Induction Chemotherapy for Primarily Unresectable Locally Advanced Pancreatic Adenocarcinoma—Who Will Benefit from a Secondary Resection?

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Neoadjuvant Treatment
3.3. Surgical Procedure
3.4. Side Effects and Complications
3.5. Effect of Preoperative Therapy
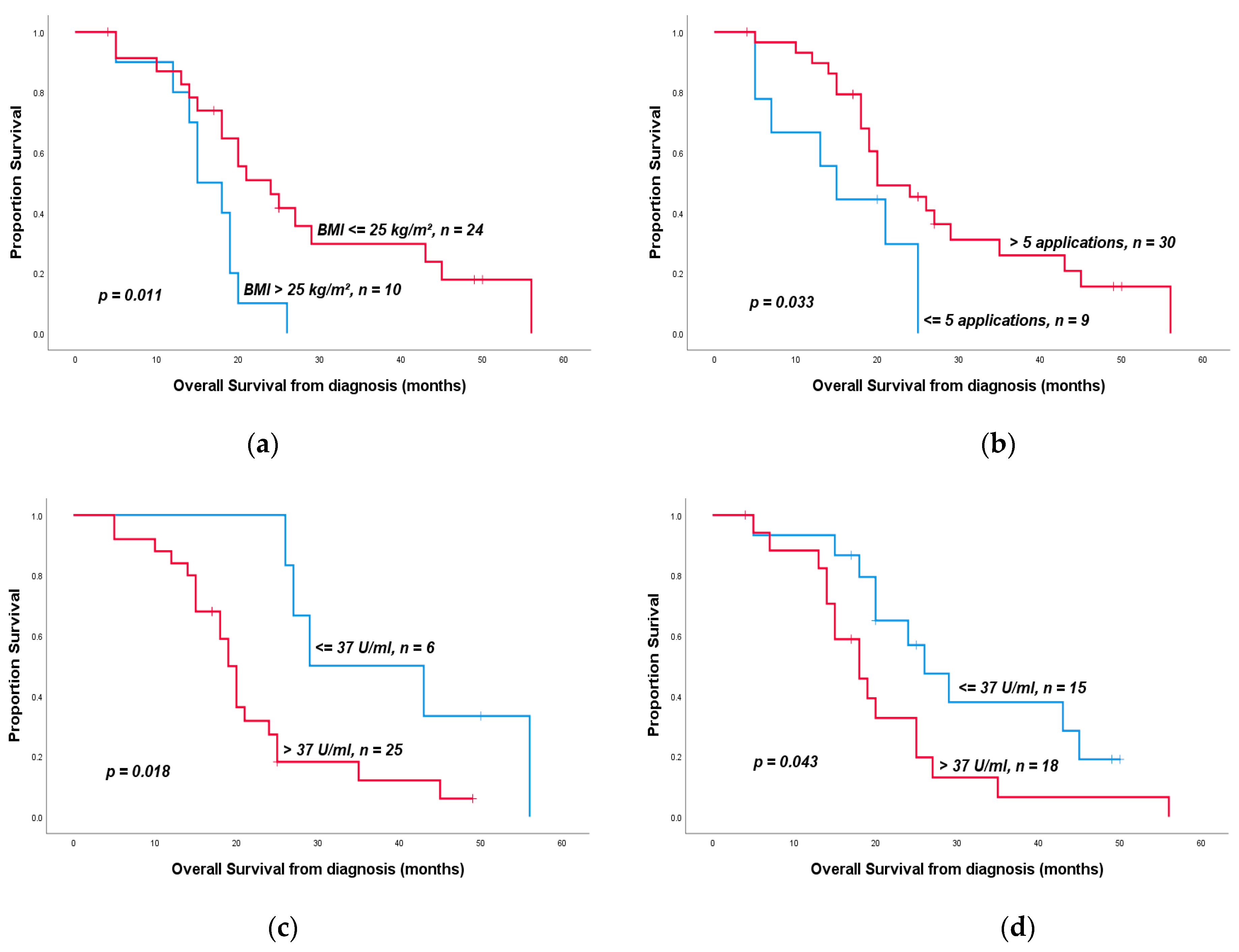
3.6. Overall Survival
3.7. Predictors of Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oettle, H.; Riess, H.; Stieler, J.M.; Heil, G.; Schwaner, I.; Seraphin, J.; Gorner, M.; Molle, M.; Greten, T.F.; Lakner, V.; et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: Outcomes from the CONKO-003 trial. J. Clin. Oncol. 2014, 32, 2423–2429. [Google Scholar] [CrossRef]
- Pelzer, U.; Schwaner, I.; Stieler, J.; Adler, M.; Seraphin, J.; Dorken, B.; Riess, H.; Oettle, H. Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: A phase III-study from the German CONKO-study group. Eur. J. Cancer 2011, 47, 1676–1681. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Li, C.P.; Bodoky, G.; Dean, A.; Shan, Y.S.; Jameson, G.; Macarulla, T.; Lee, K.H.; Cunningham, D.; Blanc, J.F.; et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): A global, randomised, open-label, phase 3 trial. Lancet 2016, 387, 545–557. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Callery, M.P.; Chang, K.J.; Fishman, E.K.; Talamonti, M.S.; William Traverso, L.; Linehan, D.C. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: Expert consensus statement. Ann. Surg. Oncol. 2009, 16, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Reiser, C.; Hinz, U.; Bachmann, J.; Debus, J.; Jaeger, D.; Friess, H.; Buchler, M.W. Surgery for recurrent pancreatic ductal adenocarcinoma. Ann. Surg. 2007, 245, 566–572. [Google Scholar] [CrossRef]
- Pan, L.; Fang, J.; Tong, C.; Chen, M.; Zhang, B.; Juengpanich, S.; Wang, Y.; Cai, X. Survival benefits of neoadjuvant chemo(radio)therapy versus surgery first in patients with resectable or borderline resectable pancreatic cancer: A systematic review and meta-analysis. World J. Surg. Oncol. 2019, 18, 1. [Google Scholar] [CrossRef]
- Hammel, P.; Huguet, F.; van Laethem, J.L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouche, O.; Shannon, J.; Andre, T.; et al. Effect of Chemoradiotherapy vs. Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Kunzmann, V.; Algül, H.; Goekkurt, E.; Siegler, G.M.; Martens, U.M.; Waldschmidt, D.; Pelzer, U.; Hennes, E.; Fuchs, M.; Siveke, J.; et al. 671O-Conversion rate in locally advanced pancreatic cancer (LAPC) after nab-paclitaxel/gemcitabine- or FOLFIRINOX-based induction chemotherapy (NEOLAP): Final results of a multicenter randomised phase II AIO trial. Ann. Oncol. 2019, 30, v253. [Google Scholar] [CrossRef]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jager, D.; Ulrich, A.; Buchler, M.W. Locally Advanced Pancreatic Cancer: Neoadjuvant Therapy With Folfirinox Results in Resectability in 60% of the Patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef]
