
Polymicrobial Bacterial Meningitis in a Patient with Chronic Suppurative Otitis Media: Case Report and Literature Review
 , , , and
, , , and
Abstract
:1. Introduction
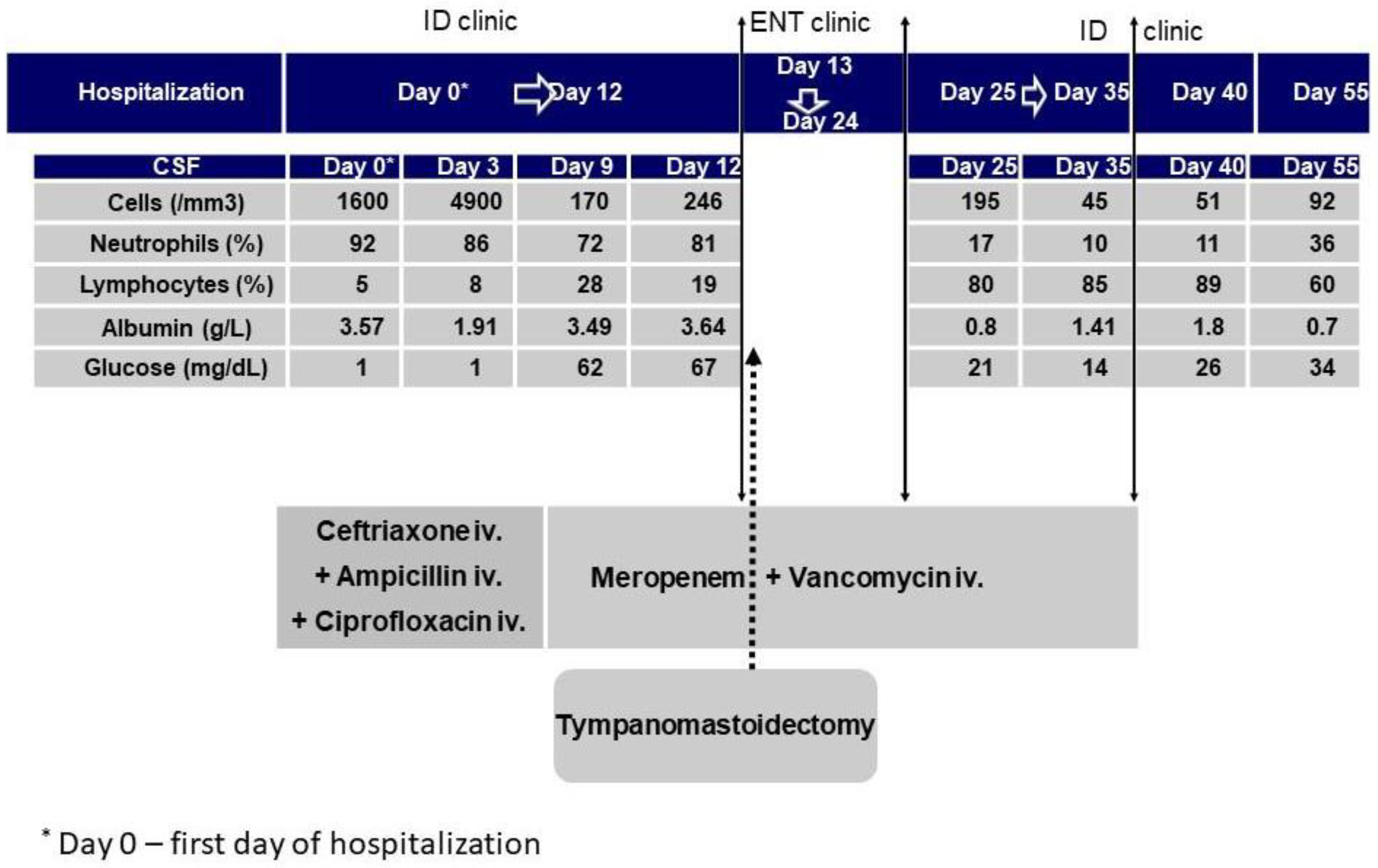
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Du, H.; Song, Z.; Wang, H.; Long, X. Polymicrobial Anaerobic Meningitis Detected by Next-Generation Sequencing: Case Report and Review of the Literature. Front. Med. 2022, 9, 840910. [Google Scholar] [CrossRef]
- Al Qahtani, H.M.; Aljoqiman, K.S.; Arabi, H.; Al Shaalan, H.; Singh, S. Fatal Meningitis in a 14-Month-Old with Currarino Triad. Case Rep. Radiol. 2016, 2016, 1346895. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, M.; Emmanuel, P.J. Expanding Molecular Diagnostics for Central Nervous System Infections. Adv. Pediatr. 2018, 65, 209–227. [Google Scholar] [CrossRef]
- Sharma, N.; Jaiswal, A.A.; Banerjee, P.K.; Garg, A.K. Complications of Chronic Suppurative Otitis Media and Their Management: A Single Institution 12 Years Experience. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-J.; Lien, C.-Y.; Chien, C.-C.; Huang, C.-R.; Tsai, N.-W.; Chang, C.-C.; Lu, C.-H.; Chang, W.-N. Anaerobic bacterial meningitis in adults. J. Clin. Neurosci. 2018, 50, 45–50. [Google Scholar] [CrossRef]
- Heintz, E.; Pettengill, M.A.; Gangat, M.A.; Hardy, D.J.; Bonnez, W.; Sobhanie, M.M. Oral flora meningoencephalitis diagnosis by next-generation DNA sequencing. Access Microbiol. 2019, 1, e000056. [Google Scholar] [CrossRef]
- Neal, T.W.; Schlieve, T. Complications of Severe Odontogenic Infections: A Review. Biology 2022, 11, 1784. [Google Scholar] [CrossRef]
- Woodhouse, A. Bacterial meningitis and brain abscess. Medicine 2021, 49, 667–674. [Google Scholar] [CrossRef]
- Wang, S.; Peng, L.; Gai, Z.; Zhang, L.; Jong, A.; Cao, H.; Huang, S.-H. Pathogenic Triad in Bacterial Meningitis: Pathogen Invasion, NF-κB Activation, and Leukocyte Transmigration that Occur at the Blood-Brain Barrier. Front. Microbiol. 2016, 7, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vata, L. Ghrelin effects on local renin angiotensin from pulmonary vessels. Acta Endocrinol. 2010, 6, 295–304. [Google Scholar] [CrossRef]
- McGill, F.; Heyderman, R.S.; Panagiotou, S.; Tunkel, A.R.; Solomon, T. Acute bacterial meningitis in adults. Lancet 2016, 388, 3036–3047. [Google Scholar] [CrossRef] [Green Version]
- Morrison, A.; Weir, I.; Silber, T. Otogenic Fusobacterium Meningitis, Sepsis, and Mastoiditis in an Adolescent. South. Med. J. 2004, 97, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Glimåker, M.; Naucler, P.; Sjölin, J. Etiology, clinical presentation, outcome and the effect of initial management in immunocompromised patients with community acquired bacterial meningitis. J. Infect. 2020, 80, 291–297. [Google Scholar] [CrossRef]
