
Orthostatic Symptoms and Reductions in Cerebral Blood Flow in Long-Haul COVID-19 Patients: Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. ME/CFS Criteria by International Consensus Criteria, Fukuda and Institute of Medicine
2.3. Tilt Test with Extracranial Doppler Cerebral Blood Flow Measurements
2.4. Doppler Measurements for the Determination of the Cardiac Index
2.5. Hemodynamic Classification of Heart and Blood Pressure Changes during Tilt Testing
2.6. Orthostatic Symptoms during Tilt
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Orthostatic Symptoms Questionnaires
Questionnaire at the First Minute of Tilt
- Did you develop, after being tilted, complaints of dizziness or lightheadedness?
- Are you, after being tilted, more fatigued in comparison to when you were lying down?
- Did you develop, after being tilted, muscle weakness of your legs?
- Did you develop, after being tilted, a feeling of dyspnea or breathlessness?
- Do you see less sharp after being tilted?
- Do you hear me differently, after being tilted, in comparison to when you were lying down?
- Are you less concentrated while standing, compared to when you were lying down?
- Did you develop, after being tilted, pain in the muscles of your neck or shoulders?
- Did you develop, after being tilted, a feeling of nausea?
- Did you develop, after being tilted, a tingling feeling in your right hand *?
- Did you develop, after being tilted, a feeling of chest pain or pressure on your chest?
- Did you develop, after being tilted, low back pain?
- Did you start to sweat after being tilted?
- Did you develop, after being tilted, palpitations?
- Did you develop, after being tilted a feeling of a pressure in your head or headache?
- *: the left hand was not asked for as the finger plethysmography cuff was placed around the middle finger of the left hand.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptom | ME | ME: Specificsymptoms | CFS | SEID |
|---|---|---|---|---|
| Chronic fatigue >6 month | X | X | ||
| Reduction physical and mental activities | * | X | X | |
| Reduction memory or concentration | X | X | X | |
| Confusion | X | |||
| Disorientation | X | |||
| Cognitive overload | X | |||
| Decision making problems | X | |||
| Slowed speech | X | |||
| Dyslexia | X | |||
| Short-term memory loss | X | |||
| Slowed thought | X | |||
| Sore throat | X # | X | ||
| Tender lymph nodes | X # | X | ||
| Muscle pain | X | X | ||
| Generalized hyperalgesia | X | |||
| Wide-spread pain (fibromyalgia) | X | |||
| Myofascial pain | X | |||
| Abdominal pain | X | |||
| Chest pain | X | |||
| Multi joint pain | X | X | ||
| Headache | X | X | ||
| Generalized headache | X | |||
| Focal headache | X | |||
| Migraine | X | |||
| Tension headache | X | |||
| Sleep disturbance/unrefreshing sleep | X | X | X | |
| Disturbed sleep patterns: | ||||
| Insomnia | X | |||
| Prolonged sleep | X | |||
| Day-night sleep reversal | X | |||
| Frequent awakenings | X | |||
| Awaking earlier compared to pre-illness | X | |||
| Vivid dreams/night mares | X | |||
| Unrefreshing sleep | X | |||
| PEM or PENE >24 h | X | X | X | |
| Rapid physical and/or mental fatigability during exercise | X | |||
| Post-exertional flare-up symptoms | X | |||
