
Clinical Characteristics and Diagnostic Prediction of Severe Fever with Thrombocytopenia Syndrome and Rickettsiosis in the Co-Endemic Wakayama Prefecture, Japan
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Study Design
2.2. Clinical Data Collection
2.3. Statistical Analyses
3. Results
3.1. Characteristics, Treatment, and Outcomes of Patients Diagnosed with Tick-Borne Infections
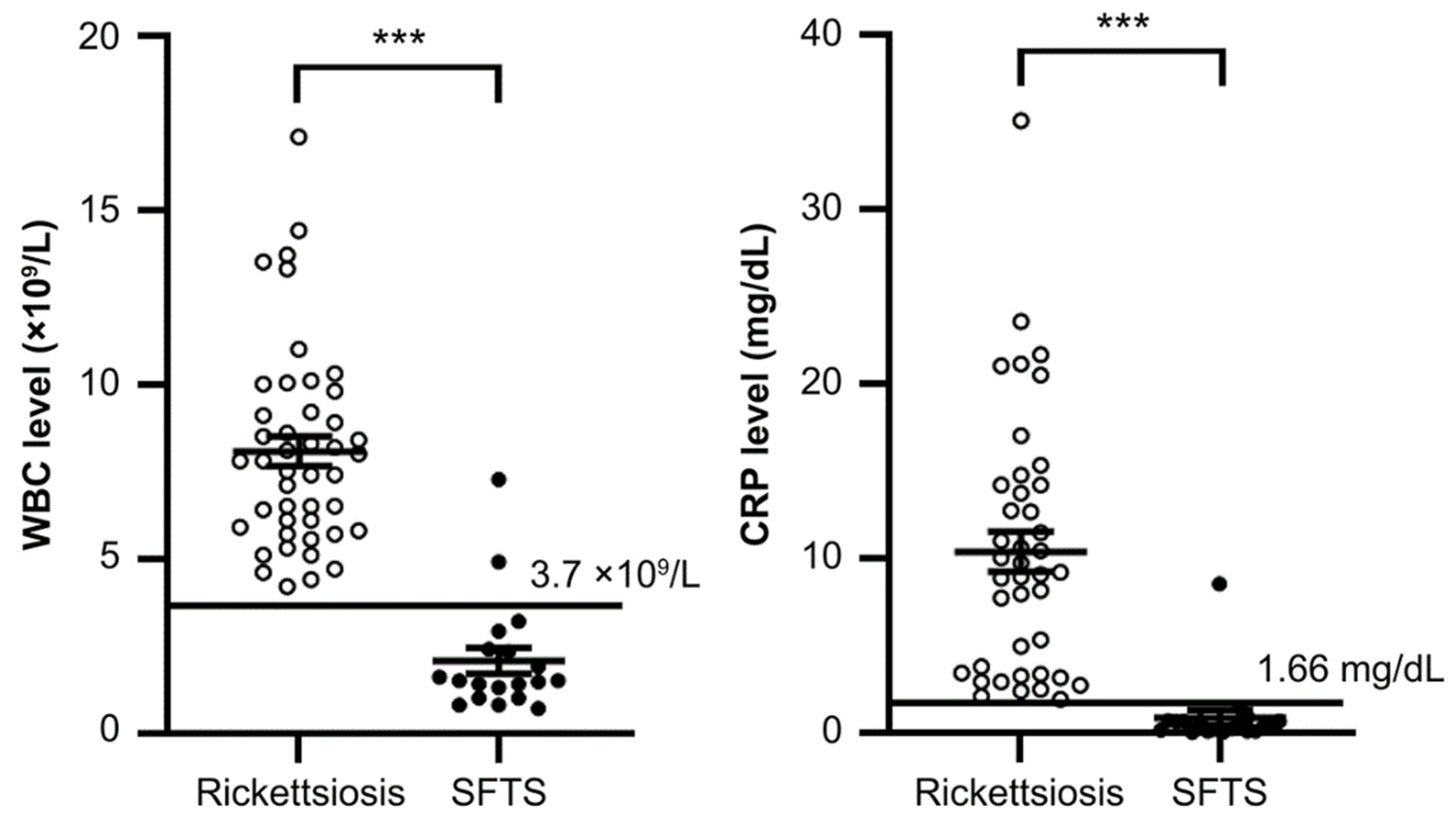
3.2. Comparison of Standard Laboratory Parameters between SFTS and Rickettsiosis
3.3. Diagnostic Performance of Standard Laboratory Parameters
3.4. Predictive Factors for Differentiating SFTS from Rickettsiosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamaji, K.; Aonuma, H.; Kanuka, H. Distribution of tick-borne diseases in Japan: Past patterns and implications for the future. J. Infect. Chemother. 2018, 24, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Arima, Y.; Shigematsu, M.; Sunagawa, T.; Saijo, M.; Oishi, K.; Ando, S. Descriptive epidemiology of rickettsial Infections in Japan: Scrub typhus and Japanese spotted fever, 2007–2016. Int. J. Infect. Dis. 2021, 105, 560–566. [Google Scholar] [CrossRef]
- Otsuka, Y.; Hagiya, H.; Fukushima, S.; Harada, K.; Koyama, T.; Otsuka, F. Trends in the Incidence of Japanese Spotted Fever in Japan: A Nationwide, Two-Decade Observational Study from 2001–2020. Am. J. Trop. Med. Hyg. 2023, 108, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Kato, H.; Yamagishi, T.; Shimada, T.; Matsui, T.; Yoshikawa, T.; Kurosu, T.; Shimojima, M.; Morikawa, S.; Hasegawa, H.; et al. Severe Fever with Thrombocytopenia Syndrome, Japan, 2013–2017. Emerg. Infect. Dis. 2020, 26, 692–699. [Google Scholar] [CrossRef]
- Crump, A.; Tanimoto, T. Severe Fever with Thrombocytopenia Syndrome: Japan under Threat from Life-threatening Emerging Tick-borne Disease. JMA J. 2020, 3, 295–302. [Google Scholar] [CrossRef]
- Seo, J.W.; Kim, D.; Yun, N.; Kim, D.M. Clinical update of severe fever with thrombocytopenia syndrome. Viruses 2021, 13, 1213. [Google Scholar] [CrossRef] [PubMed]
- Blanton, L.S. The Rickettsioses: A Practical Update. Infect. Dis. Clin. N. Am. 2019, 33, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.J.; Liang, M.F.; Zhang, S.Y.; Liu, Y.; Li, J.D.; Sun, Y.L.; Zhang, L.; Zhang, Q.F.; Popov, V.L.; Li, C.; et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Maeda, K.; Suzuki, T.; Ishido, A.; Shigeoka, T.; Tominaga, T.; Kamei, T.; Honda, M.; Ninomiya, D.; Sakai, T.; et al. The first identification and retrospective study of Severe Fever with Thrombocytopenia Syndrome in Japan. J. Infect. Dis. 2014, 209, 816–827. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases-Japan. Severe Fever with Thrombocytopenia Syndrome (SFTS) in Japan, as of June 2019; Infectious Agent Surveillance Report; The Institute of Tokyo: Tokyo, Japan, 2019. [Google Scholar]