- Van de Beek, D.; Cabellos, C.; Dzupova, O.; Esposito, S.; Klein, M.; Kloek, A.T.; Leib, S.L.; Mourvillier, B.; Ostergaard, C.; Pagliano, P.; et al. ESCMID guideline: Diagnosis and treatment of acute bacterial meningitis. Clin. Microbiol. Infect. 2016, 3, S37–S62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klapa, S.; Grefer, J.; Sobottka, I.; Kurowski, V. A 56-Year-Old Woman with Chronic Hepatitis C Liver Disease and Meningitis due to Streptococcus equi subsp. Zooepidemicus. Case Rep. Crit. Care 2021, 2021, 7227054. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-Y.; Yang, F.-C.; Lee, J.-T.; Wang, C.-W. Streptococcus anginosus, tooth extraction and brain abscess. Qjm Int. J. Med. 2013, 107, 671–672. [Google Scholar] [CrossRef]
- Maritsa, S.-H.; Mouhib, N.; Tariq, C. 720: A little Streptococcus anginosus goes a long way: A strange case of meningitis. Crit. Care Med. 2019, 47, 340. [Google Scholar]
- Castillo, Y.; Delgadillo, N.A.; Neuta, Y.; Hernández, A.; Acevedo, T.; Cárdenas, E.; Montaño, A.; Lafaurie, G.I.; Castillo, D.M. Antibiotic Susceptibility and Resistance Genes in Oral Clinical Isolates of Prevotella intermedia, Prevotella nigrescens, and Prevotella melaninogenica. Antibiotics 2022, 11, 888. [Google Scholar] [CrossRef]
- Al Majid, F.; Aldrees, A.; Barry, M.; Binkhamis, K.; Allam, A.; Almohaya, A. Streptococcus anginosus group infections: Management and outcome at a tertiary care hospital. J. Infect. Public Health 2020, 13, 1749–1754. [Google Scholar] [CrossRef]
- Olender, A.; Bogut, A.; Bańska, A. The role of opportunistic “Corynebacterium” spp. in human infections. Eur. J. Clin. Exp. Med. 2019, 7, 157–161. [Google Scholar] [CrossRef]
- Zhang, M.J.; Cao, X.J.; Fan, J.; Yin, Z.G.; Yu, K. Corynebacterium striatum meningitis combined with suspected brain and lung abscesses: A case report and review. BMC Infect. Dis. 2020, 20, 389. [Google Scholar] [CrossRef]
- Dragomirescu, C.C.; Lixandru, B.E.; Coldea, I.L.; Corneli, O.N.; Pana, M.; Palade, A.M.; Cristea, V.C.; Suciu, I.; Suciu, G.; Manolescu, L.S.C.; et al. Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania. Antibiotics 2020, 9, 31. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Choi, J.Y.; Yong, D.; Lee, K.; Kim, J.M. Clinical features and prognostic factors of anaerobic infections: A 7-year ret-rospective study. Korean J. Intern. Med. 2009, 24, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Finegold, S. Host factors predisposing to anaerobic infections. FEMS Immunol. Med. Microbiol. 1993, 6, 159–163. [Google Scholar] [CrossRef]
- Siegler, D.; Faiers, M.C.; Willis, A.T. Bacteroides meningitis complicating chronic mastoiditis. Postgrad. Med. J. 1982, 58, 560–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkey, P.M.; Jewes, L.A. How common is meningitis caused by anaerobic bacteria? J. Clin. Microbiol. 1985, 22, 325. [Google Scholar] [CrossRef]
