
Role of Human Papilloma Virus and Lifestyle Factors in Overall Survival of Patients with Oropharyngeal Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. HPV and Cancer Diagnoses
2.3. Detection and Genotyping of HPV
2.4. Staging and Treatment
2.5. Consumption of Alcohol and Tobacco
2.6. Statistical Analyses
3. Results
3.1. HPV Status and Patient Characteristics
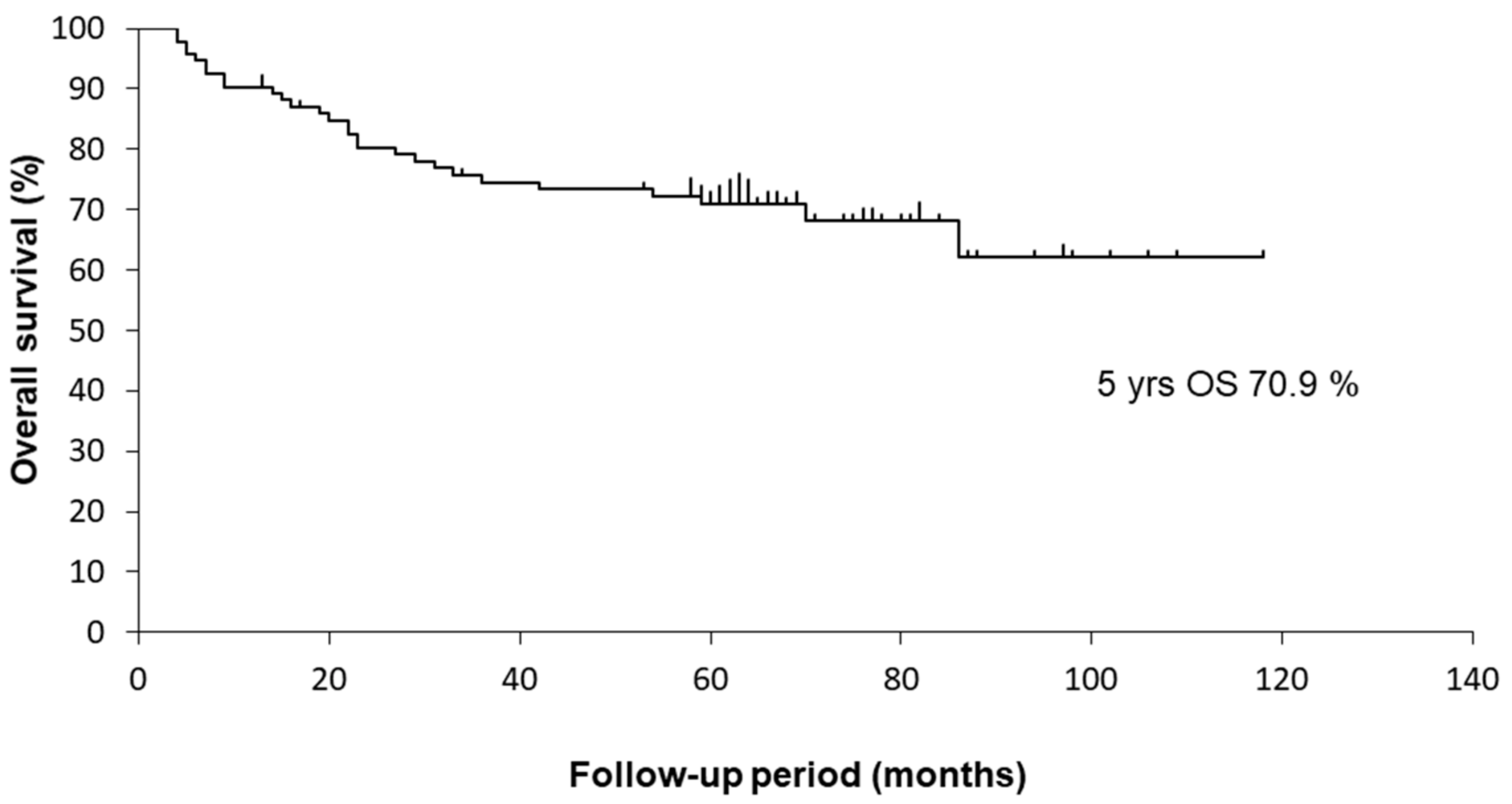
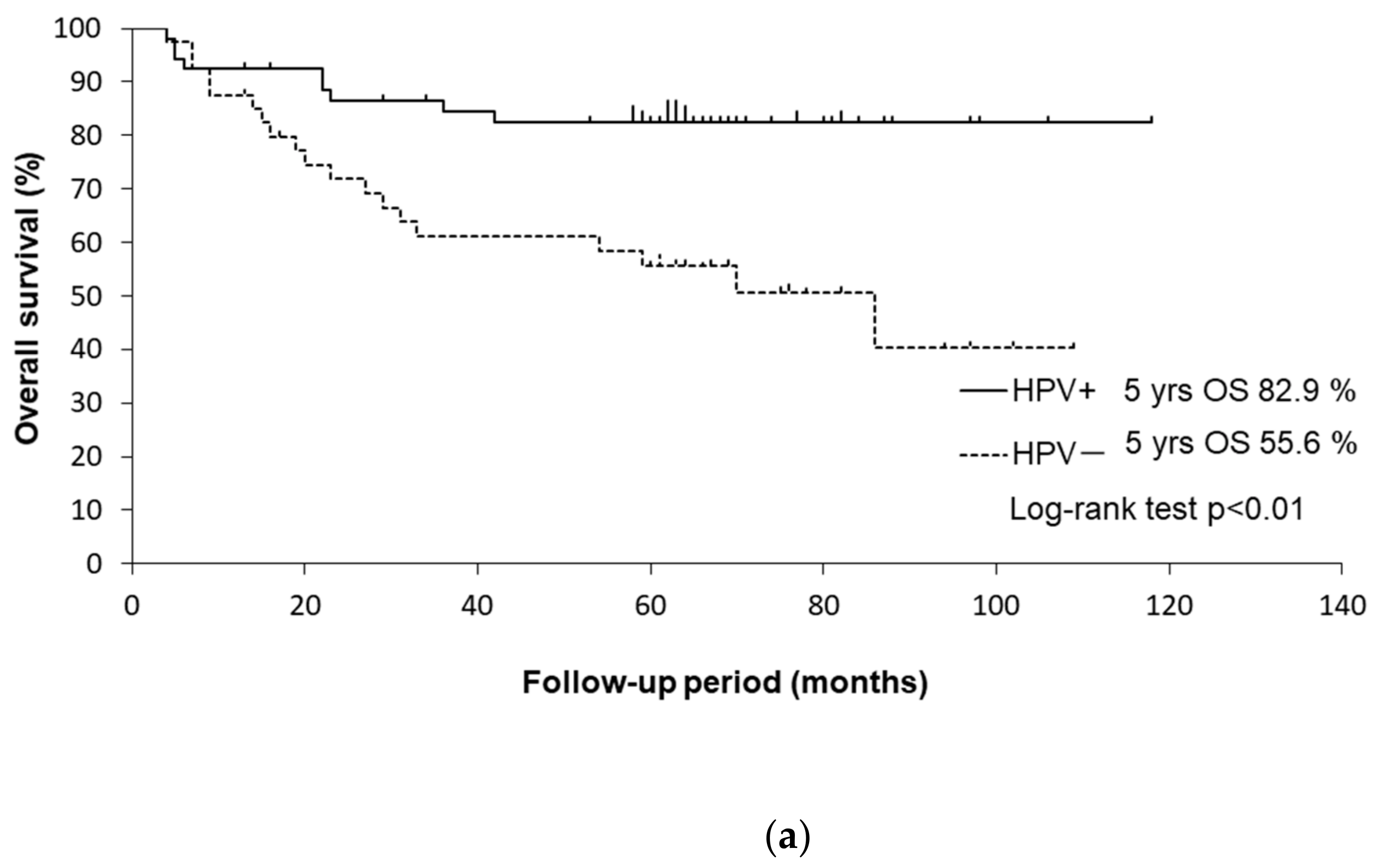
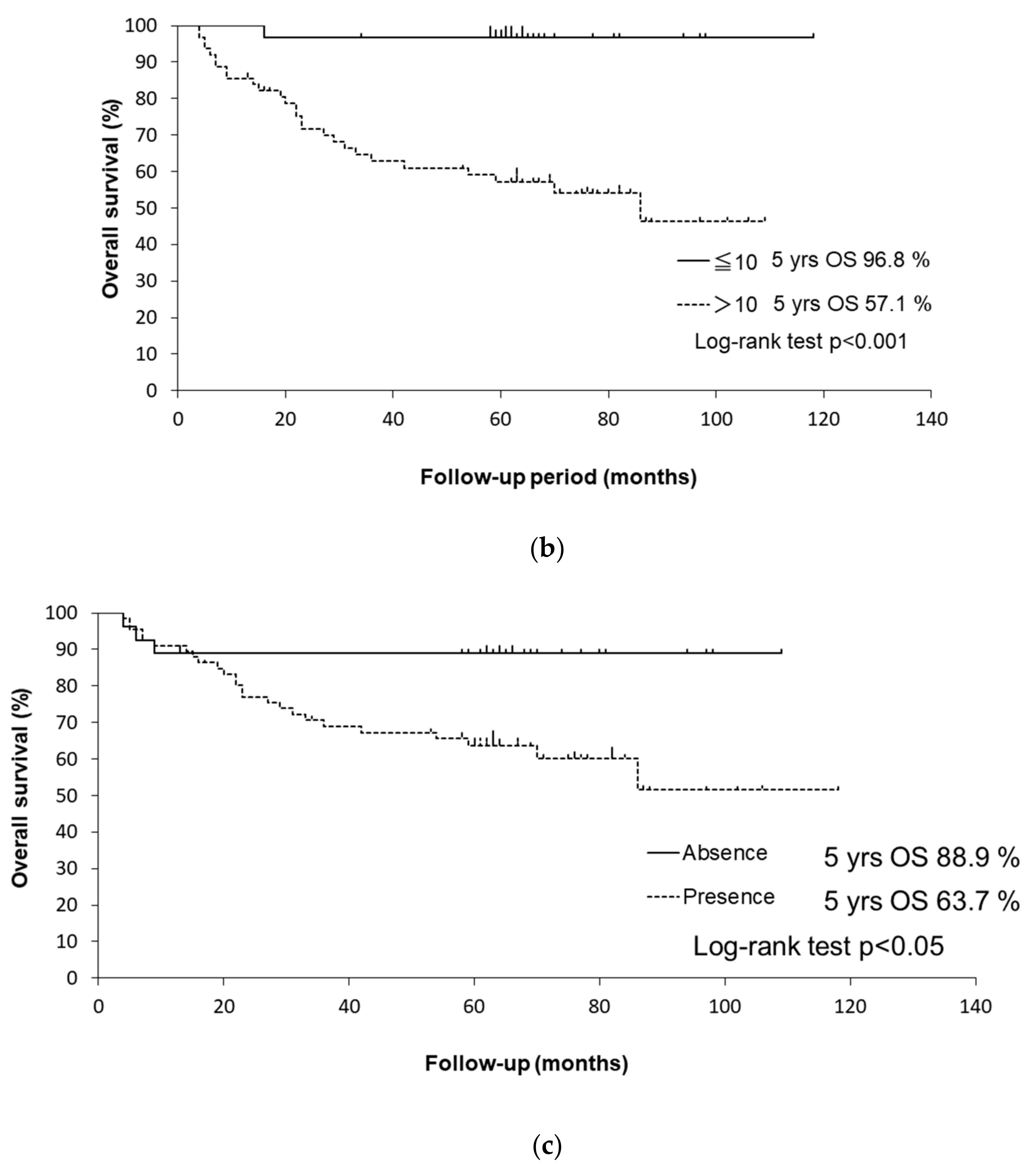
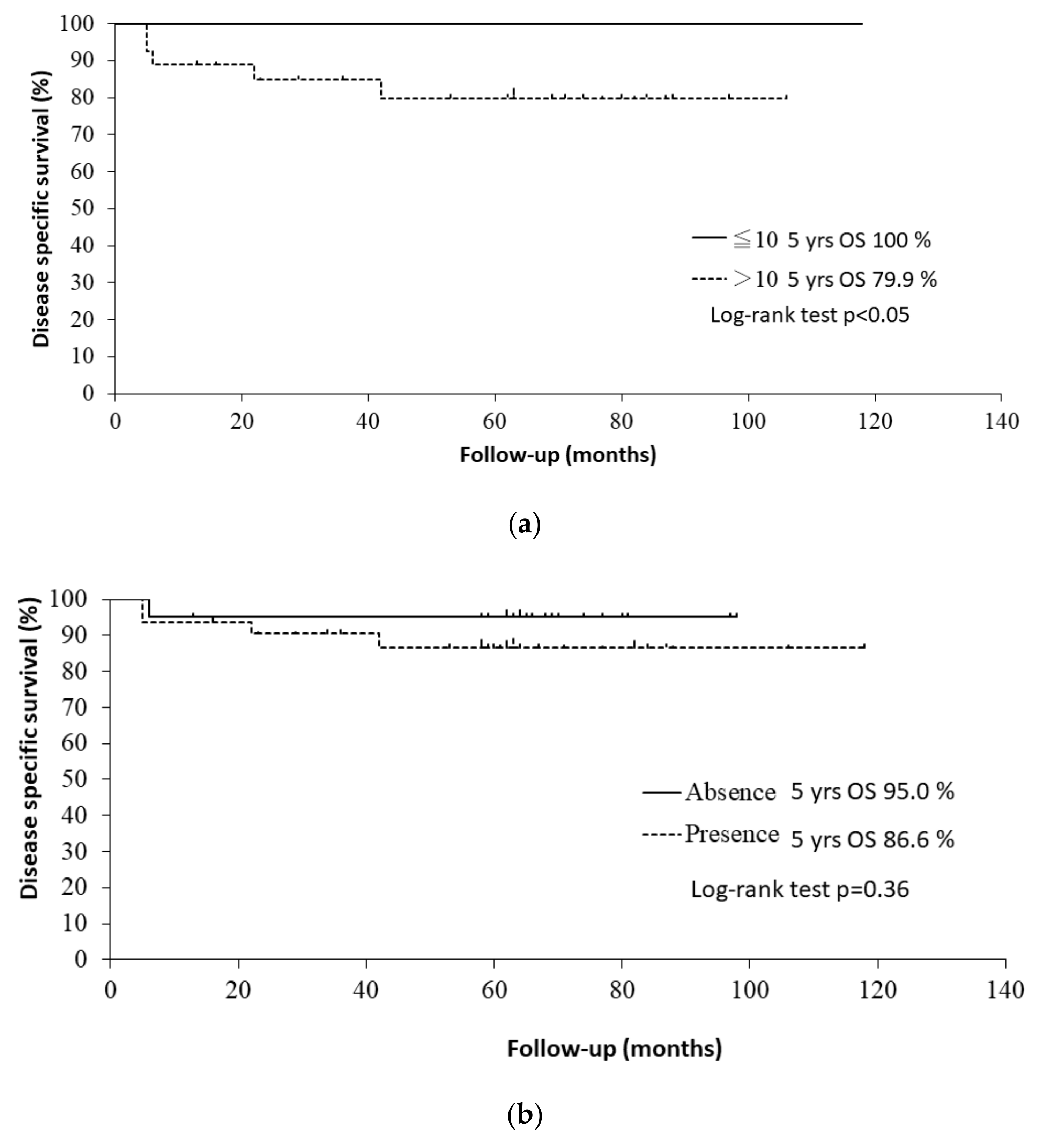
3.2. Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; Dandona, L.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Blot, W.J.; McLaughlin, J.K.; Winn, D.M.; Austin, D.F.; Greenberg, R.S.; Preston-Martin, S.; Bernstein, L.; Schoenberg, J.B.; Stemhagen, A.; Fraumeni, J.F. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res. 1988, 48, 3282–3287. [Google Scholar] [PubMed]
- Wyss, A.; Hashibe, M.; Chuang, S.-C.; Lee, Y.-C.A.; Zhang, Z.-F.; Yu, G.-P.; Winn, D.M.; Wei, Q.; Talamini, R.; Szeszenia-Dabrowska, N.; et al. Cigarette, Cigar, and Pipe Smoking and the Risk of Head and Neck Cancers: Pooled Analysis in the International Head and Neck Cancer Epidemiology Consortium. Am. J. Epidemiol. 2013, 178, 679–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Bonilla-Velez, J.; Mroz, E.A.; Hammon, R.J.; Rocco, J.W. Impact of human papillomavirus on oropharyngeal cancer biology and response to therapy: Implications for treatment. Otolaryngol. Clin. N. Am. 2013, 46, 521–543. [Google Scholar] [CrossRef] [Green Version]