- Ding, F.; Zhang, W.; Wang, L.; Hu, W.; Soares Magalhaes, R.J.; Sun, H.; Zhou, H.; Sha, S.; Li, S.; Liu, Q.; et al. Epidemiologic features of severe fever with thrombocytopenia syndrome in China, 2011–2012. Clin. Infect. Dis. 2013, 56, 1682–1683. [Google Scholar] [CrossRef]
- Park, S.Y.; Kwon, J.S.; Kim, J.Y.; Kim, S.M.; Jang, Y.R.; Kim, M.C.; Cho, O.H.; Kim, T.; Chong, Y.P.; Lee, S.O.; et al. Severe fever with thrombocytopenia syndrome-associated encephalopathy/encephalitis. Clin. Microbiol. Infect. 2018, 24, 432.e1–432.e4. [Google Scholar] [CrossRef]
- Miyamoto, S.; Ito, T.; Terada, S.; Eguchi, T.; Furubeppu, H.; Kawamura, H.; Yasuda, T.; Kakihana, Y. Fulminant myocarditis associated with severe fever with thrombocytopenia syndrome: A case report. BMC Infect. Dis. 2019, 19, 266. [Google Scholar] [CrossRef] [PubMed]
- Dualis, H.; Zefong, A.C.; Joo, L.K.; Dadar Singh, N.K.; Syed Abdul Rahim, S.S.; Avoi, R.; Jeffree, M.S.; Hassan, M.R.; Ibrahim, M.Y.; Omar, A. Factors and outcomes in severe fever with thrombocytopenia syndrome (SFTS): A systematic review. Ann. Med. Surg. 2021, 67, 102501. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Song, Z.; Wei, X.; Yuan, H.; Xu, X.; Liang, H.; Wen, H. Clinical laboratory parameters and fatality of Severe fever with thrombocytopenia syndrome patients: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2022, 16, e0010489. [Google Scholar] [CrossRef] [PubMed]
- Gai, Z.; Liang, M.; Zhang, Y.; Zhang, S.; Jin, C.; Wang, S.W.; Sun, L.; Zhou, N.; Zhang, Q.; Sun, Y.; et al. Person-to-person transmission of severe fever with thrombocytopenia syndrome bunyavirus through blood contact. Clin. Infect. Dis. 2012, 54, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Choi, W.; Park, S.W.; Wang, E.B.; Lee, W.J.; Jee, Y.; Lim, K.S.; Lee, H.J.; Kim, S.M.; Lee, S.O.; et al. Nosocomial transmission of severe fever with thrombocytopenia syndrome in Korea. Clin. Infect. Dis. 2015, 60, 1681–1683. [Google Scholar] [CrossRef]
- Yoo, J.R.; Lee, K.H.; Heo, S.T. Surveillance results for family members of patients with severe fever with thrombocytopenia syndrome. Zoonoses Public Health 2018, 65, 903–907. [Google Scholar] [CrossRef]
- Hu, L.; Li, J.; Zhang, H.; Bian, T.; Pan, J.; Li, J.; Xu, X.; Gao, Y.; Chen, G.; Ye, Y.; et al. Predisposing factors for person-to-person transmission of severe fever with thrombocytopenia syndrome bunyavirus. J. Hosp. Infect. 2022, 123, 174–178. [Google Scholar] [CrossRef]
