Imaging Characterization of Renal Masses


Abstract
:1. Introduction
2. Imaging Tools to Characterize Renal Masses
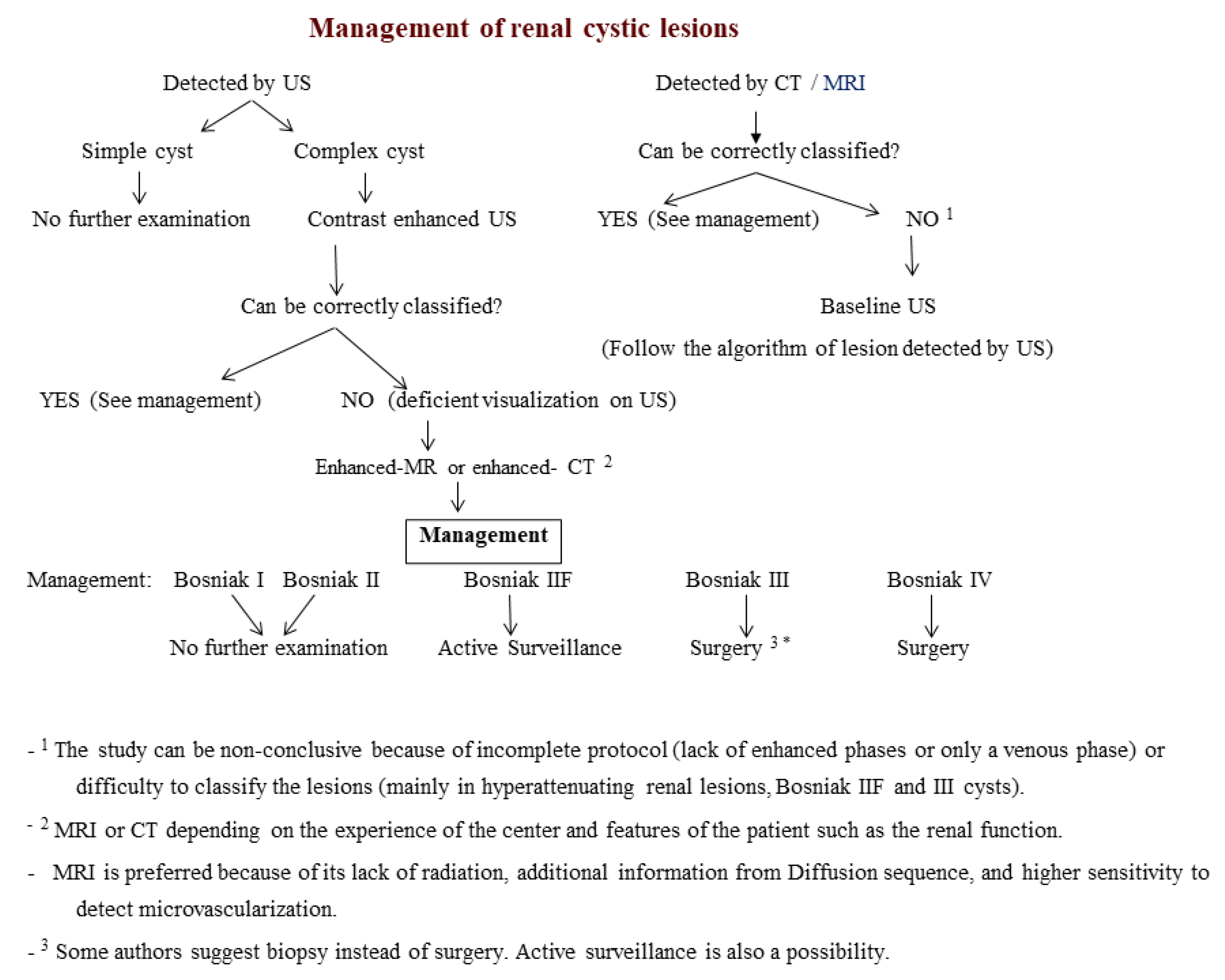
3. Characterization of Cystic Masses
Bosniak Classification
4. Characterization of Solid Masses
4.1. Nodular Masses
4.2. Infiltrative Masses
Author Contributions
Funding
Conflicts of Interest
References
- Nicolau, C.; Aldecoa, I.; Bunesch, L.; Mallofre, C.; Sebastia, C. The Role of Contrast Agents in the Diagnosis of Renal Diseases. Curr. Probl. Diagn. Radiol. 2015, 44, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.K.; Huang, W.C.; Pandharipande, P.V.; Chandarana, H. Solid renal masses: What the numbers tell us. AJR Am. J. Roentgenol. 2014, 202, 1196–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidhu, P.S.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.A.; Cosgrove, D.; et al. The EFSUMB guidelines and recommendations for the clinical practice of contrast-enhanced ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Long Version). Ultraschall Med. Eur. J. Ultrasound 2018, 39, e2–e44. [Google Scholar]
- Deng, Y.; Soule, E.; Samuel, A.; Shah, S.; Cui, E.; Asare-Sawiri, M.; Sundaram, C.; Lall, C.; Sandrasegaran, K. CT texture analysis in the differentiation of major renal cell carcinoma subtypes and correlation with Fuhrman grade. Eur. Radiol. 2019, 29, 6922–6929. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Tan, Q.; Mao, W.; Dai, C.; Hu, X.; Hou, J.; Zeng, M.; Zhou, J. Differentiating between malignant and benign renal tumors: Do IVIM and diffusion kurtosis imaging perform better than DWI? Eur. Radiol. 2019, 29, 6930–6939. [Google Scholar] [CrossRef] [PubMed]
- Sasaguri, K.; Takahashi, N. CT and MR imaging for solid renal mass characterization. Eur. J. Radiol. 2018, 99, 40–54. [Google Scholar] [CrossRef]
- Lassel, E.A.; Rao, R.; Schwenke, C.; Schoenberg, S.O.; Michaely, H.J. Diffusion-weighted imaging of focal renal lesions: A meta-analysis. Eur. Radiol. 2014, 24, 241–249. [Google Scholar] [CrossRef]
- Dai, C.; Cao, Y.; Jia, Y.; Ding, Y.; Sheng, R.; Zeng, M.; Zhou, J. Differentiation of renal cell carcinoma subtypes with different iodine quantification methods using single-phase contrast-enhanced dual-energy CT: Areal vs. volumetric analyses. Abdom. Radiol. 2018, 43, 672–678. [Google Scholar] [CrossRef]
- Mileto, A.; Nelson, R.C.; Paulson, E.K.; Marin, D. Dual-Energy MDCT for Imaging the Renal Mass. Am. J. Roentgenol. 2015, 204, W640–W647. [Google Scholar] [CrossRef]
- Coy, H.; Young, J.R.; Douek, M.L.; Brown, M.S.; Sayre, J.; Raman, S.S. Quantitative computer-aided diagnostic algorithm for automated detection of peak lesion attenuation in differentiating clear cell from papillary and chromophobe renal cell carcinoma, oncocytoma, and fat-poor angiomyolipoma on multiphasic multidetector com. Abdom. Radiol. 2017, 42, 1919–1928. [Google Scholar] [CrossRef]
