
Beyond the Acute Phase: Long-Term Impact of COVID-19 on Functional Capacity and Prothrombotic Risk—A Pilot Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
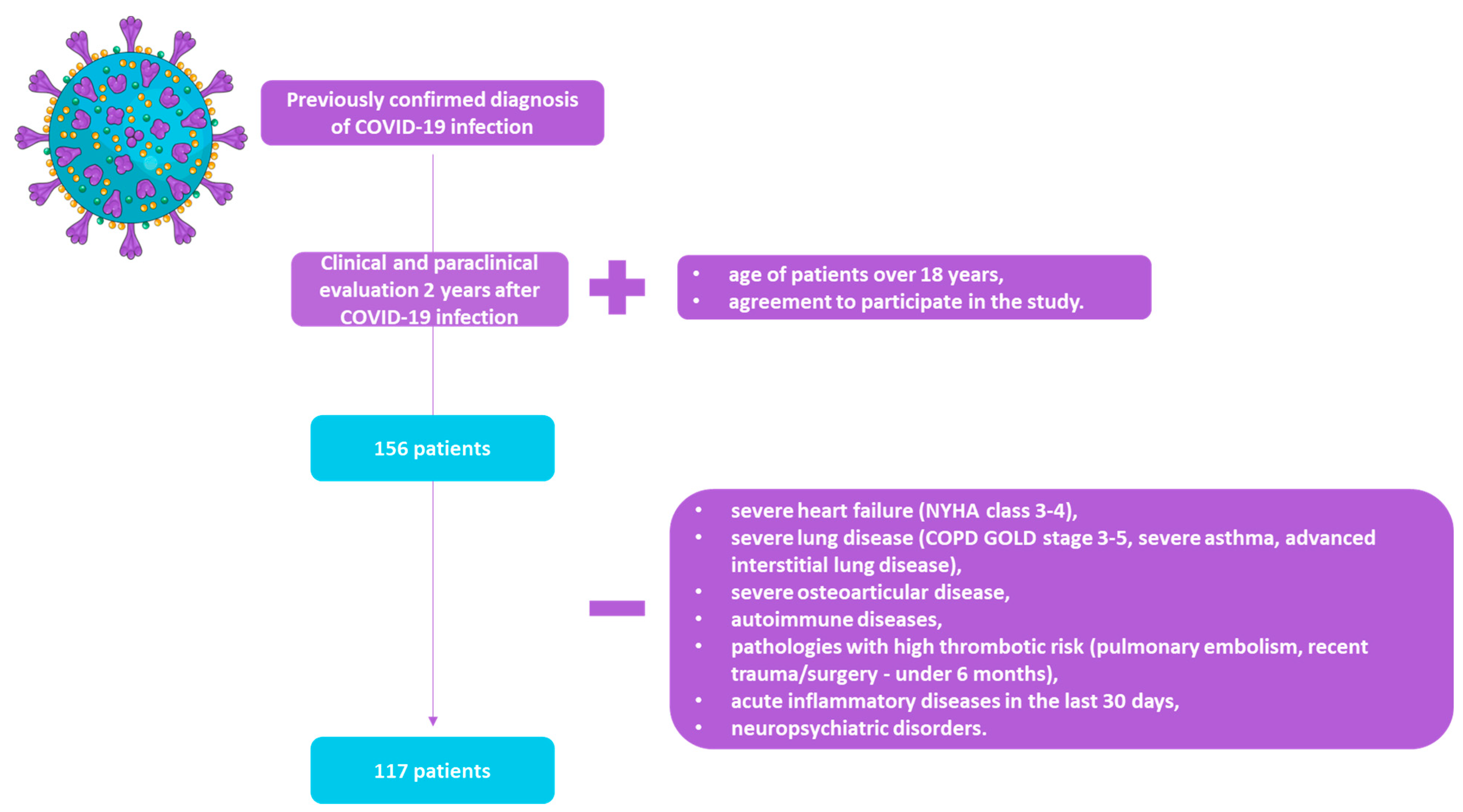
2.1. Study Design
2.2. Measurements
2.2.1. General Data, Past Medical History, and Symptoms
2.2.2. Laboratory Data
2.2.3. Pulmonary Function Tests (Spirometry, Body Plethysmography)
- –
- Obstructive ventilatory pattern if FEV1/FVC ratio is less than 70%, FEV1 is less than 80%, and hyperinflation if increased RV and TLC;
- –
- Restrictive pattern if normal FEV1/FVC ratio (<70%) and a reduction in FVC and TLC under 80% of predicted values;
- –
- Mixed pattern when both FEV1/FVC ratio and TLC, as well FVC, are decreased below predicted values.