| Post-exertional exhaustion | X | |||
| Prolonged recovery | X | |||
| Reduction pre-illness physical and mental activity | X | |||
| Orthostatic intolerance | X | X | ||
| Postural orthostatic tachycardia syndrome | X | |||
| Neurally mediated hypotension | X | |||
| Palpitations | X | |||
| Dizziness/lightheadedness | X | |||
| Sensory hypersensitivity | X | |||
| Hypersensitivity: | ||||
| Light | X | |||
| Sound | X | |||
| Vibrations | X | |||
| Odor | X | |||
| Taste | X | |||
| Touch | X | |||
| Eye focus problems | X | |||
| Depth perception problems | X | |||
| Motor disturbance | X | |||
| Coordination problems | X | |||
| Ataxia | X | |||
| Muscle weakness | X | |||
| Fasciculations | X | |||
| Susceptibility viral infection with prolonged recovery | X | |||
| Gastrointestinal problems | X | |||
| Nausea | X | |||
| Abdominal pain | X | |||
| Bloating | X | |||
| IBS | X | |||
| Genitourinary problems | X | |||
| Increased urgency | X | |||
| Increased polyuria | X | |||
| Increased nocturia | X | |||
| Sensitivity to food, medication, odors, chemicals | X | |||
| Respiratory problems | X | |||
| Thermostatic instability | X | |||
| Subnormal body temperature | X | |||
| Marked diurnal fluctuations temperature | X | |||
| Sweating episodes | X | |||
| Feeling of feverishness with/without low grade fever | X | |||
| Cold extremities | X | |||
| Extremes of temperature intolerance | X |
References
- Carfi, A.; Bernabei, R.; Landi, F. Gemelli Against C-P-ACSG. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Low, P.A.; Sandroni, P.; Joyner, M.; Shen, W.K. Postural tachycardia syndrome (POTS). J. Cardiovasc. Electrophysiol. 2009, 20, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Institute Of Medicine (IOM). (Ed.) Beyond Mayalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Miglis, M.G.; Prieto, T.; Shaik, R.; Muppidi, S.; Sinn, D.I.; Jaradeh, S. A case report of postural tachycardia syndrome after COVID-19. Clin. Auton. Res. 2020, 30, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Kanjwal, K.; Jamal, S.; Kichloo, A.; Grubb, B.P. New-onset Postural Orthostatic Tachycardia Syndrome Following Coronavirus Disease 2019 Infection. J. Innov. Card. Rhythm Manag. 2020, 11, 4302–4304. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Novak, P. Post COVID-19 syndrome associated with orthostatic cerebral hypoperfusion syndrome, small fiber neuropathy and benefit of immunotherapy: A case report. Eneurologicalsci 2020, 21, 100276. [Google Scholar] [CrossRef]
- Petracek, L.S.; Suskauer, S.J.; Vickers, R.F.; Patel, N.R.; Violand, R.L.; Swope, R.L.; Rowe, P.C. Adolescent and Young Adult ME/CFS after Confirmed or Probable COVID-19. Front. Med. 2021, 8, 668944. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cockshell, S.J.; Mathias, J.L. Cognitive functioning in chronic fatigue syndrome: A meta-analysis. Psychol. Med. 2010, 40, 1253–1267. [Google Scholar] [CrossRef] [PubMed]
