Prognostic Utility of Circulating Growth Factors in Aortic Valve Stenosis: A Pilot Study


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Laboratory Assays
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
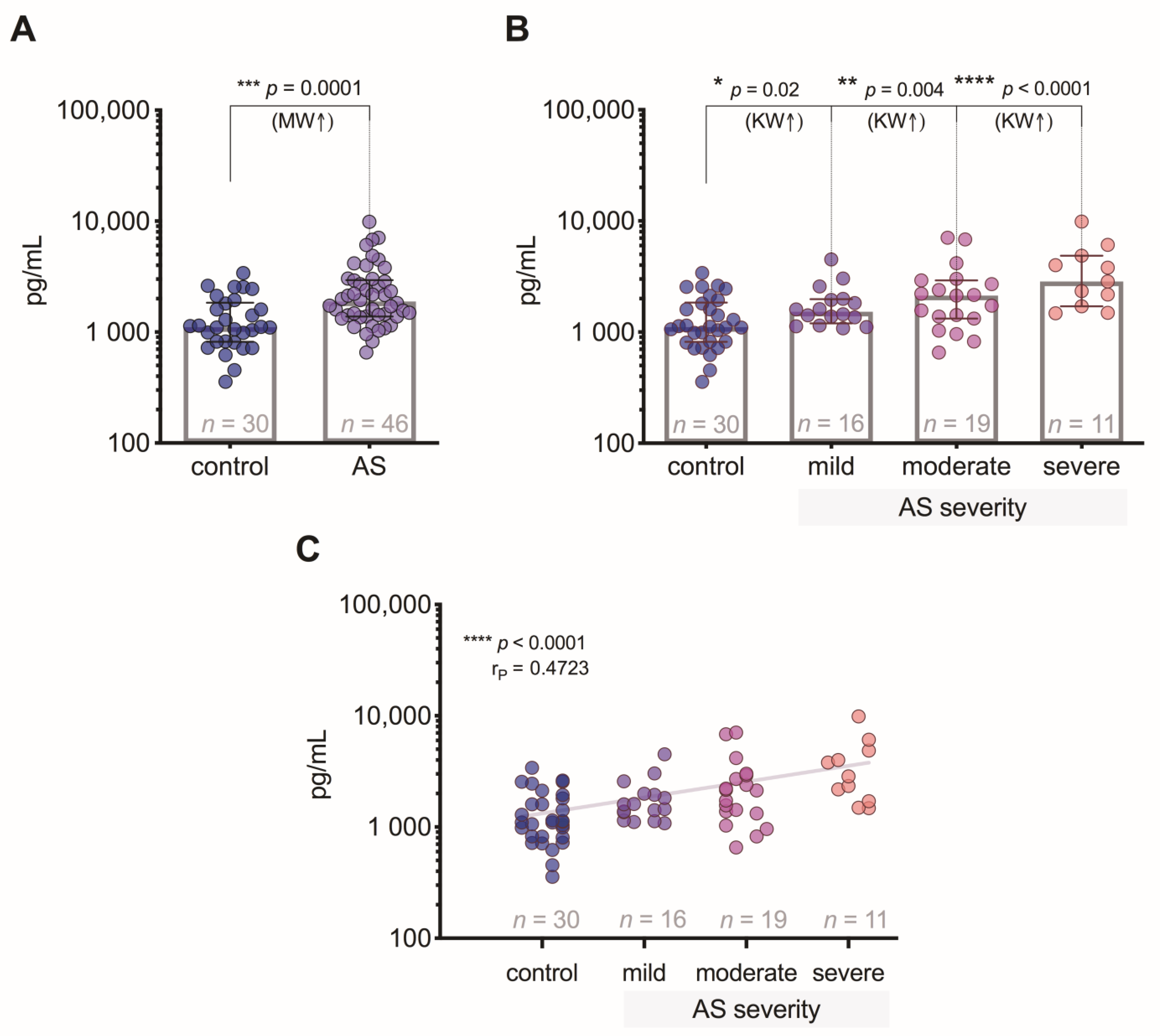
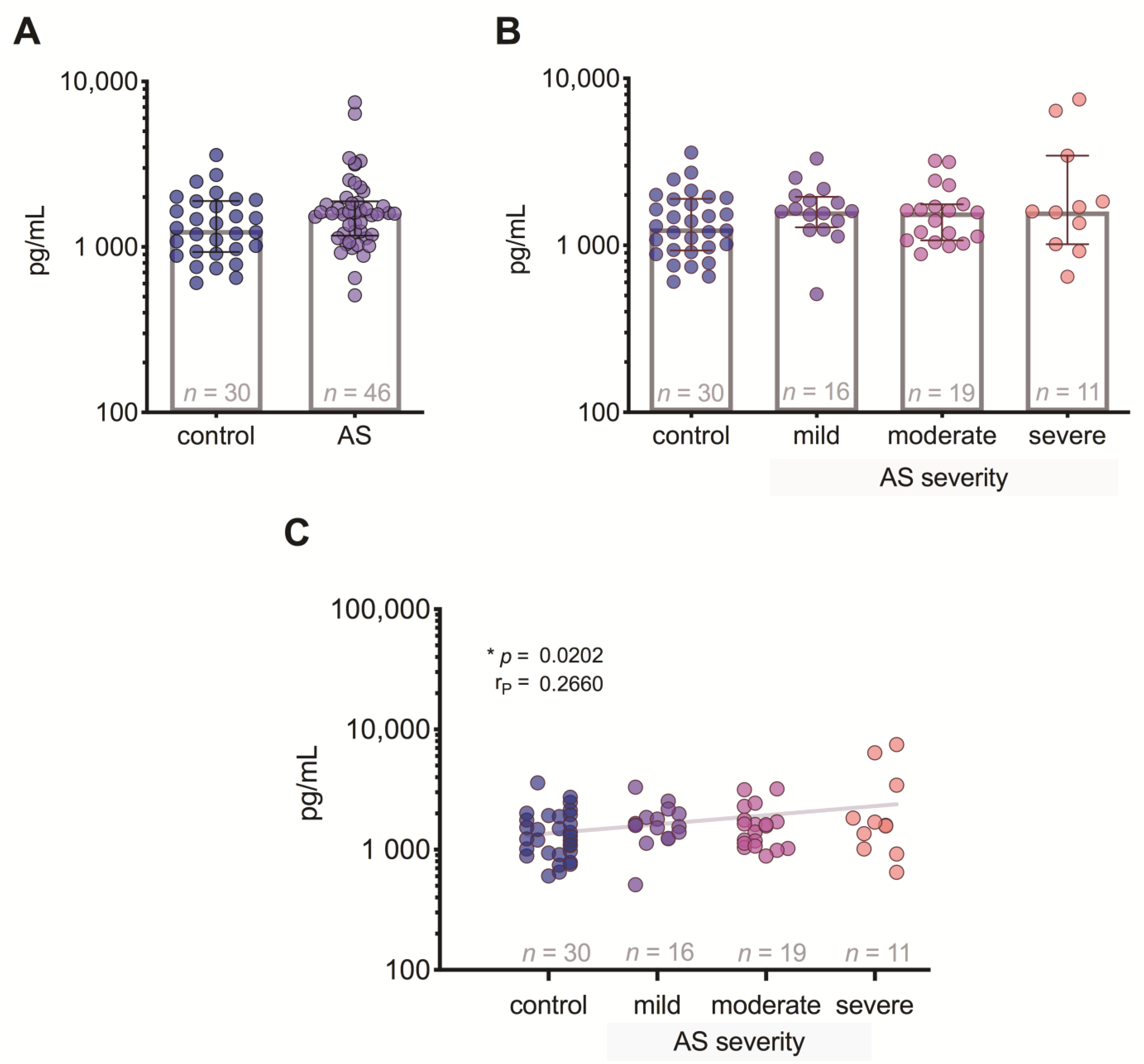
3.2. GDF-15 Level Differences between the Patient Groups
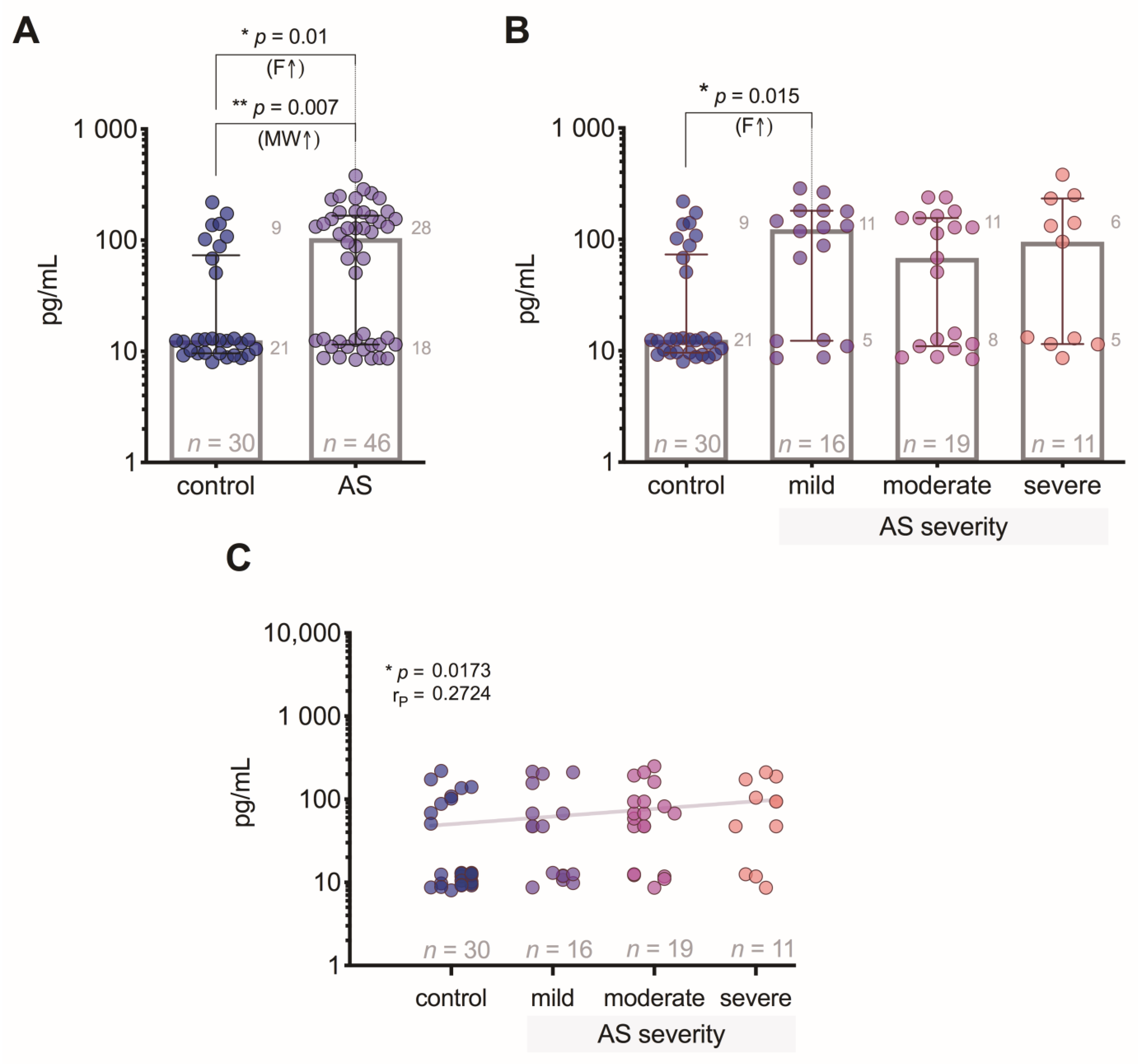
3.3. VEGF-A Level Differences between the Patient Groups
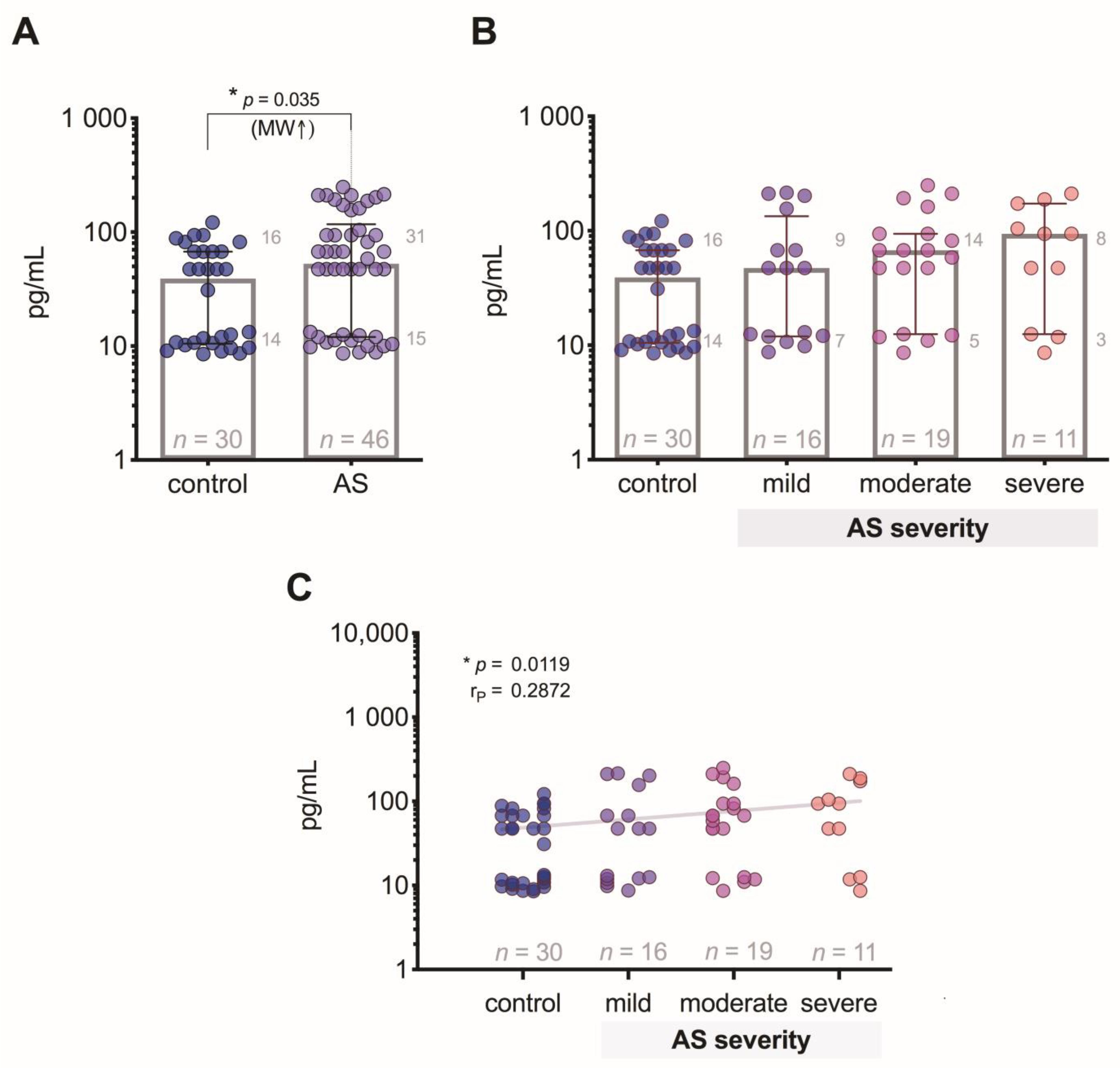
3.4. FGF-2 Level Differences between the Patient Groups
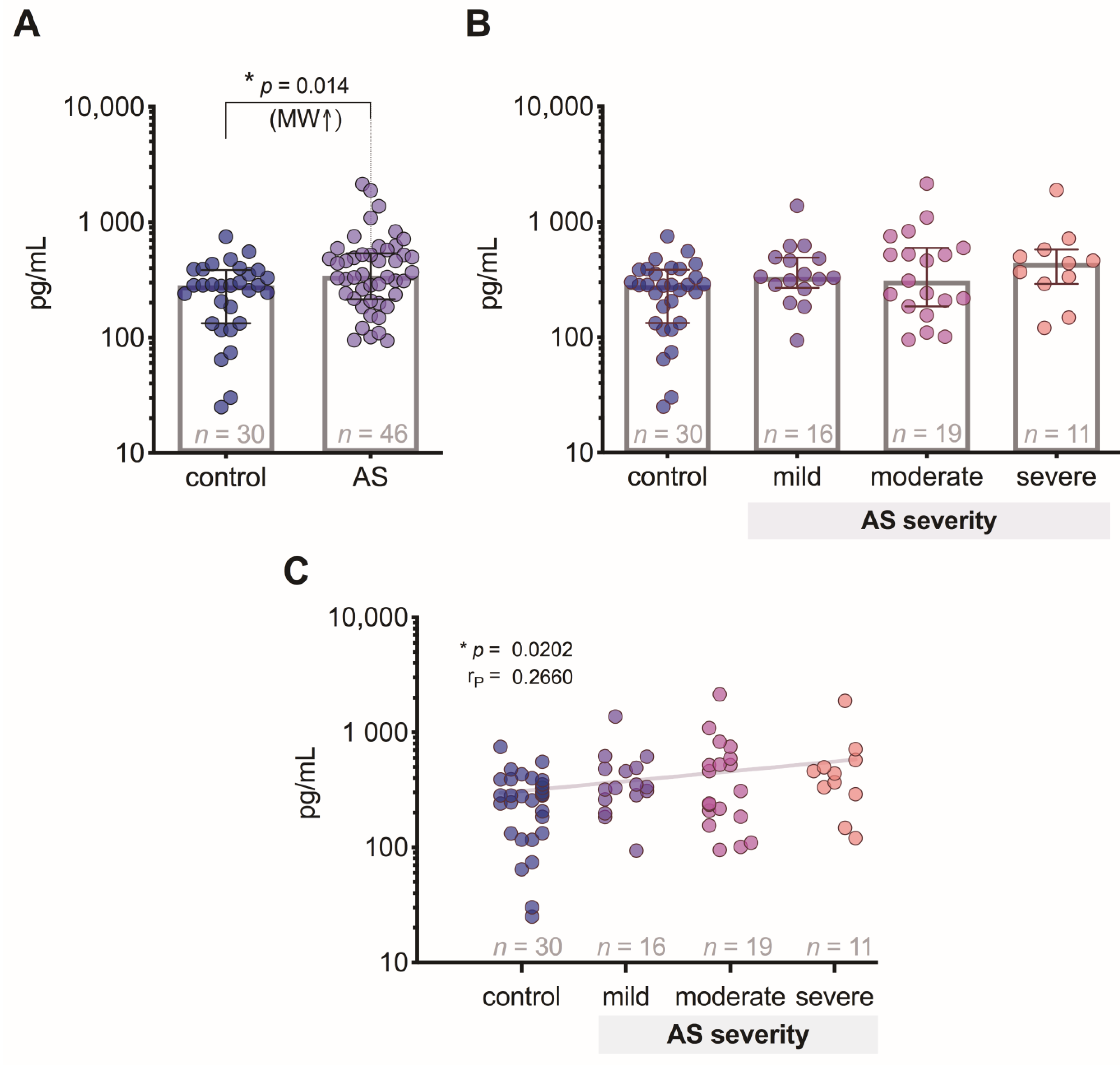
3.5. FGF-21 Level Differences between the Patient Groups
3.6. Ang-2 Level Differences between the Patient Groups
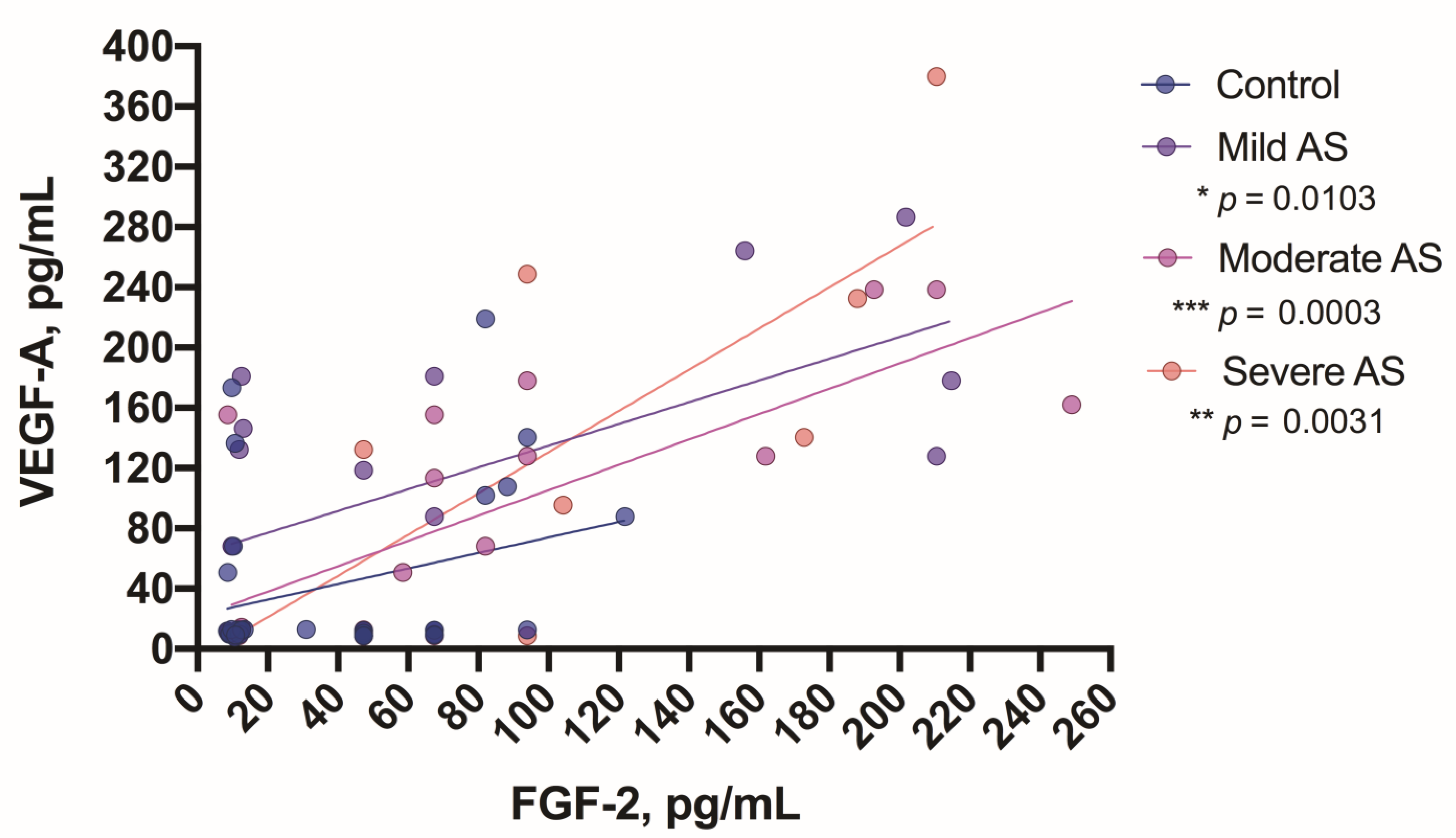
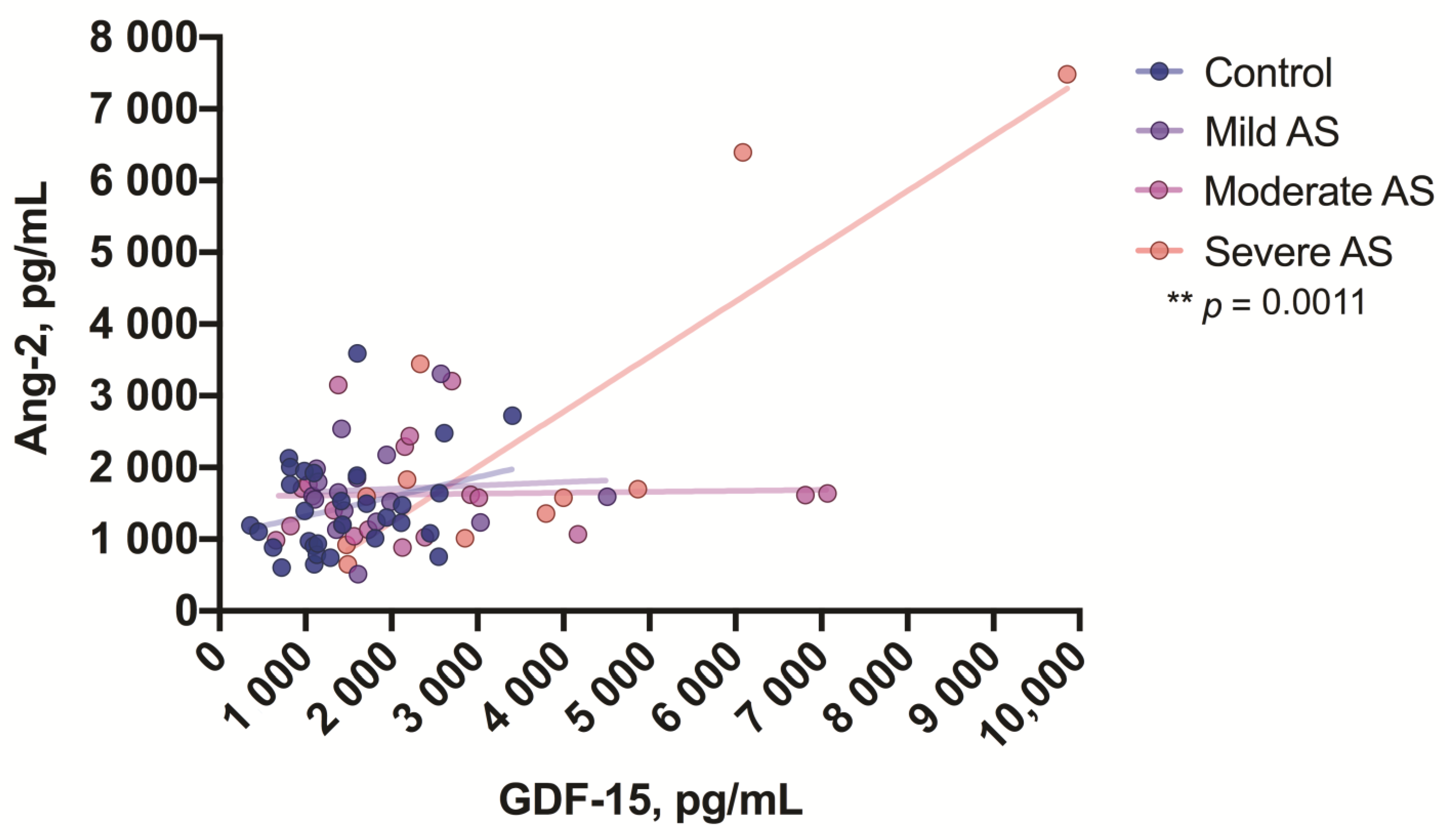
3.7. Correlations between the Study Growth Factors
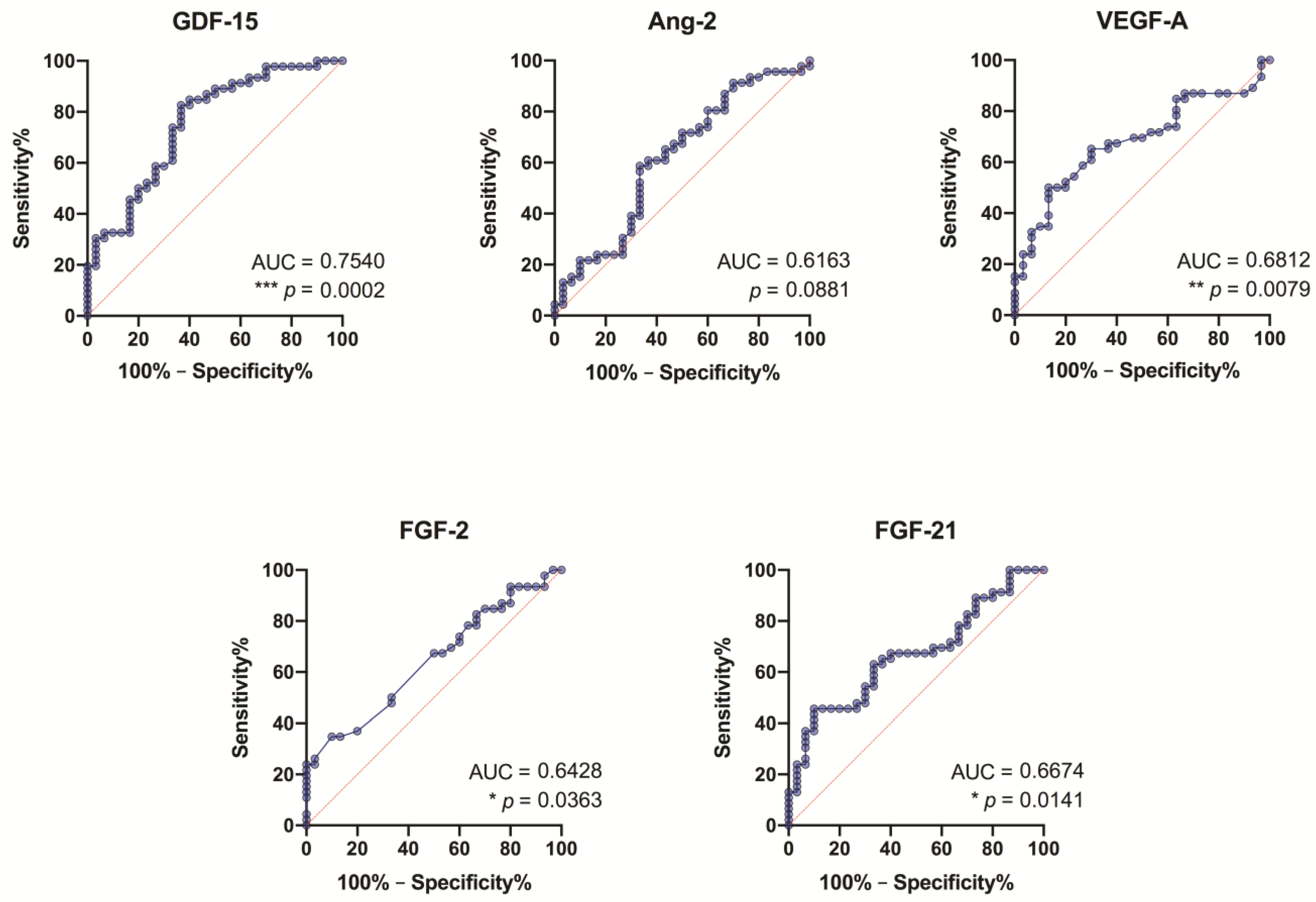
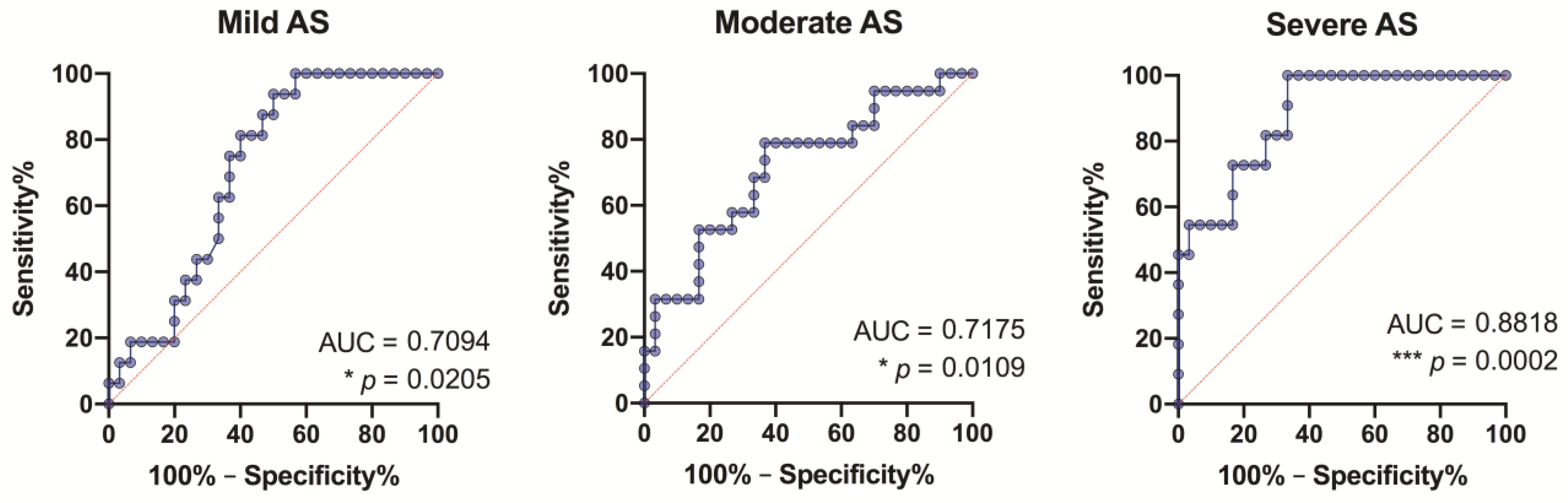