- Marur, S.; Li, S.; Cmelak, A.J.; Gillison, M.L.; Zhao, W.J.; Ferris, R.L.; Westra, W.H.; Gilbert, J.; Bauman, J.E.; Wagner, L.I.; et al. E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced-Dose Radiation and Weekly Cetuximab in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx— ECOG-ACRIN Cancer Research Group. J. Clin. Oncol. 2017, 35, 490–497. [Google Scholar] [CrossRef]
- Gillison, M.L.; Zhang, Q.; Jordan, R.; Xiao, W.; Westra, W.H.; Trotti, A.; Spencer, S.; Harris, J.; Chung, C.H.; Ang, K.K. Tobacco Smoking and Increased Risk of Death and Progression for Patients With p16-Positive and p16-Negative Oropharyngeal Cancer. J. Clin. Oncol. 2012, 30, 2102–2111. [Google Scholar] [CrossRef]
- Lassen, P.; Lacas, B.; Pignon, J.-P.; Trotti, A.; Zackrisson, B.; Zhang, Q.; Overgaard, J.; Blanchard, P. Prognostic impact of HPV-associated p16-expression and smoking status on outcomes following radiotherapy for oropharyngeal cancer: The MARCH-HPV project. Radiother. Oncol. 2018, 126, 107–115. [Google Scholar] [CrossRef]
- Hafkamp, H.C.; Manni, J.J.; Haesevoets, A.; Voogd, A.; Schepers, M.; Bot, F.; Hopman, A.; Ramaekers, F.; Speel, E.-J.M. Marked differences in survival rate between smokers and nonsmokers with HPV 16-associated tonsillar carcinomas. Int. J. Cancer 2008, 122, 2656–2664. [Google Scholar] [CrossRef]