- Lien, C.-Y.; Huang, C.-R.; Tsai, W.-C.; Hsu, C.-W.; Tsai, N.-W.; Chang, C.-C.; Lu, C.-H.; Chien, C.-C.; Chang, W.-N. Epidemiologic trend of adult bacterial meningitis in southern Taiwan (2006–2015). J. Clin. Neurosci. 2017, 42, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Shah, H.N.; Collins, D.M. Prevotella, a New Genus to Include Bacteroides Melaninogenicus and Related Species Formerly Classified in the Genus Bacteroides. Int. J. Syst. Bacteriol. 1990, 40, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Bancescu, G.; Didilescu, A.; Bancescu, A.; Bari, M. Antibiotic susceptibility of 33 Prevotella strains isolated from Romanian patients with abscesses in head and neck spaces. Anaerobe 2015, 35 Pt A, 41–44. [Google Scholar] [CrossRef]
- Brook, I. Prevotella intermedia meningitis associated with cerebrospinal fluid leakage in an adolescent. Pediatr. Infect. Dis. J. 2003, 22, 751–753. [Google Scholar] [CrossRef]
- Könönen, E.; Fteita, D.; Gursoy, U.K.; Gursoy, M. Prevotella species as oral residents and infectious agents with potential impact on systemic conditions. J. Oral Microbiol. 2022, 14, 2079814. [Google Scholar] [CrossRef] [PubMed]
- Kalay, G.; Dalgic, N.; Bozan, T.; Toprak, N.U.; Bayraktar, B.; Soyletir, G. Polymicrobial anaerobic meningitis caused by Bacteroides fragilis, Bacteroides thetaiotaomicron, Fusobacterium necrophorum and Slackia exigua in a patient with mastoiditis following otitis media. Anaerobe 2019, 56, 95–97. [Google Scholar] [CrossRef]
- Pittman, M.E.; Thomas, B.S.; Wallace, M.A.; Weber, C.J.; Burnham, C.-A.D. Routine Testing for Anaerobic Bacteria in Cerebrospinal Fluid Cultures Improves Recovery of Clinically Significant Pathogens. J. Clin. Microbiol. 2014, 52, 1824–1829. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Hirata, M.; Hossain, D.N.; Kunz, A. Prevotella melaninogenica Meningitis and Abscess: Normal Flora in an Abnormal Location. Pediatrics 2018, 142, 602. [Google Scholar] [CrossRef]
- Mittal, M.K.; Zimmerman, R.A. Meningitis and Epidural Abscess Related to Pansinusitis. Pediatr. Emerg. Care 2009, 25, 267–268. [Google Scholar] [CrossRef]
- Luca, C.; Mihalache, D.; Luca, V.; Turcu, T. The clinical picture, treatment and prognosis of meningitis due to anaerobic and nonfermentative bacteria. Rev. Med. Chir. Soc. Med. Nat. Iasi 1999, 103, 158–160. [Google Scholar] [PubMed]
- Miftode, E.; Vâţă, A.; Leca, D.; Hurmuzache, M.; Dorneanu, O.; Manciuc, C.; Luca, V.; Dorobăţ, C. Community acquired acute bacterial meningitis—A 10 years review. Rev. Med. Chir. Soc. Med. Nat. Iasi 2009, 113, 402–409. [Google Scholar] [PubMed]
- Mo, S.; Wei, L.; Chen, H.; Li, R.; Li, S.; Luo, G. A chinese case of prevotella intermedia and streptococcus constellatus intracranial mixed infection. Metab. Brain Dis. 2018, 33, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Llitjos, J.-F.; Mongardon, N.; Loubinoux, J.; Sonneville, R.; Charpentier, J.; Pène, F.; Mira, J.-P. Polymicrobial anaerobic meningitis. Med. Mal. Infect. 2016, 46, 230–232. [Google Scholar] [CrossRef]
