
The Very First Romanian Unruptured 13-Weeks Gestation Tubal Ectopic Pregnancy
 , , and
, , and 
Abstract
:1. Introduction
2. Case Presentation
2.1. Patient Information
2.2. Clinical History
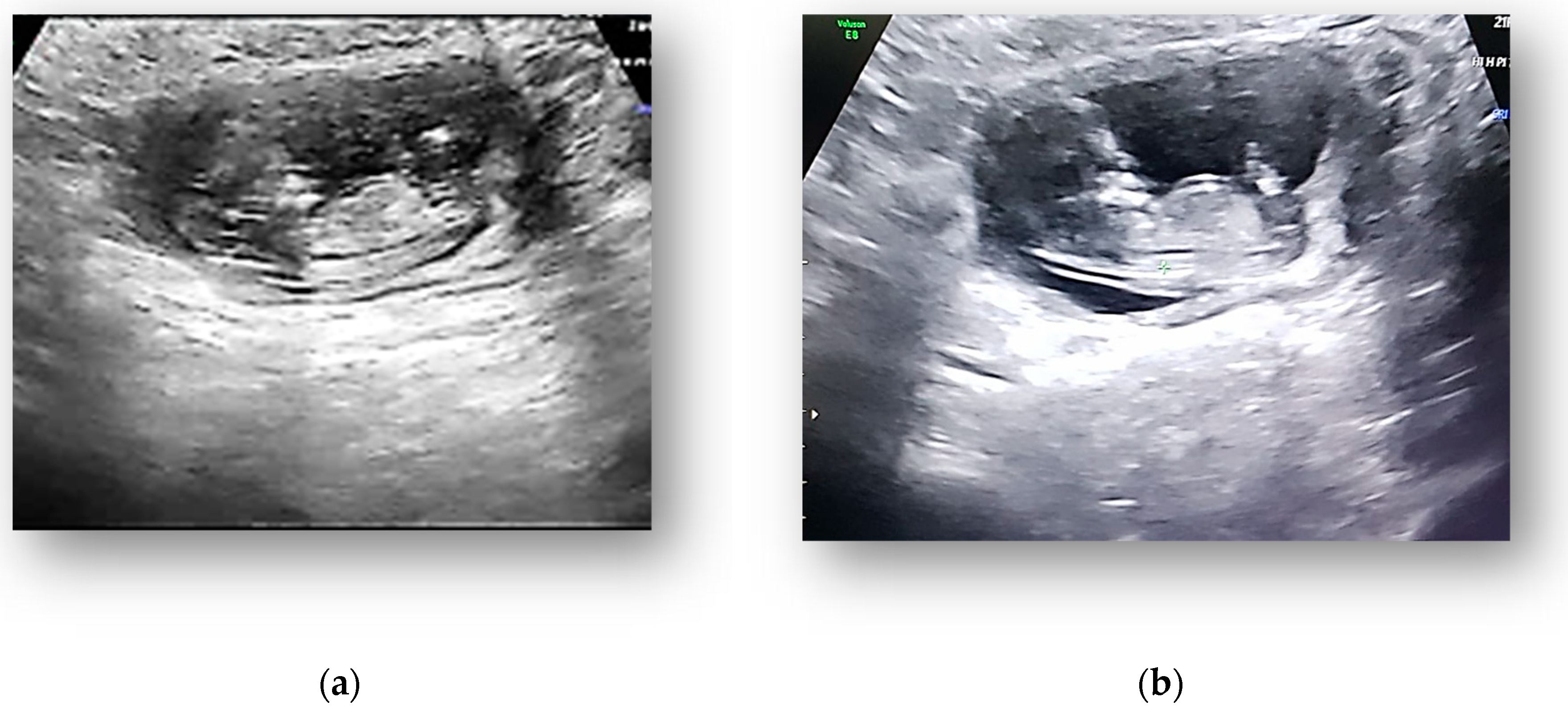
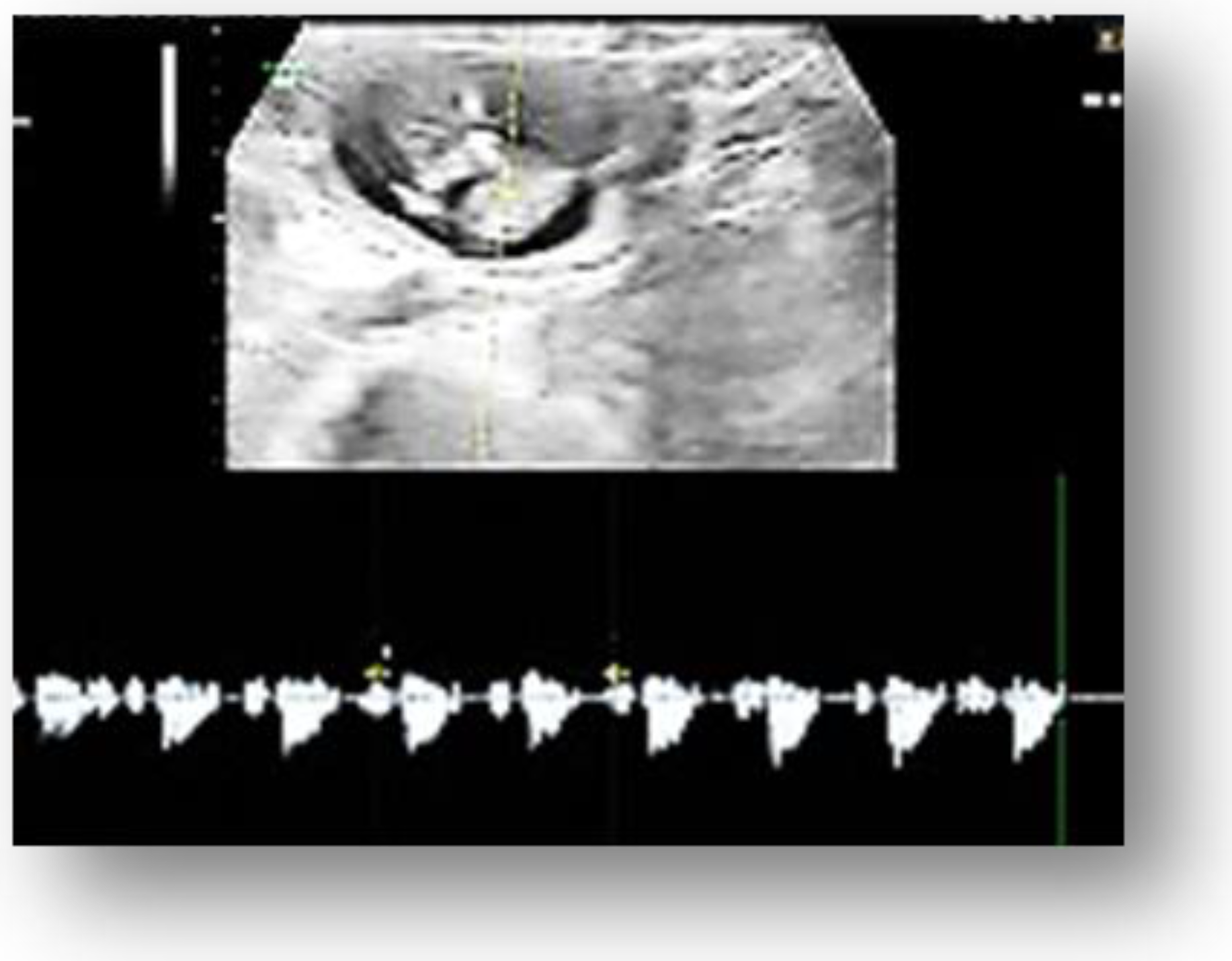
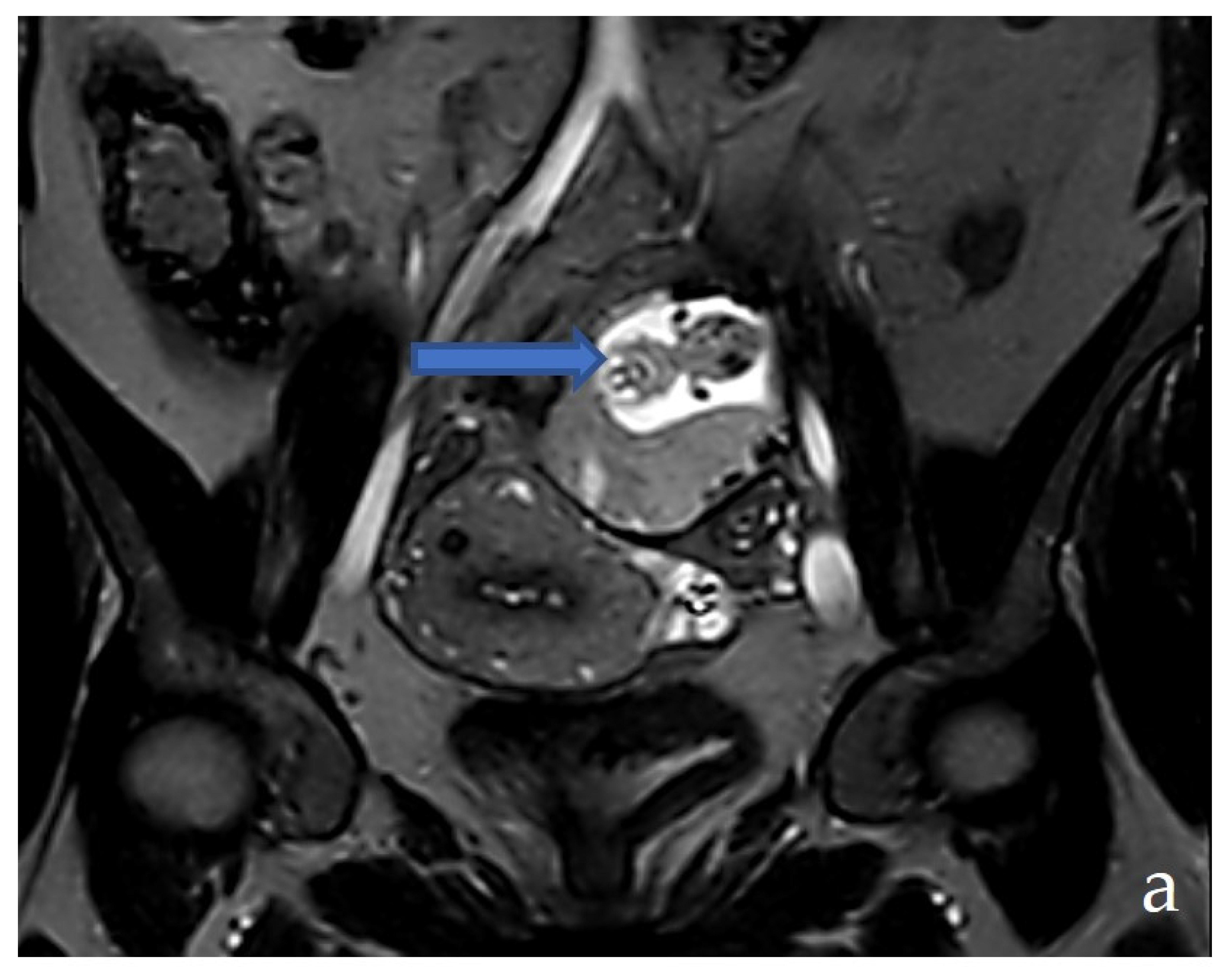
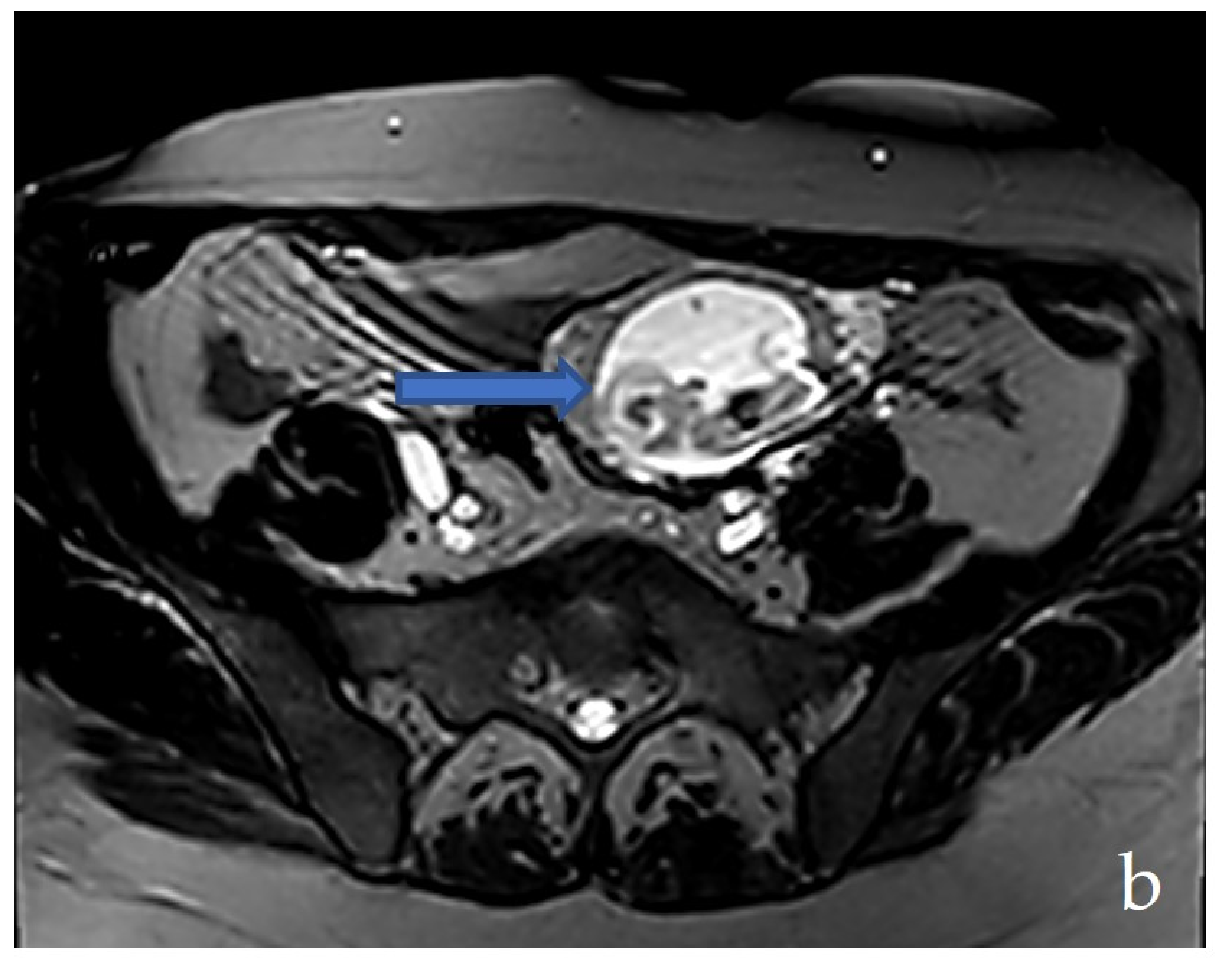
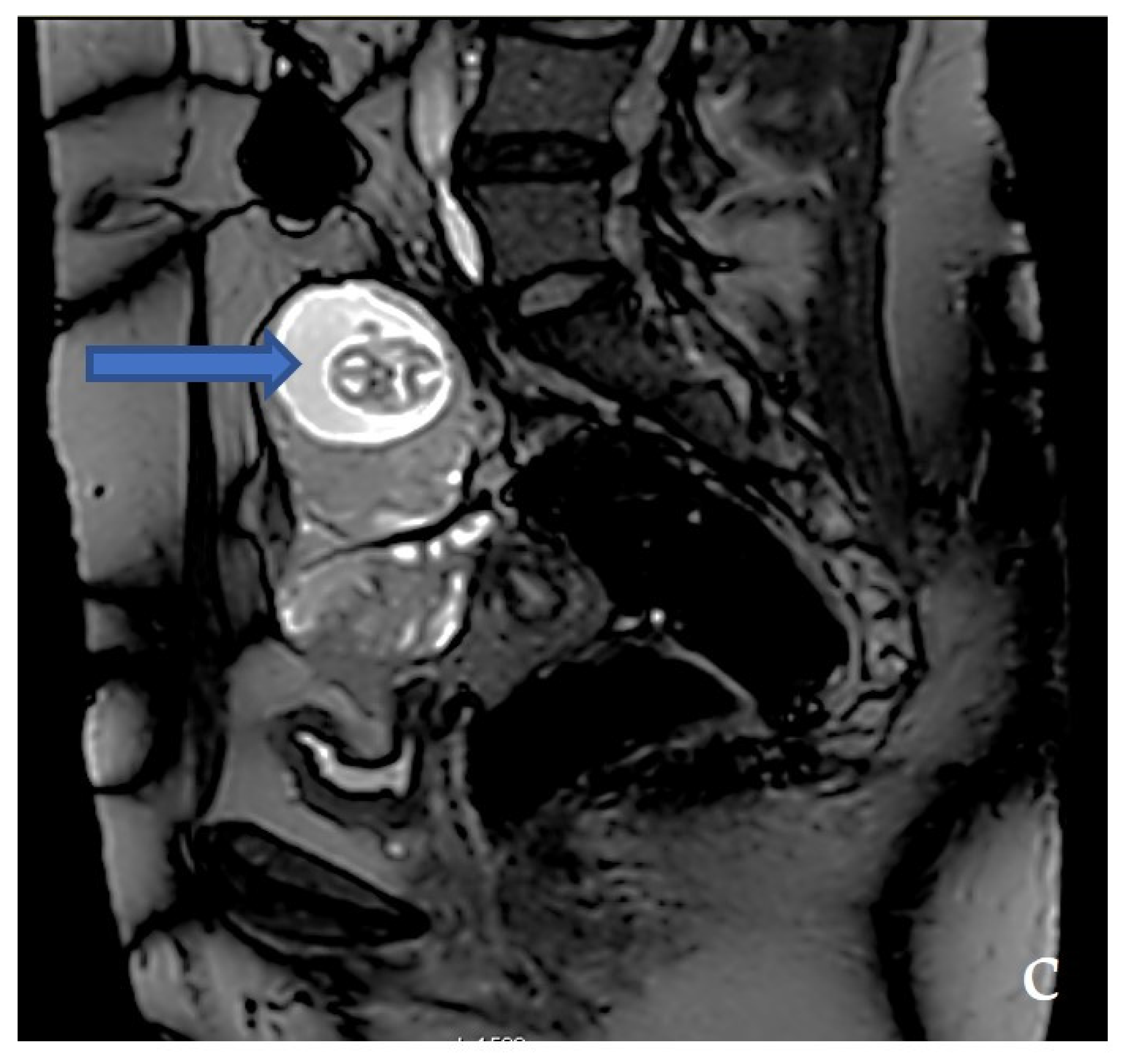
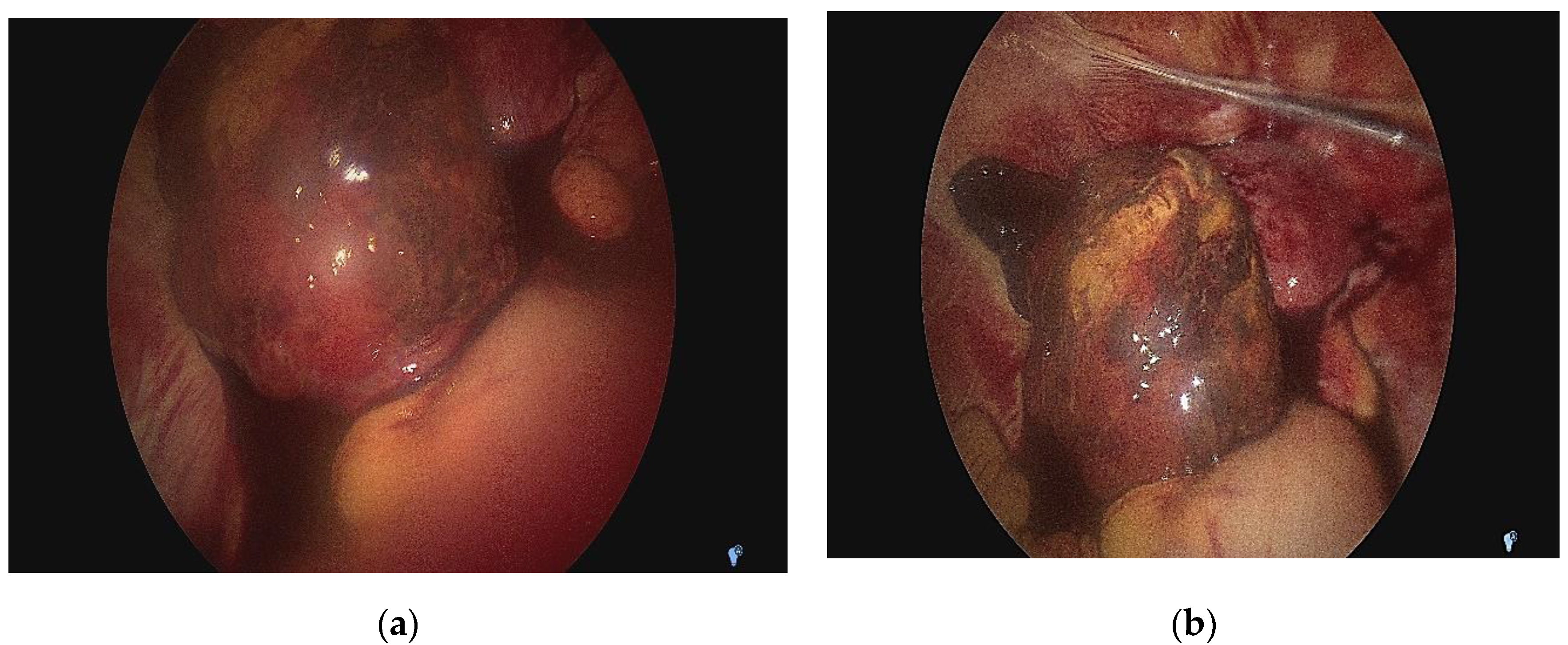
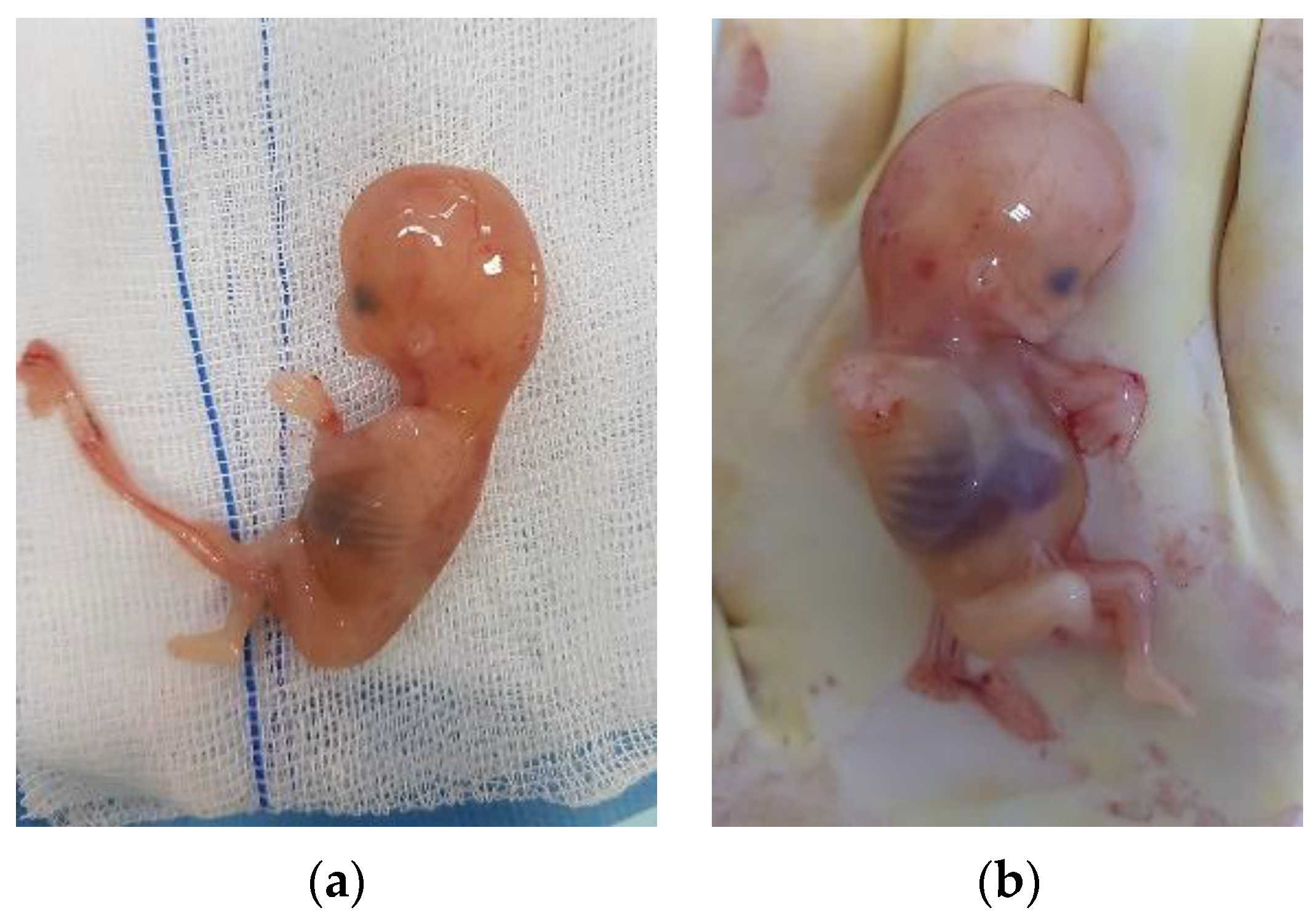
2.3. Diagnostic Assessment and Investigations
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taran, F.-A.; Kagan, K.-O.; Hübner, M.; Hoopmann, M.; Wallwiener, D.; Brucker, S. The Diagnosis and Treatment of Ectopic Pregnancy. Dtsch. Arztebl. Int. 2015, 112, 693–704. [Google Scholar] [CrossRef]
- Mhaskar, R.; Harish, M.; Jaiprakash, T. Unruptured Ampullary Ectopic Pregnancy at 16-week Period of Gestation with Live Fetus. J. Obstet. Gynaecol. India 2014, 64, 73–74. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 191: Tubal Ectopic Pregnancy. Obstet. Gynecol. 2018, 131, e65–e77. [Google Scholar] [CrossRef] [PubMed]
- Panelli, D.M.; Phillips, C.H.; Brady, P.C. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: A review. Fertil. Res. Pract. 2015, 1, 15. [Google Scholar] [CrossRef] [PubMed]
- Bouyer, J.; Coste, J.; Fernandez, H.; Pouly, J.L.; Job-Spira, N. Sites of ectopic pregnancy: A 10 year population-based study of 1800 cases. Hum. Reprod. 2002, 17, 3224–3230. [Google Scholar] [CrossRef]
