
Clinical Significance of Ventricular Premature Contraction Provoked by the Treadmill Test

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
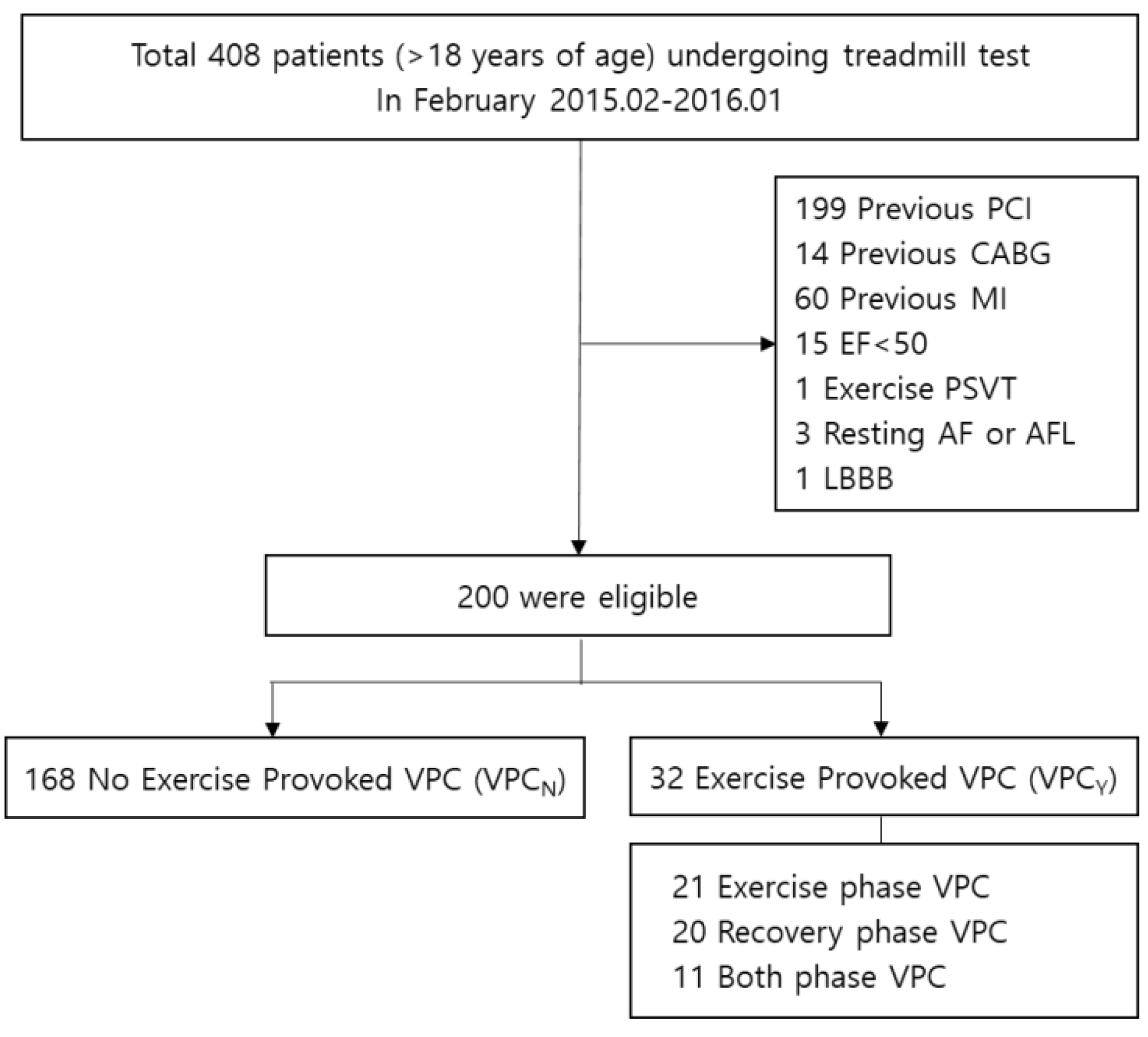
2.1. Study Population
2.2. Data Collection
2.3. Exercise Test
2.4. Classification of VPC
2.5. Statistics
3. Results
4. Discussion
Limitations
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gianrossi, R.; Detrano, R.; Mulvihill, D.; Lehmann, K.; Dubach, P.; Colombo, A.; McArthur, D.; Froelicher, V. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation 1989, 80, 87–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, D.B.; Harrell, F.E.; Lee, K.L.; Califf, R.M.; Rosati, R.A. Estimating the likelihood of significant coronary artery disease. Am. J. Med. 1983, 75, 771–780. [Google Scholar] [CrossRef]
- Gibbons, R.J.; Balady, G.J.; Bricker, J.T.; Chaitman, B.R.; Fletcher, G.F.; Froelicher, V.F.; Mark, D.B.; McCallister, B.D.; Mooss, A.N.; O’Reilly, M.G.; et al. ACC/AHA 2002 guideline update for exercise testing: Summary article. A report of the American college of cardiology/American Heart Association task force on practice guidelines (committee to update the 1997 exercise testing guidelines). J. Am. Coll. Cardiol. 2002, 40, 1531–1540. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Farzam, K.; Richards, J.R. Premature Ventricular Contraction (PVC); StatPearls: Treasure Island, San Francisco, FL, USA, 2020. [Google Scholar]
- Weiner, D.A.; Levine, S.R.; Klein, M.D.; Ryan, T.J. Ventricular arrhythmias during exercise testing: Mechanism, response to coronary bypass surgery and prognostic significance. Am. J. Cardiol. 1984, 53, 1553–1557. [Google Scholar] [CrossRef]
- Marieb, M.A.; Beller, G.A.; Gibson, R.S.; Lerman, B.B.; Kaul, S. Clinical relevance of exercise-induced ventricular arrhythmias in suspected coronary artery disease. Am. J. Cardiol. 1990, 66, 172–178. [Google Scholar] [CrossRef]
- Schweikert, R.A.; Pashkow, F.J.; Snader, C.E.; Marwick, T.H.; Lauer, M.S. Association of exercise-induced ventricular ectopic activity with thallium myocardial perfusion and angiographic coronary artery disease in stable, low-risk populations. Am. J. Cardiol. 1999, 83, 530–534. [Google Scholar] [CrossRef]
