
Anti-Citrullinated Peptide Antibody Expression and Its Association with Clinical Features and Outcomes in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
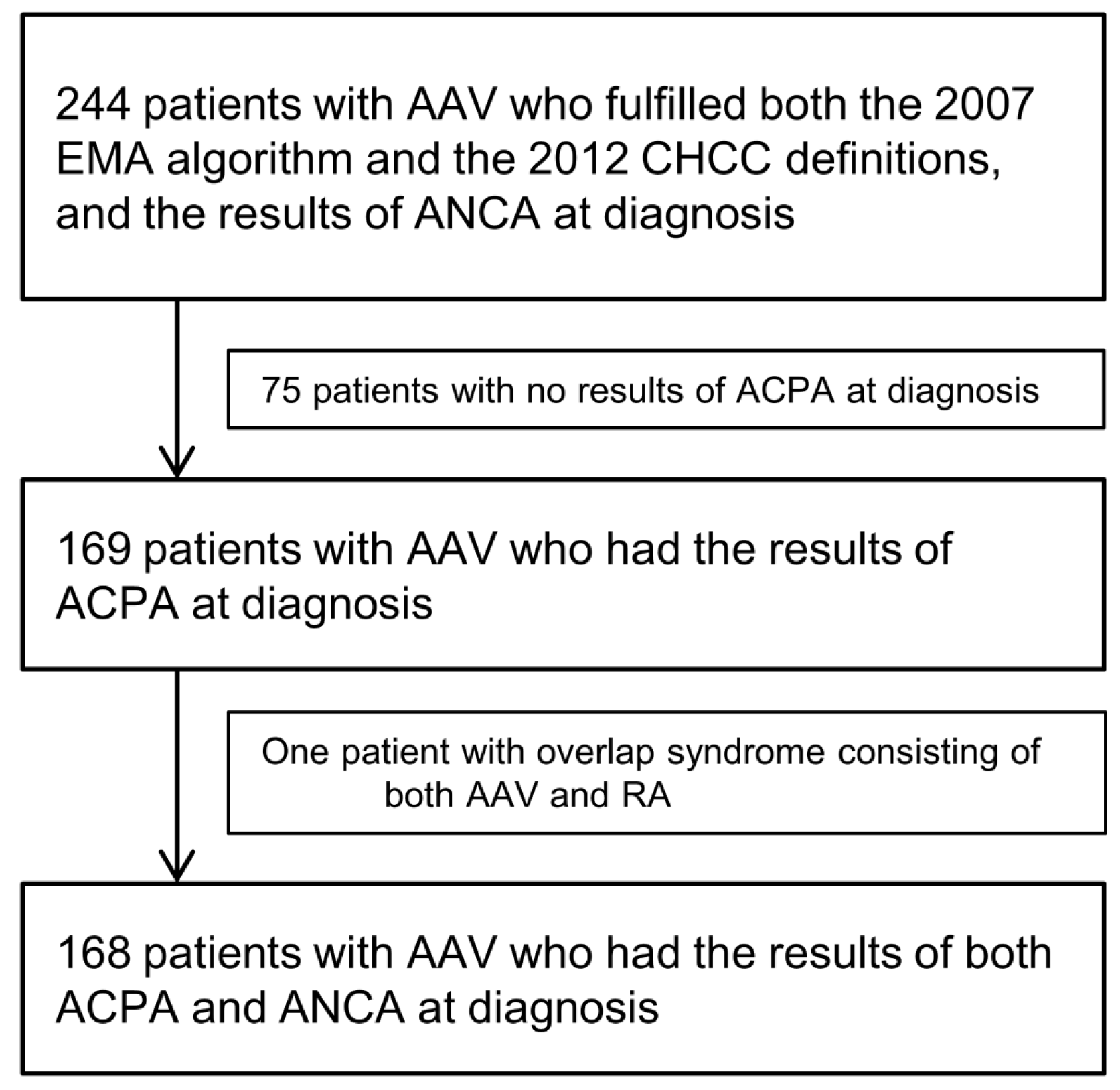
2.1. Selection of Study Subjects
2.2. Variables Assessment at Diagnosis
2.3. Outcomes Evaluated during the Follow-up
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Differences between 153 ACPA-Negative and 15 ACPA-Positive AAV Patients
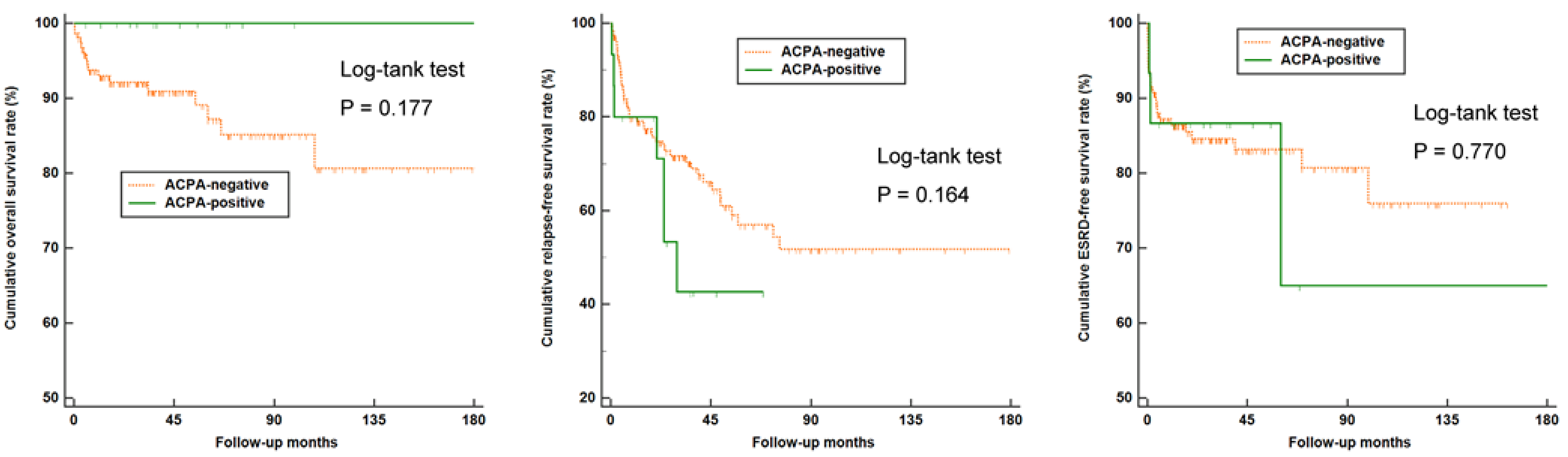
3.3. Comparison of Overall, Relapse-Free, and ESRD-Free Survival Rates between ACPA-Negative and ACPA-Positive AAV Patients
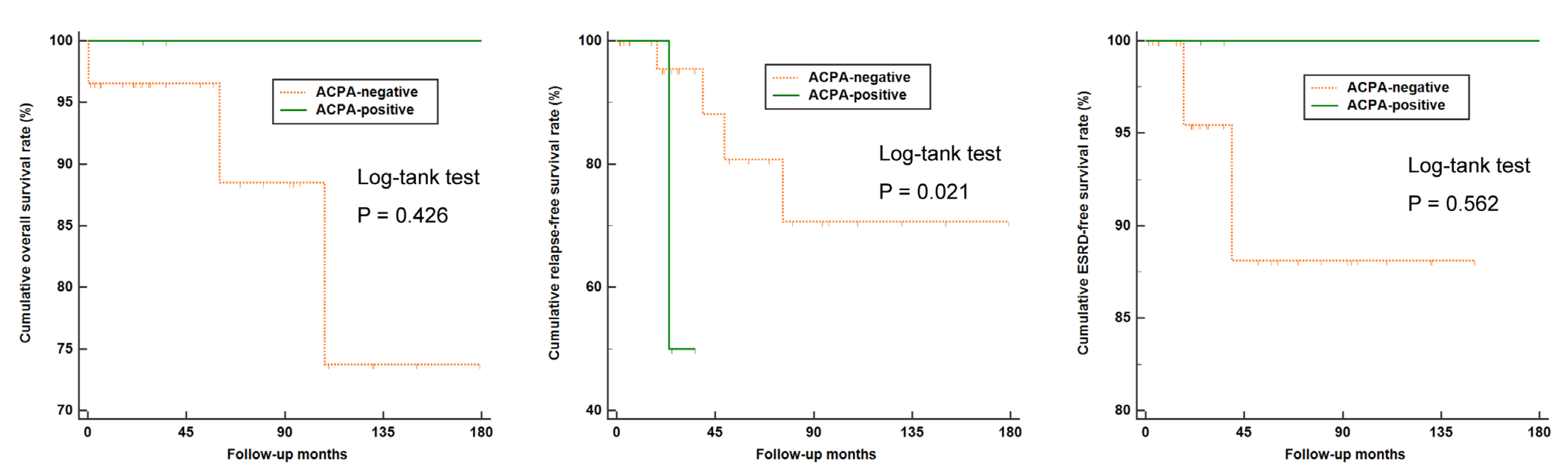
3.4. Disease Relapse Rate among Patients with and without ANCA
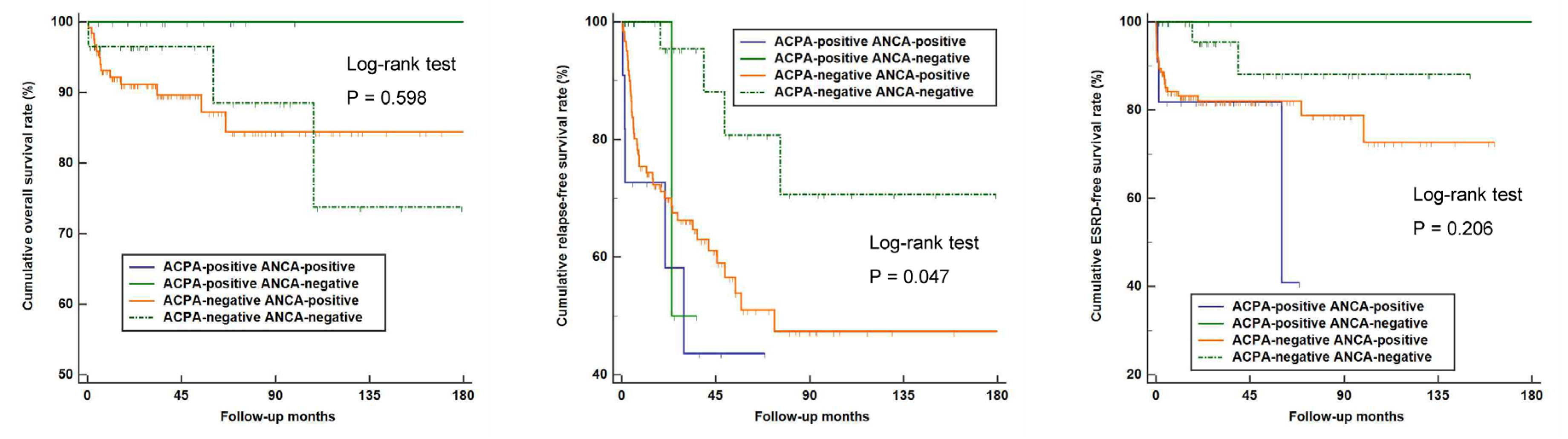
3.5. Comparison of the Overall, Relapse-Free, and ESRD-Free Survival Rates According to ACPA and ANCA Detection
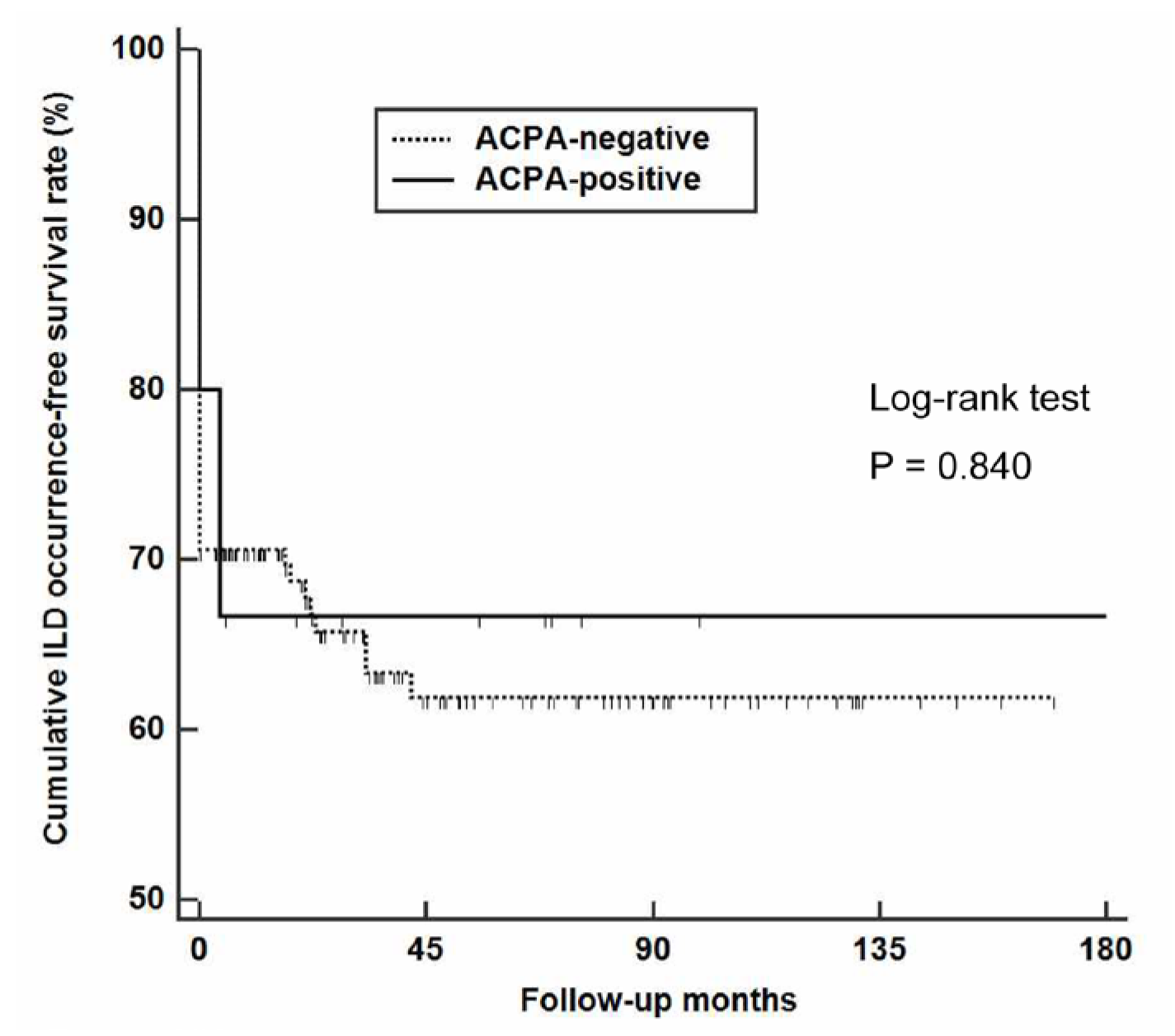
3.6. Occurrence of ILD According to ACPA Positivity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mondal, S.; Thompson, P.R. Protein Arginine Deiminases (PADs): Biochemistry and Chemical Biology of Protein Citrullination. Acc. Chem. Res. 2019, 52, 818–832. [Google Scholar] [CrossRef] [PubMed]
- Makrygiannakis, D.; Klint, E.A.; Lundberg, I.E.; Lofberg, R.; Ulfgren, A.-K.; Klareskog, L.; Catrina, A.I. Citrullination is an inflammation-dependent process. Ann. Rheum. Dis. 2006, 65, 1219–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-Y.; Yang, H.-Y.; Lai, J.-H. Anti-Citrullinated Protein Antibodies in Patients with Rheumatoid Arthritis: Biological Effects and Mechanisms of Immunopathogenesis. Int. J. Mol. Sci. 2020, 21, 4015. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, I.E.A.; Peene, I.; Cebecauer, L.; Isenberg, D.; Huizinga, T.W.J.; Union, A.; Meheus, L.; De Bosschere, K.; Hulstaert, F.; Veys, E.M.; et al. Presence of rheumatoid factor and antibodies to citrullinated peptides in systemic lupus erythematosus. Ann. Rheum. Dis. 2005, 64, 330–332. [Google Scholar] [CrossRef] [Green Version]
- Amezcua-Guerra, L.M.; Springall, R.; Marquez-Velasco, R.; Gómez-García, L.; Vargas, A.; Bojalil, R. Presence of antibodies against cyclic citrullinated peptides in patients with ‘rhupus’: A cross-sectional study. Arthritis Res. Ther. 2006, 8, R144. [Google Scholar] [CrossRef] [Green Version]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The american rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Care Res. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Kay, J.; Upchurch, K.S. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology 2012, 51, vi5–vi9. [Google Scholar] [CrossRef] [Green Version]
- Perry, E.; Kelly, C.; Eggleton, P.; De Soyza, A.; Hutchinson, D. The lung in ACPA-positive rheumatoid arthritis: An initiating site of injury? Rheumatology 2014, 53, 1940–1950. [Google Scholar] [CrossRef] [Green Version]
- van Boheemen, L.; van Beers-Tas, M.H.; Kroese, J.M.; van de Stadt, L.A.; van Schaardenburg, D.; Nurmohamed, M.T. Cardiovascular risk in persons at risk of developing rheumatoid arthritis. PLoS ONE 2020, 15, e0237072. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kronbichler, A.; Park, D.D.-Y.; Park, Y.; Moon, H.; Kim, H.; Choi, J.H.; Choi, Y.; Shim, S.; Lyu, I.S.; et al. Neutrophil extracellular traps (NETs) in autoimmune diseases: A comprehensive review. Autoimmun. Rev. 2017, 16, 1160–1173. [Google Scholar] [CrossRef] [PubMed]