- Maxwell, J.H.; Kumar, B.; Feng, F.Y.; Worden, F.P.; Lee, J.S.; Eisbruch, A.; Wolf, G.T.; Prince, M.E.; Moyer, J.S.; Teknos, T.N.; et al. Tobacco Use in Human Papillomavirus-Positive Advanced Oropharynx Cancer Patients Related to Increased Risk of Distant Metastases and Tumor Recurrence. Clin. Cancer Res. 2010, 16, 1226–1235. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.H.; Xu, W.; Waldron, J.; Siu, L.; Shen, X.; Tong, L.; Ringash, J.; Bayley, A.; Kim, J.; Hope, A.; et al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM Stage and Prognostic Groups for Human Papillomavirus–Related Oropharyngeal Carcinomas. J. Clin. Oncol. 2015, 33, 836–845. [Google Scholar] [CrossRef]
- Maruyama, H.; Yasui, T.; Ishikawa-Fujiwara, T.; Morii, E.; Yamamoto, Y.; Yoshii, T.; Takenaka, Y.; Nakahara, S.; Todo, T.; Hongyo, T.; et al. Human papillomavirus and p53 mutations in head and neck squamous cell carcinoma among Japanese population. Cancer Sci. 2014, 105, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, M.H.; McMillan, N.A.; Johnson, N.W. HPV—Associated head and neck cancers in the Asia Pacific: A critical literature review & meta—Analysis. Cancer Epidemiol. 2015, 39, 923–938. [Google Scholar]
- Saito, Y.; Hayashi, R.; Iida, Y.; Mizumachi, T.; Fujii, T.; Matsumoto, F.; Beppu, T.; Yoshida, M.; Shinomiya, H.; Kamiyama, R.; et al. Optimization of therapeutic strategy for p16-positive oropharyngeal squamous cell carcinoma: Multi-institutional observational study based on the national Head and Neck Cancer Registry of Japan. Cancer 2020, 126, 4177–4187. [Google Scholar] [CrossRef]
