
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Neurological Entity?

 ,
, {kind=link}
Abstract
:1. Introduction
2. Development
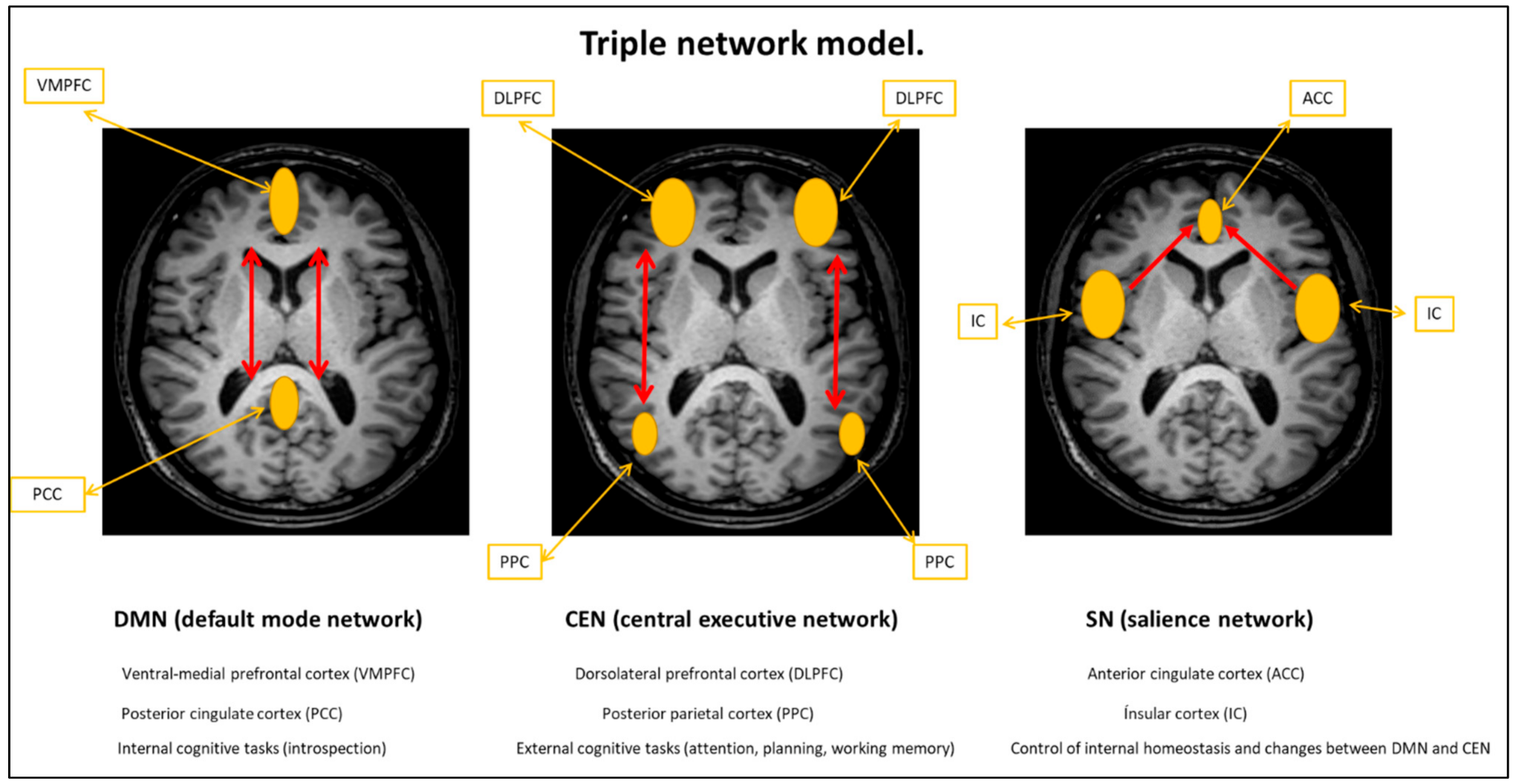
3. Neuroimaging
4. Dysautonomia
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The Chronic Fatigue Syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Pigeon, W.R.; Sateia, M.J.; Ferguson, R.J. Distinguishing between excessive daytime sleepiness and fatigue: Toward improved detection and treatment. J. Psychosom. Res. 2003, 54, 61–69. [Google Scholar] [CrossRef]
- Watanabe, T.; Evengård, B.; Natelson, B.H.; Jason, L.A.; Kuratsune, H. Preface and Mini-Review: Fatigue Science for Human Health; Springer: New York, NY, USA, 2007; pp. 5–11. [Google Scholar]
- Arruti, M.; Avellaneda, A.; Barbado, F.J.; De la Cruz, J.; Díaz-Delgado, R.; Gutierrez, E.; Izquierdo, M.; Palacín, C.; Pérez, A.; Ramón, J.R.; et al. Spanish Consensus Document Chronic Fatigue Syndrome. SEMERGEN—Med. Fam. 2008, 35, 385–405. [Google Scholar]
- Johnston, S.; Brenu, E.W.; Staines, D.R.; Marshall-Gradisnik, S. The adoption of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis case definitions to assess prevalence: A systematic review. Ann. Epidemiol. 2013, 23, 371–376. [Google Scholar] [CrossRef]
- World Health Organization. Chapter VIII: Diseases of the nervous system (Others disorders of the nervous system) (ICD-11). In International Statistical Classification of Diseases and Related Health Problems, 11th ed.; Code 8E49; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Wojcik, W.; Armstrong, D.; Kanaan, R. Is Chronic Fatigue Syndrome a neurological condition? A survey of UK neurologists. J. Psychosom. Res. 2011, 70, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Afari, N.; Buchwald, D. Chronic Fatigue Syndrome: A review. Am. J. Psychiatry 2003, 160, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Prins, J.B.; van der Meer, J.W.; Bleijenberg, G. Chronic Fatigue Syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Jason, L.A.; Richman, J.A.; Rademaker, A.W.; Jordan, K.M.; Plioplys, A.V.; Taylor, R.R.; McCready, W.; Huang, C.F.; Plioplys, S. Community-based study of Chronic Fatigue Syndrome. Arch. Intern. Med. 1999, 159, 2129–2137. [Google Scholar] [CrossRef]
- Bierl, C.; Nisenbaum, R.; Hoaglin, D.C.; Randall, B.; Jones, A.B.; Unger, E.R.; Reeves, W.C. Regional distribution of fatiguing illnesses in the United States: A pilot study. Popul. Health Metrics 2004, 2, 1. [Google Scholar] [CrossRef]
- Jason, L.A.; Benton, M.C.; Valentine, L.; Johnson, A.; Torres-Harding, S. The economic impact of ME/CFS: Individual and societal costs. Dyn. Med. 2008, 7, 6. [Google Scholar] [CrossRef]
- Fischer, D.B.; William, A.H.; Strauss, A.C.; Unger, E.R.; Jason, L.A.; Marshall, G.D.; Dimitrakoff, J.D. Chronic Fatigue Syndrome: The current status and future potentials of emerging biomarkers. Fatigue Biomed. Health Behav. 2014, 2, 93–109. [Google Scholar] [CrossRef]
- Brurberg, K.G.; Fønhus, M.S.; Larun, L.; Flottorp, S.; Malterud, K. Case definitions for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME): A systematic review. BMJ Open 2014, 4, e003973. [Google Scholar] [CrossRef]