- Khandpur, R.; Carmona-Rivera, C.; Vivekanandan-Giri, A.; Gizinski, A.; Yalavarthi, S.; Knight, J.S.; Friday, S.; Li, S.; Patel, R.M.; Subramanian, V.; et al. NETs Are a Source of Citrullinated Autoantigens and Stimulate Inflammatory Responses in Rheumatoid Arthritis. Sci. Transl. Med. 2013, 5, 178ra40. [Google Scholar] [CrossRef] [Green Version]
- Nakazawa, D.; Masuda, S.; Tomaru, U.; Ishizu, A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat. Rev. Rheumatol. 2018, 15, 91–101. [Google Scholar] [CrossRef]
- Kraaij, T.; Kamerling, S.W.; van Dam, L.; Bakker, J.A.; Bajema, I.M.; Page, T.; Brunini, F.; Pusey, C.D.; Toes, R.; Scherer, H.U.; et al. Excessive neutrophil extracellular trap formation in ANCA-associated vasculitis is independent of ANCA. Kidney Int. 2018, 94, 139–149. [Google Scholar] [CrossRef]
- Chirivi, R.G.S.; van Rosmalen, J.W.G.; van der Linden, M.; Euler, M.; Schmets, G.; Bogatkevich, G.; Kambas, K.; Hahn, J.; Braster, Q.; Soehnlein, O.; et al. Therapeutic ACPA inhibits NET formation: A potential therapy for neutrophil-mediated inflammatory diseases. Cell. Mol. Immunol. 2021, 18, 1528–1544. [Google Scholar] [CrossRef] [Green Version]
- McAdoo, S.P.; Medjeral-Thomas, N.; Gopaluni, S.; Tanna, A.; Mansfield, N.; Galliford, J.; Griffith, M.; Levy, J.; Cairns, T.D.; Jayne, D.; et al. Long-term follow-up of a combined rituximab and cyclophosphamide regimen in renal anti-neutrophil cytoplasm antibody-associated vasculitis. Nephrol. Dial. Transplant. 2018, 34, 63–73. [Google Scholar] [CrossRef]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2008, 68, 1827–1832. [Google Scholar] [CrossRef] [Green Version]