- Cvejic, E.; Birch, R.C.; Vollmer-Conna, U. Cognitive Dysfunction in Chronic Fatigue Syndrome: A Review of Recent Evidence. Curr. Rheumatol. Rep. 2016, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Roma, M.; Marden, C.L.; Flaherty, M.A.K.; Jasion, S.E.; Cranston, E.M.; Rowe, P.C. Impaired Health-Related Quality of Life in Adolescent Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: The Impact of Core Symptoms. Front. Pediatr. 2019, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- van Campen, C.L.M.C.; Verheugt, F.W.A.; Rowe, P.C.; Visser, F.C. Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: A quantitative, controlled study using Doppler echography. Clin. Neurophysiol. Pract. 2020, 5, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Katz, B.Z.; Shiraishi, Y.; Mears, C.J.; Binns, H.J.; Taylor, R. Chronic fatigue syndrome after infectious mononucleosis in adolescents. Pediatrics 2009, 124, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.; Asprusten, T.T.; Godang, K.; Leegaard, T.M.; Osnes, L.T.; Skovlund, E.; Tjade, T.; Glenne Øie, M.; Bratholm Wyller, V.B. Predictors of chronic fatigue in adolescents six months after acute Epstein-Barr virus infection: A prospective cohort study. Brain Behav. Immun. 2019, 75, 94–100. [Google Scholar] [CrossRef]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.-Y.; Lam, S.-P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: Long-term follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [Green Version]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients with Joint Hypermobility Show Larger Cerebral Blood Flow Reductions during Orthostatic Stress Testing than Patients without Hypermobility: A Case Control Study. Med. Res. Arch. 2021, 9, 18. [Google Scholar] [CrossRef]
- Beighton, P.; Solomon, L.; Soskolne, C.L. Articular mobility in an African population. Ann. Rheum Dis. 1973, 32, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, D.J.; Scammell, B.E.; Batt, M.E.; Palmer, D. Development and validation of self-reported line drawings of the modified Beighton score for the assessment of generalised joint hypermobility. BMC Med. Res. Methodol. 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- van Campen, C.L.M.C.; Verheugt, F.W.A.; Visser, F.C. Cerebral blood flow changes during tilt table testing in healthy volunteers, as assessed by Doppler imaging of the carotid and vertebral arteries. Clin. Neurophysiol. Pract. 2018, 3, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Ogoh, S.; Hirasawa, A.; Oue, A.; Sadamoto, T. The distribution of blood flow in the carotid and vertebral arteries during dynamic exercise in humans. J. Physiol. 2011, 589 Pt 11, 2847–2856. [Google Scholar] [CrossRef]
- van Campen, C.L.M.C.; Visser, F.C. Validation of Stroke volume measured with suprasternal aortic Doppler imaging: Comparison to transthoracic Stroke Volume measurements. J. Thromb. Circ. 2018, 1–5. [Google Scholar] [CrossRef]
- van Campen, C.L.M.C.; Visser, F.C.; de Cock, C.C.; Vos, H.S.; Kamp, O.; Visser, C.A. Comparison of the haemodynamics of different pacing sites in patients undergoing resynchronisation treatment: Need for individualisation of lead localisation. Heart 2006, 92, 1795–1800. [Google Scholar] [CrossRef]