- Mirghani, H.; Amen, F.; Blanchard, P.; Moreau, F.; Guigay, J.; Hartl, D.; Guily, J.L.S. Treatment de-escalation in HPV-positive oropharyngeal carcinoma: Ongoing trials, critical issues and perspectives. Int. J. Cancer 2015, 136, 1494–1503. [Google Scholar] [CrossRef]
- Nishiwaki, M.; Yamamoto, T.; Tone, S.; Murai, T.; Ohkawara, T.; Matsunami, T.; Koizumi, M.; Takagi, Y.; Yamaguchi, J.; Kondo, N.; et al. Genotyping of Human Papillomaviruses by a Novel One-Step Typing Method with Multiplex PCR and Clinical Applications. J. Clin. Microbiol. 2008, 46, 1161–1168. [Google Scholar] [CrossRef] [Green Version]
- Mayne, S.T.; Cartmel, B.; Kirsh, V.; Goodwin, W.J. Alcohol and tobacco use pre- and post-diagnosis, and survival in a cohort of patients with early stage cancers of the oral cavity, pharynx, and larynx. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3368–3374. [Google Scholar] [CrossRef] [Green Version]
- Parsons, J.T.; Mendenhall, W.M.; Stringer, S.P.; Amdur, R.J.; Hinerman, R.W.; Villaret, D.B.; Moore-Higgs, G.J.; Greene, B.D.; Speer, T.W.; Cassisi, N.J.; et al. Squamous cell carcinoma of the oropharynx. Cancer 2002, 94, 2967–2980. [Google Scholar] [CrossRef]
