ± 29 | ||
| 6 | 5 (3,28%) | 4 (3.33%) | 1 (3.12%) | 627 ± 70 | ||
| 7> | 6 (3,94%) | 4 (3,33%) | 2 (6.25%) | 1177 ± 526 | ||
| Costs (EUR) | NMSC | BCC | SCC |
|---|---|---|---|
| Total direct costs | |||
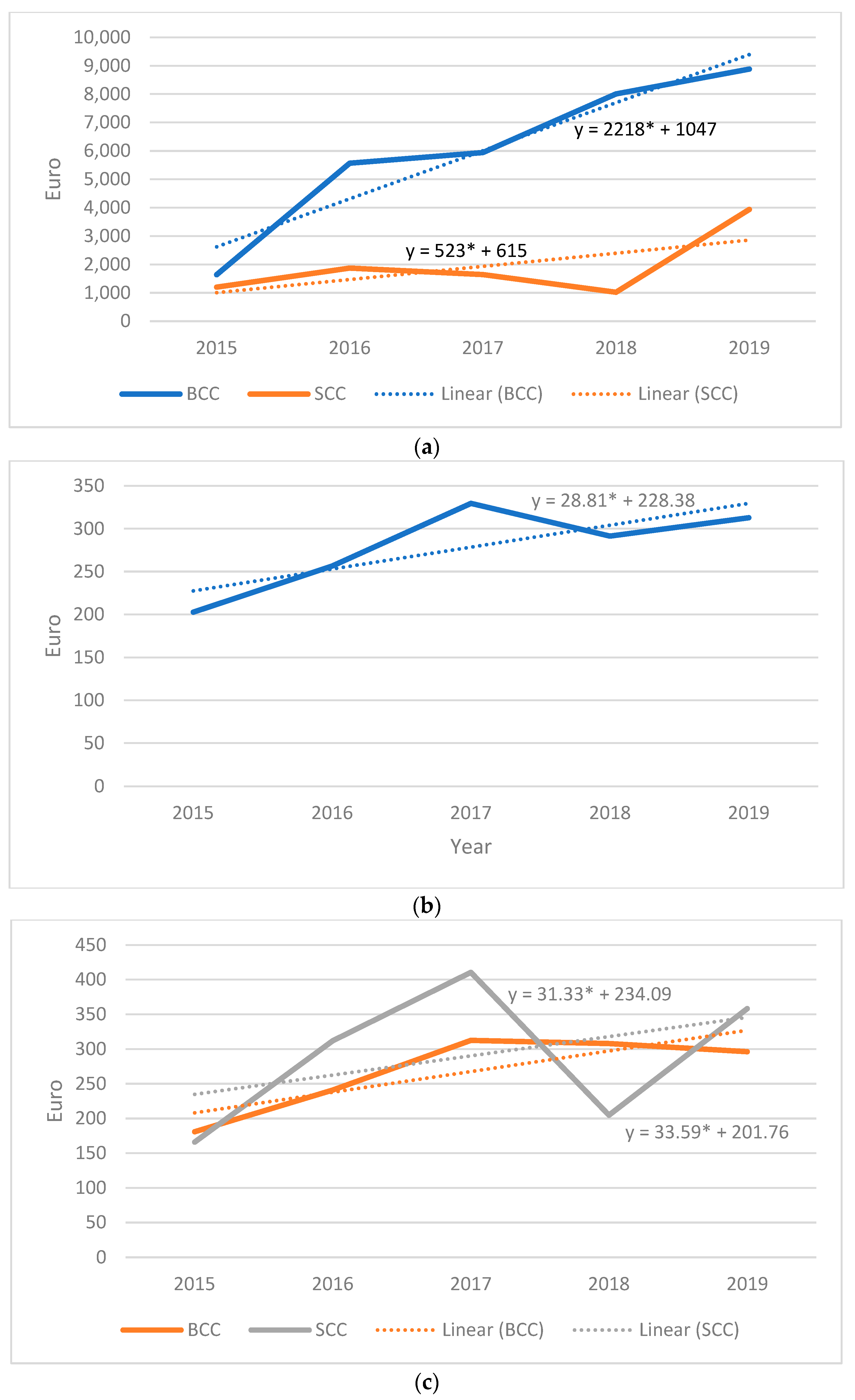
| Average cost per patient | 336 | 317 | 252 |
| Average cost per episode | 294 | 282 | 341 |
| Drug costs | |||
| Average cost per patient | 20 | 22 | 13 |
| Average cost per episode | 18 | 19 | 12 |
| Paraclinical examination costs | |||
| Average cost per patient | 42 | 38 | 49 |
| Average cost per episode | 37 | 33 | 48 |
| Supply costs | |||
| Average cost per patient | 18 | 17 | 17 |
| Average cost per episode | 15 | 15 | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faur, C.I.; Moldovan, M.A.; Văleanu, M.; Rotar, H.; Filip, L.; Roman, R.C. The Prevalence and Treatment Costs of Non-Melanoma Skin Cancer in Cluj-Napoca Maxillofacial Center. Medicina 2023, 59, 220. https://doi.org/10.3390/medicina59020220
Faur CI, Moldovan MA, Văleanu M, Rotar H, Filip L, Roman RC. The Prevalence and Treatment Costs of Non-Melanoma Skin Cancer in Cluj-Napoca Maxillofacial Center. Medicina. 2023; 59(2):220. https://doi.org/10.3390/medicina59020220
Chicago/Turabian StyleFaur, Cosmin Ioan, Mădălina Anca Moldovan, Mădălina Văleanu, Horațiu Rotar, Laura Filip, and Rareș Călin Roman. 2023. "The Prevalence and Treatment Costs of Non-Melanoma Skin Cancer in Cluj-Napoca Maxillofacial Center" Medicina 59, no. 2: 220. https://doi.org/10.3390/medicina59020220