- Kusumoto, F.; Venet, T.; Schiller, N.B.; Sebastian, A.; Foster, E. Measurement of aortic blood flow by Doppler echocardiography: Temporal, technician, and reader variability in normal subjects and the application of generalizability theory in clinical research. J. Am. Soc. Echocardiogr. 1995, 8, 647–653. [Google Scholar] [CrossRef]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton. Neurosci. 2011, 161, 46–48. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, R.S.; Grubb, B.P.; Olshansky, B., 2nd; Shen, W.K.; Calkins, H.; Brignole, M.; Raj, S.R.; Krahn, A.D.; Morillo, C.A.; Stewart, J.M.; et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015, 12, e41–e63. [Google Scholar] [CrossRef] [Green Version]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients with Syncope: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2017, 70, 620–663. [Google Scholar] [CrossRef]
- Naschitz, J.E.; Rosner, I.; Rozenbaum, M.; Gaitini, L.; Bistritzki, I.; Zuckerman, E.; Sabo, E.; Yeshurun, D. The capnography head-up tilt test for evaluation of chronic fatigue syndrome. In Seminars in Arthritis and Rheumatism; W. B. Saunders: Philadelphia, PA, USA, 2000; Volume 30, pp. 79–86. [Google Scholar]
- Ocon, A.J.; Messer, Z.R.; Medow, M.S.; Stewart, J.M. Increasing orthostatic stress impairs neurocognitive functioning in chronic fatigue syndrome with postural tachycardia syndrome. Clin. Sci. 2012, 122, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Matsushima, R.; Tamai, H.; Kajimoto, Y. Impaired postural cerebral hemodynamics in young patients with chronic fatigue with and without orthostatic intolerance. J. Pediatr. 2002, 140, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Bou-Holaigah, I.; Rowe, P.C.; Kan, J.; Calkins, H. The relationship between neurally mediated hypotension and the chronic fatigue syndrome. JAMA 1995, 274, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Boissoneault, J.; Letzen, J.; Robinson, M.; Staud, R. Cerebral blood flow and heart rate variability predict fatigue severity in patients with chronic fatigue syndrome. Brain Imaging Behav. 2019, 13, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Medow, M.S.; Sood, S.; Messer, Z.; Dzogbeta, S.; Terilli, C.; Stewart, J.M. Phenylephrine alteration of cerebral blood flow during orthostasis: Effect on n-back performance in chronic fatigue syndrome. J. Appl. Physiol. 2014, 117, 1157–1164. [Google Scholar] [CrossRef] [Green Version]
- Biswal, B.; Kunwar, P.; Natelson, B.H. Cerebral blood flow is reduced in chronic fatigue syndrome as assessed by arterial spin labeling. J. Neurol. Sci. 2011, 301, 9–11. [Google Scholar] [CrossRef] [Green Version]
- Razumovsky, A.Y.; DeBusk, K.; Calkins, H.; Snader, S.; Lucas, K.E.; Vyas, P.; Hanley, D.F.; Rowe, P.C. Cerebral and systemic hemodynamics changes during upright tilt in chronic fatigue syndrome. J. Neuroimaging 2003, 13, 57–67. [Google Scholar] [CrossRef] [PubMed]
- van Campen, C.L.M.C.; Visser, F.C. The abnormal Cardiac Index and Stroke Volume Index changes during a normal Tilt Table Test in ME/CFS patients compared to healthy volunteers, are not related to deconditioning. J. Thromb. Circ. 2018, 1–8. [Google Scholar] [CrossRef]
- Timmers, H.J.; Wieling, W.; Soetekouw, P.M.; Bleijenberg, G.; Van Der Meer, J.W.; Lenders, J.W. Hemodynamic and neurohumoral responses to head-up tilt in patients with chronic fatigue syndrome. Clin. Auton. Res. 2002, 12, 273–280. [Google Scholar] [CrossRef]