- Ganeshalingham, A.; Buckley, D.; Shaw, I.; Freeman, J.T.; Wilson, F.; Best, E. Bacteroides fragilis concealed in an infant with Escherichia coli meningitis. J. Paediatr. Child. Health 2014, 50, 78–80. [Google Scholar] [CrossRef]
- Luo, L.; Wang, C.; Shen, N.; Zhao, R.; Tao, Y.; Mo, X.; Cao, Q. Polymicrobial anaerobic bacterial meningitis secondary to dermal sinus: A case report. Transl. Pediatr. 2021, 10, 3118–3123. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, E.; Roux, A.; Demers, J.; Vanier, L.E.; Moore, L. A 40-Year-Old Woman with Cauda Equina Syndrome Caused by Rectothecal Fistula Arising from an Anterior Sacral Meningocele. Neurosurgery 2010, 67, E1464–E1467. [Google Scholar] [CrossRef] [PubMed]
- Guerin, J.; Leibinger, F.; Raskine, L.; Ekherian, J. Polymicrobial meningitis revealing an anterior sacral meningocele in a 23-year-old woman. J. Infect. 2000, 40, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Jeltema, H.-R.; Broens, P.M.A.; Brouwer, O.F.; Groen, R.J.M. Severe bacterial meningitis due to an enterothecal fistula in a 6-year-old child with Currarino syndrome: Evaluation of surgical strategy with review of the literature. Child’s Nerv. Syst. 2019, 35, 1129–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, C.; Sacks, B.; Jao, J. Polymicrobial feculent meningitis. Clin. Infect. Dis. 1995, 21, 693–694. [Google Scholar] [CrossRef] [PubMed]
- García-Lechuz, J.M.; Hernangómez, S.; San Juan, R.; Bouza, E. Feculent meningitis: Polymicrobial meningitis in colorectal surgery. Diagn. Microbiol. Infect. Dis. 2000, 38, 169–170. [Google Scholar] [CrossRef]
- Walsh, T.J.; Weinstein, R.A.; Malinoff, H.; Breyer, M.D.; Berelowitz, B.A. Meningorectal fistula as a cause of polymicrobial anaerobic meningitis. Am. J. Clin. Pathol. 1982, 78, 127–130. [Google Scholar] [CrossRef]
- Thyss, J.; Chabert, J.M.; Bocquet, J.P.; Gazaix, M.; Korn, M.; Carles, D.; Etesse, H. Méningite post-opératoire plurimicrobienne à germes aérobies et anaérobies traitée par l’ornidazole. Nouv. Press. Med. 1980, 9, 381. [Google Scholar]
- Schartz, D.A.; Polacco, M.A.; Holmgren, E.P.; McCool, R.R. A Rare Case of Odontogenic Chronic Suppurative Otitis Media. Cureus 2019, 11, e4284. [Google Scholar] [CrossRef] [Green Version]
- Niemelä, S.; Lempinen, L.; Löyttyniemi, E.; Oksi, J.; Jero, J. Bacterial meningitis in adults: A retrospective study among 148 patients in an 8-year period in a university hospital, Finland. BMC Infect. Dis. 2023, 23, 45. [Google Scholar] [CrossRef]
- Cheng, H.; Xu, L.; Yang, F.; Jia, L.; Zhao, D.; Li, H.; Liu, W.; Li, Y.; Liu, X.; Geng, X.; et al. Case report: Meningitis and intracranial aneurysm caused by mixed infection of oral microflora dominated by anaerobes. Front. Neurol. 2022, 13, 889838. [Google Scholar] [CrossRef]
