
Chronic Otitis Media in Patients with Chronic Rhinosinusitis: A Systematic Review


 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Electronic Database Search
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
3. Results
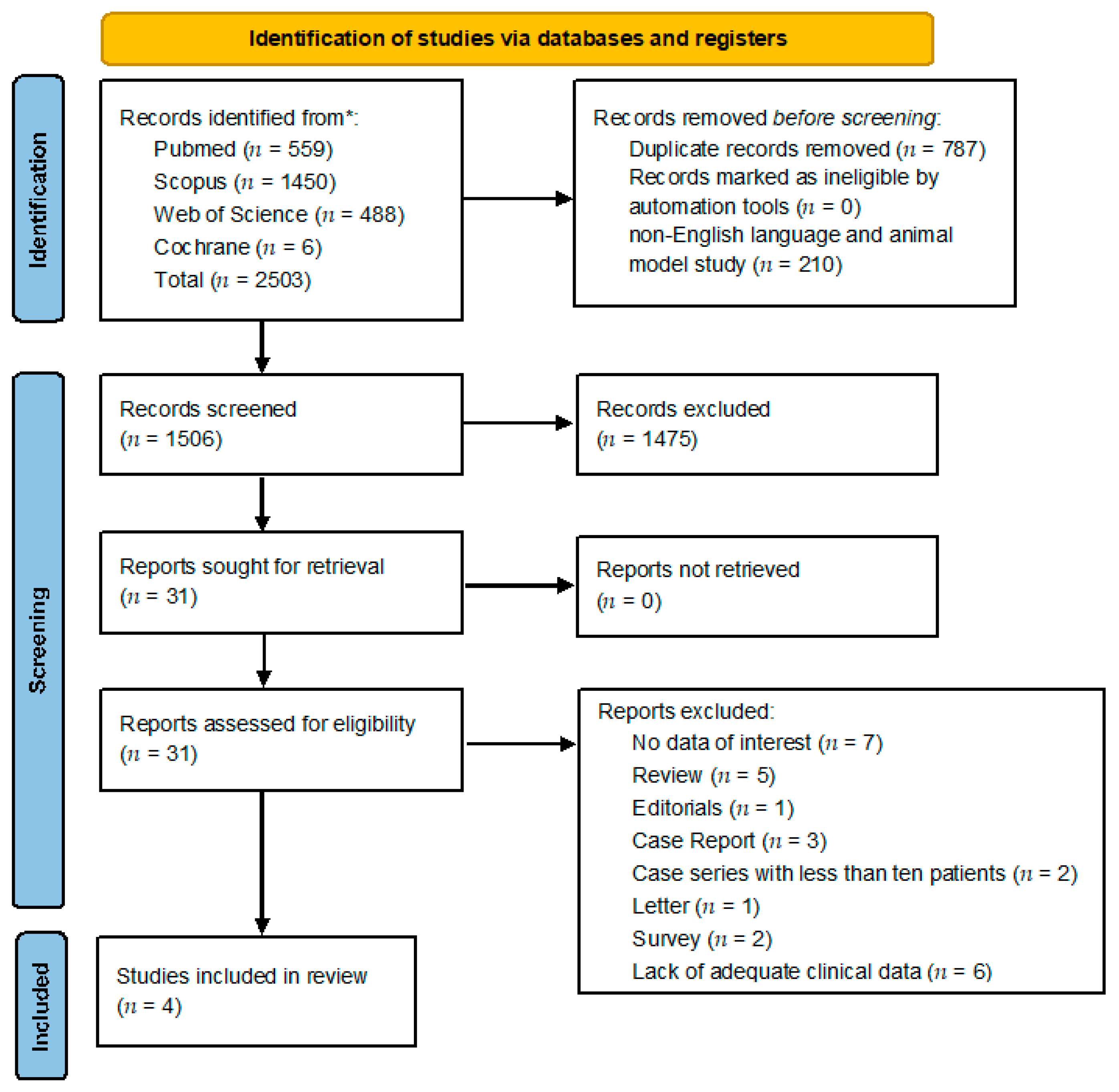
3.1. Retrieving Investigations
3.2. Quality Assessment
3.3. Qualitative Synthesis
3.3.1. Epidemiological Characteristics
3.3.2. Clinical Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brescia, G.; Zanotti, C.; Parrino, D.; Barion, U.; Marioni, G. Nasal polyposis pathophysiology: Endotype and phenotype open issues. Am. J. Otolaryngol. 2018, 39, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Marioni, G. Structured histopathology for endotyping and planning rational treatment in chronic rhinosinusitis. Am. J. Otolaryngol. 2021, 42, 102795. [Google Scholar] [CrossRef] [PubMed]
- Aarhus, L.; Tambs, K.; Kvestad, E.; Engdahl, B. Childhood otitis media: A cohort study with 30-year follow-up of hearing (the HUNT Study). Ear Hear. 2015, 36, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amali, A.; Hosseinzadeh, N.; Samadi, S.; Nasiri, S.; Zebardast, J. Sensorineural hearing loss in patients with chronic suppurative otitis media: Is there a significant correlation? Electron. Physician 2017, 9, 3823–3827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elzinga, H.B.E.; van Oorschot, H.D.; Stegeman, I.; Smit, A.L. Relation between otitis media and sensorineural hearing loss: A systematic review. BMJ Open 2021, 11, e050108. [Google Scholar] [CrossRef]
- Chung, J.H.; Lee, S.H.; Woo, S.Y.; Kim, S.W.; Cho, Y.S. Prevalence and associated factors of chronic suppurative otitis media: Data from the Korea National Health and Nutrition Examination Survey, 2009–2012: Chronic Otitis Media. Laryngoscope 2016, 126, 2351–2357. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Lisi, C.V.; Gerring, R.; Mittal, J.; Mathee, K.; Narasimhan, G.; Azad, R.K.; Yao, Q.; Grati, M.; Yan, D.; et al. Current concepts in the pathogenesis and treatment of chronic suppurative otitis media. J. Med. Microbiol. 2015, 64, 1103–1116. [Google Scholar] [CrossRef] [PubMed]
- Acuin, J. Chronic suppurative otitis media. BMJ Clin. Evid. 2007, 2007, 0507. [Google Scholar] [PubMed]