- Jha, N.K.; Ojha, S.; Jha, S.K.; Dureja, H.; Singh, S.K.; Shukla, S.D.; Chellappan, D.K.; Gupta, G.; Bhardwaj, S.; Kumar, N.; et al. Evidence of Coronavirus (CoV) Pathogenesis and Emerging Pathogen SARS-CoV-2 in the Nervous System: A Review on Neurological Impairments and Manifestations. J. Mol. Neurosci. 2021, 71, 2192–2209. [Google Scholar] [CrossRef]
- Zhou, Z.; Kang, H.; Li, S.; Zhao, X. Understanding the neurotropic characteristics of SARS-CoV-2: From neurological manifestations of COVID-19 to potential neurotropic mechanisms. J. Neurol. 2020, 267, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Yachou, Y.; El Idrissi, A.; Belapasov, V.; Ait Benali, S. Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2: Understanding the neurological manifestations in COVID-19 patients. Neurol. Sci. 2020, 41, 2657–2669. [Google Scholar] [CrossRef] [PubMed]
- Montalvan, V.; Lee, J.; Bueso, T.; De Toledo, J.; Rivas, K. Neurological manifestations of COVID-19 and other coronavirus infections: A systematic review. Clin. Neurol. Neurosurg. 2020, 194, 105921. [Google Scholar] [CrossRef]
- Almqvist, J.; Granberg, T.; Tzortzakakis, A.; Klironomos, S.; Kollia, E.; Ohberg, C.; Martin, R.; Piehl, F.; Ouellette, R.; Ineichen, B.V. Neurological manifestations of coronavirus infections—A systematic review. Ann. Clin. Transl. Neurol. 2020, 7, 2057–2071. [Google Scholar] [CrossRef]
- Sriwastava, S.; Tandon, M.; Podury, S.; Prasad, A.; Wen, S.; Guthrie, G.; Kakara, M.; Jaiswal, S.; Subedi, R.; Elkhooly, M.; et al. COVID-19 and neuroinflammation: A literature review of relevant neuroimaging and CSF markers in central nervous system inflammatory disorders from SARS-CoV2. J. Neurol. 2021, 268, 4448–4478. [Google Scholar] [CrossRef]
- Mukerji, S.S.; Solomon, I.H. What can we learn from brain autopsies in COVID-19? Neurosci. Lett. 2021, 742, 135528. [Google Scholar] [CrossRef]
- Nakatomi, Y.; Mizuno, K.; Ishii, A.; Wada, Y.; Tanaka, M.; Tazawa, S.; Onoe, K.; Fukuda, S.; Kawabe, J.; Takahashi, K.; et al. Neuroinflammation in Patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: An 11C-(R)-PK11195 PET Study. J. Nucl. Med. 2014, 55, 945–950. [Google Scholar] [CrossRef] [Green Version]
- Mueller, C.; Lin, J.C.; Sheriff, S.; Maudsley, A.A.; Younger, J.W. Evidence of widespread metabolite abnormalities in Myalgic encephalomyelitis/chronic fatigue syndrome: Assessment with whole-brain magnetic resonance spectroscopy. Brain Imaging Behav. 2020, 14, 562–572. [Google Scholar] [CrossRef]
- Shan, Z.Y.; Barnden, L.R.; Kwiatek, R.A.; Bhuta, S.; Hermens, D.F.; Lagopoulos, J. Neuroimaging characteristics of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A systematic review. J. Transl. Med. 2020, 18, 335. [Google Scholar] [CrossRef] [PubMed]
- Boissoneault, J.; Letzen, J.; Lai, S.; O’Shea, A.; Craggs, J.; Robinson, M.E.; Staud, R. Abnormal resting state functional connectivity in patients with chronic fatigue syndrome: An arterial spin-labeling fMRI study. Magn. Reson. Imaging 2016, 34, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V.; Cowan, J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther. Adv. Infect Dis. 2021, 8, 20499361211009385. [Google Scholar] [CrossRef] [PubMed]
