CT and MRI in Urinary Tract Infections: A Spectrum of Different Imaging Findings

Abstract
:1. Introduction
2. Cross-Sectional Imaging Features of Urinary Tract Infections
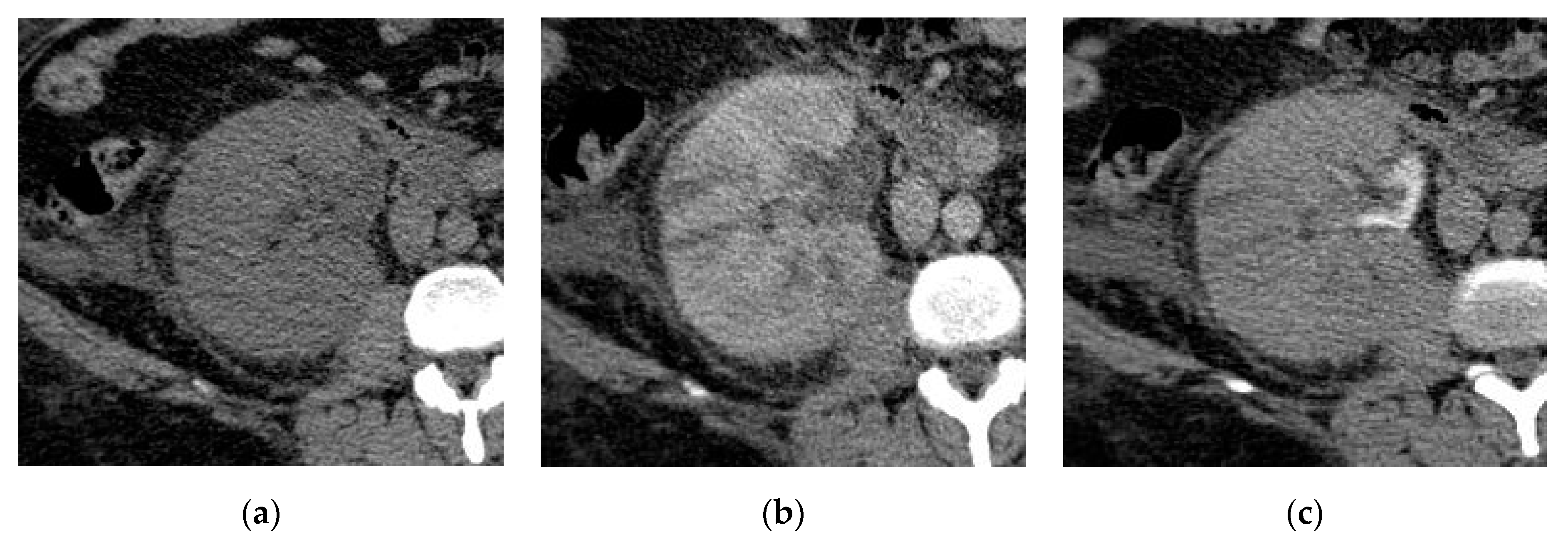