- Marchisio, P.; Ghisalberti, E.; Fusi, M.; Baggi, E.; Ragazzi, M.; Dusi, E. Paranasal sinuses and middle ear infections: What do they have in common? Pediatr. Allergy Immunol. 2007, 18, 31–34. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, M.W.; Min, C.; Park, I.S.; Park, B.; Byun, S.H.; Choi, H.G.; Hong, S.J. Increased risk of chronic otitis media in chronic rhinosinusitis patients: A longitudinal follow-up study using a national health screening cohort. Rhinology 2021, 59, 292. [Google Scholar] [CrossRef]
- Damar, M.; Dinc, A.E.; Erdem, D.; Biskin, S.; Elicora, S.S.; Kumbul, Y. The role of the nasal and paranasal sinus pathologies on the development of chronic otitis media and its subtypes: A computed tomography Study. Niger. J. Clin. Pract. 2017, 20, 1156–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, C.D.; Kim, J.S.; Lee, E.J. Association of gastroesophageal reflux disease with increased risk of chronic otitis media with effusion in adults: A nationwide population-based cohort study. Medicine 2021, 100, e26940. [Google Scholar] [CrossRef]
- Lechien, J.R.; Debie, G.; Mahillon, V.; Thill, M.P.; Rodriguez, A.; Horoi, M.; Kampouridis, S.; Muls, V.; Saussez, S. A 10-year follow-up of a randomized prospective study of 2 treatments for chronic rhinosinusitis without nasal polyps and investigation of the impact of gastroeosophageal reflux disease in the resistance to treatment. Ear Nose Throat J. 2021, 100, 569S–577S. [Google Scholar] [CrossRef] [Green Version]
- Songu, M.; Islek, A.; Imre, A.; Aslan, H.; Aladag, I.; Pinar, E.; Oncel, S. Risk factors for otitis media with effusion in children with adenoid hypertrophy. Acta Otorhinolaryngol. Ital. 2020, 40, 133–137. [Google Scholar] [CrossRef]
- Ciprandi, G.; Torretta, S.; Marseglia, G.L.; Licari, A.; Chiappini, E.; Benazzo, M.; Tosca, M.A.; Marchisio, P. Allergy and Otitis Media in Clinical Practice. Curr. Allergy Asthma Rep. 2020, 20, 33. [Google Scholar] [CrossRef]
- Bemanian, M.H.; Rezaei, K.; Atighechi, S.; Shafiei, A. The Relation of Allergy to Adenoid Hypertrophy and Otitis Media with Effusion: A Cross-sectional Study. Iran. J. Allergy Asthma Immunol. 2020, 19, 529–533. [Google Scholar] [CrossRef]
- Malagutti, N.; Rotondo, J.C.; Cerritelli, L.; Melchiorri, C.; De Mattei, M.; Selvatici, R.; Oton-Gonzalez, L.; Stomeo, F.; Mazzoli, M.; Borin, M.; et al. High Human Papillomavirus DNA loads in Inflammatory Middle Ear Diseases. Pathogens 2020, 9, 224. [Google Scholar] [CrossRef] [Green Version]
- Lam, K.; Schleimer, R.; Kern, R.C. The Etiology and Pathogenesis of Chronic Rhinosinusitis: A Review of Current Hypotheses. Curr. Allergy Asthma Rep. 2015, 15, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 October 2022).