3.8. ROC Analysis of the Study Growth Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanatani, S.; Izumiya, Y.; Takashio, S.; Kojima, S.; Yamamuro, M.; Araki, S.; Rokutanda, T.; Tsujita, K.; Yamamoto, E.; Tanaka, T.; et al. Growth differentiation factor 15 can distinguish between hypertrophic cardiomyopathy and hypertensive hearts. Heart Vessels 2014, 29, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Montoro-García, S.; Hernández-Romero, D.; Jover, E.; García-Honrubia, A.; Vilchez, J.A.; Casas, T.; Martínez, P.; Climent, V.; Caballero, L.; Valdés, M.; et al. Growth differentiation factor-15, a novel biomarker related with disease severity in patients with hypertrophic cardiomyopathy. Eur. J. Intern. Med. 2012, 23, 169–174. [Google Scholar] [CrossRef]
- Toutouzas, K.; Stathogiannis, K.; Latsios, G.; Synetos, A.; Drakopoulou, M.; Penesopoulou, V.; Michelongona, A.; Tsiamis, E.; Tousoulis, D. Biomarkers in Aortic Valve Stenosis and their Clinical Significance in Transcatheter Aortic Valve Implantation. Curr. Med. Chem. 2019, 26, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Kobayashi, Y.; Moneghetti, K.J.; Brenner, D.A.; O’Malley, R.; Schnittger, I.; Wu, J.C.; Murtagh, G.; Beshiri, A.; Fischbein, M.; et al. GDF-15 (Growth Differentiation Factor 15) Is Associated with Lack of Ventricular Recovery and Mortality after Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2017, 10, e005594. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wei, L.; Yang, X.; Zhong, J.J. Roles of Growth Differentiation Factor 15 in Atherosclerosis and Coronary Artery Disease. Am. Heart Assoc. 2019, 8, e012826. [Google Scholar] [CrossRef] [PubMed]
- Scholz, A.; Plate, K.H.; Reiss, Y. Angiopoietin-2: A multifaceted cytokine that functions in both angiogenesis and inflammation. Ann. N. Y. Acad. Sci. 2015, 1347, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Arevalos, C.A.; Berg, J.M.; Nguyen, J.M.; Godfrey, E.L.; Iriondo, C.; Grande-Allen, K.J. Valve Interstitial Cells Act in a Pericyte Manner Promoting Angiogensis and Invasion by Valve Endothelial Cells. Ann. Biomed. Eng. 2016, 44, 