- Casella, G.; Pavesi, P.C.; Sangiorgio, P.; Rubboli, A.; Bracchetti, D. Exercise-induced ventricular arrhythmias in patients with healed myocardial infarction. Int. J. Cardiol. 1993, 40, 229–235. [Google Scholar] [CrossRef]
- Beckerman, J.; Mathur, A.; Stahr, S.; Myers, J.; Chun, S.; Froelicher, V. Exercise-induced ventricular arrhythmias and cardiovascular death. Ann. Noninvasive Electrocardiol. 2005, 10, 47–52. [Google Scholar] [CrossRef]
- Jouven, X.; Zureik, M.; Desnos, M.; Courbon, D.; Ducimetière, P. Long-term outcome in asymptomatic men with exercise-induced premature ventricular depolarizations. New Engl. J. Med. 2000, 343, 826–833. [Google Scholar] [CrossRef]
- Morshedi-Meibodi, A.; Evans, J.C.; Levy, D.; Larson, M.; Vasan, R.S. Clinical correlates and prognostic significance of exercise-induced ventricular premature beats in the community: The framingham heart study. Circulation 2004, 109, 2417–2422. [Google Scholar] [CrossRef] [Green Version]
- Partington, S.; Myers, J.; Cho, S.; Froelicher, V.; Chun, S. Prevalence and prognostic value of exercise-induced ventricular arrhythmias. Am. Hear. J. 2003, 145, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Marine, J.E.; Shetty, V.; Chow, G.V.; Wright, J.G.; Gerstenblith, G.; Najjar, S.S.; Lakatta, E.G.; Fleg, J.L. Prevalence and prognostic significance of exercise-induced nonsustained ventricular tachycardia in asymptomatic volunteers: BLSA (Baltimore Longitudinal Study of Aging). J. Am. Coll. Cardiol. 2013, 62, 595–600. [Google Scholar] [CrossRef] [Green Version]
- Sami, M.; Chaitman, B.; Fisher, L.; Holmes, D.; Fray, D.; Alderman, E. Significance of exercise-induced ventricular arrhythmia in stable coronary artery disease: A coronary artery surgery study project. Am. J. Cardiol. 1984, 54, 1182–1188. [Google Scholar] [CrossRef]
- McHenry, P.L.; Morris, S.N.; Kavalier, M.; Jordan, J.W. Comparative study of exercise-induced ventricular arrhythmias in normal subjects and patients with documented coronary artery disease. Am. J. Cardiol. 1976, 37, 609–616. [Google Scholar] [CrossRef]
- Bruce, R.A.; DeRouen, T.A.; Hossack, K.F.; Blake, B.; Hofer, V.R. Value of maximal exercise tests in risk assessment of primary coronary heart disease events in healthy men: Five years’ experience of the Seattle heart watch study. Am. J. Cardiol. 1980, 46, 371–378. [Google Scholar] [CrossRef]