- Iyer, N.G.; Tan, D.S.W.; Tan, V.K.M.; Wang, W.; Hwang, J.; Tan, N.-C.; Sivanandan, R.; Tan, H.-K.; Lim, D.W.-T.; Ang, M.-K.; et al. Randomized trial comparing surgery and adjuvant radiotherapy versus concurrent chemoradiotherapy in patients with advanced, nonmetastatic squamous cell carcinoma of the head and neck: 10-year update and subset analysis. Cancer 2015, 121, 1599–1607. [Google Scholar] [CrossRef]
- Kelly, J.R.; Park, H.S.; An, Y.; Yarbrough, W.G.; Contessa, J.N.; Decker, R.; Mehra, S.; Judson, B.L.; Burtness, B.; Husain, Z. Upfront surgery versus definitive chemoradiotherapy in patients with human papillomavirus-associated oropharyngeal squamous cell cancer. Oral Oncol. 2018, 79, 64–70. [Google Scholar] [CrossRef]
- Reyna, V.F.; Nelson, W.L.; Han, P.K.; Pignone, M.P. Decision making and cancer. Am. Psychol. 2015, 70, 105–118. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 94 | HPV Status | ||
|---|---|---|---|
| Positive n = 53 | Negative n = 41 | ||
| No. (%) | No. (%) | No. (%) | |
| Lateral wall | 64 (68) | 40 (75) | 24 (59) |
| Anterior wall | 23 (25) | 13 (25) | 10 (24) |
| Posterior wall | 4 (4) | 0 (0) | 4 (10) |
| Superior wall | 3 (3) | 0 (0) | 3 (7) |
| Tclassification | N0 | N1 | N2 | N3 | Total |
|---|---|---|---|---|---|
| T1 | 1 | 0 | 2 | 0 | 3 (3%) |
| T2 | 8 | 9 | 33 | 1 | 51 (54%) |
| T3 | 1 | 4 | 10 | 3 | 18 (19%) |
| T4 | 2 | 3 | 15 | 2 | 22 (24%) |
| Total | 12 (13%) | 16 (17%) | 60 (64%) | 6 (6%) | 94 |