2707–2723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, R.M.; Miller, J.D.; Heistad, D.D. Fibrocalcific aortic valve disease: Opportunity to understand disease mechanisms using mouse models. Circ. Res. 2013, 113, 209–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinvil, A.; Arbel, Y.; Topilsky, Y.; Barak, L.; Entin-Meer, M.; Levy, R.; Schwartz, A.L.; Keren, G.; Finkelstein, A.; Banai, S. Sustained Elevation of Vascular Endothelial Growth Factor and Angiopoietin-2 Levels After Transcatheter Aortic Valve Replacement. Can. J. Cardiol. 2016, 32, 1454–1461. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, A.G.; Schroeder, M.E.; Walker, C.J.; Anseth, C.J. FGF-2 inhibits contractile properties of valvular interstitial cell myofibroblasts encapsulated in 3D MMP-degradable hydrogels. APL Bioeng. 2018, 2, 046104. [Google Scholar] [CrossRef] [PubMed]
- Planavila, A.; Redondo-Angulo, I.; Villarroya, F. FGF21 and Cardiac Physiopathology. Front. Endocrinol. 2015, 6, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenart-Lipińska, M.; Duma, D.; Hałabiś, M.; Dziedzic, M.; Solski, J. Fibroblast growth factor 21—A key player in cardiovascular disorders? Horm. Mol. Biol. Clin. Investig. 2016, 30. [Google Scholar] [CrossRef]
- Lurins, J.; Lurina, D.; Tretjakovs, P.; Mackevics, V.; Lejnieks, A.; Rapisarda, V.; Baylon, V. Increased serum chemerin level to predict early onset of aortic valve stenosis. Biomed. Rep. 2018, 8, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto, M.E.; Salas, J.L.; Vargas-Barron, J.; Marquez, R.; Rodriguez-Hernandez, A.; Bojalil-Parra, R.; Pérez-Torres, I.; Guarner-Lans, V. Pre- and post-surgical evaluation of the inflammatory response in patients with aortic stenosis treated with different types of prosthesis. BMC Cardiovasc. Disord. 2017, 17, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahanian, A.; Iung, B. The new ESC/EACTS guidelines on the management of valvular heart disease. Arch. Cardiovasc. Dis. 2012, 105, 465–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahanian, A.; Alfieri, O.; Andreotti, F.; Antunes, M.J.; Barón-Esquivias, G.; Baumgartner, H.; Borger, M.A.; Carrel, T.P.; De