- Drory, Y.; Pines, A.; Fisman, E.Z.; Kellermann, J.J. Persistence of arrhythmia exercise response in healthy young men. Am. J. Cardiol. 1990, 66, 1092–1094. [Google Scholar] [CrossRef]
- Elhendy, A.; Chandrasekaran, K.; Gersh, B.J.; Mahoney, D.; Burger, K.N.; Pellikka, P.A. Functional and prognostic significance of exercise-induced ventricular arrhythmias in patients with suspected coronary artery disease. Am. J. Cardiol. 2002, 90, 95–100. [Google Scholar] [CrossRef]
- Meine, T.J.; Patel, M.R.; Shaw, L.K.; Borges-Neto, S. Relation of ventricular premature complexes during recovery from a myocardial perfusion exercise stress test to myocardial ischemia. Am. J. Cardiol. 2006, 97, 1570–1572. [Google Scholar] [CrossRef]
- Lanza, G.A.; De Vita, A.; Kaski, J.-C. ‘Primary’ microvascular angina: Clinical characteristics, pathogenesis and management. Interv. Cardiol. Rev. 2018, 13, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Dewey, F.E.; Kapoor, J.R.; Williams, R.S.; Lipinski, M.J.; Ashley, E.A.; Hadley, D.; Myers, J.; Froelicher, V.F. Ventricular arrhythmias during clinical treadmill testing and prognosis. Arch. Intern. Med. 2008, 168, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, I.S.; Prineas, R.J.; Neaton, J.D.; Jacobs, D.R.J.; Crow, R.S. Crow RS: Relation between ventricular premature complexes and sudden cardiac death in apparently healthy men. Am. J. Cardiol. 1987, 60, 1036. [Google Scholar] [CrossRef]
- Spirito, P.; Chiarella, F.; Carratino, L.; Berisso, M.Z.; Bellotti, P.; Vecchio, C. Clinical course and prognosis of hypertrophic cardiomyopathy in an outpatient population. N. Engl. J. Med. 1989, 320, 749–755. [Google Scholar] [CrossRef]
- Fontaine, G.; Fontaliran, F.; Frank, R. Arrhythmogenic right ventricular cardiomyopathies: Clinical forms and main differential diagnoses. Circulation 1998, 97, 1532–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourque, J.M.; Beller, G.A. Value of exercise ECG for risk stratification in suspected or known CAD in the era of advanced imaging technologies. JACC Cardiovasc. Imaging 2015, 8, 1309–1321. [Google Scholar] [CrossRef] [Green Version]