- Murray, H.; Baakdah, H.; Bardell, T.; Tulandi, T. Diagnosis and treatment of ectopic pregnancy. Can. Med. Assoc. J. 2005, 173, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Spong, C.Y.; Dashe, J.S.; Hoffman, B.L. Ectopic Pregnancy. Williams Obstetretics, 24th ed.; McGraw-Hill Education: New York, NY, USA, 2013. [Google Scholar]
- Grimes, D.A. The morbidity and mortality of pregnancy. Still risky business. Am. J. Obstet. Gynecol. 1994, 170, 1489–1494. [Google Scholar]
- Khalil, M.M.; Badran, E.Y.; Ramadan, M.F.; Shazly, S.A.-E.M.; Ali, M.K.; Abdel Badee, A.Y. An advanced second trimester tubal pregnancy: Case report. Middle East Fertil. Soc. J. 2012, 17, 136–138. [Google Scholar] [CrossRef]
- Nkwabong, E.; Tincho, E. A case of a 26 weeks ampullary pregnancy mimicking IUD. Anatol. J. Obs. Gynecol. 2012, 1, 422–424. [Google Scholar]
- Sachan, R.; Gupta, P.; Patel, M. Second trimester unruptured ampullary ectopic pregnancy with variable presentations: Report of two cases. Int. J. Case Reports Images 2012, 3, 1–4. [Google Scholar]
- Kumar, V.; Gupta, J. Tubal ectopic pregnancy. BMJ Clin. Evid. 2015, 2015, 1406. [Google Scholar] [PubMed]
- Parker, J.; Bisits, A. Laparoscopic Surgical Treatment of Ectopic Pregnancy: Salpingectomy or Salpingostomy? Aust. N. Z. J. Obstet. Gynaecol. 1997, 37, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Clausen, I. Conservative versus radical surgery for tubal pregnancy. Acta Obstet. Gynecol. Scand. 