- Guillevin, L.; Pagnoux, C.; Seror, R.; Mahr, A.; Mouthon, L.; Toumelin, P.L. The Five-Factor Score revisited: Assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine 2011, 90, 19–27. [Google Scholar] [CrossRef]
- Mukhtyar, C.; Hellmich, B.; Jayne, D.; Flossmann, O.; Luqmani, R. Remission in antineutrophil cytoplasmic antibody-associated systemic vasculitis. Clin. Exp. Rheumatol. 2006, 24, S93. [Google Scholar]
- Salama, A.D. Relapse in Anti-Neutrophil Cytoplasm Antibody (ANCA)–Associated Vasculitis. Kidney Int. Rep. 2019, 5, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majka, D.S.; Holers, V.M. Can we accurately predict the development of rheumatoid arthritis in the preclinical phase? Arthritis Rheum 2003, 48, 2701–2705. [Google Scholar] [CrossRef] [PubMed]
- Skare, T.L.; Nisihara, R.; Barbosa, B.B.; da Luz, A.; Utiyama, S.; Picceli, V. Anti-CCP in systemic lupus erythematosus patients: A cross sectional study in Brazilian patients. Clin. Rheumatol. 2013, 32, 1065–1070. [Google Scholar] [CrossRef]
- Ziegelasch, M.; Van Delft, M.A.M.; Wallin, P.; Skogh, T.; Magro-Checa, C.; Steup-Beekman, G.M.; Trouw, L.A.; Kastbom, A.; Sjöwall, C. Antibodies against carbamylated proteins and cyclic citrullinated peptides in systemic lupus erythematosus: Results from two well-defined European cohorts. Arthritis Res. Ther. 2016, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Atzeni, F.; Sarzi-Puttini, P.; Lama, N.; Bonacci, E.; Bobbio-Pallavicini, F.; Montecucco, C.; Caporali, R. Anti-cyclic citrullinated peptide antibodies in primary Sjogren’s syndrome may be associated with non-erosive synovitis. Arthritis Res. Ther. 2008, 10, R51. [Google Scholar] [CrossRef] [Green Version]