- Murga, I.; Lafuente, J.V. De la neurastenia a la enfermedad postesfuerzo: Evolución de los criterios diagnósticos del Síndrome de Fatiga Crónica/Encefalomielitis Miálgica. Atención Primaria 2019, 51, 579–585. [Google Scholar] [CrossRef]
- Clayton, E.W.; Alegría, M.; Bateman, L.; Chu, L.; Cleeland, C.; Ronald, W.D.; Diamond, B.; Ganiats, T.; Keller, B.; Klimas, N.; et al. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Redefining an Illness; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Morris, G.; Maes, M. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Encephalomyelitis Disseminata/Multiple Sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. BMC Med. 2013, 11, 205. [Google Scholar] [CrossRef]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic Encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Francás, N.S. Percepción de Fatiga Central en la Enfermedad de Parkinson: Factores Clínicos, Psicopatológicos y Neuropsicológicos. Ph.D. Thesis, Universitát Autónoma de Barcelona, Barcelona, Spain, 2012; pp. 33–91. [Google Scholar]
- Chaudhuri, A.; Behan, P.O. Fatigue in neurological disorders. Lancet 2004, 63, 978–988. [Google Scholar] [CrossRef]
- Nakagawa, S.; Takeuchi, H.; Taki, Y.; Nouchi, R.; Kotozaki, Y.; Shinada, T.; Maruyama, T.; Sekiguchi, A.; IiZuka, K.; Yokoyama, R.; et al. Basal ganglia correlates of fatigue in young adults. Sci. Rep. 2016, 6, 21386. [Google Scholar] [CrossRef] [PubMed]
- Maestú, F.; Pereda, E.; del Pozo, F. Conectividad Funcional y Anatómica en el Cerebro Humano; Elsevier: Amsterdam, The Netherlands, 2015; p. 149. [Google Scholar]
- Vercruysse, P.; Vieau, D.; Blum, D.; Petersén, Å.; Dupuis, L. Hypothalamic alterations in neurodegenerative diseases and their relation to abnormal energy metabolism. Front. Mol. Neurosci. 2018, 11, 2. [Google Scholar] [CrossRef]
- Jackson, M.L.; Bruck, D. Sleep abnormalities in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: A review. J. Clin. Sleep Med. 2012, 8, 719–728. [Google Scholar] [CrossRef]
- Mariman, A.N.; Vogelaers, D.P.; Tobback, E.; Delesie, L.M.; Hanoulle, I.P.; Pevernagie, D.A. Sleep in the Chronic Fatigue Syndrome. Sleep Med. Rev. 2013, 17, 193–199. [Google Scholar] [CrossRef]
- Cambras, T.; Castro-Marrero, J.; Zaragoza, M.C.; Diez-Noguera, A.; Alegre, J. Circadian rhythm abnormalities and autonomic dysfunction in patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. PLoS ONE 2018, 13, e0198106. [Google Scholar] [CrossRef]
- Reeves, W.; Lloyd, A.; Vernon, S.D.; Klimas, N.; Jason, L.A.; Bleijenberg, G.; Evengard, B.; White, P.D.; Nisenbaum, R.; Unger, E.R.; et al. Identification of ambiguities in 1994 Chronic Fatigue Syndrome research case definition and recommendations. BMC Health Serv. Res. 2003, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.Y.; Kwiatek, R.; Burnet, R.; Del Fante, P.; Staines, D.R.; Marshall-Gradisnik, S.M.; Barnden, L.R. Progressive brain changes in patients with Chronic Fatigue Syndrome: A Longitudinal MRI study. J. Magn. Reson. Imaging 