1996, 75, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Thornton, K.L.; Diamond, M.P.; DeCherney, A.H. Linear salpingostomy for ectopic pregnancy. Obstet. Gynecol. Clin. N. Am. 1991, 18, 95–109. [Google Scholar] [CrossRef]
- Nama, V.; Manyonda, I. Tubal ectopic pregnancy: Diagnosis and management. Arch. Gynecol. Obstet. 2009, 279, 443–453. [Google Scholar] [CrossRef]
- Bangsgaard, N.; Lund, C.O.; Ottesen, B.; Nilas, L. Improved fertility following conservative surgical treatment of ectopic pregnancy. BJOG An. Int. J. Obstet. Gynaecol. 2003, 110, 765–770. [Google Scholar] [CrossRef]
- Mol, B.W.; Matthijsse, H.C.; Tinga, D.J.; Huynh, T.; Hajenius, P.J.; Ankum, W.M.; Bossuyt, P.M.; van der Veen, F. Fertility after conservative and radical surgery for tubal pregnancy. Hum. Reprod. 1998, 13, 1804–1809. [Google Scholar] [CrossRef]
- Kelly, A.J.; Sowter, M.C.; Trinder, J. The Management of Tubal Pregnancy; Royal College of Obstetricians and Gynaecologists: London, UK, 2004. [Google Scholar]
- Gracia, C.R.; Barnhart, K.T. Diagnosing ectopic pregnancy: Decision analysis comparing six strategies. Obstet. Gynecol. 2001, 97, 464–470. [Google Scholar] [CrossRef]
- Rulin, M.C. Is salpingostomy the surgical treatment of choice for unruptured tubal pregnancy? Obstet. Gynecol. 1995, 86, 1010–1013. [Google Scholar]
- Mukul, L.V.; Teal, S.B. Current Management of Ectopic Pregnancy. Obstet. Gynecol. Clin. North Am. 2007, 34, 403–419. [Google Scholar] [CrossRef]