- Shouman, K.; Vanichkachorn, G.; Cheshire, W.P.; Suarez, M.D.; Shelly, S.; Lamotte, G.J.; Sandroni, P.; Benarroch, E.E.; Berini, S.E.; Cutsforth-Gregory, J.K.; et al. Autonomic dysfunction following COVID-19 infection: An early experience. Clin. Auton. Res. 2021, 31, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.; Stahlberg, M.; Runold, M.; Nygren-Bonnier, M.; Nilsson, J.; Olshansky, B.; Bruchfeld, J.; Fedorowski, A. Long-Haul Post-COVID-19 Symptoms Presenting as a Variant of Postural Orthostatic Tachycardia Syndrome: The Swedish Experience. JACC Case Rep. 2021, 3, 573–580. [Google Scholar] [CrossRef]
- Blitshteyn, S.; Whitelaw, S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: A case series of 20 patients. Immunol. Res. 2021, 69, 205–211. [Google Scholar] [CrossRef]
- Ocon, A.J.; Medow, M.S.; Taneja, I.; Clarke, D.; Stewart, J.M. Decreased upright cerebral blood flow and cerebral autoregulation in normocapnic postural tachycardia syndrome. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H664–H673. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.J.; Kim, S.E.; Park, K.M.; Park, J.; Ha, S.Y.; Kwon, O.-Y. Cerebral hemodynamics in orthostatic intolerance with normal head-up tilt test. Acta Neurol. Scand. 2016, 134, 108–115. [Google Scholar] [CrossRef]
- Hermosillo, A.G.; Jordan, J.L.; Vallejo, M.; Kostine, A.; Marquez, M.F.; Cardenas, M. Cerebrovascular blood flow during the near syncopal phase of head-up tilt test: A comparative study in different types of neurally mediated syncope. Europace 2006, 8, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Wells, R.; Malik, V.; Brooks, A.G.; Linz, D.; Elliott, A.D.; Sanders, P.; Page, A.; Baumert, M.; Lau, D.H. Cerebral Blood Flow and Cognitive Performance in Postural Tachycardia Syndrome: Insights from Sustained Cognitive Stress Test. J. Am. Heart Assoc. 2020, 9, e017861. [Google Scholar] [CrossRef]
- Masuki, S.; Eisenach, J.H.; Schrage, W.G.; Johnson, C.P.; Dietz, N.M.; Wilkins, B.W.; Sandroni, P.; Low, P.A.; Joyner, M.J. Reduced stroke volume during exercise in postural tachycardia syndrome. J. Appl. Physiol. 2007, 103, 1128–1135. [Google Scholar] [CrossRef]
- Fu, Q.; Vangundy, T.B.; Galbreath, M.M.; Shibata, S.; Jain, M.; Hastings, J.L.; Bhella, P.S.; Levine, B.D. Cardiac origins of the postural orthostatic tachycardia syndrome. J. Am. Coll. Cardiol. 2010, 55, 2858–2868. [Google Scholar] [CrossRef] [Green Version]
- Parsaik, A.; Allison, T.G.; Singer, W.; Sletten, D.M.; Joyner, M.J.; Benarroch, E.E.; Low, P.A.; Sandroni, P. Deconditioning in patients with orthostatic intolerance. Neurology 2012, 79, 1435–1439. [Google Scholar] [CrossRef] [Green Version]
- van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Deconditioning does not explain orthostatic intolerance in ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome. J. Transl. Med. 2021, 19, 193. [Google Scholar] [CrossRef] [PubMed]
- Nisenbaum, R.; Jones, J.F.; Unger, E.R.; Reyes, M.; Reeves, W.C. A population-based study of the clinical course of chronic fatigue syndrome. Health Qual. Life Outcome 2003, 3, 49. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; Porter, N.; Brown, M.; Anderson, V.; Brown, A.; Hunnell, J.; Lerch, A. CFS: A Review of Epidemiology and Natural History Studies. Bull. IACFS ME 2009, 17, 88–106. [Google Scholar] [PubMed]