2016, 44, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Barnden, L.R.; Shan, Z.Y.; Staines, D.R.; Marshall-Gradisnik, S.; Finegan, K.; Ireland, T.; Bhuta, S. Hyperintense sensorimotor T1 spin echo MRI is associated with brainstem abnormality in Chronic Fatigue Syndrome. NeuroImage Clin. 2018, 20, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Finkelmeyer, A.; He, J.; Maclachlan, L.; Watson, S.; Gallagher, P.; Newton, J.L.; Blamire, A.M. Grey and white matter differences in Chronic Fatigue Syndrome—A voxel-based morphometry study. Neuroimage Clin. 2018, 17, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Barnden, L.R.; Crouch, B.; Kwiatek, R.; Burnet, R.; Del Fante, P. Evidence in Chronic Fatigue Syndrome for severity-dependent upregulation of prefrontal myelination that is independent of anxiety and depression. NMR Biomed. 2015, 28, 404–413. [Google Scholar] [CrossRef]
- Zeineh, M.M.; Kang, J.; Atlas, S.W.; Raman, M.M.; Reiss, A.L.; Norris, J.L.; Valencia, I.; Montoya, J.G. Right Arcuate Fasciculus abnormality in Chronic Fatigue Syndrome. Radiology 2015, 274, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Caseras, X.; Mataix-Cols, D.; Giampietro, V.; Rimes, K.A.; Brammer, M.; Zelaya, F.; Chalder, T.; Godfrey, E.L. Probing the working memory system in Chronic Fatigue Syndrome: A functional magnetic resonance imaging study using the n-back task. Psychosom. Med. 2006, 68, 947–955. [Google Scholar] [CrossRef]
- Gay, C.W.; Robinson, M.E.; Lai, S.; O´Shea, A.; Craggs, J.G.; Price, D.D.; Staud, R. Abnormal resting-state functional connectivity in patients with Chronic Fatigue Syndrome: Results of seed and data-driven analyses. Brain Connect. 2016, 6, 48–56. [Google Scholar] [CrossRef]
- Chen, C. Neurometabolites in anterior cingulate cortex in Chronic Fatigue Syndrome: A magnetic resonance spectroscopy study at 7 Tesla. Master’s Thesis, University of Oxford, Oxford, UK, 2017; p. 49. [Google Scholar]
- Shan, Z.Y.; Finegan, K.; Bhuta, S.; Ireland, T.; Staines, D.; Marshall-Gradisnik, S.; Barnden, L.R. Brain function characteristics of Chronic Fatigue Syndrome: A task fMRI study. NeuroImage Clin. 2018, 19, 279–286. [Google Scholar] [CrossRef]
- Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef]
- Zinn, M.A.; Zinn, M.L.; Jason, L.A. Small-World network analysis of cortical connectivity in CFS using quantitative EEG. NeuroRegulation 2017, 4, 125–137. [Google Scholar] [CrossRef]
- Zinn, M.A.; Zinn, M.L.; Valencia, I.; Jason, L.A.; Montoya, J.G. Cortical hypoactivation during resting EEG suggests central nervous system pathology in patients with Chronic Fatigue Syndrome. Biol. Psychol. 2018, 136, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Zinn, M.L.; Zinn, M.A.; Jason, L.A. Intrinsic functional hypoconnectivity in core neurocognitive networks suggests central nervous system pathology in patients with Myalgic Encephalomyelitis: A Pilot Study. Appl. Psychophysiol. Biofeedback 2016, 41, 283–300. [Google Scholar] [CrossRef] [PubMed]