- Sando, E.; Suzuki, M.; Katoh, S.; Fujita, H.; Taira, M.; Yaegashi, M.; Ariyoshi, K. Distinguishing Japanese Spotted Fever and Scrub Typhus, Central Japan, 2004–2015. Emerg. Infect. Dis. 2018, 24, 1633–1641. [Google Scholar] [CrossRef]
- Saijo, M. Pathophysiology of severe fever with thrombocytopenia syndrome and development of specific antiviral therapy. J. Infect. Chemother. 2018, 24, 773–781. [Google Scholar] [CrossRef]
- Saraswati, K.; Day, N.P.J.; Mukaka, M.; Blacksell, S.D. Scrub typhus point-of-care testing: A systematic review and meta-analysis. PLoS. Negl. Trop. Dis. 2018, 12, e0006330. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Umekita, K.; Yamanaka, A.; Hara, S.; Yamaguchi, T.; Inoue, E.; Okayama, A. Impact of C-reactive protein levels on differentiating of severe fever with thrombocytopenia syndrome from Japanese spotted fever. Open Forum Infect. Dis. 2020, 7, ofaa473. [Google Scholar] [CrossRef] [PubMed]
- Ohagi, Y.; Tamura, S.; Nakamoto, C.; Nakamoto, H.; Saijo, M.; Shimojima, M.; Nakano, Y.; Fujimoto, T. Mild clinical course of severe Fever with thrombocytopenia syndrome virus infection in an elderly Japanese patient. Case Rep. Infect. Dis. 2014, 2014, 918135. [Google Scholar] [CrossRef] [PubMed]
- Tamura, S.; Kaki, T.; Niwa, M.; Yamano, Y.; Kawai, S.; Yamashita, Y.; Tanaka, H.; Saito, Y.; Kajimoto, Y.; Koizumi, Y.; et al. Risk Factors for Therapeutic Intervention of Remdesivir in Mild to Moderate COVID-19 -A Single-Center Retrospective Study of the COVID-19 Fourth Pandemic Period in Wakayama, Japan. Medicina 2022, 58, 118. [Google Scholar] [CrossRef]
- Lee, J.S.; Chung, S.Y. The Threat of Climate Change on Tick-Borne Infections: Rising Trend of Infections and Geographic Distribution of Climate Risk Factors Associated with Ticks. J. Infect. Dis. 2023, 227, 295–303. [Google Scholar] [CrossRef]
- Kato, H.; Yamagishi, T.; Shimada, T.; Matsui, T.; Shimojima, M.; Saijo, M.; Oishi, K.; SFTS Epidemiological Research Group-Japan. Epidemiological and clinical features of severe fever with thrombocytopenia syndrome in Japan, 2013–2014. PLoS ONE 2016, 11, e0165207. [Google Scholar] [CrossRef]
- Zu, Z.; Hu, Y.; Zheng, X.; Chen, C.; Zhao, Y.; Jin, Y.; Lin, H.; He, N. A ten-year assessment of the epidemiological features and fatal risk factors of hospitalised severe fever with thrombocytopenia syndrome in Eastern China. Epidemiol. Infect. 2022, 150, e131. [Google Scholar] [CrossRef]