| Total n = 94 | HPV Status | No. of Pack-Years | Alcohol Consumption | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Positive n = 53 | Negative n = 41 | ≤10 n = 31 | >10 n = 63 | Presence n = 67 | Absence n = 27 | |||||
| No. (%) | No. (%) | No. (%) | p Value | No. (%) | No. (%) | p Value | No. (%) | No. (%) | p Value | |
| Age, range (median) years | 35–79 (59) | 35–79 (58) | 37–78 (60) | 0.20 b | 37–76 (57) | 35–79 (60) | 0.37 b | 35–78 (59) | 41–79 (59) | 0.95 b |
| Sex | 0.71 a | <0.01 a | 0.04 a | |||||||
| Male | 75 (80) | 43 (81) | 32 (78) | 17 (55) | 58 (92) | 57 (85) | 18 (67) | |||
| Female | 19 (20) | 10 (19) | 9 (22) | 14 (45) | 5 (8) | 10 (15) | 9 (33) | |||
| Clinical T classification | 0.28 a | 0.01 a | 0.81 a | |||||||
| T1–2 | 54 (57) | 33 (62) | 21 (51) | 24 (77) | 30 (48) | 39 (58) | 15 (56) | |||
| T3–4 | 40 (43) | 20 (38) | 20 (49) | 7 (23) | 33 (52) | 28 (42) | 12 (44) | |||
| Clinical N classification | 0.27 a | 0.01 a | 0.08 a | |||||||
| N0 | 12 (13) | 5 (9) | 7 (17) | 8 (26) | 4 (6) | 6 (9) | 6 (22) | |||
| N1–3 | 82 (87) | 48 (91) | 34 (83) | 23 (74) | 59 (94) | 61 (91) | 21 (78) | |||
| Clinical stage | 0.14 a | <0.01 a | 0.06 a | |||||||
| Stage I–II | 9 (10) | 3 (6) | 6 (15) | 6 (19) | 3 (5) | 4 (6) | 5 (19) | |||
| Stage III–IV | 85 (90) | 50 (94) | 35 (85) | 25 (81) | 60 (95) | 63 (94) | 22 (81) | |||
| Tobacco smoking, range (median) pack-years | 0–88(29) | 0–83(21) | 0–88(38) | <0.01 b | 0–10 (1) | 12–88 (42) | 0–88(35) | 0–60 (14) | <0.01 b | |