- Biswal, B.; Kunwar, P.; Natelson, B.H. Cerebral blood flow is reduced in Chronic Fatigue Syndrome as assessed by Arterial Spin Labeling. J. Neurol. Sci. 2011, 301, 9–11. [Google Scholar] [CrossRef]
- He, J.; Hollingsworth, K.G.; Newton, J.L.; Blamire, A.M. Cerebral vascular control is associated with skeletal muscle pH in Chronic Fatigue Syndrome patients both at rest and during dynamic stimulation. Neuroimage Clin. 2013, 2, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Natelson, B.H.; Mao, X.; Stegner, A.J.; Lange, G.; Vu, D.; Blate, M.; Kang, G.; Soto, E.; Kapusuz, T.; Shungu, D.C. Multimodal and simultaneous assessments of brain and spinal fluid abnormalities in Chronic Fatigue Syndrome and the effects of psychiatric comorbidity. J. Neurol. Sci. 2017, 375, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Mathew, S.J.; Mao, X.; Keegan, K.A.; Levine, S.M.; Smith, E.L.; Heier, L.A.; Otcheretko, V.; Coplan, J.D.; Shungu, D.C. Ventricular cerebrospinal fluid lactate is increased in Chronic Fatigue Syndrome compared with generalized anxiety disorder: An in vivo 3.0 T (1)H MRS imaging study. NMR Biomed. 2009, 22, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Murrough, J.W.; Mao, X.; Collins, K.A.; Kelly, C.; Andrade, G.; Nestadt, P.; Levine, S.M.; Mathew, S.J.; Shungu, D.C. Increased ventricular lactate in Chronic Fatigue Syndrome measured by 1H MRS imaging at 3.0 T. II: Comparison with major depressive disorder. NMR Biomed. 2010, 23, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Shungu, D.C.; Weiduschat, N.; Murrough, J.W.; Mao, X.; Pillemer, S.; Dyke, J.P.; Medow, M.S.; Natelson, B.H.; Stewart, J.M.; Mathew, S.J. Increased ventricular lactate in Chronic Fatigue Syndrome. Relationships to cortical glutathione and clinical symptoms implicate oxidative stress in disorder pathophysiology. NMR Biomed. 2012, 25, 1073–1087. [Google Scholar] [CrossRef]
- Natelson, B.H.; Vu, D.; Coplan, J.D.; Mao, X.; Blate, M.; Kang, G.; Soto, E.; Kapusuz, T.; Shungu, D.C. Elevations of ventricular lactate levels occur in both Chronic Fatigue Syndrome and Fibromyalgia. Fatigue Biomed. Health Behav. 2017, 5, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Bradley, K.A.L.; Mao, X.; Case, J.A.C.; Kang, G.; Shungu, D.C.; Gabbay, V. Increased ventricular cerebrospinal fluid lactate in depressed adolescents. Eur. Psychiatry 2016, 32, 1–8. [Google Scholar] [CrossRef] [PubMed]
- van der Schaaf, M.E.; De Lange, F.P.; Schmits, I.C.; Geurts, D.E.M.; Roelofs, K.; van der Meer, J.W.M.; Toni, I.; Knoop, H. Prefrontal structure varies as a function of pain symptoms in Chronic Fatigue Syndrome. Biol. Psychiatry 2017, 81, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Nakatomi, Y.; Mizuno, K.; Ishii, R.; Wada, Y.; Tanaka, M.; Tazawa, S.; Onoe, K.; Fukuda, S.; Kawabe, J.; Takahashi, K.; et al. Neuroinflammation in patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: An 11C-(R)-PK11195 PET study. J. Nucl. Med. 2014, 55, 945–950. [Google Scholar] [CrossRef]
- Nakatomi, Y.; Kuratsune, H.; Watanabe, Y. Neuroinflammation in the brain of patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Brain Nerve 2018, 70, 19–25. [Google Scholar]