2.2.4. Six-Minute Walk Test
- Male gender: 867 − [5.71 × age] + [1.03 × height (cm)] (m);
- Female gender: 525 − [2.86 × age] + [2.71 × height (cm)] − [6.22 × BMI] (m).
2.2.5. Other Data
2.3. Statistical Analysis
2.4. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spiteri, G.; Fielding, J.; Diercke, M.; Campese, C.; Enouf, V.; Gaymard, A.; Bella, A.; Sognamiglio, P.; Sierra Moros, M.J.; Riutort, A.N.; et al. First Cases of Coronavirus Disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Euro Surveill. Bull. Eur. Sur Mal. Transm. Eur. Commun. Dis. Bull. 2020, 25, 2000178. [Google Scholar] [CrossRef]
- Perumal, R.; Shunmugam, L.; Naidoo, K.; Abdool Karim, S.S.; Wilkins, D.; Garzino-Demo, A.; Brechot, C.; Parthasarathy, S.; Vahlne, A.; Nikolich, J.Ž. Long COVID: A Review and Proposed Visualization of the Complexity of Long COVID. Front. Immunol. 2023, 14, 1117464. [Google Scholar] [CrossRef] [PubMed]
- Bull-Otterson, L.; Baca, S.; Saydah, S.; Boehmer, T.K.; Adjei, S.; Gray, S.; Harris, A.M. Post–COVID Conditions among Adult COVID-19 Survivors Aged 18–64 and ≥65 Years—United States, March 2020–November 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 713–717. [Google Scholar] [CrossRef]
- Department of Health and Human Services, Office of the Assistant Secretary for Health. National Research Action Plan on Long COVID. 2022. Available online: https://www.covid.gov/sites/default/files/documents/National-Research-Action-Plan-on-Long-COVID-08012022.pdf (accessed on 15 November 2023).
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-Term Cardiovascular Outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.W.; Stiles, L.E.; Shaik, R.; Schneider, L.; Muppidi, S.; Tsui, C.T.; Geng, L.N.; Bonilla, H.; Miglis, M.G. Characterization of Autonomic Symptom Burden in Long COVID: A Global Survey of 2314 Adults. Front. Neurol. 2022, 13, 1012668. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-Term and Long-Term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Duong-Quy, S.; Vo-Pham-Minh, T.; Tran-Xuan, Q.; Huynh-Anh, T.; Vo-Van, T.; Vu-Tran-Thien, Q.; Nguyen-Nhu, V. Post-COVID-19 Pulmonary Fibrosis: Facts—Challenges and Futures: A Narrative Review. Pulm. Ther. 2023, 9, 295–307. [Google Scholar] [CrossRef]
- das Posses Bridi, G.; Tanni, S.E.; Baldi, B.G. Current Understanding of Post-COVID Pulmonary Fibrosis: Where Are We? Arch. Bronconeumol. 2023, 59, 69–70. [Google Scholar] [CrossRef]
- Tanni, S.E.; Fabro, A.T.; de Albuquerque, A.; Ferreira, E.V.M.; Verrastro, C.G.Y.; Sawamura, M.V.Y.; Ribeiro, S.M.; Baldi, B.G. Pulmonary Fibrosis Secondary to COVID-19: A Narrative Review. Expert Rev. Respir. Med. 2021, 15, 791–803. [Google Scholar] [CrossRef]