- Gemenetzis, G.; Groot, V.P.; Blair, A.B.; Laheru, D.A.; Zheng, L.; Narang, A.K.; Fishman, E.K.; Hruban, R.H.; Yu, J.; Burkhart, R.A.; et al. Survival in Locally Advanced Pancreatic Cancer After Neoadjuvant Therapy and Surgical Resection. Ann. Surg. 2019, 270, 340–347. [Google Scholar] [CrossRef]
- Malinka, T.; Timmermann, L.; Klein, F.; Geisel, D.; Pratschke, J.; Bahra, M. Is there a Role for the Appleby Procedure in 2020? Results from a Matched-Pair-Analysis. Anticancer Res. 2020, 40, 387–392. [Google Scholar] [CrossRef]
- Schmocker, R.K.; Wright, M.J.; Ding, D.; Beckman, M.J.; Javed, A.A.; Cameron, J.L.; Lafaro, K.J.; Burns, W.R.; Weiss, M.J.; He, J.; et al. An Aggressive Approach to Locally Confined Pancreatic Cancer: Defining Surgical and Oncologic Outcomes Unique to Pancreatectomy with Celiac Axis Resection (DP-CAR). Ann. Surg. Oncol. 2020. [Google Scholar] [CrossRef]
- Katz, M.H.; Fleming, J.B.; Bhosale, P.; Varadhachary, G.; Lee, J.E.; Wolff, R.; Wang, H.; Abbruzzese, J.; Pisters, P.W.; Vauthey, J.N.; et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012, 118, 5749–5756. [Google Scholar] [CrossRef]
- Reni, M.; Zanon, S.; Balzano, G.; Nobile, S.; Pircher, C.C.; Chiaravalli, M.; Passoni, P.; Arcidiacono, P.G.; Nicoletti, R.; Crippa, S.; et al. Selecting patients for resection after primary chemotherapy for non-metastatic pancreatic adenocarcinoma. Ann. Oncol. 2017, 28, 2786–2792. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Meyer Zum Buschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartwig, W.; Gluth, A.; Hinz, U.; Koliogiannis, D.; Strobel, O.; Hackert, T.; Werner, J.; Buchler, M.W. Outcomes after extended pancreatectomy in patients with borderline resectable and locally advanced pancreatic cancer. Br. J. Surg. 2016, 103, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Roland, C.L.; Yang, A.D.; Katz, M.H.; Chatterjee, D.; Wang, H.; Lin, H.; Vauthey, J.N.; Pisters, P.W.; Varadhachary, G.R.; Wolff, R.A.; et al. Neoadjuvant therapy is associated with a reduced lymph node ratio in patients with potentially resectable pancreatic cancer. Ann. Surg. Oncol. 2015, 22, 1168–1175. [Google Scholar] [CrossRef]
- Diehl, S.J.; Lehmann, K.J.; Sadick, M.; Lachmann, R.; Georgi, M. Pancreatic cancer: Value of dual-phase helical CT in assessing resectability. Radiology 1998, 206, 373–378. [Google Scholar] [CrossRef]