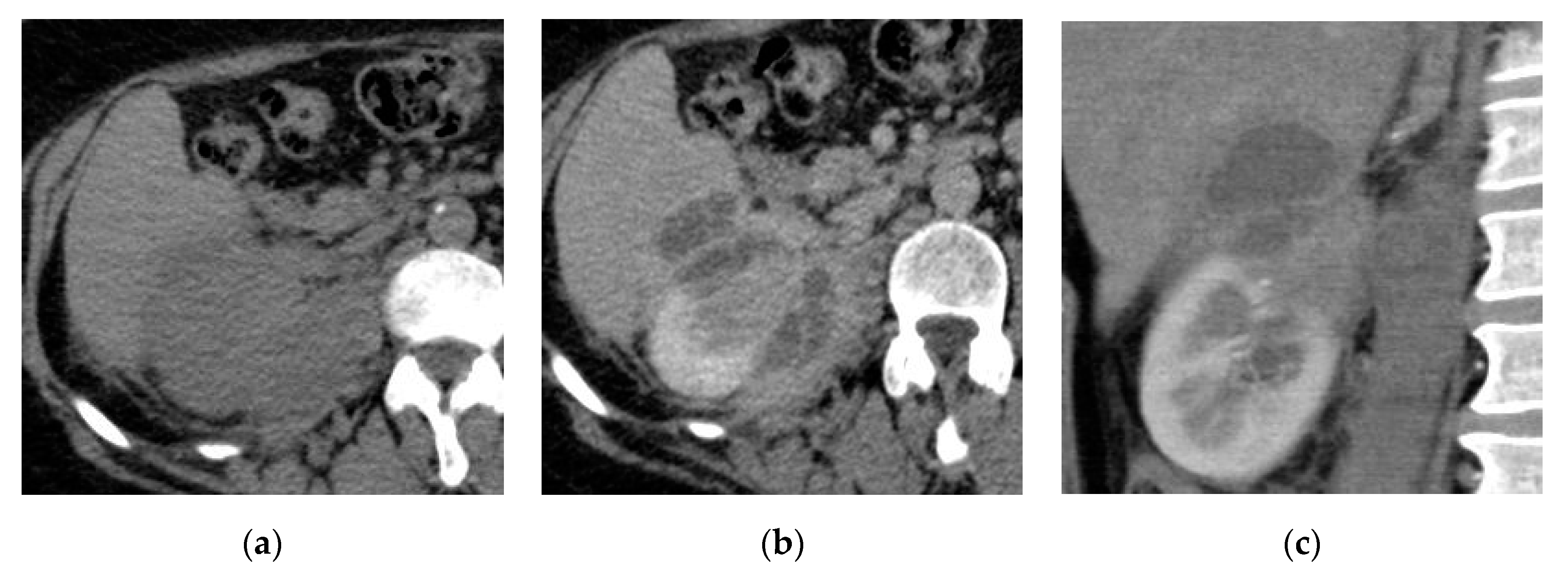
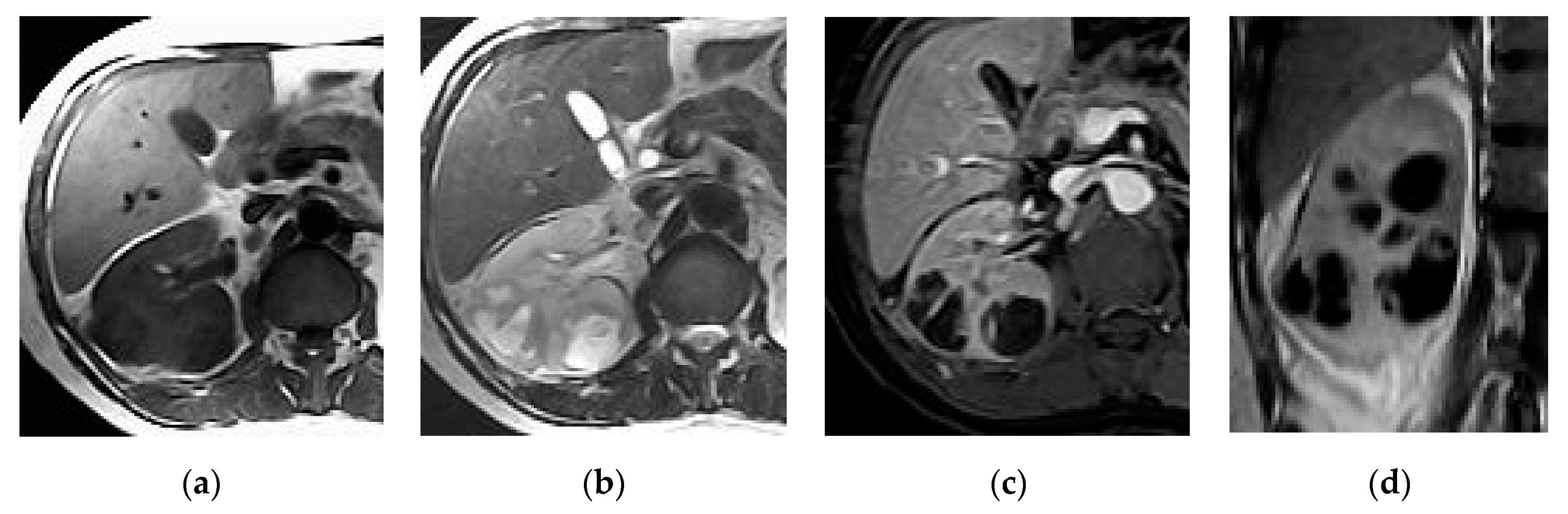
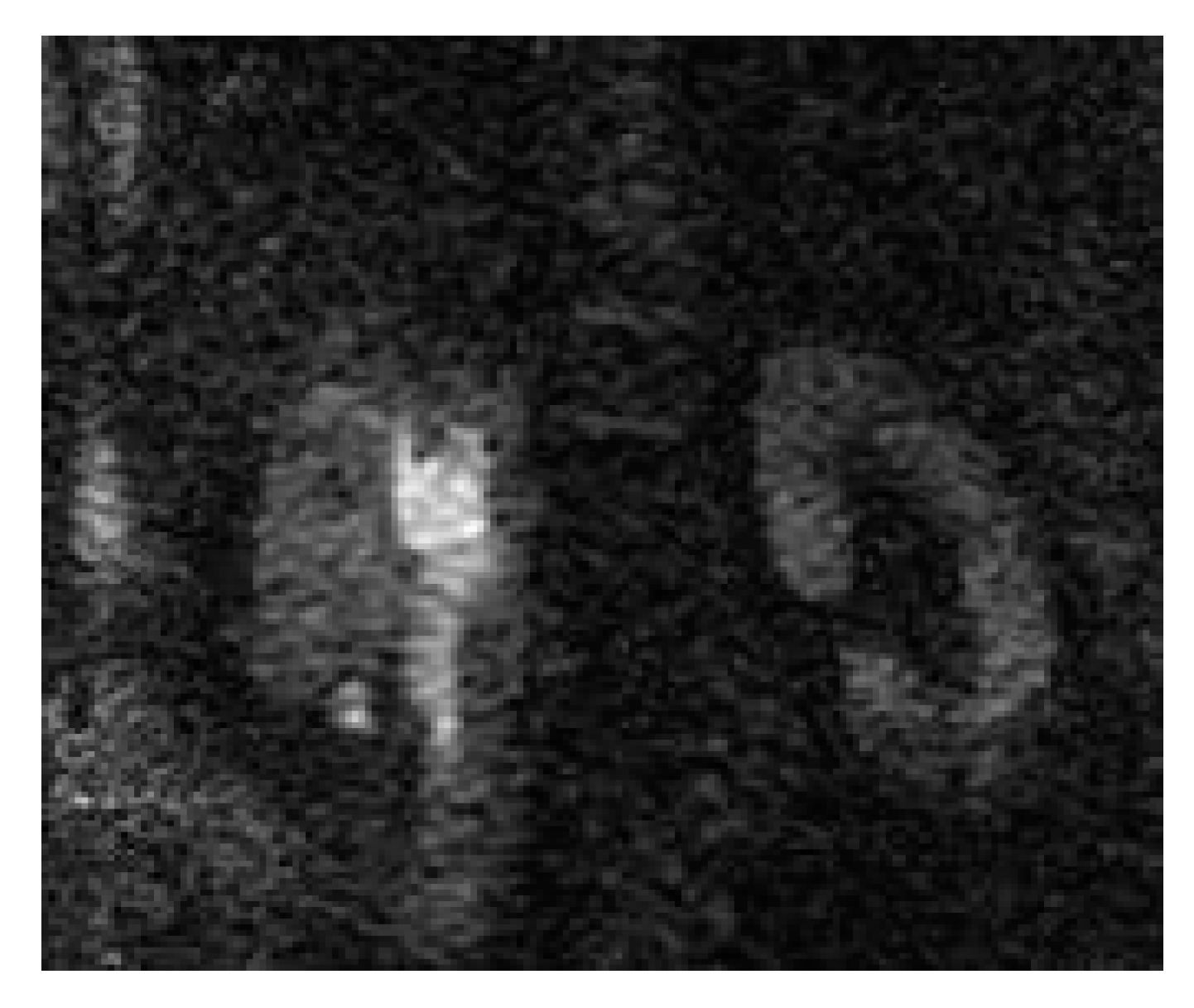