| No. of pack-years | <0.01 a | <0.01 a | ||||||||
| ≤10 | 31 (33) | 25 (47) | 6 (15) | 15 (22) | 16 (59) | |||||
| >10 | 63 (67) | 28 (53) | 35 (85) | 52 (78) | 11 (41) | |||||
| Alcohol consumption | 0.03 a | <0.01 a | ||||||||
| Presence | 67 (71) | 33 (62) | 34 (83) | 15 (48) | 52 (83) | |||||
| Absence | 27 (29) | 20 (38) | 7 (17) | 16 (52) | 11 (17) | |||||
| HPV status | <0.01 a | 0.03 a | ||||||||
| Positive | 53 (56) | 25 (81) | 28 (44) | 33 (49) | 20 (74) | |||||
| Negative | 41 (44) | 6 (19) | 35 (56) | 34 (51) | 7 (26) | |||||
| Treatment group | 0.49 a | 0.36 a | 0.07 a | |||||||
| Surgery | 24 (26) | 11 (21) | 13 (32) | 9 (29) | 15 (24) | 21 (31) | 3 (11) | |||
| Radiation | 70 (74) | 42 (79) | 28 (68) | 22 (71) | 48 (76) | 46 (69) | 24 (89) | |||
| Induction chemotherapy | 0.57 a | 0.13 a | 0.53 a | |||||||
| Presence | 67 (71) | 39 (74) | 28 (68) | 19 (61) | 48 (76) | 49 (72) | 18 (67) | |||
| Absence | 27 (29) | 14 (26) | 13 (32) | 12 (39) | 15 (24) | 18 (27) | 9 (33) | |||
| HR | 95% CI | p | ||
|---|---|---|---|---|
| Age | >50 vs. ≤50 | 1.61 | 0.55–4.65 | 0.38 |
| Sex | Male vs. Famale | 4.02 | 0.95–16.9 | 0.06 |
| Clinical T | T3-4 vs. T1-2 | 2.87 | 1.32–6.25 | 0.01 |
| Clinical N | N1-3 vs. N0 | 2.23 | 0.53–9.41 | 0.27 |
| Clinical stage | III-IV vs. I-II | 3.62 | 0.49–26.6 | 0.21 |
| Smoking (no. of pack-years) | >10 vs. ≤10 | 17.5 | 2.37–129.0 | 0.01 |