- Asagi, A.; Ohta, K.; Nasu, J.; Tanada, M.; Nadano, S.; Nishimura, R.; Teramoto, N.; Yamamoto, K.; Inoue, T.; Iguchi, H. Utility of contrast-enhanced FDG-PET/CT in the clinical management of pancreatic cancer: Impact on diagnosis, staging, evaluation of treatment response, and detection of recurrence. Pancreas 2013, 42, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Bardales, R.H.; Stelow, E.B.; Mallery, S.; Lai, R.; Stanley, M.W. Review of endoscopic ultrasound-guided fine-needle aspiration cytology. Diagn. Cytopathol. 2006, 34, 140–175. [Google Scholar] [CrossRef]
- Naumann, P.; Eberlein, J.; Farnia, B.; Liermann, J.; Hackert, T.; Debus, J.; Combs, S.E. Cachectic Body Composition and Inflammatory Markers Portend a Poor Prognosis in Patients with Locally Advanced Pancreatic Cancer Treated with Chemoradiation. Cancers 2019, 11, 1655. [Google Scholar] [CrossRef] [Green Version]
- Kolb, R.; Sutterwala, F.S.; Zhang, W. Obesity and cancer: Inflammation bridges the two. Curr. Opin. Pharmacol. 2016, 29, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Majumder, K.; Gupta, A.; Arora, N.; Singh, P.P.; Singh, S. Premorbid Obesity and Mortality in Patients With Pancreatic Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 355–368e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engle, D.D.; Tiriac, H.; Rivera, K.D.; Pommier, A.; Whalen, S.; Oni, T.E.; Alagesan, B.; Lee, E.J.; Yao, M.A.; Lucito, M.S.; et al. The glycan CA19-9 promotes pancreatitis and pancreatic cancer in mice. Science 2019, 364, 1156–1162. [Google Scholar] [CrossRef]
- Gao, H.F.; Wang, Q.Y.; Zhang, K.; Chen, L.Y.; Cheng, C.S.; Chen, H.; Meng, Z.Q.; Zhou, S.M.; Chen, Z. Overexpressed N-fucosylation on the cell surface driven by FUT3, 5, and 6 promotes cell motilities in metastatic pancreatic cancer cell lines. Biochem. Biophys. Res. Commun. 2019, 511, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Deng, S.; Jin, K.; Gong, Y.; Cheng, H.; Fan, Z.; Qian, Y.; Huang, Q.; Ni, Q.; Luo, G.; et al. Lewis antigennegative pancreatic cancer: An aggressive subgroup. Int. J. Oncol. 2020, 56, 900–908. [Google Scholar] [CrossRef] [Green Version]
- Boone, B.A.; Steve, J.; Zenati, M.S.; Hogg, M.E.; Singhi, A.D.; Bartlett, D.L.; Zureikat, A.H.; Bahary, N.; Zeh, H.J., 3rd. Serum CA 19-9 response to neoadjuvant therapy is associated with outcome in pancreatic adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 4351–4358. [Google Scholar] [CrossRef]