- Goodman, L.S.; Gilman, A. The Pharmacological Basis of Therapeutics; The Macmillan: Stuttgart, Germany, 1955. [Google Scholar]
- Stovall, T.G.; Ling, F.W.; Gray, L.A. Single-dose methotrexate for treatment of ectopic pregnancy. Obstet. Gynecol. 1991, 77, 754–757. [Google Scholar] [PubMed]
- Lipscomb, G.H.; McCord, M.L.; Stovall, T.G.; Huff, G.; Portera, S.G.; Ling, F.W. Predictors of Success of Methotrexate Treatment in Women with Tubal Ectopic Pregnancies. N. Engl. J. Med. 1999, 341, 1974–1978. [Google Scholar] [CrossRef] [PubMed]
- Lipscomb, G.H.; Bran, D.; McCord, M.L.; Portera, J.C.; Ling, F.W. Analysis of three hundred fifteen ectopic pregnancies treated with single-dose methotrexate. Am. J. Obstet. Gynecol. 1998, 178, 1354–1358. [Google Scholar] [CrossRef]
- Sowter, M.C.; Farquhar, C.M.; Petrie, K.J.; Gudex, G. A randomised trial comparing single dose systemic methotrexate and laparoscopic surgery for the treatment of unruptured tubal pregnancy. BJOG An. Int. J. Obstet. Gynaecol. 2001, 108, 192–203. [Google Scholar] [CrossRef]
- Barnhart, K.T.; Gosman, G.; Ashby, R.; Sammel, M. The medical management of ectopic pregnancy: A meta-analysis comparing “single dose” and “multidose” regimens. Obstet. Gynecol. 2003, 101, 778–784. [Google Scholar] [CrossRef]
- Condous, G.; Timmerman, D.; Goldstein, S.; Valentin, L.; Jurkovic, D.; Bourne, T. Pregnancies of unknown location: Consensus statement. Ultrasound Obstet. Gynecol. 2006, 28, 121–122. [Google Scholar] [CrossRef]