- Van Zanten, A.; Arends, S.; Roozendaal, C.; Limburg, P.C.; Maas, F.; Trouw, L.A.; Toes, R.E.M.; Huizinga, T.W.J.; Bootsma, H.; Brouwer, E. Presence of anticitrullinated protein antibodies in a large population-based cohort from the Netherlands. Ann. Rheum. Dis. 2017, 76, 1184–1190. [Google Scholar] [CrossRef]
- Correia, C.S.; Briones, M.R.; Guo, R.; Ostrowski, R.A. Elevated anti-cyclic citrullinated peptide antibody titer is associated with increased risk for interstitial lung disease. Clin. Rheumatol. 2019, 38, 1201–1206. [Google Scholar] [CrossRef]
- Alunno, A.; Bistoni, O.; Pratesi, F.; La Paglia, G.M.C.; Puxeddu, I.; Migliorini, P.; Gerli, R. Anti-citrullinated alpha enolase antibodies, interstitial lung disease and bone erosion in rheumatoid arthritis. Rheumatology 2018, 57, 850–855. [Google Scholar] [CrossRef] [Green Version]
- McAdoo, S.P.; Tanna, A.; Hrušková, Z.; Holm, L.; Weiner, M.; Arulkumaran, N.; Kang, A.; Satrapová, V.; Levy, J.; Ohlsson, S.; et al. Patients double-seropositive for ANCA and anti-GBM antibodies have varied renal survival, frequency of relapse, and outcomes compared to single-seropositive patients. Kidney Int. 2017, 92, 693–702. [Google Scholar] [CrossRef] [Green Version]
- Haschka, J.; Englbrecht, M.; Hueber, A.; Manger, B.; Kleyer, A.; Reiser, M.; Finzel, S.; Tony, H.-P.; Kleinert, S.; Feuchtenberger, M.; et al. Relapse rates in patients with rheumatoid arthritis in stable remission tapering or stopping antirheumatic therapy: Interim results from the prospective randomised controlled RETRO study. Ann. Rheum. Dis. 2015, 75, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Patients (N = 168) | ACPA-Negative AAV Patients (N = 153) | ACPA-Positive AAV Patients (N = 15) | p-Value |
|---|---|---|---|---|
| At the time of diagnosis | ||||
| Demographic data | ||||