- Yamamoto, S.; Ouchi, Y.; Nakatsuka, D.; Tahara, T.; Mizuno, K.; Tajima, S.; Onoe, H.; Yoshikawa, E.; Tsukada, H.; Iwase, M.; et al. Reduction of [11C](+)3-MPB binding in brain of Chronic Fatigue Syndrome with serum autoantibody against muscarinic cholinergic receptor. PLoS ONE 2012, 7, e51515. [Google Scholar] [CrossRef]
- Finkelmeyer, A.; He, J.; Maclachlan, L.; Blamire, A.M.; Newton, J.L. Intracranial compliance is associated with symptoms of orthostatic intolerance in Chronic Fatigue Syndrome. PLoS ONE 2018, 13, e0200068. [Google Scholar] [CrossRef]
- Barnden, R.L.; Shan, Z.Y.; Staines, D.R.; Marshall-Gradisnik, S.; Finegan, K.; Ireland, T.; Bhuta, S. Intra brainstem connectivity is impaired in Chronic Fatigue Syndrome. NeuroImage Clin. 2019, 24, 102045. [Google Scholar] [CrossRef]
- Newton, J.L.; Okonkwo, O.; Sutcliffe, K.; Seth, A.; Shin, J.; Jones, D.E.J. Symptoms of autonomic dysfunction in Chronic Fatigue Syndrome. QJM Int. J. Med. 2007, 100, 519–526. [Google Scholar] [CrossRef]
- Robinson, L.J.; Durham, J.; MacLachlan, L.L.; Newton, J.L. Autonomic function in Chronic Fatigue Syndrome with and without painful temporomandibular disorder. Fatigue Biomed. Health Behav. 2015, 3, 205–219. [Google Scholar] [CrossRef]
- Low, P.A.; Benarroch, E.E. Clinical Autonomic Disorders; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Van Cauwenbergh, D.; Nijs, J.; Koss, D.; Van Weijnen, L.; Struyf, F.; Meeus, M. Malfunctioning of the autonomic nervous system in patients with Chronic Fatigue Syndrome: A systematic literature review. Eur. J. Clin. Investig. 2014, 44, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Garner, R.; Baraniuk, J.N. Orthostatic intolerance in Chronic Fatigue Syndrome. J. Transl. Med. 2019, 17, 185. [Google Scholar] [CrossRef]
- Clark, J.E.; Ng, W.F.; Rushton, S.; Watson, S.; Newton, J.L. Network structure underpinning (dys)homeostasis in Chronic Fatigue Syndrome; Preliminary findings. PLoS ONE 2019, 14, e0213724. [Google Scholar]
- Ahmed, N.S.; Gottlob, I.; Proudlock, F.A.; Hutchinson, C.V. Restricted spatial windows of visibility in Myalgic Encephalomyelitis (ME). Vision 2018, 2, 2. [Google Scholar] [CrossRef] [PubMed]
- Sletten, D.M.; Suarez, G.A.; Low, P.A.; Mandrekar, J.; Singer, W. COMPASS 31: A refined and abbreviated Composite Autonomic Symptom score. Mayo Clin. Proc. 2012, 87, 1196–1201. [Google Scholar] [CrossRef]
- Meeus, M.; Goubert, D.; Backer, F.D.; Struyf, F.; Hermans, L.; Coppieters, I.; Wandele, I.D.; Silva, H.D.; Calders, P. Heart rate variability in patients with Fibromyalgia and patients with Chronic Fatigue Syndrome: A systematic review. Semin. Arthritis Rheum. 2013, 43, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.; Mora, T.; Vargas, A.; Fuentes-Iniestra, M.; Martinez-Kavin, M. Sympathetic nervous system dysfunction in Fibromyalgia, Chronic Fatigue Syndrome, Irritable Bowel Syndrome, and Interstitial Cystitis: A review of case-control studies. J. Clin. Rheumatol. 