- Liang, S.; Xie, W.; Li, Z.; Zhang, N.; Wang, X.; Qin, Y.; Bao, C.; Hu, J. Analysis of fatal cases of severe fever with thrombocytopenia syndrome in Jiangsu province, China, between 2011 and 2022: A retrospective study. Front. Public Health 2023, 11, 1076226. [Google Scholar] [CrossRef]
- Yasunaga, H.; Horiguchi, H.; Kuwabara, K.; Hashimoto, H.; Matsuda, S. Delay in tetracycline treatment increases the risk of complications in Tsutsugamushi disease: Data from the Japanese diagnosis procedure combination database. Intern. Med. 2011, 50, 37–42. [Google Scholar] [CrossRef]
- Kim, M.C.; Chong, Y.P.; Lee, S.O.; Choi, S.H.; Kim, Y.S.; Woo, J.H.; Kim, S.H. Differentiation of severe fever with thrombocytopenia syndrome from scrub typhus. Clin. Infect. Dis. 2018, 66, 1621–1624. [Google Scholar] [CrossRef]
- Park, S.W.; Lee, C.S.; Kim, J.H.; Bae, I.G.; Moon, C.; Kwak, Y.G.; Kim, B.N.; Lee, J.H.; Ryu, S.Y.; Jang, H.C.; et al. Severe fever with thrombocytopenia syndrome: Comparison with scrub typhus and clinical diagnostic prediction. BMC Infect. Dis. 2019, 19, 174. [Google Scholar] [CrossRef] [PubMed]
- Nakada, N.; Yamamoto, K.; Tanaka, M.; Ashizawa, H.; Yoshida, M.; Umemura, A.; Fukuda, Y.; Katoh, S.; Sumiyoshi, M.; Mihara, S.; et al. Clinical differentiation of severe fever with thrombocytopenia syndrome from Japanese spotted fever. Viruses 2022, 14, 1807. [Google Scholar] [CrossRef] [PubMed]
- Sul, H.; Yun, N.R.; Kim, D.M.; Kim, Y.K.; Kim, J.; Hur, J.; Jung, S.I.; Ryu, S.Y.; Lee, J.Y.; Huh, K.; et al. Development of a scoring system to differentiate severe fever with thrombocytopenia syndrome from scrub typhus. Viruses 2022, 14, 1093. [Google Scholar] [CrossRef]
- van Eekeren, L.E.; de Vries, S.G.; Wagenaar, J.F.P.; Spijker, R.; Grobusch, M.P.; Goorhuis, A. Under-diagnosis of rickettsial disease in clinical practice: A systematic review. Travel Med. Infect. Dis. 2018, 26, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, T.; Kakimoto, K.; Doi, I.; Kawakami, C.; Shimada, T.; Matsui, T.; Oishi, K.; Saijo, M. Transmission routes of the virus causing viral hemorrhagic fever: Extreme precautions are prudent but high-quality evidence must be gathered. Infect. Control Hosp. Epidemiol. 2019, 40, 608–609. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (n = 64) | Rickettsiosis (n = 45) | SFTS (n = 19) | p-Value |
|---|---|---|---|---|
| age (years) | 0.14 | |||
| median [IQR] | 75.5 [68.5–84] | 79 [69–85] | 74 [63–81] | |
| sex, n (%) | 0.83 | |||
| male | 29 (45) | 20 (44) | 9 (47) | |
| female | 35 (51) | 25 (56) | 10 (53) | |
| comorbidities, n (%) | ||||
| hypertension | 25 (39) | 15 (33) | 10 (53) | 0.15 |
| diabetes mellitus | 8 (12) | 4 (9) | 4 (21) | 0.18 |
| hepatic disease | 1 (2) | 1 (2) | 0 (0) | 0.51 |