2.1. Acute Pyelonephritis
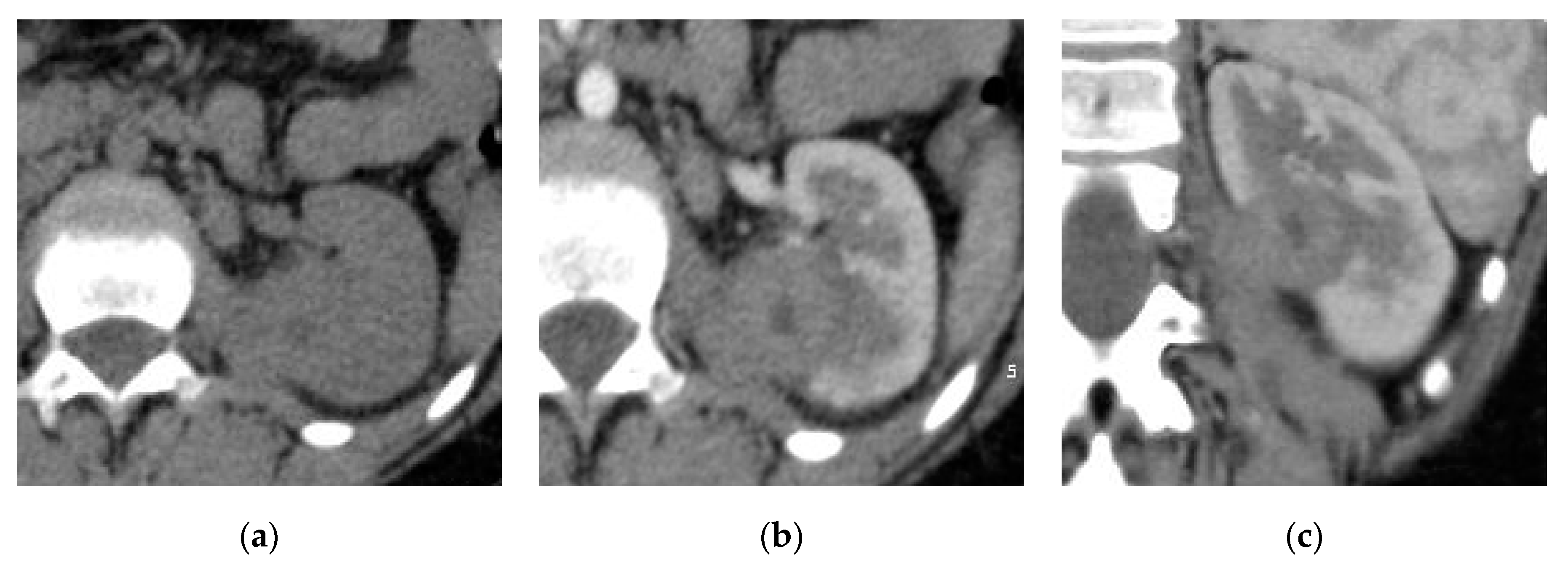
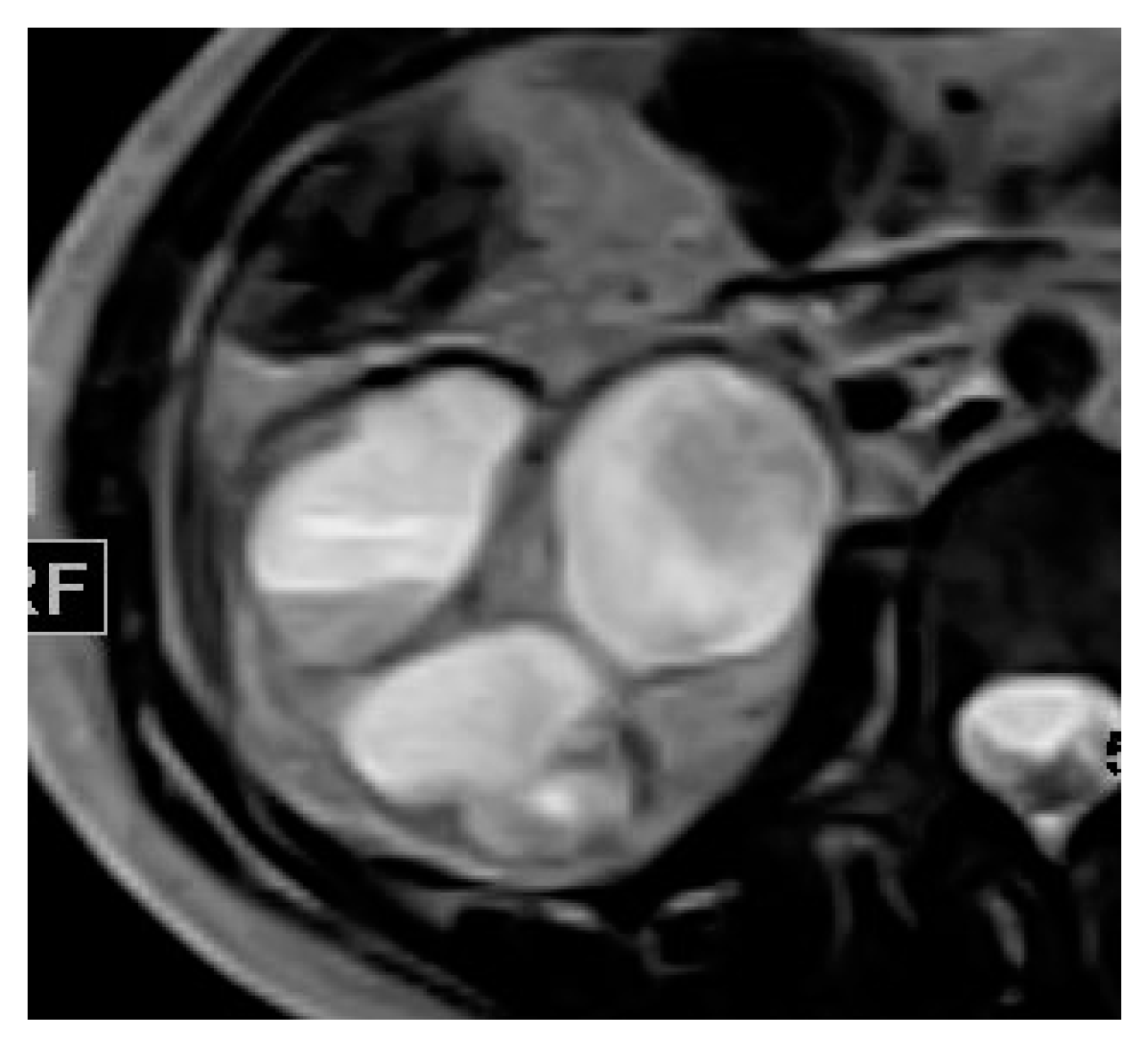