| Age (years) | 58.6 (13.2) | 59.0 (13.2) | 54.1 (12.9) | 0.165 |
| Male gender (N, (%)) | 56 (33.3) | 53 (34.6) | 3 (20.0) | 0.390 |
| Smoking history (N, (%)) | 5 (3.0) | 5 (3.3) | 0 (0) | 1.000 |
| ACPA positivity (N, (%)) | 15 (8.9) | 0 (0.0) | 15 (100.0) | <0.001 |
| AAV subtypes (N, (%)) | 0.960 | |||
| MPA | 95 (56.5) | 86 (56.2) | 9 (60.0) | |
| GPA | 36 (21.4) | 33 (21.6) | 3 (20.0) | |
| EGPA | 37 (22.0) | 34 (22.2) | 3 (20.0) | |
| ANCA positivity (N, (%)) | ||||
| MPO-ANCA (or P-ANCA) positivity | 123 (73.2) | 112 (73.2) | 11 (73.3) | 1.000 |
| PR3-ANCA (or C-ANCA) positivity | 20 (11.9) | 18 (11.8) | 2 (13.3) | 0.694 |
| Both | 8 (4.8) | 6 (3.9) | 2 (13.3) | 0.152 |
| ANCA negative | 33 (19.6) | 29 (19.0) | 4 (26.7) | 0.498 |
| Clinical manifestations based on BVAS items (N, (%)) | ||||
| General | 70 (41.7) | 64 (41.8) | 6 (40.0) | 0.891 |
| Articular | 15 (8.9) | 12 (7.8) | 3 (20.0) | 0.136 |
| Cutaneous | 35 (20.8) | 30 (19.6) | 5 (33.3) | 0.212 |
| Mucous and ocular | 4 (2.4) | 4 (2.6) | 0 (0) | 1.000 |
| Otorhinolaryngologic | 80 (47.6) | 75 (49.0) | 5 (33.3) | 0.288 |
| Pulmonary | 109 (64.9) | 101 (66.0) | 8 (53.3) | 0.326 |
| Cardiovascular | 35 (20.8) | 33 (21.6) | 2 (13.3) | 0.739 |
| Gastrointestinal | 8 (4.8) | 8 (5.2) | 0 (0) | 1.000 |
| Renal | 99 (58.9) | 91 (59.5) | 8 (53.3) | 0.644 |
| Nervous systemic | 63 (37.5) | 56 (36.6) | 7 (46.7) | 0.442 |
| AAV-specific indices | ||||
| BVAS | 13.3 (7.4) | 13.4 (7.4) | 12.0 (7.9) | 0.491 |
| FFS | 1.3 (1.0) | 1.3 (1.0) | 1.1 (1.1) | 0.299 |
| Comorbidities (N, (%)) | ||||
| Diabetes Mellitus | 44 (26.2) | 42 (27.5) | 2 (13.3) | 0.358 |
| Hypertension | 67 (39.9) | 63 (41.2) | 4 (26.7) | 0.408 |