- Chiner-Vives, E.; Cordovilla-Pérez, R.; de la Rosa-Carrillo, D.; García-Clemente, M.; Izquierdo-Alonso, J.L.; Otero-Candelera, R.; Pérez-de Llano, L.; Sellares-Torres, J.; de Granda-Orive, J.I. Short and Long-Term Impact of COVID-19 Infection on Previous Respiratory Diseases. Arch. Bronconeumol. 2022, 58, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Baldi, B.G.; Tanni, S.E. Pulmonary fibrosis and follow-up of COVID-19 survivors: An urgent need for clarification. J. Bras. Pneumol. 2021, 47, e20210213. [Google Scholar] [CrossRef] [PubMed]
- McGroder, C.F.; Zhang, D.; Choudhury, M.A.; Salvatore, M.M.; D’Souza, B.M.; Hoffman, E.A.; Wei, Y.; Baldwin, M.R.; Garcia, C.K. Pulmonary Fibrosis 4 Months after COVID-19 Is Associated with Severity of Illness and Blood Leucocyte Telomere Length. Thorax 2021, 76, 1242–1245. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; Jing, H.; Wang, C.; Novakovic, V.A.; Shi, J. Persistent Lung Injury and Prothrombotic State in Long COVID. Front. Immunol. 2022, 13, 862522. [Google Scholar] [CrossRef] [PubMed]
- Godoy, L.C.; Goligher, E.C.; Lawler, P.R.; Slutsky, A.S.; Zarychanski, R. Anticipating and Managing Coagulopathy and Thrombotic Manifestations of Severe COVID-19. CMAJ Can. Med. Assoc. J. 2020, 192, E1156–E1161. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, K.M.; Vasarmidi, E.; Russell, A.-M.; Andrejak, C.; Crestani, B.; Delcroix, M.; Dinh-Xuan, A.T.; Poletti, V.; Sverzellati, N.; Vitacca, M.; et al. European Respiratory Society Statement on Long COVID Follow-Up. Eur. Respir. J. 2022, 60, 2102174. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yu, C.; Jing, H.; Wu, X.; Novakovic, V.A.; Xie, R.; Shi, J. Long COVID: The Nature of Thrombotic Sequelae Determines the Necessity of Early Anticoagulation. Front. Cell. Infect. Microbiol. 2022, 12, 861703. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, H.; Townsend, L.; Morrin, H.; Ahmad, A.; Comerford, C.; Karampini, E.; Englert, H.; Byrne, M.; Bergin, C.; O’Sullivan, J.M.; et al. Persistent Endotheliopathy in the Pathogenesis of Long COVID Syndrome. J. Thromb. Haemost. 2021, 19, 2546–2553. [Google Scholar] [CrossRef]
- Nicolai, L.; Kaiser, R.; Stark, K. Thromboinflammation in Long COVID—The Elusive Key to Postinfection Sequelae? J. Thromb. Haemost. 2023, 21, 2020–2031. [Google Scholar] [CrossRef]
- Barnes, G.D.; Burnett, A.; Allen, A.; Ansell, J.; Blumenstein, M.; Clark, N.P.; Crowther, M.; Dager, W.E.; Deitelzweig, S.B.; Ellsworth, S.; et al. Thromboembolic Prevention and Anticoagulant Therapy during the COVID-19 Pandemic: Updated Clinical Guidance from the Anticoagulation Forum. J. Thromb. Thrombolysis 2022, 54, 197–210. [Google Scholar] [CrossRef]
- Maia, R.; Carvalho, V.; Faria, B.; Miranda, I.; Catarino, S.; Teixeira, S.; Lima, R.; Minas, G.; Ribeiro, J. Diagnosis Methods for COVID-19: A Systematic Review. Micromachines 2022, 13, 1349. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Herzog, C.A.; Asinger, R.W.; Berger, A.K.; Charytan, D.M.; Díez, J.; Hart, R.G.; Eckardt, K.-U.; Kasiske, B.L.; McCullough, P.A.; Passman, R.S.; et al. Cardiovascular Disease in Chronic Kidney Disease. A Clinical Update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011, 80, 572–586. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur. Respir. J. 2023, 28, 316–338. [Google Scholar] [CrossRef]