- Siddaiah, M.; Krishna, S.; McInnes, M.D.; Quon, J.S.; Shabana, W.M.; Papadatos, D.; Schieda, N. Is ultrasound useful for further evaluation of homogeneously hyperattenuating renal lesions detected on CT? Am. J. Roentgenol. 2017, 209, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S.G.; Pedrosa, I.; Ellis, J.H.; Hindman, N.M.; Schieda, N.; Smith, A.D.; Remer, E.M.; Shinagare, A.B.; Curci, N.E.; Raman, S.S.; et al. Bosniak classification of cystic renal masses, version 2019: An update proposal and needs assessment. Radiology 2019, 292, 475–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miskin, N.; Qin, L.; Matalon, S.A.; Tirumani, S.H.; Alessandrino, F.; Silverman, S.G.; Shinagare, A.B. Stratification of cystic renal masses into benign and potentially malignant: Applying machine learning to the bosniak classification. Abdom. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bosniak, M.A. The Bosniak renal cyst classification: 25 Years later. Radiology 2012, 262, 781–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Israel, G.M.; Silverman, S.G. The incidental renal mass. Radiol. Clin. North Am. 2011, 49, 369–383. [Google Scholar] [CrossRef]
- Bielskienė, N.; Augustinavičius, V.; Valančienė, D.; Tamošiūnas, A.E.; Jankevičius, F. Bosniak category III renal lesions: Likelihood of malignancy based on computed tomography findings. Cent. Eur. J. Urol. 2018, 71, 58–63. [Google Scholar] [CrossRef]
- Pruthi, D.K.; Liu, Q.; Kirkpatrick, I.D.C.; Gelfond, J.; Drachenberg, D.E. Long-Term Surveillance of Complex Cystic Renal Masses and Heterogeneity of Bosniak 3 Lesions. J. Urol. 2018, 200, 1192–1199. [Google Scholar] [CrossRef]
- Reese, A.C.; Johnson, P.T.; Gorin, M.A.; Pierorazio, P.M.; Allaf, M.E.; Fishman, E.K.; Netto, G.J.; Pavlovich, C.P. Pathological characteristics and radiographic correlates of complex renal cysts. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 1010–1016. [Google Scholar] [CrossRef] [Green Version]
- Sebastià, C.; Corominas, D.; Musquera, M.; Paño, B.; Ajami, T.; Nicolau, C. Active surveillance of small renal masses. Insights Imaging 2020, 11, 63. [Google Scholar] [CrossRef]
- Kashan, M.; Ghanaat, M.; Hötker, A.M.; Duzgol, C.; Sanchez, A.; Di Natale, R.G.; Blum, K.A.; Becerra, M.F.; Manley, B.J.; Casuscelli, J.; et al. Cystic Renal Cell Carcinoma: A Report on Outcomes of Surgery and Active Surveillance in Patients Retrospectively Identified on Pretreatment Imaging. J. Urol. 2018, 200, 275–282. [Google Scholar] [CrossRef]
- Boissier, R.; Ouzaid, I.; Nouhaud, F.X.; Khene, Z.; Dariane, C.; Chkir, S.; Chelly, S.; Giwerc, A.; Allenet, C.; Lefrancq, J.B.; et al. Long-term oncological outcomes of cystic renal cell carcinoma according to the Bosniak classification. Int. Urol. Nephrol. 2019, 51, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Israel, G.M.; Hindman, N.; Bosniak, M.A. Evaluation of cystic renal masses: Comparison of CT and MR imaging by using the Bosniak classification system. Radiology 2004, 231, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Nicolau, C.; Bunesch, L.; Sebastia, C. Renal complex cysts in adults: Contrast-enhanced ultrasound. Abdom. Imaging 2011, 36, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Liu, J.J.K.; Zheng, Y.; Tan, C.H. Bosniak classification of cystic renal masses: Utility of contrastenhanced ultrasound using version 2019. Med. Ultrason. 2020, 22, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Park, B.K.; Kim, B.; Kim, S.H.; Ko, K.; Lee, H.M.; Choi, H.Y. Assessment of cystic renal masses based on Bosniak classification: Comparison of CT and contrast-enhanced US. Eur. J. Radiol. 2007, 61, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Nicolau, C.; Bunesch, L.; Paño, B.; Salvador, R.; Ribal, M.J.; Mallofré, C.; Sebastià, C. Prospective evaluation of CT indeterminate renal masses using US and contrast-enhanced ultrasound. Abdom. Imaging. 2015, 40, 542–551. [Google Scholar] [CrossRef]