- Klem, I.; Heitner, J.F.; Shah, D.J.; Sketch, M.H.; Behar, V.; Weinsaft, J.; Cawley, P.; Parker, M.; Elliott, M.; Judd, R.M.; et al. Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhancement infarction imaging. J. Am. Coll. Cardiol. 2006, 47, 1630–1638. [Google Scholar] [CrossRef] [Green Version]
- Dang, G.; Shahreyar, M.; Oktay, A.A.; Sulaiman, S.; Husein, H.; Inashvili, A.; Elhangouche, N.; Subramanian, P.; Bashir, M.W.; Pathak, A.; et al. Positive predictive value of noninvasive stress testing is poor in the real world. Crit. Pathw. Cardiol. 2018, 17, 38–42. [Google Scholar] [CrossRef]


{kind=link}
| VPCY (n = 32) | VPCN (n = 168) | p Value (VPCY vs. VPCN) | VPCE+ (n = 21) | p Value (VPCE vs. Others) | VPCR (n = 20) | p Value (VPCR vs. Others) | |
|---|---|---|---|---|---|---|---|
| Demographics | |||||||
| Age | 56.4 ± 16.6 | 52.7 ± 14.0 | 0.180 | 57.7 ± 16.1 | 0.139 | 53.8 ± 17.9 | 0.869 |
| Sex (male) | 27 (84.4%) | 122 (72.6%) | 0.162 | 3 (14.3%) | 0.213 | 5 (25.0%) | 0.957 |
| Height | 167.0 ± 7.7 | 167.0 ± 8.7 | 0.988 | 166.3 ± 8.0 | 0.696 | 165.7 ± 7.2 | 0.495 |
| Weight | 68.4 ± 9.4 | 68.7 ± 11.9 | 0.888 | 69.8 ± 10.2 | 0.649 | 67.3 ± 10.1 | 0.586 |
| BMI | 24.5 ± 2.8 | 24.6 ± 3.1 | 0.951 | 25.2 ± 2.8 | 0.319 | 24.5 ± 2.7 | 0.907 |
| Family Hx | |||||||
| FHxCAD | 4 (12.5%) | 14 (8.3%) | 0.498 | 4 (19.0%) | 0.103 | 3 (15.0%) | 0.399 |
| FHxSCD | 3 (9.4%) | 3 (1.8%) | 0.053 | 1 (4.8%) | 0.491 | 3 (15.0%) | 0.014 |
| Pre. Medical Hx | |||||||
| DM | 5 (15.6%) | 23 (13.7%) | 0.782 | 3 (14.3%) | 1.000 | 3 (15.0%) | 1.000 |
| HTN | 12 (37.5%) | 71 (42.3%) | 0.616 | 9 (42.9%) | 0.894 | 9 (45.0%) | 0.738 |
| Dyslipidemia | 7 (21.9%) | 55 (32.7%) | 0.223 | 3 (14.3%) | 0.080 | 6 (30.0%) | 0.919 |
| CVA | 3 (9.4%) | 7 (4.2%) | 0.202 | 2 (9.5%) | 0.283 | 2 (10.0%) | 0.263 |
| PAD | 2 (6.2%) | 14 (8.3%) | 1.000 | 2 (9.5%) | 0.678 | 2 (10.0%) | 0.665 |
| Clinical finding | |||||||
| Resting HR | 79.7 ± 11.5 | 77.0 ± 14.2 | 0.299 | 79.3 ± 11.5 | 0.497 | 78.5 ± 11.8 | 0.719 |
| Resting SBP | 127.8 ± 18.2 | 124.5 ± 19.0 | 0.379 | 131.3 ± 18.5 | 0.110 | 126.0 ± 17.5 | 0.814 |
| ECG finding | |||||||
| QRS duration | 95.5 ± 21.3 | 95.3 ± 15.8 | 0.953 | 97.4 ± 25.8 | 0.551 | 93.8 ± 13.8 | 0.673 |
| QTc | 422.6 ± 34.6 | 424.3 ± 27.8 | 0.754 | 426.5 ± 35.2 | 0.683 | 425.9 ± 38.1 | 0.762 |
| VPC at rest | 7 (21.9%) | 3 (1.8%) | 0.000 | 6 (28.6%) | 0.000 | 5 (25.0%) | 0.001 |