- Truty, M.J.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Cleary, S.P.; Graham, R.P.; Goenka, A.H.; Hallemeier, C.L.; Haddock, M.G.; Harmsen, W.S.; et al. Factors Predicting Response, Perioperative Outcomes, and Survival Following Total Neoadjuvant Therapy for Borderline/Locally Advanced Pancreatic Cancer. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Okada, K.; Kawai, M.; Hirono, S.; Satoi, S.; Yanagimoto, H.; Ioka, T.; Miyazawa, M.; Shimizu, A.; Kitahata, Y.; Yamaue, H. Impact of treatment duration of neoadjuvant FIRINOX in patients with borderline resectable pancreatic cancer: A pilot trial. Cancer Chemother. Pharmacol. 2016, 78, 719–726. [Google Scholar] [CrossRef]
- Michelakos, T.; Pergolini, I.; Castillo, C.F.; Honselmann, K.C.; Cai, L.; Deshpande, V.; Wo, J.Y.; Ryan, D.P.; Allen, J.N.; Blaszkowsky, L.S.; et al. Predictors of Resectability and Survival in Patients with Borderline and Locally Advanced Pancreatic Cancer who Underwent Neoadjuvant Treatment With FOLFIRINOX. Ann. Surg. 2019, 269, 733–740. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Mirkin, K.A.; Greenleaf, E.K.; Hollenbeak, C.S.; Wong, J. Correlation of clinical and pathological staging and response to neoadjuvant therapy in resected pancreatic cancer. Int. J. Surg. 2018, 52, 221–228. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics (n = 40) | |||||
|---|---|---|---|---|---|
| Age | |||||
| Mean | 60.6 (37–82) years | ||||
| Gender | |||||
| Male | 22 (55.0%) pts | ||||
| Female | 18 (45.0%) pts | ||||
| Primary Localization | |||||
| Head | 21 (52.5%) pts | ||||
| Korpus | 13 (32.5%) pts | ||||
| Tail | 6 (15%) pts | ||||
| At Diagnosis | After Induction/Before Resection | ||||
| N | % | N | % | p | |
| ECOG | 0.03 | ||||
| 0 | 22 | 66.7 | 10 | 37 | |
| 1 | 10 | 30.3 | 12 | 44.4 | |
| 2 | 1 | 3 | 5 | 18.5 | |
| n.a. | 7 | 13 | |||
| ASA Score | |||||
| 1 | 2 | 5.7 | |||
| 2 | 15 | 42.9 | |||
| 3 | 18 | 51.4 | |||
| n.a. | 5 | ||||
| BMI [kg/m2] | Median 23.9 (17.2–28.7) | Median 22.6 (16.8–29.9) | |||
| <18.5 | 1 | 3.7 | 1 | 2.9 | 0.25 |
| 18.5–24.9 | 18 | 66.7 | 23 | 67.6 | |
| ≥25 | 8 | 29.6 | 10 | 29.4 | |
| n.a. | 13 | 6 | |||
| Parameter | Category | N | % |
|---|---|---|---|
| Induction Therapy | |||
| FOLFIRINOX | 23 | 57.5 | |
| Nab-Paclitaxel/Gemcitabine | 7 | 17.5 | |
| FOLFIRINOX ► Nab-Pac/Gem | 8 | 20 | |
| Gemcitabine mono | 1 | 2.5 | |
| Cisplatin/Capecitabine | 1 | 2.5 | |
| Number of Applications | |||
| Median | 8 (3–25) | ||
| ≥8 Applications | 20 | 51.3 | |
| <8 Applications | 19 | 48.7 | |
| n.a. | 1 | ||
| Duration of neoadjuvant Therapy | |||
| Median (months) | 3 (1–24) | ||
| >3 months | 18 | 48.6 | |
| ≤3 months | 19 | 51.4 | |
| n.a. | 3 | ||
| Adjuvant Therapy | |||