Bonis, M.; Evangelista, A.; et al. Guidelines on the management of valvular heart disease (version 2012): The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. J. Cardiothorac. Surg. 2012, 42, S1–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabiani, I.; Santoni, T.; Angelillis, M.; Petricciuolo, S.; Colli, A.; Pellegrini, G.; Mazzei, D.; Pugliese, M.R.; Petronio, A.S.; De Caterina, R. Growth Differentiation Factor 15 in Severe Aortic Valve Stenosis: Relationship with Left Ventricular Remodeling and Frailty. J. Clin. Med. 2020, 9, 2998. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Shao, M.; Liu, H.; Chen, J.; Hu, J.; Zhu, L.; Liu, F.; Wang, D.; Zou, Y.; Xiong, Y.; et al. Fibroblast growth factor 21 enhances angiogenesis and wound healing of human brain microvascular endothelial cells by activating PPARγ. J. Pharmacol. Sci. 2019, 140, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, D.D.; Tuttolomondo, A.; Musiari, G.; Schimmenti, C.; D’Angelo, A.; Pinto, A. Are the Myokines the Mediators of Physical Activity-Induced Health Benefits? Curr. Pharm. Des. 2016, 22, 3622–3647. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls n = 30 | Mild Aortic Valve Stenosis n = 16 | Moderate Aortic Valve Stenosis n = 19 | Severe Aortic Valve Stenosis n = 11 | ||
|---|---|---|---|---|---|
| Gender (%) | Male Female | 6 (20) 24 (80) | 1 (6) 15 (94) | 8 (42) 11 (58) | 7 (64) 4 (36) |
| Age (years) | Mdn (IQR) | 70 (60–75) | 72 (66–75) | 74 (65–79) | 69 (60–75) |
| 1 BMI | M (±SD) p-value vs. control | 27.97 (5.10) | 29.53 (4.97) p = 0.16 | 27.18 (4.76) p = 0.19 | 27.02 (4.04) p = 0.30 |
| 2 SV (mL) | M (±SD) p-value vs. control | 81.97 (22.20) | 72.13 (11.99) p = 0.26 | 79.89 (20.45) p = 0.45 | 78.09 (17.39) p = 0.12 |
| 3 EF (%) | M (±SD) p-value vs. control | 61.22 (6.44) | 57.58 (9.79) p = 0.17 | 61.32 (8,24) p = 0.17 | 57.73 (8,65) p = 0.15 |