- Yuk, J.-S.; Lee, J.H.; Park, W.I.; Ahn, H.S.; Kim, H.J. Systematic review and meta-analysis of single-dose and non-single-dose methotrexate protocols in the treatment of ectopic pregnancy. Int. J. Gynecol. Obstet. 2018, 141, 295–303. [Google Scholar] [CrossRef]
- Shalev, E.; Peleg, D.; Tsabari, A.; Romano, S.; Bustan, M. Spontaneous resolution of ectopic tubal pregnancy: Natural history. Fertil. Steril. 1995, 63, 15–19. [Google Scholar] [CrossRef]
- Lozeau, A.-M.; Potter, B. Diagnosis and management of ectopic pregnancy. Am. Fam. Physician 2005, 72, 1707–1714. [Google Scholar]
- Butts, S.; Sammel, M.; Hummel, A.; Chittams, J.; Barnhart, K. Risk factors and clinical features of recurrent ectopic pregnancy: A case control study. Fertil. Steril. 2003, 80, 1340–1344. [Google Scholar] [CrossRef]
- Alur-Gupta, S.; Cooney, L.G.; Senapati, S.; Sammel, M.D.; Barnhart, K.T. Two-dose versus single-dose methotrexate for treatment of ectopic pregnancy: A meta-analysis. Am. J. Obstet. Gynecol. 2019, 221, 95–108. [Google Scholar] [CrossRef]
- Murphy, A.A.; Nager, C.W.; Wujek, J.J.; Michael Kettel, L.; Torp, V.A.; Chin, H.G. Operative laparoscopy versus laparotomy for the management of ectopic pregnancy: A prospective trial. In Proceedings of the 46th Annual Meeting of The American Fertility Society, Washington, DC, USA, 13–18 October 1990. [Google Scholar]