- Pheley, A.M.; Melby, D.; Schenck, C.; Mandel, J.; Peterson, P.K. Can we predict recovery in chronic fatigue syndrome? Minn Med. 1999, 82, 52–56. [Google Scholar] [PubMed]
- Hill, N.F.; Tiersky, L.A.; Scavalla, V.R.; Lavietes, M.; Natelson, B.H. Natural history of severe chronic fatigue syndrome. Arch. Phys. Med. Rehabil. 1999, 80, 1090–1094. [Google Scholar] [CrossRef]
- van der Werf, S.P.; de Vree, B.; Alberts, M.; van der Meer, J.W.; Bleijenberg, G. Natural course and predicting self-reported improvement in patients with chronic fatigue syndrome with a relatively short illness duration. J. Psychosom. Res. 2002, 53, 749–753. [Google Scholar] [CrossRef]
- Reyes, M.; Dobbins, J.G.; Nisenbaum, R.; Subedar, N.S.; Randall, B.; Reeves, W.C. Chronic Fatigue Syndrome Progression and Self-Defined Recovery. J. Chronic. Fatigue Syndr. 1999, 5, 17–27. [Google Scholar] [CrossRef]





| Healthy Controls (n = 20) Group 1 | COVID-19 POTS (n = 10) Group 2 | ME/CFS POTS (n = 20) Group 3 | ME/CFS normHRBP (n = 20) Group 4 | ANOVA and Post-Hoc Tukey | |
|---|---|---|---|---|---|
| Male/female (n) | 6/14 | 3/7 | 6/14 | 6/14 | ns |
| Age (years) | 30 (7) | 30 (7) | 30 (7) | 30 (7) | F (3, 66) = 0.010; p = 0.99 |
| Fulfilling typical ME criteria | 9 (90%) | 20 (100%) | 18 (90%) | Chi-square 2128.2 p = 0.35 | |
| Fulfilling atypical ME criteria | 1 (10%) | 0 (0%) | 2 (10%) | ||
| Fulfilling CFS criteria | 10 (100%) | 20 (100%) | 20 (100%) | ns | |
| Fulfilling IOM criteria | 10 (100%) | 20 (100%) | 20 (100%) | ns | |
| Disease duration, years, #(range) | NA | 1 (1–1.8) | 9.5 (4–14.5) | 10 (7–13.8) | X2(2) = 21.03; p < 0.0001. Post-hoc tests: 2 vs. 3 p = 0.0002; 2 vs. 4 p < 0.0001 |
| BSA (m2) | 1.88 (0.19) | 1.85 (0.17) | 1.90 (0.22) | 1.75 (0.12) | F (3, 66) = 2.86; p = 0.048 |
| BMI (kg/m2) | 24.8 (4.5) | 23.2 (5.4) | 22.8 (3.8) | 23.4 (4.1) | F (3, 66) = 0.79; p = 0.50 |
| Symptom/Symptom Cluster | COVID-19 Cases % Present | 95% CI COVID-19 | ME/CFS Controls % Present | 95% CI ME/CFS | p-Value # |
|---|---|---|---|---|---|
| Fatigue | 100 | 100–100 | 100 | 100–100 | 1.0 * |
| Exercise intolerance physical/mental | 100 | 100–100 | 97.5 | 93–102 | 1.0 * |
| PEM post physical/mental exercise | 100 | 100–100 | 100 | 100–100 | 1.0 * |
| Prolonged recovery | 100 | 100–100 | 100 | 100–100 | 1.0 * |
| Memory problems | 90 | 71–109 | 92.5 | 84–101 | 0.80 # |
| Headache | 100 | 100–100 | 92.5 | 84–101 | 1.0 * |
| Muscle pain | 100 | 100–100 | 75 | 62–88 | 0.18 * |
| Joint pain | 80 | 55–105 | 70 | 56–84 | 0.53 # |
| Unrefreshing sleep | 100 | 100–100 | 100 | 100–100 | 1.0 * |
| Sensory hypersensitivity | 100 | 100–100 | 87.5 | 77–98 | 0.57 * |
| Neuromotor abnormalities | 100 | 100–100 | 92.5 | 84–101 | 1.0 * |
| Sore Throat | 80 | 55–105 | 77.5 | 65–90 | 0.86 # |
| Tender lymph nodes | 90 | 71–109 | 60 | 45–75 | 0.07 # |
| Viral infection hypersensitivity | 70 | 42–98 | 57.5 | 42–73 | 0.47 # |
| Gastro-intestinal problems | 100 | 100–100 | 90 | 81–99 | 0.57 * |
| Genito-urinary problems | 60 | 30–90 | 42.5 | 27–58 | 0.32 # |
| Food/chemical hypersensitivity | 40 | 10–70 | 75 | 62–88 | 0.03 # |