| 4 SVI | M (±SD) p-value vs. control | 44.45 (11.19) | 39.26 (8.39) p = 0.38 | 42.36 (11.67) p = 0.51 | 41.97 (9.99) p = 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmanis, J.; Tretjakovs, P.; Svirskis, S.; Gersone, G.; Hofmane, D.; Rozenberga, U.; Blumfelds, L.; Bahs, G.; Lejnieks, A.; Mackevics, V. Prognostic Utility of Circulating Growth Factors in Aortic Valve Stenosis: A Pilot Study. Medicina 2021, 57, 78. https://doi.org/10.3390/medicina57010078
Hofmanis J, Tretjakovs P, Svirskis S, Gersone G, Hofmane D, Rozenberga U, Blumfelds L, Bahs G, Lejnieks A, Mackevics V. Prognostic Utility of Circulating Growth Factors in Aortic Valve Stenosis: A Pilot Study. Medicina. 2021; 57(1):78. https://doi.org/10.3390/medicina57010078
Chicago/Turabian StyleHofmanis, Juris, Peteris Tretjakovs, Simons Svirskis, Gita Gersone, Dace Hofmane, Ulla Rozenberga, Leons Blumfelds, Guntis Bahs, Aivars Lejnieks, and Vitolds Mackevics. 2021. "Prognostic Utility of Circulating Growth Factors in Aortic Valve Stenosis: A Pilot Study" Medicina 57, no. 1: 78. https://doi.org/10.3390/medicina57010078