2.2. Renal and Perinephric Abscesses
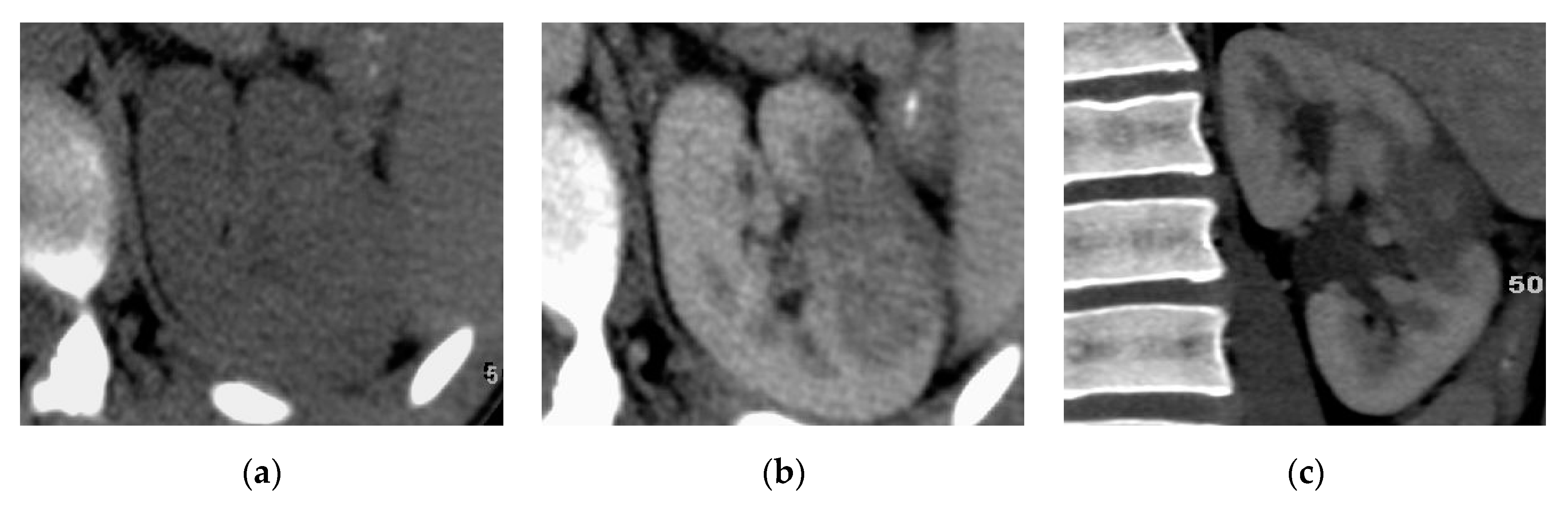