| Orthostatic intolerance | 100 | 100–100 | 97.5 | 93–102 | 1.0 * |
| Respiratory symptoms | 100 | 100–100 | 87.5 | 77–98 | 0.57 * |
| Thermal instability | 80 | 55–105 | 72.5 | 59–86 | 0.63 # |
| Extreme temperature intolerance | 90 | 71–109 | 77.5 | 65–90 | 0.50 # |
| Healthy Controls (n = 20) Group 1 | COVID-19 POTS (n = 10) Group 2 | ME/CFS POTS (n = 20) Group 3 | ME/CFS normHRBP (n = 20) Group 4 | ANOVA and Post-Hoc Tukeys | |
|---|---|---|---|---|---|
| Heart rate supine (bpm) | 68 (12) | 73 (15) | 78 (16) | 79 (14) | F (3, 66) = 2.59; p = 0.06 |
| Heart rate end-tilt (bpm) | 79 (12) | 108 (16) | 113 (19) | 92 (12) | F (3, 66) = 20.67; p < 0.0001. Post-hoc tests: 1 vs. 2 p < 0.0001; 1 vs. 3 p < 0.0001 and 3 vs. 4 p = 0.0001 |
| Systolic BP supine (mmHg) | 138 (18) | 133 (16) | 132 (24) | 133 (17) | F (3, 66) = 0.42; p = 0.74 |
| Systolic BP end-tilt (mmHg) | 134 (15) | 136 (15) | 129 (18) | 133 (17) | F (3, 66) = 0.64; p = 0.59 |
| Diastolic BP supine (mmHg) | 79 (10) | 85 (12) | 81 (19) | 78 (12) | F (3, 66) = 0.68; p = 0.57 |
| Diastolic BP end-tilt (mmHg) | 83 (8) | 100 (11) | 89 (17) | 86 (8) | F (3, 66) = 4.68; p = 0.0051. Post-hoc tests: 1 vs. 2 p = 0.0032 |
| CBF supine (mL/min) | 617 (83) | 629 (70) | 637 (121) | 605 (86) | F (3, 66) = 0.43; p = 0.73 |
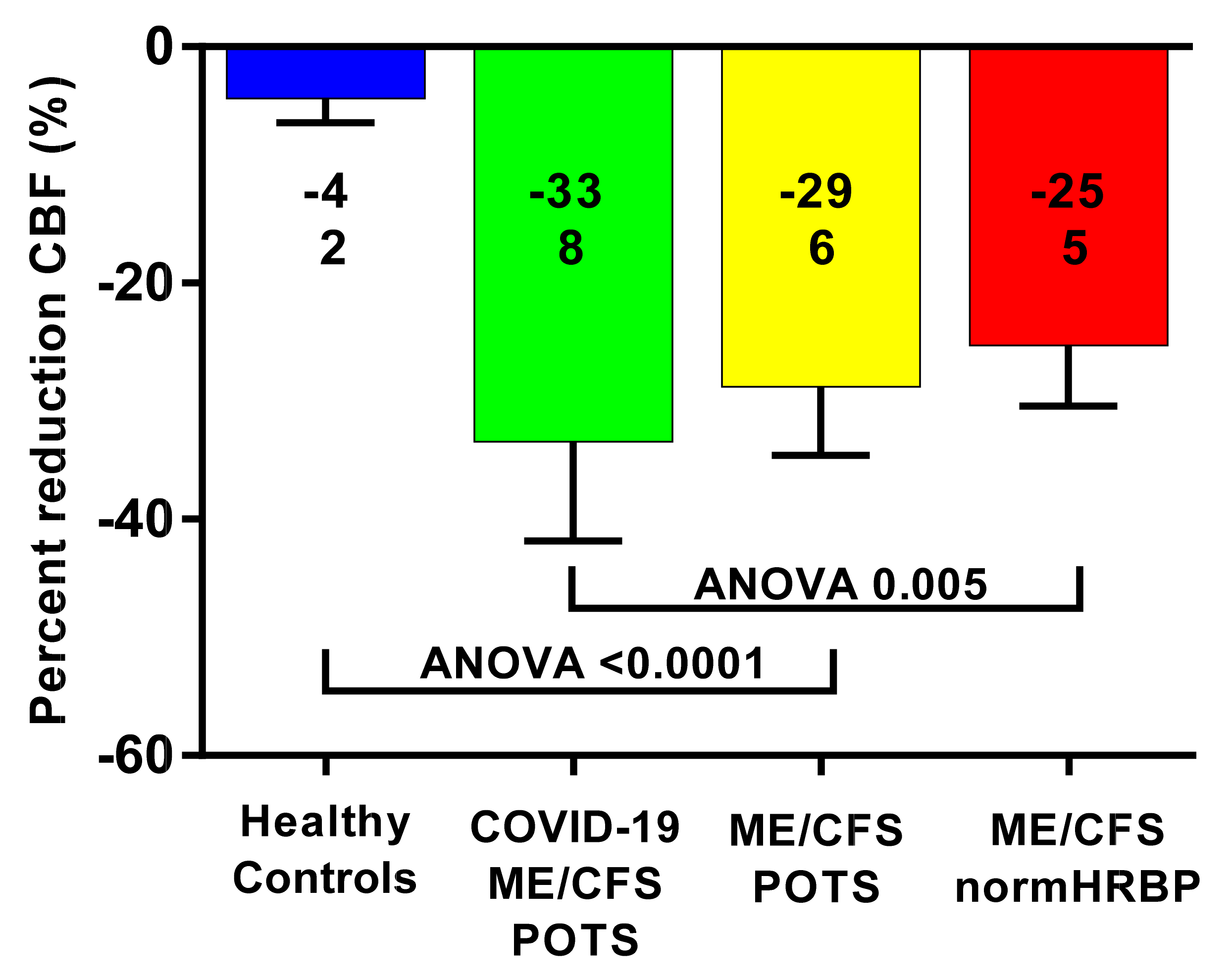
| CBF end-tilt (mL/min) | 591 (84) | 418 (64) | 455 (95) | 451 (69) | F (3, 66) = 15.74; p < 0.0001. Post-hoc tests: 1 vs. 2 p < 0.0001; 1 vs. 3 p < 0.0001 and 1 vs. 4 p < 0.0001 |
| PETCO2 supine (mmHg) | 37 (2) | 39 (3) | 38 (3) | 37 (2) | F (3, 66) = 1.76; p = 0.16 |
| PETCO2 end-tilt (mmHg) | 36 (2) | 29 (3) | 27 (6) | 29 (4) | F (3, 66) = 16.19; p = 0.0002. Post-hoc tests: 1 vs. 2 p < 0.0001; 1 vs. 3 p < 0.0001 and 1 vs. 4 p < 0.0001 |
| Delta PETCO2 (mmHg) | −1 (1) | −10 (3) | −10 (3) | −8 (4) | F (3, 66) = 37.18; p < 0.0001. Post-hoc tests: 1 vs. 2 p < 0.0001; 1 vs. 3 p < 0.0001 and 1 vs. 4 p < 0.0001 |
| CI supine (L/min/m2) | 2.29 (0.30) | 2.86 (0.36) | 2.82 (0.46) | 2.65 (0.39) | F (3, 66) = 8.08; p = 0.0001. Post-hoc tests: 1 vs. 2 p = 0.0016; 1 vs. 3 p = 0.0003 |
| CI end-tilt (L/min/m2) | 2.08 (0.24) | 2.20 (0.54) | 2.19 (0.48) | 1.99 (0.30) | F (3, 66) = 1.25; p = 0.30 |
| Perc reduction CI (%) | −9 (5) | −23 (14) | −22 (12) | −25 (5) | F (3, 66) = 12.22; p < 0.0001. Post-hoc tests: 1 vs. 2 p = 0.0008; 1 vs. 3 p = 0.0002 and 1 vs. 4 p < 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campen, C.M.C.v.; Rowe, P.C.; Visser, F.C. Orthostatic Symptoms and Reductions in Cerebral Blood Flow in Long-Haul COVID-19 Patients: Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Medicina 2022, 58, 28. https://doi.org/10.3390/medicina58010028
Campen CMCv, Rowe PC, Visser FC. Orthostatic Symptoms and Reductions in Cerebral Blood Flow in Long-Haul COVID-19 Patients: Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Medicina. 2022; 58(1):28. https://doi.org/10.3390/medicina58010028
Chicago/Turabian StyleCampen, C. (Linda) M. C. van, Peter C. Rowe, and Frans C. Visser. 2022. "Orthostatic Symptoms and Reductions in Cerebral Blood Flow in Long-Haul COVID-19 Patients: Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome" Medicina 58, no. 1: 28. https://doi.org/10.3390/medicina58010028