2014, 20, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Cvejic, E.; Sandler, C.X.; Keech, A.; Barry, B.K.; Lloyd, A.R.; Vollmer-Conna, U. Autonomic nervous system function, activity patterns, and sleep after physical or cognitive challenge in people with Chronic Fatigue Syndrome. J. Psychosom. Res. 2017, 103, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Orjatsalo, M.; Alakuijala, A.; Pertinen, M. Autonomic Nervous System functioning related to nocturnal sleep in patients with Chronic Fatigue Syndrome compared to tired controls. J. Clin. Sleep Med. 2018, 14, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N. Objective evidence of Post-exertional “Malaise” in Myalgic Encephalomyelitis and Chronic Fatigue Syndrome. J. Sports Med. Doping Stud. 2015, 5, 159. [Google Scholar] [CrossRef]
- Lengert, N.; Drossel, B. In silico analysis of exercise intolerance in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Biophys. Chem. 2015, 202, 21–31. [Google Scholar] [CrossRef]
- Cook, D.B.; Light, A.R.; Light, K.C.; Broderick, G.; Shields, M.R.; Dougherty, R.J.; Meyer, J.D.; VanRiper, S.; Stegner, A.J.; Ellingson, L.D.; et al. Neural consequences of post-exertion Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Brain Behav. Immun. 2017, 62, 87–99. [Google Scholar] [CrossRef]
- Löbel, M.; Grabowski, P.; Heidecke, H.; Bauer, S.; Hanitsch, L.G.; Wittke, K.; Meisel, C.; Reinke, P.; Volk, H.D.; Fluge, O.; et al. Antibodies to beta adrenergic and muscarinic cholinergic receptors in patients with Chronic Fatigue Syndrome. Brain Behav. Immun. 2016, 52, 32–39. [Google Scholar] [CrossRef]
- Noda, M.; Ifuku, M.; Hossain, M.S.; Katafuchi, T. Glial activation and expression of the serotonin transporter in Chronic Fatigue Syndrome. Front. Psychiatry 2018, 9, 589. [Google Scholar] [CrossRef]
- Balinas, C.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. Transient receptor potential melastatin-2 channels are overexpressed in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome patients. J. Transl. Med. 2019, 17, 401. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Nutt, D.J. Serotonin and brain function: A tale of two receptors. J. Psychopharmacol. 2017, 31, 1091–1120. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ouchi, Y.; Onoe, H.; Yoshikawa, E.; Tsukada, H.; Takahashi, H.; Iwase, M.; Yamaguti, K.; Kuratsune, H.; Watanabe, Y. Reduction of serotonin transporters of patients with Chronic Fatigue Syndrome. NeuroReport 2004, 15, 2571–2574. [Google Scholar] [CrossRef] [PubMed]
- Cleare, A.J.; Messa, C.; Rabiner, E.A.; Grasby, P.M. Brain 5-HT1A receptor binding in Chronic Fatigue Syndrome measured using Positron Emission Tomography and [11C]WAY-100635. Biol. Psychiatry 2005, 57, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Bozzini, S.; Boiocchi, C.; Carlo-Stella, N.; Ricevuti, G.; Cuccia, M. The possible underworld of Chronic Fatigue Syndrome: From neurotransmitters polymorphisms to disease. J. Neurol. Res. 2012, 2, 16–24. [Google Scholar] [CrossRef]
- Tanaka, S.; Kuratsune, H.; Hidaka, Y.; Hakariya, Y.; Tatsumi, K.I.; Takano, T.; Kanakura, Y.; Amino, N. Autoantibodies against muscarinic cholinergic receptor in Chronic Fatigue Syndrome. Int. J. Mol. Med. 2003, 12, 225–230. [Google Scholar] [CrossRef]