- Bertolotto, M.; Cicero, C.; Perrone, R.; Degrassi, F.; Cacciato, F.; Cova, M.A. Renal masses with equivocal enhancement at CT: Characterization with contrast-enhanced ultrasound. Am. J. Roentgenol. 2015, 204, W557–W565. [Google Scholar] [CrossRef]
- Clevert, D.A.; Minaifar, N.; Weckbach, S.; Jung, E.M.; Stock, K.; Reiser, M.; Staehler, M. Multislice computed tomography versus contrast-enhanced ultrasound in evaluation of complex cystic renal masses using the Bosniak classification system. Clin. Hemorheol. Microcirc. 2008, 39, 171–178. [Google Scholar] [CrossRef]
- Zhong, J.; Cao, F.; Guan, X.; Chen, J.; DIng, Z.; Zhang, M. Renal cyst masses (Bosniak category II-III) may be over evaluated by the Bosniak criteria based on MR findings. Medicine 2017, 96, e9361. [Google Scholar] [CrossRef]
- Inci, E.; Hocaoglu, E.; Aydin, S.; Cimilli, T. Diffusion-weighted magnetic resonance imaging in evaluation of primary solid and cystic renal masses using the Bosniak classification. Eur. J. Radiol. 2012, 81, 815–820. [Google Scholar] [CrossRef]
- Balyemez, F.; Aslan, A.; Inan, I.; Ayaz, E.; Karagöz, V.; Özkanli, S.Ş.; Acar, M. Diffusion-weighted magnetic resonance imaging in cystic renal masses. Can. Urol Assoc. J. 2017, 11, E8–E14. [Google Scholar] [CrossRef] [PubMed]
- Harisinghani, M.G.; Maher, M.M.; Gervais, D.A.; McGovern, F.; Hahn, P.; Jhaveri, K.; Varghese, J.; Mueller, P.R. Incidence of malignancy in complex cystic renal masses (Bosniak category III): Should imaging-guided biopsy precede surgery? Am. J. Roentgenol. 2003, 180, 755–758. [Google Scholar] [CrossRef] [PubMed]
- Jamis-Dow, C.A.; Choyke, P.L.; Jennings, S.B.; Linehan, W.M.; Thakore, K.N.; Walther, M.M. Small (≤3-cm) renal masses: Detection with CT versus US and pathologic correlation. Radiology 1996, 198, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Kay, F.U.; Pedrosa, I. Imaging of Solid Renal Masses. Radiol. Clin. N. Am. 2017, 55, 243–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, M.; Suzuki, T.; Suzuki, Y.; Terasawa, Y.; Sasano, H.; Arai, Y. Natural history of small renal cell carcinoma: Evaluation of growth rate, histological grade, cell proliferation and apoptosis. J. Urol. 2004, 172, 863–866. [Google Scholar] [CrossRef]
- Sunela, K.L.; Lehtinen, E.T.; Kataja, M.J.; Kujala, P.M.; Soimakallio, S.; Kellokumpu-Lehtinen, P.L.I. Development of renal cell carcinoma (RCC) diagnostics and impact on prognosis. BJU Int. 2014, 113, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]
- Cheville, J.C.; Lohse, C.M.; Zincke, H.; Weaver, A.L.; Blute, M.L. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am. J. Surg Pathol. 2003, 27, 612–624. [Google Scholar] [CrossRef]
- Inamura, K. Renal cell tumors: Understanding their molecular pathological epidemiology and the 2016 WHO classification. Int. J. Mol. Sci. 2017, 18, 2195. [Google Scholar] [CrossRef] [Green Version]