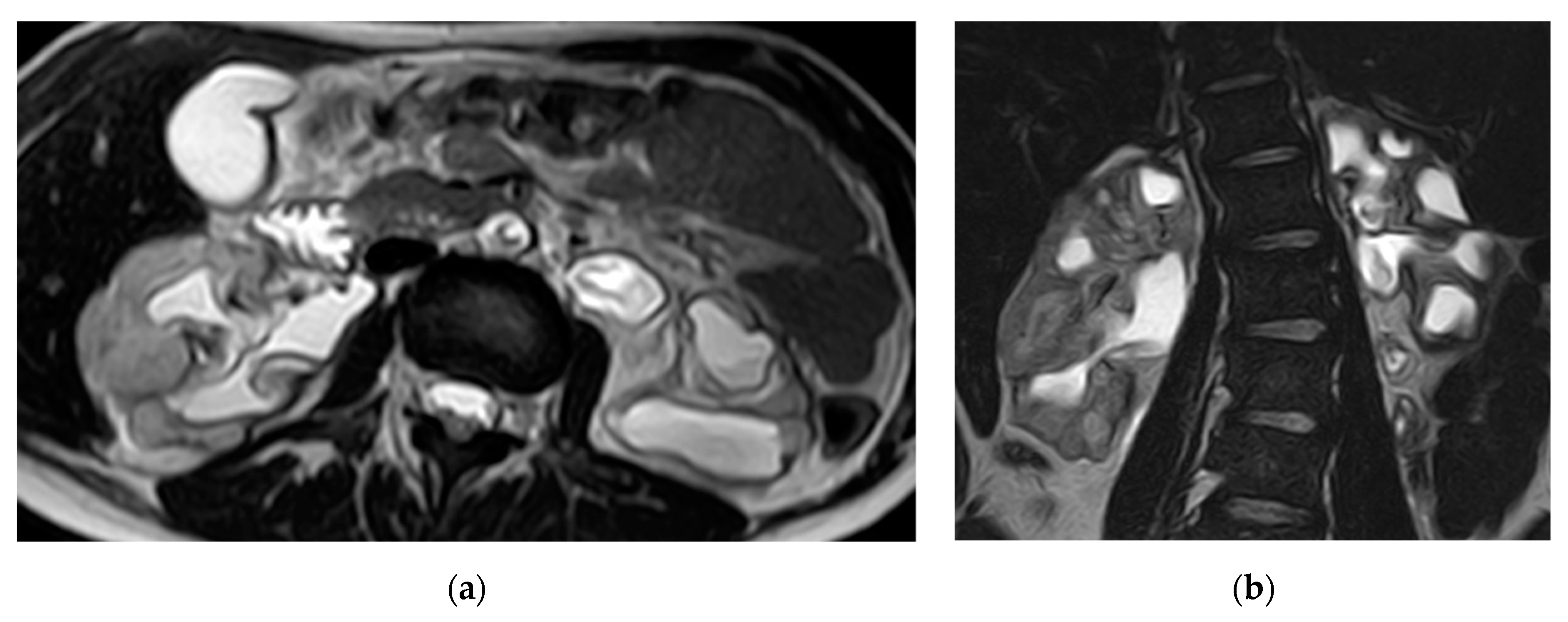
2.3. Pyonephrosis
2.4. Chronic Pyelonephritis
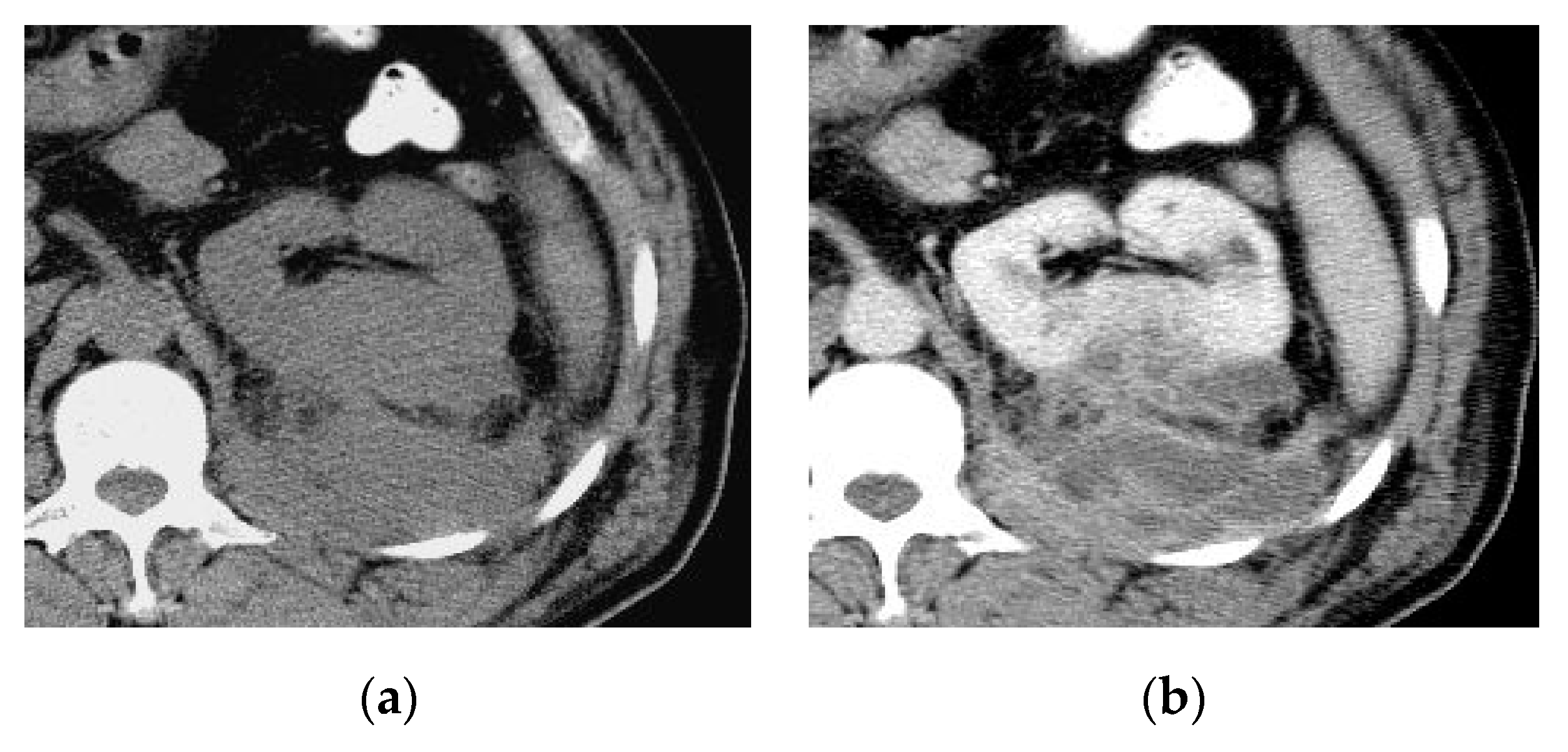