- Abdulkareem, T.A. Ectopic Pregnancy: Diagnosis, Prevention and Management; Abduljabbar, H.S., Ed.; IntechOpen: Rijeka, Croatia, 2017; p. 3. [Google Scholar] [CrossRef]
- Ankum, W.M.; Mol, B.W.J.; van der Veen, F.; Bossuyt, P.M.M. Risk factors for ectopic pregnancy: A meta-analysis. in part by grant OG 93/007 from the Ziekenfonds-Raad, Amstelveen, The Netherlands. Fertil Steril 1996, 65, 1093–1099. [Google Scholar] [CrossRef]
- Gueye, M.D.N.; Gueye, M.; Thiam, I.; Mbaye, M.; Gaye, A.M.; Diouf, A.A.; Niang, M.M.; Moreau, J.C. Unruptured tubal pregnancy in the second trimester. South Sudan Med. J. 2013, 6, 95–96. [Google Scholar]
- Radaelli, T.; Bulfamante, G.; Cetin, I.; Marconi, A.M.; Pardi, G. Advanced tubal pregnancy associated with severe fetal growth restriction: A case report. J. Matern. Neonatal. Med. 2003, 13, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Perkins, K.M.; Boulet, S.L.; Kissin, D.M.; Jamieson, D.J.; Group for the NARTS (NASS). Risk of Ectopic Pregnancy Associated With Assisted Reproductive Technology in the United States, 2001–2011. Obstet. Gynecol. 2015, 125, 70. [Google Scholar] [CrossRef] [Green Version]
- Backman, T.; Rauramo, I.; Huhtala, S.; Koskenvuo, M. Pregnancy during the use of levonorgestrel intrauterine system. Am. J. Obstet. Gynecol. 2004, 190, 50–54. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 193 Summary: Tubal Ectopic Pregnancy. Obstet. Gynecol. 2018, 131, e91–e103. [Google Scholar] [CrossRef]