- Maradesha, P.S.; Samatha, K.J.; Veenapani, M.K. An analysis between chronic suppurative otitis media and chronic bacterial rhinosinusitis. J. Evol. Med. Dent. Sci. JEMDS 2016, 5, 4764–4768. [Google Scholar] [CrossRef]
- Kuo, C.L.; Yen, Y.C.; Chang, W.P.; Shiao, A.S. Association between middle ear cholesteatoma and chronic rhinosinusitis. JAMA Otolaryngol.-Head Neck Surg. 2017, 143, 757–763. [Google Scholar] [CrossRef]
- Daval, M.; Picard, H.; Bequignon, E.; Bedbeder, P.; Coste, A.; Ayache, D.; Escabasse, V. Chronic otitis media with effusion in chronic sinusitis with polyps. ENT-Ear Nose Throat J. 2018, 97, E13–E18. [Google Scholar] [CrossRef] [Green Version]
- Lund, V.J.; Kennedy, D.W. Staging for rhinosinusitis. Otolaryngol. Neck. Surg. 1997, 117, S35–S40. [Google Scholar] [CrossRef]
- Hong, S.N.; Lee, W.H.; Lee, S.H.; Rhee, C.S.; Lee, C.H.; Kim, J.W. Chronic rhinosinusitis with nasal polyps is associated with chronic otitis media in the elderly. Eur. Arch. Otorhinolaryngol. 2017, 274, 1463–1470. [Google Scholar] [CrossRef]
- Finkelstein, Y.; Talmi, Y.P.; Rubel, Y.; Bar-Ziv, J.; Zohar, Y. Otitis media with effusion as a presenting symptom of chronic sinusitis. J. Laryngol. Otol. 1989, 103, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.P.; Irani, B.S.; Vaughan-Jones, R.J.; Padgham, N.D. Maxillary sinusitis in children with otitis media with effusion. J. Laryngol. Otol. 1994, 108, 842–844. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.K.; Park, D.C.; Kim, S.W.; Cha, C.I.; Cha, S.H.; Yeo, S.G. Effect of paranasal sinusitis on the development of otitis media with effusion: Influence of Eustachian tube function and adenoid immunity. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1609–1618. [Google Scholar] [CrossRef]
- Kim, C.S.; Jung, H.W.; Yoo, K.Y. Prevalence and risk factors of chronic otitis media in Korea: Results of a nation-wide survey. Acta Otolaryngol. 1993, 113, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz-Demirdag, Y. Should newborns be screened for immunodeficiency? Lessons learned from infants with recurrent otitis media. Curr. Allergy Asthma Rep. 2011, 11, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Prasad, H.K.; Bhojwani, K.M.; Shenoy, V.; Prasad, S.C. HIV manifestations in otolaryngology. Am. J. Otolaryngol. 2006, 27, 179–185. [Google Scholar] [CrossRef]
- Brook, I.; Yocum, P.; Shah, K. Aerobic and anaerobic bacteriology of concurrent chronic otitis media with effusion and chronic sinusitis in children. Arch. Otolaryngol. Neck Surg. 2000, 126, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Post, J.C.; Hiller, N.L.; Nistico, L.; Stoodley, P.; Ehrlich, G.D. The role of biofilms in otolaryngologic infections: Update 2007. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 347–351. [Google Scholar] [CrossRef]
- Jaiswal, A.S.; Tanwar, P.; Irugu, D.V.K.; Sikka, K.; Monga, R.; Thakar, A.; Verma, H. Human papilloma virus in the etiopathogenesis of allergic nasal polyposis: A prospective study. Am. J. Otolaryngol. 2022, 43, 103273. [Google Scholar] [CrossRef] [PubMed]