- Park, J.G.; Ramar, K.; Olson, E.J. Updates on Definition, Consequences, and Management of Obstructive Sleep Apnea. Mayo Clin. Proc. 2011, 86, 549–555. [Google Scholar] [CrossRef] [PubMed]
- NICE. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence: Clinical Guidelines; National Institute for Health and Care Excellence (NICE): London, UK, 2020; ISBN 978-1-47313-943-5. [Google Scholar]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Criée, C.P.; Sorichter, S.; Smith, H.J.; Kardos, P.; Merget, R.; Heise, D.; Berdel, D.; Köhler, D.; Magnussen, H.; Marek, W.; et al. Body Plethysmography—Its Principles and Clinical Use. Respir. Med. 2011, 105, 959–971. [Google Scholar] [CrossRef]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS Technical Standard on Interpretive Strategies for Routine Lung Function Tests. Eur. Respir. J. 2022, 60, 2101499. [Google Scholar] [CrossRef]
- Hama Amin, B.J.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; Mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 Pulmonary Fibrosis; a Meta-Analysis Study. Ann. Med. Surg. 2022, 77, 103590. [Google Scholar] [CrossRef] [PubMed]
- Chetta, A.; Zanini, A.; Pisi, G.; Aiello, M.; Tzani, P.; Neri, M.; Olivieri, D. Reference Values for the 6-Min Walk Test in Healthy Subjects 20–50 Years Old. Respir. Med. 2006, 100, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Debski, M.; Tsampasian, V.; Haney, S.; Blakely, K.; Weston, S.; Ntatsaki, E.; Lim, M.; Madden, S.; Perperoglou, A.; Vassiliou, V.S. Post-COVID-19 Syndrome Risk Factors and Further Use of Health Services in East England. PLoS Glob. Public Health 2022, 2, e0001188. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female Gender Is Associated with Long COVID Syndrome: A Prospective Cohort Study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef] [PubMed]
- Florencio, L.L.; Fernández-de-las-Peñas, C. Long COVID: Systemic Inflammation and Obesity as Therapeutic Targets. Lancet Respir. Med. 2022, 10, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Pérez-González, A.; Araújo-Ameijeiras, A.; Fernández-Villar, A.; Crespo, M.; Poveda, E. Long COVID in Hospitalized and Non-Hospitalized Patients in a Large Cohort in Northwest Spain, a Prospective Cohort Study. Sci. Rep. 2022, 12, 3369. [Google Scholar] [CrossRef]
- Adegunsoye, A.; Baccile, R.; Best, T.J.; Zaksas, V.; Zhang, H.; Karnik, R.; Patel, B.K.; Solomonides, A.E.; Parker, W.F.; Solway, J. Pharmacotherapy and Pulmonary Fibrosis Risk after SARS-CoV-2 Infection: A Prospective Nationwide Cohort Study in the United States. Lancet Reg. Health—Am. 2023, 25, 100566. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic Dysfunction in ‘Long COVID’: Rationale, Physiology and Management Strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Pasini, E.; Corsetti, G.; Romano, C.; Scarabelli, T.M.; Chen-Scarabelli, C.; Saravolatz, L.; Dioguardi, F.S. Serum Metabolic Profile in Patients With Long-COVID (PASC) Syndrome: Clinical Implications. Front. Med. 2021, 8, 714426. [Google Scholar] [CrossRef]