- Anderson, A.C.; von Ohle, C.; Frese, C.; Boutin, S.; Bridson, C.; Schoilew, K.; Peikert, S.A.; Hellwig, E.; Pelz, K.; Wittmer, A.; et al. The oral microbiota is a reservoir for antimicrobial resistance: Resistome and phenotypic resistance characteristics of oral biofilm in health, caries, and periodontitis. Ann. Clin. Microbiol. Antimicrob. 2023, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Barie, P.S.; Narayan, M.; Jose, V.M.A.; Shapiro, M.J. Antibiotic Use in the Intensive Care Unit: The Old and the New. In Current Therapy of Trauma and Surgical Critical Care; Elsevier: Amsterdam, The Netherlands, 2023; pp. 803–814.e1. [Google Scholar]
- Rubinstein, E.; Keynan, Y. Vancomycin Revisited—60 Years Later. Front. Public Health 2014, 2, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunkel, A.R.; Hasbun, R.; Bhimraj, A.; Byers, K.; Kaplan, S.L.; Scheld, W.M.; van de Beek, D.; Bleck, T.P.; Garton, H.J.L.; Zunt, J.R. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin. Infect. Dis. 2017, 64, e34–e65. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Sample | Bacteria | Susceptibility | |
|---|---|---|---|
| Sensible | Resistant | ||
| CSF | Streptococcus anginosus group | PEN, CRO, CTX, MXF, TEC, VA | - |
| Corynebacterium spp. | PEN, CLI, RIF, VA, LIN | - | |
| Prevotella spp. | AMX, AMC, TIC, TPZ, IPM, CLI, MXF, RIF | PEN, MTR | |
| Ear drainage | Proteus mirabilis | AMP, AMC, AMS, SXT, CTX, CAZ, GEN | - |
| Enterococcus faecalis | AMP i.v | - | |
| Author | Gender/Age | Comorbidities | Microorganisms | Treatment | Evolution |
|---|---|---|---|---|---|
| Li et al., 2022 [1] | F/16 years | Sinusitis | CSF: Porphyromonas gingivalis, Prevotella enoeca, Campylobacter rectus, Fusobacterium uncleatum, Actinomyces israelii | Ceftriaxone/ Vancomycin/ Metronidazole | Favorable |
| Kalay et al., 2019 [32] | M/16 years | Mastoiditis | CSF: Bacteroides fragilis, Bacteroides thetaiotaomicron, Fusobacterium necrophorum, Slackia exigua | Metronidazole/ Meropenem | Favorable |
| Mo et al., 2018 [38] | M/48 years | Cerebral infarction Possible sinusitis | CSF: Prevotella intermedia and Streptococcus constellatus | Ceftriaxone | Unknown |
| Mittal et al., 2009 [35] | F/11 years | Pansinusitis Epidural abscess | CSF: negative culture Sinus fluid cultures: Staphylococcus aureus, alpha hemolytic streptococci, Eikenella spp.; Prevotella intermedia, Fusobacterium spp, Peptostreptococcus anaerobius. | Cefotaxime + vancomycin/ ceftriaxone + metroniddazole + surgery | Favorable |
| Llitjos et al., 2017 [39] | F/69 years | None relevant | CSF: Peptostreptococcus micros, Fusobacterium necrophorum, Porphyromonas gingivalis, Campylobacter rectus | High-dose amoxicillin/ metronidazole | Death on day 47 |