- Kagoshima, H.; Hori, R.; Kojima, T.; Okanoue, Y.; Taguchi, A.; Yamamoto, H.; Hasebe, K.; Shoji, K. Successful treatment of eosinophilic chronic rhinosinusitis and eosinophilic otitis media using the anti-IL-5 receptor monoclonal antibody benralizumab: A case report. Respir. Med. Case Rep. 2020, 30, 101135. [Google Scholar] [CrossRef] [PubMed]
- Fermo, S.; Frosolini, A.; Parrino, D.; Chiappetta, A.; Marioni, G.; de Filippis, C. Eustachian tube insufflation with thermal water: Effectiveness in the treatment of pediatric otitis media with effusion. Am. J. Otolaryngol. 2022, 43, 103504. [Google Scholar] [CrossRef] [PubMed]
- Franz, L.; Manica, P.; Claudatus, J.; Frigo, A.C.; Marioni, G.; Staffieri, A. Sulfurous-arsenical-ferruginous thermal water nasal inhalation and irrigation in children with recurrent upper respiratory tract infections: Clinical outcomes and predictive factors. Am. J. Otolaryngol. 2021, 42, 103083. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Frasconi, S.; Contro, G.; Frigo, A.C.; Marioni, G. Structured histopathology and laboratory evidence in nasal polyposis with different pathogenesis. Am. J. Otolaryngol. 2023, 44, 103649. [Google Scholar] [CrossRef]
- Brescia, G.; Alessandrini, L.; Giacomelli, L.; Parrino, D.; Zanotti, C.; Tealdo, G.; Franz, L.; Carraro, V.; Barion, U.; Marioni, G. A classification of chronic rhinosinusitis with nasal polyps based on structured histopathology. Histopathology 2020, 76, 296–307. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country | Study Type | Number of Total Patients Analyzed | Gender (M/F) No. Cases | Age | Healthy Control Group | CRS Case Group | CRS Patients Who Develop COM | Quality [14] |
|---|---|---|---|---|---|---|---|---|---|---|
| Maradesha et al. [21] | 2016 | India | Retrospective observational study | 60 | 41/19 | Mean 33 ± 11 yrs (range 18–60 yrs) | NR | 60 | 60 | Fair |
| Kuo et al. [22] | 2017 | Taiwan | Longitudinal prospective cohorts’ study | 76,020 | 6800/5870 | Mean 27.57 ± 22.03 yrs | 63,350 | 12,670 | 66 | Good |
| Daval et al. [23] | 2018 | France | Cross-sectional study | 80 | 42/38 | Mean 48 yrs (range 15–76 yrs) | NR | 80 | 20 | Poor |
| Kim et al. [10] | 2021 | Korea | Retrospective Cohort Study | 40,285 | 4908/3149 | 40–44 yrs (747 cases) 45–49 yrs (1498 cases) 50–54 yrs (1653 cases) 55–59 yrs (1557 cases) 60–64 yrs (1180 cases) 65–69 yrs (783 cases) 70–74 yrs (425 cases) 75–79 yrs (164 cases) 80–84 yrs (43 cases) 85 + yrs (7 cases) | 32,228 | 8057 | 845 | Poor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescia, G.; Frosolini, A.; Franz, L.; Daloiso, A.; Fantin, F.; Lovato, A.; Filippis, C.d.; Marioni, G. Chronic Otitis Media in Patients with Chronic Rhinosinusitis: A Systematic Review. Medicina 2023, 59, 123. https://doi.org/10.3390/medicina59010123
Brescia G, Frosolini A, Franz L, Daloiso A, Fantin F, Lovato A, Filippis Cd, Marioni G. Chronic Otitis Media in Patients with Chronic Rhinosinusitis: A Systematic Review. Medicina. 2023; 59(1):123. https://doi.org/10.3390/medicina59010123
Chicago/Turabian StyleBrescia, Giuseppe, Andrea Frosolini, Leonardo Franz, Antonio Daloiso, Francesco Fantin, Andrea Lovato, Cosimo de Filippis, and Gino Marioni. 2023. "Chronic Otitis Media in Patients with Chronic Rhinosinusitis: A Systematic Review" Medicina 59, no. 1: 123. https://doi.org/10.3390/medicina59010123