- Outwater, E.K.; Bhatia, M.; Siegelman, E.S.; Burke, M.A.; Mitchell, D.G. Lipid in renal clear cell carcinoma: Detection on opposed-phase gradient-echo MR images. Radiology 1997, 205, 103–107. [Google Scholar] [CrossRef]
- Pedrosa, I.; Sun, M.R.; Spencer, M.; Genega, E.M.; Olumi, A.F.; Dewolf, W.C.; Rofsky, N.M. MR imaging of renal masses: Correlation with findings at surgery and pathologic analysis. Radiographics 2008, 28, 985–1003. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, N.R.; Davis, N.F.; Flynn, R.; McDermott, T.; Thornhill, J.A.; Manecksha, R.P. Dilemmas in diagnosis and natural history of renal oncocytoma and implications for management. J. Can. Urol. Assoc. 2015, 9, E709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, D.H.; Zisman, A.; Pantuck, A.J.; Freedland, S.J.; Said, J.W.; Belldegrun, A.S. Changing concepts in the management of renal oncocytoma. Urology 2002, 59, 635–642. [Google Scholar] [CrossRef]
- Perez-Ordonez, B.; Hamed, G.; Campbell, S.; Erlandson, R.A.; Russo, P.; Gaudin, P.B.; Reuter, V.E. Renal oncocytoma: A clinicopathologic study of 70 cases. Am. J. Surg. Pathol. 1997, 21, 871–883. [Google Scholar] [CrossRef]
- Zbar, B.; Glenn, G.; Merino, M.; Middelton, L.; Peterson, J.; Toro, J.; Coleman, J.; Pinto, P.; Schmidt, L.S.; Choyke, P.; et al. Familial Renal Carcinoma: Clinical Evaluation, Clinical Subtypes and Risk of Renal Carcinoma Development. J. Urol. 2007, 177, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Menko, F.H.; Van Steensel, M.A.; Giraud, S.; Friis-Hansen, L.; Richard, S.; Ungari, S.; Nordenskjöld, M.; vO Hansen, T.; Solly, J.; Maher, E.R.; et al. Birt-Hogg-Dubé syndrome: Diagnosis and management. Lancet Oncol. 2009, 10, 1199–1206. [Google Scholar] [CrossRef]
- Zhang, J.; Lefkowitz, R.A.; Ishill, N.M.; Wang, L.; Moskowitz, C.S.; Russo, P.; Eisenberg, H.; Hricak, H. Solid renal cortical tumors: Differentiation with CT. Radiology 2007, 244, 494–504. [Google Scholar] [CrossRef]
- Bird, V.G.; Kanagarajah, P.; Morillo, G.; Caruso, D.J.; Ayyathurai, R.; Leveillee, R.; Jorda, M. Differentiation of oncocytoma and renal cell carcinoma in small renal masses (<4 cm): The role of 4-phase computerized tomography. World J. Urol. 2011, 29, 787–792. [Google Scholar] [CrossRef]
- Woo, S.; Cho, J.Y.; Kim, S.H.; Kim, S.Y. Comparison of segmental enhancement inversion on biphasic MDCT between small renal oncocytomas and chromophobe renal cell carcinomas. AJR Am. J. Roentgenol. 2013, 201, 598–604. [Google Scholar] [CrossRef]
- Wu, J.; Zhu, Q.; Zhu, W.; Chen, W.; Wang, S. Comparative study of CT appearances in renal oncocytoma and chromophobe renal cell carcinoma. Acta Radiol. 2016, 57, 500–506. [Google Scholar] [CrossRef]
- Allen, B.C.; Tirman, P.; Jennings Clingan, M.; Manny, J.; Del Gaizo, A.J.; Leyendecker, J.R. Characterizing solid renal neoplasms with MRI in adults. Abdom. Imaging 2014, 39, 358–387. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, S.; Rajesh, A.; Mayer, N.J.; Mulcahy, K.A.; Haroon, A. Renal oncocytoma: CT features cannot reliably distinguish oncocytoma from other renal neoplasms. Clin. Radiol. 2009, 64, 517–522. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Hindman, N.; Fitzgerald, E.F.; Niver, B.E.; Melamed, J.; Babb, J.S. MRI features of renal oncocytoma and chromophobe renal cell carcinoma. AJR Am. J. Roentgenol. 2010, 195, W421–W427. [Google Scholar] [CrossRef] [PubMed]