- Lin, H.; Liu, X.; Sun, H.; Zhang, J.; Dong, S.; Liu, M.; Li, L.; Tian, J.; Guo, Y.; Gan, J.; et al. Sustained Abnormality with Recovery of COVID-19 Convalescents: A 2-Year Follow-up Study. Sci. Bull. 2022, 67, 1556–1561. [Google Scholar] [CrossRef]
- Lechuga, G.C.; Morel, C.M.; De-Simone, S.G. Hematological Alterations Associated with Long COVID-19. Front. Physiol. 2023, 14, 1203472. [Google Scholar] [CrossRef] [PubMed]
- Schrottmaier, W.C.; Pirabe, A.; Pereyra, D.; Heber, S.; Hackl, H.; Schmuckenschlager, A.; Brunnthaler, L.; Santol, J.; Kammerer, K.; Oosterlee, J.; et al. Adverse Outcome in COVID-19 Is Associated With an Aggravating Hypo-Responsive Platelet Phenotype. Front. Cardiovasc. Med. 2021, 8, 795624. [Google Scholar] [CrossRef] [PubMed]
- Len, P.; Iskakova, G.; Sautbayeva, Z.; Kussanova, A.; Tauekelova, A.T.; Sugralimova, M.M.; Dautbaeva, A.S.; Abdieva, M.M.; Ponomarev, E.D.; Tikhonov, A.; et al. Meta-Analysis and Systematic Review of Coagulation Disbalances in COVID-19: 41 Studies and 17,601 Patients. Front. Cardiovasc. Med. 2022, 9, 794092. [Google Scholar] [CrossRef] [PubMed]
- Ercan, H.; Schrottmaier, W.C.; Pirabe, A.; Schmuckenschlager, A.; Pereyra, D.; Santol, J.; Pawelka, E.; Traugott, M.T.; Schörgenhofer, C.; Seitz, T.; et al. Platelet Phenotype Analysis of COVID-19 Patients Reveals Progressive Changes in the Activation of Integrin AIIbβ3, F13A1, the SARS-CoV-2 Target EIF4A1 and Annexin A5. Front. Cardiovasc. Med. 2021, 8, 779073. [Google Scholar] [CrossRef] [PubMed]
- Lundström, A.; Sandén, P.; Mitroulis, I.; van der Meijden, P.E.J. Editorial: Platelet Function in COVID-19. Front. Cardiovasc. Med. 2022, 9, 912472. [Google Scholar] [CrossRef] [PubMed]
- Quispe-Pari, J.F.; Gonzales-Zamora, J.A.; Munive-Dionisio, J.; Castro-Contreras, C.; Villar-Astete, A.; Kong-Paravicino, C.; Vilcapoma-Balbin, P.; Hurtado-Alegre, J. Mean Platelet Volume as a Predictor of COVID-19 Severity: A Prospective Cohort Study in the Highlands of Peru. Diseases 2022, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Demircioglu, O.; Kocakaya, D.; Cimsit, C.; Cimsit, N.C. New Grading System for Post-COVID-19 Pulmonary Fibrosis Based on Computed Tomography Findings. Medicine 2022, 101, e30146. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and Cognitive Impairment in Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. Brain. Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Skala, M.; Svoboda, M.; Kopecky, M.; Kocova, E.; Hyrsl, M.; Homolac, M.; Chrobok, V.; Bostik, P.; Fajfr, M.; Prasil, P.; et al. Heterogeneity of Post-COVID Impairment: Interim Analysis of a Prospective Study from Czechia. Virol. J. 2021, 18, 73. [Google Scholar] [CrossRef]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary Recovery after COVID-19: An Observational Prospective Multicentre Trial. Eur. Respir. J. 2021, 57, 2003481. [Google Scholar] [CrossRef]