- Maes, M.; Ringel, K.; Kubera, M.; Anderson, G.; Morris, G.; Galecki, P.; Geffard, M. In Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, increased autoimmune activity against 5-HT is associated with immuno-inflammatory pathways and bacterial translocation. J. Affect. Disord. 2013, 150, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Sotzny, F.; Blanco, J.; Capelli, E.; Castro-Marrero, J.; Steiner, S.; Murovska, M.; Scheibenbogen, C.; European Network on ME/CFS (EUROMENE). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Evidence for an autoimmune disease. Autoimmun. Rev. 2018, 17, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Scheibenbogen, C.; Löbel, M.; Freitag, H.; Krueger, A.; Bauer, S.; Antelmann, M.; Doehner, W.; Scherbakov, N.; Heidecke, H.; Reinke, P.; et al. Immunoadsorption to remove ß2 adrenergic receptor antibodies in Chronic Fatigue Syndrome CFS/ME. PLoS ONE 2018, 13, e0193672. [Google Scholar] [CrossRef]
- Giannoccaro, P.M.; Cossins, J.; Sørland, K.; Fluge, Ø.; Vincent, A. Searching for serum antibodies to neuronal proteins in patients with Myalgic Encephalopathy/Chronic Fatigue Syndrome. Clin. Ther. 2019, 41, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, I.; Palmer, J.; Apostolou, E.; Gottfries, C.-G.; Rizwan, M.; Dahle, C.; Rosén, A. Metabolic dysfunction in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome not due to anti-mitochondrial antibodies. Front. Med. 2020, 7, 108. [Google Scholar] [CrossRef] [PubMed]
- Lebow, M.A.; Chen, A. Overshadowed by the amygdala: The bed nucleus of the stria terminalis emerges as key to psychiatric disorders. Mol. Psychiatry 2016, 21, 450–463. [Google Scholar] [CrossRef]
- Mudie, K.; Estévez-López, F.; Sekulic, S.; Ivanovs, A.; Sepulveda, N.; Zalewski, P.; Mengshoel, A.M.; De Korwin, J.D.; Capo, N.H.; Alegre-Martin, J.; et al. Recommendations for Epidemiological Research in ME/CFS from the EUROMENE Epidemiology Working Group. Preprints 2020. [Google Scholar] [CrossRef]
- Nacul, L.; Authier, F.J.; Scheibenbogen, C.; Lorusso, L.; Helland, I.B.; Alegre-Martin, J.; Sirbu, C.A.; Mengshoel, A.M.; Polo, O.; Behrends, U.; et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina 2021, 57, 510. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murga Gandasegui, I.; Aranburu Laka, L.; Gargiulo, P.-Á.; Gómez-Esteban, J.-C.; Lafuente Sánchez, J.-V. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Neurological Entity? Medicina 2021, 57, 1030. https://doi.org/10.3390/medicina57101030
Murga Gandasegui I, Aranburu Laka L, Gargiulo P-Á, Gómez-Esteban J-C, Lafuente Sánchez J-V. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Neurological Entity? Medicina. 2021; 57(10):1030. https://doi.org/10.3390/medicina57101030
Chicago/Turabian StyleMurga Gandasegui, Iñigo, Larraitz Aranburu Laka, Pascual-Ángel Gargiulo, Juan-Carlos Gómez-Esteban, and José-Vicente Lafuente Sánchez. 2021. "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Neurological Entity?" Medicina 57, no. 10: 1030. https://doi.org/10.3390/medicina57101030