- Schieda, N.; McInnes, M.D.F.; Cao, L. Diagnostic accuracy of segmental enhancement inversion for diagnosis of renal oncocytoma at biphasic contrast enhanced CT: Systematic review. Eur Radiol. 2014, 24, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.J.; Hayes, W.S.; Hartman, D.S.; McCarthy, W.F.; Davis, C.J. Renal oncocytoma and carcinoma: Failure of differentiation with CT. Radiology 1993, 186, 693–696. [Google Scholar] [CrossRef] [PubMed]
- El-Esawy, S.S.; Abou El-Ghar, M.E.; Gaballa, G.M.; Zahra, S.A. Characterization of solid renal masses using 64-slice multidetector CT scanner. Sci. World J. 2009, 9, 441–448. [Google Scholar] [CrossRef] [Green Version]
- Lee-Felker, S.A.; Felker, E.R.; Tan, N.; Margolis, D.J.; Young, J.R.; Sayre, J.; Raman, S.S. Qualitative and quantitative MDCT features for differentiating clear cell renal cell carcinoma from other solid renal cortical masses. AJR Am. J. Roentgenol. 2014, 203, W516–W524. [Google Scholar] [CrossRef]
- Paño, B.; Macías, N.; Salvador, R.; Torres, F.; Buñesch, L.; Sebastià, C.; Nicolau, C. Usefulness of MDCT to differentiate between renal cell carcinoma and oncocytoma: Development of a predictive model. Am. J. Roentgenol. 2016, 206, 764–774. [Google Scholar] [CrossRef]
- Hindman, N.; Ngo, L.; Genega, E.M.; Melamed, J.; Wei, J.; Braza, J.M.; Rofsky, N.M.; Pedrosa, I. Angiomyolipoma with Minimal Fat: Can It Be Differentiated from Clear Cell Renal Cell Carcinoma by Using Standard MR Techniques? Radiology 2012, 265, 468–477. [Google Scholar] [CrossRef]
- Jinzaki, M.; Silverman, S.G.; Akita, H.; Nagashima, Y.; Mikami, S.; Oya, M. Renal angiomyolipoma: A radiological classification and update on recent developments in diagnosis and management. Abdom. Imaging 2014, 39, 588–604. [Google Scholar] [CrossRef] [Green Version]
- Hodgdon, T.; Mcinnes, M.D.F.; Schieda, N.; Flood, T.A.; Lamb, L.; Thornhill, R.E. Can Quantitative cT Texture analysis be Used to Differentiate Fat-poor renal angiomyolipoma from renal cell carcinoma on Unenhanced cT images? Radiology 2015, 276, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Kay, F.U.; Pedrosa, I. Imaging of Solid Renal Masses. Urol. Clin. N. Am. 2018, 45, 311–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tordjman, M.; Mali, R.; Madelin, G.; Prabhu, V.; Kang, S.K. Diagnostic test accuracy of ADC values for identification of clear cell renal cell carcinoma: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 4023–4038. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Lin, M.; Ouyang, H.; Zhou, C.; Zhang, H. Application of ADC measurement in characterization of renal cell carcinomas with different pathological types and grades by 3.0 T diffusion-weighted MRI. Eur. J. Radiol. 2012, 81, 3061–3066. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cheng, L.; Zhang, X.; Wang, D.; Guo, A.; Gao, Y.; Ye, H. Renal cell carcinoma: Diffusion-weighted MR imaging for subtype differentiation at 3.0 T. Radiology 2010, 257, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Woolen, S.A.; Shankar, P.R.; Gagnier, J.J.; MacEachern, M.P.; Singer, L.; Davenport, M.S. Risk of Nephrogenic Systemic Fibrosis in Patients with Stage 4 or 5 Chronic Kidney Disease Receiving a Group II Gadolinium-Based Contrast Agent: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2020, 180, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Richard, P.O.; Jewett, M.A.; Bhatt, J.R.; Kachura, J.R.; Evans, A.J.; Zlotta, A.R.; Hermanns, T.; Juvet, T.; Finelli, A. Renal Tumor Biopsy for Small Renal Masses: A Single-center 13-year Experience. Eur. Urol. 2015, 68, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Maturen, K.E.; Nghiem, H.V.; Caoili, E.M.; Higgins, E.G.; Wolf, J.S.; Wood, D.P. Renal mass core biopsy: Accuracy and impact on clinical management. AJR Am. J. Roentgenol. 2007, 188, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.S.; Schieda, N.; Silverman, S.G. Update on Indications for Percutaneous Renal Mass Biopsy in the Era of Advanced CT and MRI. Am. J. Roentgenol. 2019, 212, 1187–1196. [Google Scholar] [CrossRef]
- Garstka, N.; Shariat, S.F.; Remzi, M. The evolving role of percutaneous biopsy in renal masses. Curr. Opin. Urol. 2018, 28, 364–368. [Google Scholar] [CrossRef]
- Ballard, D.H.; De Alba, L.; Migliaro, M.; Previgliano, C.H.; Sangster, G.P. CT imaging spectrum of infiltrative renal diseases. Abdom. Radiol. 2017, 42, 2700–2709. [Google Scholar] [CrossRef] [PubMed]
- Pickhardt, P.J.; Lonergan, G.J.; Davis, C.J.; Kashitani, N.; Wagner, B.J. From the archives of the AFIP. Infiltrative renal lesions: Radiologic-pathologic correlation. Armed Forces Institute of Pathology. Radiographics 2000, 20, 215–243. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Zhu, W.; Wu, J.; Chen, W. Imaging features of primary renal lymphoma. Acta Radiol. 2018, 59, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Beltran, A.; Carrasco, J.C.; Cheng, L.; Scarpelli, M.; Kirkali, Z.; Montironi, R. 2009 update on the classification of renal epithelial tumors in adults. Int. J. Urol. 2009, 16, 432–443. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. Renal Cell carcinoma EAU guidelines on renal cell carcinoma: The 2019 update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Taneja, R.; Bhargava, P.; Cuevas, C.; Dighe, M.K. Common and less-common renal masses and masslike conditions. Radiol Clin. N. Am. 2012, 50, 245–257. [Google Scholar] [CrossRef]
- Blitman, N.M.; Berkenblit, R.G.; Rozenblit, A.M.; Levin, T.L. Renal medullary carcinoma: CT and MRI features. Am. J. Roentgenol. 2005, 185, 268–272. [Google Scholar] [CrossRef]
- Muglia, V.F.; Prando, A. Renal cell carcinoma: Histological classification and correlation with imaging findings. Radiol. Bras. 2015, 48, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Raza, S.A.; Sohaib, S.A.; Sahdev, A.; Bharwani, N.; Heenan, S.; Verma, H.; Patel, U. Centrally infiltrating renal masses on CT: Differentiating intrarenal transitional cell carcinoma from centrally located renal cell carcinoma. Am. J. Roentgenol. 2012, 198, 846–853. [Google Scholar] [CrossRef]