- Venturelli, S.; Benatti, S.V.; Casati, M.; Binda, F.; Zuglian, G.; Imeri, G.; Conti, C.; Biffi, A.M.; Spada, M.S.; Bondi, E.; et al. Surviving COVID-19 in Bergamo Province: A Post-Acute Outpatient Re-Evaluation. Epidemiol. Infect. 2021, 149, e32. [Google Scholar] [CrossRef] [PubMed]
- George, P.M.; Reed, A.; Desai, S.R.; Devaraj, A.; Faiez, T.S.; Laverty, S.; Kanwal, A.; Esneau, C.; Liu, M.K.C.; Kamal, F.; et al. A Persistent Neutrophil-Associated Immune Signature Characterizes Post–COVID-19 Pulmonary Sequelae. Sci. Transl. Med. 2022, 14, eabo5795. [Google Scholar] [CrossRef] [PubMed]
- Burgy, O.; Loriod, S.; Beltramo, G.; Bonniaud, P. Extracellular Lipids in the Lung and Their Role in Pulmonary Fibrosis. Cells 2022, 11, 1209. [Google Scholar] [CrossRef] [PubMed]
- Durrington, P. Blood Lipids after COVID-19 Infection. Lancet Diabetes Endocrinol. 2023, 11, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Wygrecka, M.; Hadzic, S.; Potaczek, D.P.; Alexopoulos, I.; El Agha, E.; Schaefer, L. Decoding the Role of Fatty Acids and Their Metabolites in Lung Fibrosis. Pol. Arch. Intern. Med. 2023, 133, 16520. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Dai, J. Lipid Metabolism in Idiopathic Pulmonary Fibrosis: From Pathogenesis to Therapy. J. Mol. Med. Berl. Ger. 2023, 101, 905–915. [Google Scholar] [CrossRef]
- Wygrecka, M.; Alexopoulos, I.; Potaczek, D.P.; Schaefer, L. Diverse Functions of Apolipoprotein A-I in Lung Fibrosis. Am. J. Physiol. Cell Physiol. 2023, 324, C438–C446. [Google Scholar] [CrossRef]
- Suppini, N.; Fira-Mladinescu, O.; Traila, D.; Motofelea, A.C.; Marc, M.S.; Manolescu, D.; Vastag, E.; Maganti, R.K.; Oancea, C. Longitudinal Analysis of Pulmonary Function Impairment One Year Post-COVID-19: A Single-Center Study. J. Pers. Med. 2023, 13, 1190. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Group (n = 117) | Without Pulmonary Fibrosis (n = 68) | With Pulmonary Fibrosis (n = 49) | p |
|---|---|---|---|---|
| Demographics | ||||
| Age | 65.74 ± 10.19 | 65.04 ± 9.07 | 66.36 ± 11.57 | 0.270 |
| Gender (females) | 81 (69.23%) | 49 (72.06%) | 32 (65.31%) | 0.435 |
| Area of residence (urban) | 70 (59.82%) | 41 (60.29%) | 29 (59.18%) | 0.904 |
| Anthropometric data | ||||
| Height, m | 1.65 ± 0.28 | 1.61 ± 0.09 | 1.71 ± 0.43 | 0.027 |
| Weight, kg | 82.21 ± 15.64 | 82.02 ± 13.91 | 82.96 ± 18.06 | 0.566 |
| BMI, kg/m2 | 31.42 ± 5.71 | 31.15 ± 5.11 | 32.16 ± 6.27 | 0.975 |
| Comorbidities | ||||
| COPD | 22 (18.80%) | 9 (13.24%) | 13 (26.53%) | 0.069 |
| OSA | 14 (11.97%) | 9 (13.24%) | 5 (10.20%) | 0.618 |
| Asthma | 21 (17.95%) | 13 (19.12%) | 8 (16.33%) | 0.698 |
| Hypertension | 78 (66.67%) | 44 (64.71%) | 34 (69.39%) | 0.596 |
| Chronic coronary syndromes | 33 (28.21%) | 17 (25.00%) | 16 (32.65%) | 0.364 |
| Arrhythmias/atrio-ventricular conduction disorders | 26 (22.22%) | 11 (16.18%) | 15 (30.61%) | 0.064 |