| Exercise test | |||||||
| Maximal HR | 157.0 ± 23.2 | 156.8 ± 25.1 | 0.954 | 154.1 ± 20.7 | 0.604 | 158.1 ± 24.7 | 0.805 |
| Maximal SBP | 190.1 ± 32.4 | 180.3 ± 27.3 | 0.074 | 190.8 ± 35.0 | 0.130 | 185.9 ± 33.5 | 0.507 |
| Exercise capacity | 11.3 ± 2.3 | 11.6 ± 2.1 | 0.468 | 11.4 ± 2.0 | 0.809 | 11.2 ± 2.7 | 0.402 |
| TMT positive | 5 (15.6%) | 15 (8.9%) | 0.329 | 5 (23.8%) | 0.042 | 3 (15.0%) | 0.430 |
| TMT Positive Result | ||
|---|---|---|
| Univariable | Multivariable | |
| Age | 1.105 (1.030–1.186) | 1.118 (1.036–1.207) |
| Sex | 0.182 (0.023–1.426) | |
| BMI | 1.012 (0.855–1.199) | |
| DM | 1.892 (0.483–7.410) | |
| HTN | 2.571 (0.901–7.343) | |
| Dyslipidemia | 2.538 (0.890–7.237) | |
| CVA | 6.429 (0.989–41.790) | |
| PAD | 1.248 (0.144–10.843) | |
| Exercise phase VPC | 4.778 (1.279–17.849) | 6.879 (1.458–32.453) |
| Recovery phase VPC | 1.500 (0.304–7.396) | |
| Coronary Artery Disease | Revascularization | |||
|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |
| Age | 1.095 (1.028–1.165) | 1.108 (1.026–1.196) | 1.083 (0.984–1.192) | |
| Sex | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | ||
| BMI | 1.045 (0.857–1.275) | 0.967 (0.697–1.342) | ||
| TMT positive result | 1.930 (0.566–6.581) | 7.547 (1.812–31.434) | 2.267 (0.312–16.472) | 8.797 (1.073–72.127) |
| Exercise phase VPC | 1.988 (0.400–9.886) | 2.933 (0.291–29.550) | ||
| Recovery phase VPC | 2.111 (0.423–10.533) | 9.889 (1.313–74.473) | 9.381 (1.144–76.948) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bak, M.-J.; Kwon, H.-J.; Choi, J.-H.; Park, S.-J.; Kim, J.-S.; On, Y.-K.; Park, K.-M. Clinical Significance of Ventricular Premature Contraction Provoked by the Treadmill Test. Medicina 2022, 58, 556. https://doi.org/10.3390/medicina58040556
Bak M-J, Kwon H-J, Choi J-H, Park S-J, Kim J-S, On Y-K, Park K-M. Clinical Significance of Ventricular Premature Contraction Provoked by the Treadmill Test. Medicina. 2022; 58(4):556. https://doi.org/10.3390/medicina58040556
Chicago/Turabian StyleBak, Min-Jung, Hee-Jin Kwon, Ji-Hoon Choi, Seung-Jung Park, June-Soo Kim, Young-Keun On, and Kyoung-Min Park. 2022. "Clinical Significance of Ventricular Premature Contraction Provoked by the Treadmill Test" Medicina 58, no. 4: 556. https://doi.org/10.3390/medicina58040556