| Dyslipidaemia | 28 (16.7) | 25 (16.3) | 3 (20.0) | 0.718 |
| Interstitial lung disease | 48 (28.6) | 45 (29.4) | 3 (20.0) | 0.559 |
| Acute phase reactants | ||||
| ESR (mm/hr) | 59.1 (38.8) | 60.9 (38.6) | 40.8 (36.6) | 0.055 |
| CRP (mg/L) | 38.5 (51.4) | 39.8 (51.9) | 25.2 (45.4) | 0.312 |
| Medications administered during the follow-up period (N, (%)) | ||||
| Glucocorticoids | 156 (92.9) | 141 (92.2) | 15 (100) | 0.604 |
| Cyclophosphamide | 88 (52.4) | 82 (53.6) | 6 (40.0) | 0.314 |
| Rituximab | 25 (14.9) | 23 (15.0) | 2 (13.3) | 1.000 |
| Mycophenolate mofetil | 21 (12.5) | 18 (11.8) | 3 (20.0) | 0.406 |
| Azathioprine | 93 (55.4) | 87 (56.9) | 6 (40.0) | 0.210 |
| Tacrolimus | 13 (7.7) | 11 (7.2) | 2 (13.3) | 0.327 |
| Methotrexate | 15 (8.9) | 12 (7.8) | 3 (20.0) | 0.136 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.S.; Pyo, J.Y.; Song, J.J.; Park, Y.-B.; Lee, S.-W. Anti-Citrullinated Peptide Antibody Expression and Its Association with Clinical Features and Outcomes in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Medicina 2022, 58, 558. https://doi.org/10.3390/medicina58040558
Ahn SS, Pyo JY, Song JJ, Park Y-B, Lee S-W. Anti-Citrullinated Peptide Antibody Expression and Its Association with Clinical Features and Outcomes in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Medicina. 2022; 58(4):558. https://doi.org/10.3390/medicina58040558
Chicago/Turabian StyleAhn, Sung Soo, Jung Yoon Pyo, Jasong Jungsik Song, Yong-Beom Park, and Sang-Won Lee. 2022. "Anti-Citrullinated Peptide Antibody Expression and Its Association with Clinical Features and Outcomes in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis" Medicina 58, no. 4: 558. https://doi.org/10.3390/medicina58040558