| chronic kidney disease | 0 (0) | 0 (0) | 0 (0) | |
| cardiac disease | 12 (19) | 11 (24) | 1 (5) | 0.072 |
| pulmonary disease | 2 (3) | 1 (2) | 1 (5) | 0.52 |
| cancer | 7 (11) | 5 (11) | 2 (11) | 0.95 |
| season, n (%) | 0.26 | |||
| spring | 7 (11) | 4 (9) | 3 (16) | |
| summer | 28 (44) | 17 (38) | 11 (58) | |
| autumn | 19 (30) | 16 (36) | 3 (16) | |
| winter | 10 (16) | 8 (18) | 2 (11) | |
| season group | 0.047 | |||
| spring–summer | 35 (55) | 21 (47) | 14 (74) | |
| autumn–winter | 29 (45) | 24 (53) | 5 (26) | |
| eschar, n (%) | 0.046 | |||
| presence | 42 (66) | 33 (73) | 9 (47) | |
| skin rash, n (%) | <0.001 | |||
| presence | 43 (67) | 43 (96) | 0 (0) | |
| gastrointestinal symptoms, n (%) | <0.001 | |||
| vomiting | 4 (6) | 0 (0) | 4 (21) | |
| abdominal pain | 9 (14) | 0 (0) | 9 (47) | |
| diarrhea | 9 (14) | 0 (0) | 9 (47) | |
| >2 symptoms | 17 (27) | 0 (0) | 17 (89) | |
| treatments, n (%) | ||||
| antimicrobial | 57 (89) | 45 (100) | 12 (63) | |
| steroid | 2 (3) | 0 (0) | 2 (11) | |
| immunoglobulin replacement | 2 (3) | 0 (0) | 2 (11) | |
| outcome, n (%) | ||||
| ICU admission | 9 (14) | 1 (2) | 8 (42) | |
| death | 4 (6) | 1 (2) | 3 (16) |
| Variable | Total (n = 64) | Rickettsiosis (n = 45) | SFTS (n = 19) | p-Value |
|---|---|---|---|---|
| WBC (×109/L) | n = 64 | n = 45 | n = 19 | <0.001 |
| median [IQR] | 6.25 [3.06–8.45] | 7.8 [5.90–9.20] | 1.5 [1.00–2.41] | |
| Hb (g/dL) | n = 64 | n = 45 | n = 19 | 0.006 |
| median [IQR] | 13.6 [12.1–15.0] | 13.3 [12.0–14.5] | 15.1 [13.4–15.8] | |
| PLT (×109/L) | n = 64 | n = 45 | n = 19 | <0.001 |
| median [IQR] | 10.55 [7.40–13.35] | 11.8 [9.60–16.1] | 5.10 [3.30–8.30] | |
| AST (IU/L) | n = 64 | n = 45 | n = 19 | <0.001 |
| median [IQR] | 63 [44–130] | 53 [39–79] | 161 [91–390] | |
| ALT (IU/L) | n = 64 | n = 45 | n = 19 | 0.001 |
| median [IQR] | 47.5 [29–90.5] | 42 [25–61] | 83 [48–135] | |
| T-Bil (IU/L) | n = 63 | n = 44 | n = 19 | 0.028 |
| median [IQR] | 0.6 [0.5–0.8] | 0.6 [0.5–0.9] | 0.5 [0.4–0.6] | |
| LDH (IU/L) | n = 63 | n = 44 | n = 19 | <0.001 |
| median [IQR] | 384 [280–541] | 353 [266–421.5] | 559 [384–1039] | |
| CK (mg/dL) | n = 62 | n = 43 | n = 19 | 0.002 |
| median [IQR] | 166 [102–398] | 135 [78–235] | 308 [155–2127] | |
| Cr (mg/dL) | n = 64 | n = 45 | n = 19 | 0.25 |
| median [IQR] | 1.0 [0.7–1.2] | 0.9 [0.8–1.2] | 1.1 [0.7–1.5] | |
| BUN (mg/dL) | n = 63 | n = 44 | n = 19 | 0.085 |
| median [IQR] | 19.5 [14–27] | 19.1 [14–24.1] | 25.3 [15–38] | |
| CRP (mg/dL) | n = 60 | n = 41 | n = 19 | <0.001 |
| median [IQR] | 4.4 [0.7–11.2] | 9.2 [3.4–14.2] | 0.4 [0.1–0.7] | |
| PT-INR | n = 52 | n = 33 | n = 19 | 0.017 |