| Stroke | 5 (4.27%) | 4 (5.88%) | 1 (2.04%) | 0.311 |
| Heart failure | 20 (17.97%) | 10 (14.71%) | 10 (20.41%) | 0.419 |
| Type 2 diabetes mellitus | 40 (34.19%) | 28 (41.18%) | 12 (24.49%) | 0.060 |
| Chronic kidney disease | 10 (8.62%) | 3 (4.41%) | 7 (14.58%) | 0.055 |
| Neoplasia | 5 (4.27%) | 2 (2.94%) | 3 (6.12%) | 0.401 |
| Active smoking | 11 (9.40%) | 5 (7.35%) | 6 (12.24%) | 0.371 |
| Alcohol consumption | 17 (14.5%) | 11 (16.18%) | 6 (12.24%) | 0.552 |
| Biological data | ||||
| CRP, mg/dL | 1.32 ± 2.02 | 0.98 ± 0.56 | 1.82 ± 3.07 | 0.048 |
| ESR, mm/h | 21.56 ± 14.51 | 20.47 ± 12.25 | 23.32 ± 17.46 | 0.737 |
| Hemoglobin, g/dL | 13.98 ± 12.66 | 14.70 ± 16.57 | 13.01 ± 1.52 | 0.395 |
| Hematocrit, % | 38.95 ± 12.66 | 38.83 ± 3.33 | 39.88 ± 4.83 | 0.311 |
| MCV | 92.83 ± 5.22 | 92.44 ± 5.26 | 93.43 ± 5.27 | 0.509 |
| Platelets (×103/mL) | 263.21 ± 68.56 | 266.68 ± 62.48 | 242.66 ± 75.13 | 0.047 |
| MPV, fL | 8.93 ± 0.89 | 7.22 ± 0.93 | 10.25 ± 0.86 | 0.038 |
| WBC (×103/mm3) | 8.10 ± 12.46 | 7.45 ± 7.86 | 9.18 ± 17.24 | 0.053 |
| Neutrophils (×103/mm3) | 6.40 ± 12.70 | 4.68 ± 7.88 | 9.07 ± 17.44 | 0.032 |
| Lymphocytes (×103/mm3) | 3.15 ± 5.54 | 2.88 ± 4.90 | 3.61 ± 6.49 | 0.856 |
| Eosinophils (×103/mm3) | 0.28 ± 0.42 | 0.26 ± 0.37 | 0.31 ± 0.48 | 0.575 |
| D-dimers, mg/L | 264.43 ± 130.37 | 245.57 ± 78.19 | 283.29 ± 160.32 | 0.018 |
| Lactate dehydrogenase, UI/L | 321.13 ± 117.53 | 296.19 ± 73.76 | 349.63 ± 151.33 | 0.039 |
| Ferritin | 109.77 ± 77.30 | 101.65 ± 75.40 | 119.71 ± 80.60 | 0.470 |
| Total cholesterol, mg/dL | 204.03 ± 46.30 | 200.41 ± 44.90 | 208.62 ± 49.18 | 0.344 |
| LDL-cholesterol, mg/dL | 125.56 ± 41.03 | 123.03 ± 38.24 | 130.47 ± 46.04 | 0.642 |
| HDL-cholesterol, mg/dL | 65.16 ± 15.57 | 63.27 ± 15.84 | 66.12 ± 14.68 | 0.205 |
| Triglycerides, mg/dL | 137.12 ± 60.29 | 139.15 ± 57.67 | 136.99 ± 64.28 | 0.460 |
| ALT, UI/L | 22.57 ± 12.56 | 21.53 ± 11.46 | 24.15 ± 14.13 | 0.611 |
| AST, UI/L | 20.47 ± 8.34 | 19.28 ± 7.79 | 21.91 ± 8.70 | 0.023 |
| Total bilirubin, mg/dL | 0.72 ± 0.91 | 0.77 ± 1.14 | 0.61 ± 0.26 | 0.700 |
| Direct bilirubin, mg/dL | 0.46 ± 2.59 | 0.68 ± 3.51 | 0.18 ± 0.09 | 0.732 |
| Alkaline phosphatase, UI/L | 85.88 ± 23.43 | 89.10 ± 25.68 | 81.30 ± 19.85 | 0.606 |
| GGT, UI/L | 40.93 ± 60.13 | 37.73 ± 67.02 | 46.39 ± 50.29 | 0.219 |
| Uric acid, mg/dL | 4.70 ± 1.52 | 4.50 ± 1.25 | 4.97 ± 1.82 | 0.180 |
| Fasting glucose, mg/dL | 114.24 ± 28.00 | 116.01 ± 32.49 | 112.15 ± 20.61 | 0.895 |
| Glycosylated hemoglobin | 6.93 ± 1.63 | 7 ± 1.62 | 6.81 ± 1.72 | 0.714 |
| Vitals, ECG derived parameters | ||||
| HR, bpm | 70.24 ± 13.88 | 68.26 ± 12.23 | 73.37 ± 15.90 | 0.033 |
| QT interval corrected, ms | 326.13 ± 148.20 | 297.12 ± 158.05 | 362.11 ± 126.45 | 0.018 |
| QRS duration, ms | 191.48 ± 147.77 | 211.48 ± 157.22 | 164.55 ± 130.11 | 0.705 |
| Spirometry | ||||
| FEV1, (%) | 95.83 ± 29.36 | 97.33 ± 29.39 | 92.53 ± 29.47 | 0.545 |