| Ganeshalingham et al., 2014 [40] | M/8-week | None | CSF: E. coli, Bacteroides fragilis | Ceftriaxone/ Amoxicillin | Death |
| Luo et al., 2021 [41] | M/9-month | Lumbar dermal sinus | CSF: Finegoldia magna, Campylobacter ureolyticus, Bacteroides fragilis, Porphyromonas bennonis | Vancomycin/ ceftriaxone/ meropenem/ metronidazole | Favorable |
| Bergeron et al., 1980 [42] | F /40 years | Anterior sacral meningocele | CSF: Escherichia coli, group F streptococci, Bacteroides fragilis, Peptostreptococcus anaerobius, Candida glabrata | Ceftazidime/ metronidazole + surgery | Favorable |
| Guerin et al., 2000 [43] | F/23 years | Anterior sacral meningocele | CSF: Enterococcus faecalis, Streptococcus constelatus, Prevotella bivia | Vancomycin/ metronidazole/ cefotaxime/ piperacillin/tazobactam | |
| Jeltema et al., 2019 [44] | F/6 years | Currarino syndrome | CSF: Streptococcus anginosus (milleri), Bacteroides fragilis. | Broad-spectrum antibiotics + surgery | |
| Chun et al., 1995 [45] | M/56 years | Colon cancer | Non—perfringens Clostridium spp., Peptostreptococcus spp., Veillonela spp. | Penicillin G/ ceftriaxone/ metronidazole | Favorable |
| García-Lechuz et al, 2000 [46] | M/68 years | Rectal cancer | Bacteroides fragilis, MRSA, Morganella morgagnii | Vancomycin/ meropenem | |
| Walsh et al., 1982 [47] | F/49 years | Rectal cancer | Bacteroides fragilis, Bacteroides thetaiotaomicron, Bacteroides melaninogenicus, Clostridium ramosum, C. clostridiforme, Peptostreptococcus anaerobius | Ampicillin/ penicillin/ chloramphenicole/ metronidazole | Death after 5 months |
| Thyss et al., 1980 [48] | F/67 years | Not known | Streptococcus mitior, Bacteroides fragilis, Eubacterium lentum | Ornidazole | Favorable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vâţă, A.; Irimie-Băluţă, E.; Roşu, F.M.; Onofrei, I.M.; Loghin, I.I.; Perţea, M.; Avădanei, A.N.; Miron, M.; Rădulescu, L.; Eşanu, I.; et al. Polymicrobial Bacterial Meningitis in a Patient with Chronic Suppurative Otitis Media: Case Report and Literature Review. Medicina 2023, 59, 1428. https://doi.org/10.3390/medicina59081428
Vâţă A, Irimie-Băluţă E, Roşu FM, Onofrei IM, Loghin II, Perţea M, Avădanei AN, Miron M, Rădulescu L, Eşanu I, et al. Polymicrobial Bacterial Meningitis in a Patient with Chronic Suppurative Otitis Media: Case Report and Literature Review. Medicina. 2023; 59(8):1428. https://doi.org/10.3390/medicina59081428
Chicago/Turabian StyleVâţă, Andrei, Erika Irimie-Băluţă, Florin Manuel Roşu, Ioana Maria Onofrei, Isabela Ioana Loghin, Mihaela Perţea, Andrei Nicolae Avădanei, Mihnea Miron, Luminiţa Rădulescu, Irina Eşanu, and et al. 2023. "Polymicrobial Bacterial Meningitis in a Patient with Chronic Suppurative Otitis Media: Case Report and Literature Review" Medicina 59, no. 8: 1428. https://doi.org/10.3390/medicina59081428