- Zacharis, K.; Kravvaritis, S.; Charitos, T.; Fouka, A. Ectopic Pregnancy at 13-week Period of Gestation with Live Fetus. HJOG 2018, 17, 99–102. [Google Scholar] [CrossRef]
- Kim, M.; Hiramatsu, K.; Fukui, K.; Amemiya, K. Unexpected Tubal Pregnancy at 13 Weeks’ Gestation that Was Treated with Laparoscopic Surgery Under Massive Hemoperitoneum. Gynecol. Minim. Invasive Ther. 2019, 8, 30–32. [Google Scholar] [CrossRef]
- Gari, R.; Abdulgader, R.; Abdulqader, O. A Live 13 Weeks Ruptured Ectopic Pregnancy: A Case Report. Cureus 2020, 12, e10993. [Google Scholar] [CrossRef]
- Hamura, N.N.; Bolnga, J.W.; Wangnapi, R.; Horne, A.W.; Rogerson, S.J.; Unger, H.W. The impact of tubal ectopic pregnancy in Papua New Guinea—A retrospective case review. BMC Pregnancy Childbirth 2013, 13, 86. [Google Scholar] [CrossRef]
- Davenport, M.J.; Lindquist, A.; Brownfoot, F.; Pritchard, N.; Tong, S.; Hastie, R. Time to resolution of tubal ectopic pregnancy following methotrexate treatment: A retrospective cohort study. PLoS ONE 2022, 17, e0268741. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; Gallos, I.; Dobson, S.; Campbell, B.K.; Coomarasamy, A.; Raine-Fenning, N. Accuracy of first-trimester ultrasound in diagnosis of tubal ectopic pregnancy in the absence of an obvious extrauterine embryo: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2016, 47, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Kirk, E.; Bottomley, C.; Bourne, T. Diagnosing ectopic pregnancy and current concepts in the management of pregnancy of unknown location. Hum. Reprod. Update 2014, 20, 250–261. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year of Publication | Age of Patient | Common Clinical Signs, Intervention and Weeks of Gestation | Reference |
|---|---|---|---|
| 2018 | 31-year-old | amenorrhea for three months and one week; abdominal pain; Hb 8.5 g/dL; β-hCG 80.427, 9 mIU/mL; salpingo-oophorectomy | [43] |
| 2019 | 39-year-old | abdominal pain; vaginal bleeding; Hb 8.7 g/dL; β-hCG 55.713 mIU/mL; salpingectomy | [44] |
| 2020 | 38-year-old | amenorrhea for three months; abdominal pain; Hb 3.2 g/L; β-hCG 11.300 IU/mL; salpingectomy | [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilea, C.; Ilie, O.-D.; Marcu, O.-A.; Stoian, I.; Doroftei, B. The Very First Romanian Unruptured 13-Weeks Gestation Tubal Ectopic Pregnancy. Medicina 2022, 58, 1160. https://doi.org/10.3390/medicina58091160
Ilea C, Ilie O-D, Marcu O-A, Stoian I, Doroftei B. The Very First Romanian Unruptured 13-Weeks Gestation Tubal Ectopic Pregnancy. Medicina. 2022; 58(9):1160. https://doi.org/10.3390/medicina58091160
Chicago/Turabian StyleIlea, Ciprian, Ovidiu-Dumitru Ilie, Olivia-Andreea Marcu, Irina Stoian, and Bogdan Doroftei. 2022. "The Very First Romanian Unruptured 13-Weeks Gestation Tubal Ectopic Pregnancy" Medicina 58, no. 9: 1160. https://doi.org/10.3390/medicina58091160