| median [IQR] | 1.1 [1.0–1.2] | 1.1 [1.1–1.2] | 1.0 [1.0–1.1] |
| n | AUC | SE | 95% CI | |
|---|---|---|---|---|
| WBC | 64 | 0.97 | 0.023 | 0.93–1 |
| Hb | 64 | 0.72 | 0.081 | 0.56–0.88 |
| PLT | 64 | 0.88 | 0.049 | 0.78–0.98 |
| AST | 64 | 0.83 | 0.059 | 0.72–0.95 |
| ALT | 64 | 0.75 | 0.064 | 0.63–0.88 |
| T-Bil | 63 | 0.67 | 0.074 | 0.53–0.82 |
| LDH | 63 | 0.81 | 0.064 | 0.68–0.93 |
| CK | 62 | 0.75 | 0.066 | 0.62–0.88 |
| Cr | 64 | 0.59 | 0.086 | 0.42–0.76 |
| BUN | 63 | 0.64 | 0.087 | 0.47–0.81 |
| CRP | 60 | 0.98 | 0.022 | 0.93–1 |
| PT-INR | 52 | 0.70 | 0.082 | 0.54–0.86 |
| n | AUC | 95% CI | Sensitivity | Specificity | LR+ | LR− | p-Value | |
|---|---|---|---|---|---|---|---|---|
| spring–summer | 64 | 0.63 | 0.51–0.76 | 53.3% | 73.7% | 2.03 | 0.63 | 0.047 |
| absence of skin rash | 64 | 0.98 | 0.95–1 | 95.6% | 100% | − | 0.04 | <0.001 |
| absence of eschar | 64 | 0.63 | 0.50–0.76 | 73.3% | 52.6% | 1.55 | 0.51 | 0.046 |
| presence of gastrointestinal symptoms | 64 | 0.95 | 0.88–1 | 89.5% | 100% | − | 0.11 | <0.001 |
| WBC < 3.7 × 109/L | 64 | 0.95 | 0.88–1 | 89.5% | 100% | − | 0.11 | <0.001 |
| PLT < 8.9 × 109/L | 64 | 0.84 | 0.76–0.94 | 89.5% | 80.0% | 4.45 | 0.13 | <0.001 |
| AST > 85.5 IU/L | 64 | 0.79 | 0.65–0.89 | 79.0% | 80.0% | 3.95 | 0.26 | <0.001 |
| LDH > 500 IU/L | 63 | 0.75 | 0.63–0.87 | 68.4% | 82.2% | 3.85 | 0.38 | <0.001 |
| CRP < 1.66 mg/dL | 60 | 0.97 | 0.92–1 | 94.7% | 100% | − | 0.05 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teramoto, K.; Tamura, S.; Yoshida, K.; Inada, Y.; Yamashita, Y.; Morimoto, M.; Mushino, T.; Koreeda, D.; Miyamoto, K.; Komiya, N.; et al. Clinical Characteristics and Diagnostic Prediction of Severe Fever with Thrombocytopenia Syndrome and Rickettsiosis in the Co-Endemic Wakayama Prefecture, Japan. Medicina 2023, 59, 2024. https://doi.org/10.3390/medicina59112024
Teramoto K, Tamura S, Yoshida K, Inada Y, Yamashita Y, Morimoto M, Mushino T, Koreeda D, Miyamoto K, Komiya N, et al. Clinical Characteristics and Diagnostic Prediction of Severe Fever with Thrombocytopenia Syndrome and Rickettsiosis in the Co-Endemic Wakayama Prefecture, Japan. Medicina. 2023; 59(11):2024. https://doi.org/10.3390/medicina59112024
Chicago/Turabian StyleTeramoto, Kan, Shinobu Tamura, Kikuaki Yoshida, Yukari Inada, Yusuke Yamashita, Masaya Morimoto, Toshiki Mushino, Daisuke Koreeda, Kyohei Miyamoto, Nobuhiro Komiya, and et al. 2023. "Clinical Characteristics and Diagnostic Prediction of Severe Fever with Thrombocytopenia Syndrome and Rickettsiosis in the Co-Endemic Wakayama Prefecture, Japan" Medicina 59, no. 11: 2024. https://doi.org/10.3390/medicina59112024