- Zulfiqar, M.; Ubilla, C.V.; Nicola, R.; Menias, C.O. Imaging of Renal Infections and Inflammatory Disease. Radiol. Clin. N. Am. 2020, 58, 909–923. [Google Scholar] [CrossRef]
- Craig, W.D.; Wagner, B.J.; Travis, M.D. Pyelonephritis: Radiologic-pathologic review. Radiographics 2008, 28, 255–277. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Volpe, A. Platinum Priority—Editorial Renal Tumor Biopsy: More Dogma Belied. Eur. Urol. 2015, 68, 10142015. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nodular Renal Masses | |
|---|---|
| Renal cell carcinoma | Clear cell RCC 1 Papillary RCC Chromophobe RCC |
| Oncocytoma | |
| Angiomyolipoma | |
| Other malignant masses | Lymphoma Metastases Transitional cell carcinoma |
| Benign masses | Leiomyoma Adenoma |
| Pseudotumors | Prominent columns of Bertin, bulging of the renal contour focal renal hypertrophy |
| Renal Lesion | Morphologic Findings | MRI Signal Intensity | Enhancement | Diffusion |
|---|---|---|---|---|
| Typical AML | Macroscopic fat detection | Signal loss on Fat-saturation sequence. | Variable depending on the amount of adipose tissue, smooth muscle and blood vessels | No obvious restriction. Low signal on the ADC map due to the presence of fat. |
| Fat-poor AML | Hyperdense on unenhanced CT (basal CT) | Hypointense signal on T2 | Variable. Usually homogeneous and prolonged | No obvious restriction. |
| Oncocytoma | Central scar (<50% cases) | Variable, but mainly hyper- or iso-intense. | Hyperenhancement on corticomedullary phase. Segmental enhancement inversion 1 | No obvious restriction. |
| Clear cell RCC | Occasional calcifications. Occasional central scar. | May show loss of signal intensity on opposed-phased sequence (due to the presence of microscopic fat) | Hyperenhancement on corticomedullary phase Heterogeneous if haemorrhagic, cystic, or necrotic areas. | Variable restriction depending on the differentiation. |
| Papillary and chromophobe RCC | Occasional calcifications. | Papillary RCC may show hypointensity on T2. | Iso-hyperenhancement on nephrographic phase Homogeneous. Occasionally very scarce enhancement (papillary RCC). | Papillary RCC: Greater restriction than clear cell RCC. |
| Renal cell carcinoma | Clear cell, papillary, or chromophobe Renal medullary carcinoma Collecting duct carcinoma Sarcomatoid differentiation |
| Urothelial carcinoma | Transitional cell carcinoma Squamous cell carcinoma |
| Lymphoproliferative disease | Renal lymphoma Renal leukemia Extramedullary plasmacytoma |
| Metastases | |
| Inflammatory conditions and pseudotumors | Developmental renal pseudotumors Pyelonephritis/abscess Xanthogranulomatous pyelonephritis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolau, C.; Antunes, N.; Paño, B.; Sebastia, C. Imaging Characterization of Renal Masses. Medicina 2021, 57, 51. https://doi.org/10.3390/medicina57010051
Nicolau C, Antunes N, Paño B, Sebastia C. Imaging Characterization of Renal Masses. Medicina. 2021; 57(1):51. https://doi.org/10.3390/medicina57010051
Chicago/Turabian StyleNicolau, Carlos, Natalie Antunes, Blanca Paño, and Carmen Sebastia. 2021. "Imaging Characterization of Renal Masses" Medicina 57, no. 1: 51. https://doi.org/10.3390/medicina57010051