| Yes | 15 | 75 | |
| No | 5 | 25 | |
| n.a. | 20 | ||
| Surgical Procedure | |||
| PPPD | 16 | 40 | |
| Whipple’s Procedure | 2 | 5 | |
| Distal pancreatectomy | 13 | 32.5 | |
| Total pancreatectomy | 9 | 22.5 | |
| Additional resection | |||
| Splenectomy | 19 | 47.5 | |
| Gastrectomy (total/partial) | 2 | 5 | |
| Partial hepatectomy | 3 | 7.5 | |
| Resection of portal vein | 7 | 17.5 | |
| Resection coeliac axis | 4 | 10 | |
| Hemicolectomy | 1 | 2.5 | |
| Post Op-Complications | |||
| BDA-Insufficiency | 26 | 65 | |
| Pancreatic fistula | 5 | 12.5 | |
| Postpancreatectomy | 9 | 22.5 | |
| haemorrhages | 1 | 2.5 |
| Total | Folfirinox | Nab-Paclitaxel/Gem | Folfirinox ►Nab-Pac/Gem | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Category | N | % | N | % | N | % | N | % | |
| General Side effects | 0–2 | 15 | 48.5 | 19 | 63.2 | 5 | 60 | 7 | 0 | 0.009 |
| 12 | 3 | 0 | ||||||||
| 3–4 | 16 | 51.6 | 7 | 36.8 | 2 | 40 | 7 | 100 | ||
| Neutropenia | 15 | 5 | 7 | |||||||
| 0–2 | 16 | 59.3 | 11 | 73.3 | 3 | 60 | 2 | 28.6 | 0.16 | |
| 3–4 | 11 | 40.7 | 4 | 26.7 | 2 | 40 | 5 | 71.4 | ||
| Anemia | 17 | 5 | 8 | |||||||
| 0–2 | 26 | 86.7 | 15 | 88.2 | 4 | 80 | 7 | 87.5 | 1 | |
| 3–4 | 4 | 13.3 | 2 | 11.8 | 1 | 20 | 1 | 12.5 | ||
| Thrombopenia | 9 | 3 | 4 | |||||||
| 0–2 | 15 | 93.8 | 8 | 88.9 | 3 | 100 | 4 | 100 | 1 | |
| 3–4 | 1 | 6.3 | 1 | 11.1 | 0 | 0 | 0 | 0 | ||
| Infections | 16 | 4 | 7 | |||||||
| 0–2 | 24 | 88.9 | 15 | 93.8 | 4 | 100 | 5 | 71.4 | 0.2 | |
| 3–4 | 3 | 7.5 | 1 | 6.2 | 0 | 0 | 2 | 28.6 | ||
| Diarrhea | 4 | 1 | 3 | |||||||
| 0–2 | 5 | 62.5 | 3 | 75 | 1 | 100 | 1 | 33.3 | 0.68 | |
| 3–4 | 3 | 37.5 | 1 | 25 | 0 | 0 | 2 | 66.7 | ||
| Nausea | 6 | 3 | 6 | |||||||
| 0–2 | 15 | 93.8 | 6 | 100 | 2 | 66.7 | 5 | 83.3 | 0.66 | |
| 3–4 | 2 | 13.3 | 0 | 0 | 1 | 33.3 | 1 | 16.7 | ||
| Neurological side effects | 0–2 | 13 | 81.3 | 10 | 70 | 3 | 100 | 3 | 100 | 0.52 |
| 7 | 3 | 3 | ||||||||
| 3–4 | 3 | 18.8 | 3 | 30 | 0 | 0 | 0 | 0 | ||
| At Diagnosis | After Induction Therapy | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Category | N | % | Mean | IQR | N | % | Mean | IQR | p |
| CA 19-9 (U/mL) | 4358.3 | 64.8–830 | 138.5 | 12.1–65.4 | 0.001 | |||||
| ≤37 U/mL | 5 | 16.1 | 15 | 44.1 | ||||||
| 37–400 U/mL | 14 | 45.2 | 17 | 50 | ||||||
| >400 U/mL | 12 | 38.7 | 2 | 5.9 | ||||||
| n.a. | 9 | 6 | ||||||||
| CA 19-9 trend (-%) | 29 | 44.7 | 18–94.75 | |||||||
| CEA (ng/mL) | 10.5 | 2.5–7 | 3.5 | 2–5.3 | 0.16 | |||||
| ≤5 ng/ml | 15 | 65.2 | 18 | 69.2 | ||||||
| >5 ng/ml | 8 | 34.8 | 8 | 30.8 | ||||||
| n.a. | 17 | 14 | ||||||||
| c/pT Status | 0.001 | |||||||||
| 0 | 0 | 0 | 5 | 12.5 | ||||||