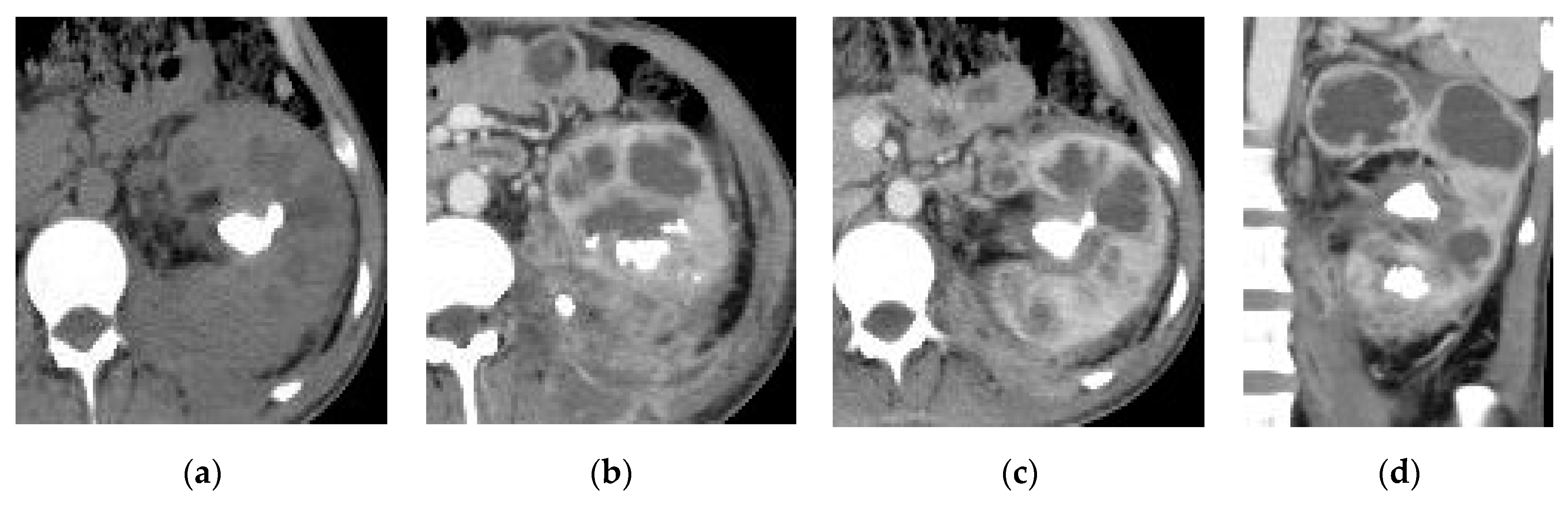
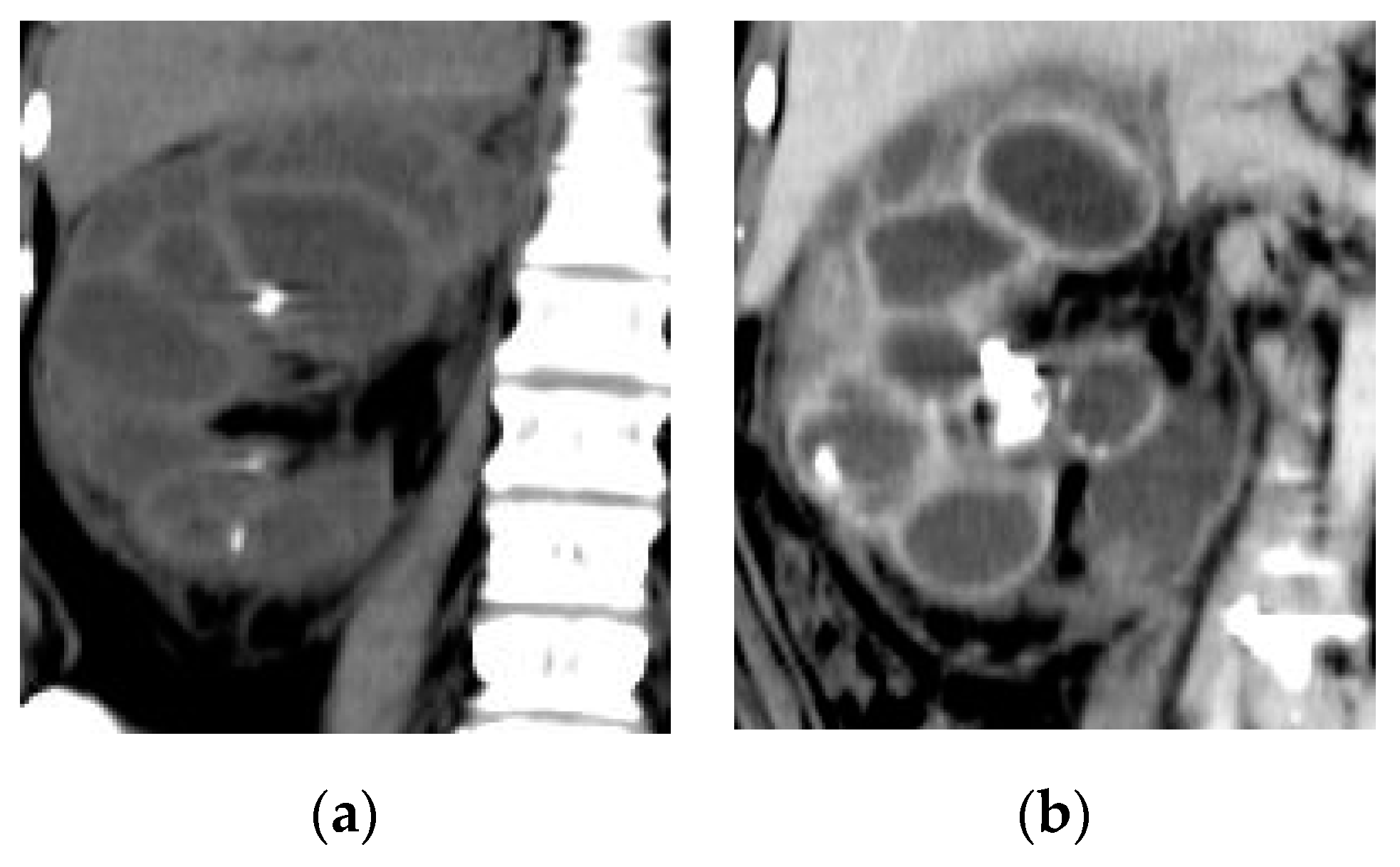
2.5. Xanthogranulomatous