| Alcohol consumption | Presence vs. Absence | 3.67 | 1.11–12.2 | 0.03 |
| HPV status | Negative vs. Positive | 3.18 | 1.43–7.04 | <0.01 |
| Treatment group | Surgery vs. Radiation | 0.85 | 0.38–1.89 | 0.69 |
| Induction chemotherapy | Presence vs. Absence | 1.27 | 0.54–3.00 | 0.58 |
| HR | 95% CI | p | ||
|---|---|---|---|---|
| Clinical stage | III–IV vs. I–II | 2.6 | 0.34–19.4 | 0.36 |
| Smoking (no. of pack-years) | >10 vs. ≤10 | 10.4 | 1.34–80.6 | 0.03 |
| Alcohol consumption | Presence vs. Absence | 1.6 | 0.48–5.50 | 0.44 |
| HPV status | Negative vs. Positive | 2.1 | 0.91–4.65 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, D.; Hanai, N.; Ozawa, T.; Kitahara, T.; Hasegawa, Y. Role of Human Papilloma Virus and Lifestyle Factors in Overall Survival of Patients with Oropharyngeal Squamous Cell Carcinoma. Medicina 2022, 58, 557. https://doi.org/10.3390/medicina58040557
Nishikawa D, Hanai N, Ozawa T, Kitahara T, Hasegawa Y. Role of Human Papilloma Virus and Lifestyle Factors in Overall Survival of Patients with Oropharyngeal Squamous Cell Carcinoma. Medicina. 2022; 58(4):557. https://doi.org/10.3390/medicina58040557
Chicago/Turabian StyleNishikawa, Daisuke, Nobuhiro Hanai, Taijiro Ozawa, Tadashi Kitahara, and Yasuhisa Hasegawa. 2022. "Role of Human Papilloma Virus and Lifestyle Factors in Overall Survival of Patients with Oropharyngeal Squamous Cell Carcinoma" Medicina 58, no. 4: 557. https://doi.org/10.3390/medicina58040557