| 1 | 0 | 0 | 8 | 20 | ||||||
| 2 | 3 | 8.1 | 11 | 27.5 | ||||||
| 3 | 14 | 37.8 | 10 | 25 | ||||||
| 4 | 20 | 54.1 | 6 | 15 | ||||||
| n.a. | 3 | 0 | ||||||||
| pN Status | ||||||||||
| 0 | 21 | 52.5 | ||||||||
| 1 | 19 | 47.5 | ||||||||
| c/pM Status | 0.18 | |||||||||
| 0 | 30 | 78.9 | 35 | 87.5 | ||||||
| 1 | 8 | 21.6 | 5 | 12.5 | ||||||
| n.a. | 2 | 0 | ||||||||
| R Status | ||||||||||
| 0 | 18 | 46.2 | ||||||||
| 1 | 21 | 53.8 | ||||||||
| n.a. | 1 | |||||||||
| Parameter | Category | OS (Months) | p | HR | 95%CI | p |
|---|---|---|---|---|---|---|
| CA 19-9 at diagnosis | ≤37 vs. >37 U/ml | 29 vs. 19 | 0.02 | 3.44 | 1.14–10.36 | 0.028 |
| CA 19-9 after induction | ≤37 vs. >37 U/mL | 26 vs. 18 | 0.043 | 2.23 | 0.99–5.03 | 0.054 |
| <400 vs. ≥400 U/mL | 24 vs. 7 | 0.001 | 17.2 | 2.38–124.45 | 0.005 | |
| CEA after induction | ≤5 vs. >5 ng/ml | 25 vs. 18 | 0.047 | 2.67 | 0.96–7.48 | 0.061 |
| BMI after induction | >25 vs. ≤25 | 15 vs. 24 | 0.01 | 0.36 | 0.15–0.83 | 0.017 |
| pN status | 0 vs. 1 | 25 vs. 15 | 0.003 | 2.99 | 1.39–6.41 | 0.005 |
| pT status | 0–1 vs. 2–4 | 43 vs. 19 | 0.008 | 3.09 | 1.26–7.62 | 0.014 |
| Pn | 0 vs. 1 | 35 vs. 19 | 0.058 | 2.46 | 0.92–6.56 | 0.072 |
| Neoadjuvant protocoll | FOLFIRINOX vs. other | 20 vs. 20 | 0.88 | 0.95 | 0.46–1.97 | 0.89 |
| Nab-Pac/Gem vs. other | 20 vs. 20 | 0.54 | 0.77 | 0.33–1.81 | 0.55 | |
| FOLFIRINOX ► Nab-Pac/Gem vs. other | 18 vs. 20 | 0.22 | 1.86 | 0.68–5.11 | 0.23 | |
| Number of neoadjuvant applications | ≤5 vs. >5 | 15 vs. 20 | 0.033 | 0.41 | 0.17–0.98 | 0.044 |
| Adjuvant therapy | no adjuvant therapy vs. adjuvant therapy | 10 vs. 25 | 0.001 | 0.21 | 0.08–0.55 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosumeck, N.; Timmermann, L.; Klein, F.; Bahra, M.; Stintzig, S.; Malinka, T.; Pelzer, U. Induction Chemotherapy for Primarily Unresectable Locally Advanced Pancreatic Adenocarcinoma—Who Will Benefit from a Secondary Resection? Medicina 2021, 57, 77. https://doi.org/10.3390/medicina57010077
Rosumeck N, Timmermann L, Klein F, Bahra M, Stintzig S, Malinka T, Pelzer U. Induction Chemotherapy for Primarily Unresectable Locally Advanced Pancreatic Adenocarcinoma—Who Will Benefit from a Secondary Resection? Medicina. 2021; 57(1):77. https://doi.org/10.3390/medicina57010077
Chicago/Turabian StyleRosumeck, Nathalie, Lea Timmermann, Fritz Klein, Marcus Bahra, Sebastian Stintzig, Thomas Malinka, and Uwe Pelzer. 2021. "Induction Chemotherapy for Primarily Unresectable Locally Advanced Pancreatic Adenocarcinoma—Who Will Benefit from a Secondary Resection?" Medicina 57, no. 1: 77. https://doi.org/10.3390/medicina57010077