| FVC, (%) | 100.38 ± 26.75 | 101.25 ± 25.44 | 98 ± 28.67 | 0.700 |
| FEV1/FVC | 78.68 ± 12.29 | 78.93 ± 11.48 | 78.30 ± 13.73 | 0.747 |
| MEF50, (%) | 74.09 ± 38.60 | 74.35 ± 38.27 | 73.33 ± 40.28 | 0.831 |
| Body Plethysmography | ||||
| DLCO corr (%) | 67.39 ± 20.66 | 69.53 ± 18.82 | 65.70 ± 22.02 | 0.311 |
| DLCO corr (ml) | 15.59 ± 5.55 | 16.08 ± 5.36 | 15.23 ± 5.74 | 0.448 |
| Body CRF | 96.30 ± 29.58 | 95.12 ± 27.63 | 98.29 ± 32.63 | 0.827 |
| Body CPT | 91.11 ± 22.49 | 88.02 ± 21.43 | 95.21 ± 23.76 | 0.125 |
| Body specific airway resistance | 7.24 ± 4.70 | 6.93 ± 4.44 | 7.66 ± 5.13 | 0.514 |
| 6-minute walk test | ||||
| Distance, m | 366.09 ± 137.45 | 365.74 ± 142.29 | 366.51 ± 133.36 | 0.847 |
| SpO2 post-test, % | 96.17 ± 1.67 | 96.28 ± 1.80 | 96.05 ± 1.52 | 0.238 |
| Distance–saturation product | 35,271.24 ± 13,289.31 | 36,332.44 ± 13,612.37 | 33,755.23 ± 12,855.12 | 0.307 |
| Dyspnea (Borg scale) | 2.89 ± 1.46 | 2.77 ± 0.86 | 3.04 ± 2.02 | 0.275 |
| With Pulmonary Fibrosis | Without Pulmonary Fibrosis | |||||||
|---|---|---|---|---|---|---|---|---|
| DLCO corr | Distance (m) | DLCO corr | Distance (m) | |||||
| r | p | r | p | r | p | r | p | |
| D-dimers | −0.621 | 0.038 | −0.213 | 0.381 | −0.419 | 0.045 | −0.128 | 0.580 |
| LDH | −0.466 | 0.127 | −0.024 | 0.942 | −0.123 | 0.703 | −0.526 | 0.079 |
| CRP | −0.251 | 0.046 | −0.120 | 0.474 | −0.413 | 0.003 | −0.404 | 0.006 |
| Platelets | −0.108 | 0.537 | 0.095 | 0.566 | −0.184 | 0.200 | −0.037 | 0.807 |
| MPV | −0.026 | 0.882 | −0.072 | 0.663 | 0.040 | 0.783 | −0.017 | 0.911 |
| Dyspnea (Borg scale) | −0.212 | 0.228 | −0.092 | 0.598 | −0.133 | 0.378 | −0.108 | 0.478 |
| FEV1 | 0.544 | 0.001 | 0.445 | 0.006 | 0.293 | 0.043 | −0.046 | 0.769 |
| FVC | 0.623 | <0.001 | 0.387 | 0.018 | 0.353 | 0.014 | 0 | 0.997 |
| MEF50 | 0.288 | 0.094 | 0.360 | 0.029 | 0.326 | 0.025 | 0.202 | 0.193 |
| QTc | −0.339 | 0.050 | −0.152 | 0.368 | 0.074 | 0.625 | −0.283 | 0.059 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojocaru, D.-C.; Mitu, F.; Leon, M.-M.; Dima-Cozma, L.C.; Adam, C.A.; Cumpăt, C.M.; Negru, R.D.; Maștaleru, A.; Onofrei, V. Beyond the Acute Phase: Long-Term Impact of COVID-19 on Functional Capacity and Prothrombotic Risk—A Pilot Study. Medicina 2024, 60, 51. https://doi.org/10.3390/medicina60010051
Cojocaru D-C, Mitu F, Leon M-M, Dima-Cozma LC, Adam CA, Cumpăt CM, Negru RD, Maștaleru A, Onofrei V. Beyond the Acute Phase: Long-Term Impact of COVID-19 on Functional Capacity and Prothrombotic Risk—A Pilot Study. Medicina. 2024; 60(1):51. https://doi.org/10.3390/medicina60010051
Chicago/Turabian StyleCojocaru, Doina-Clementina, Florin Mitu, Maria-Magdalena Leon, Lucia Corina Dima-Cozma, Cristina Andreea Adam, Carmen Marinela Cumpăt, Robert D. Negru, Alexandra Maștaleru, and Viviana Onofrei. 2024. "Beyond the Acute Phase: Long-Term Impact of COVID-19 on Functional Capacity and Prothrombotic Risk—A Pilot Study" Medicina 60, no. 1: 51. https://doi.org/10.3390/medicina60010051