Pyelonephritis (XGP)
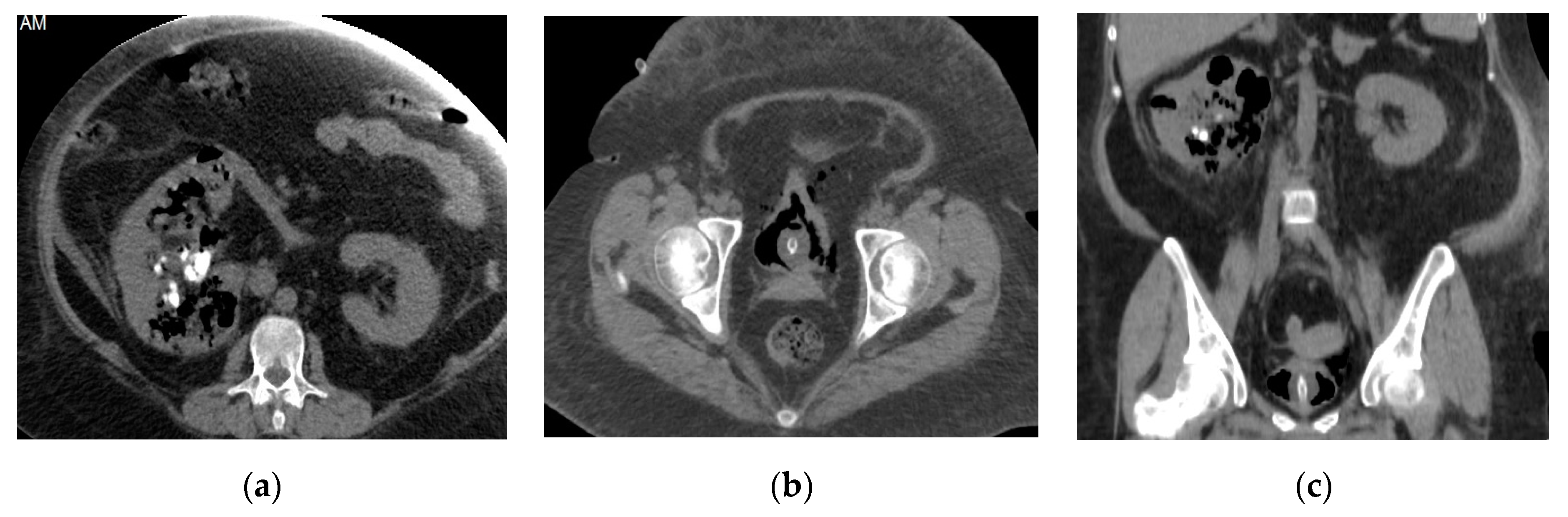
2.6. Emphysematous Urinary Tract Infection
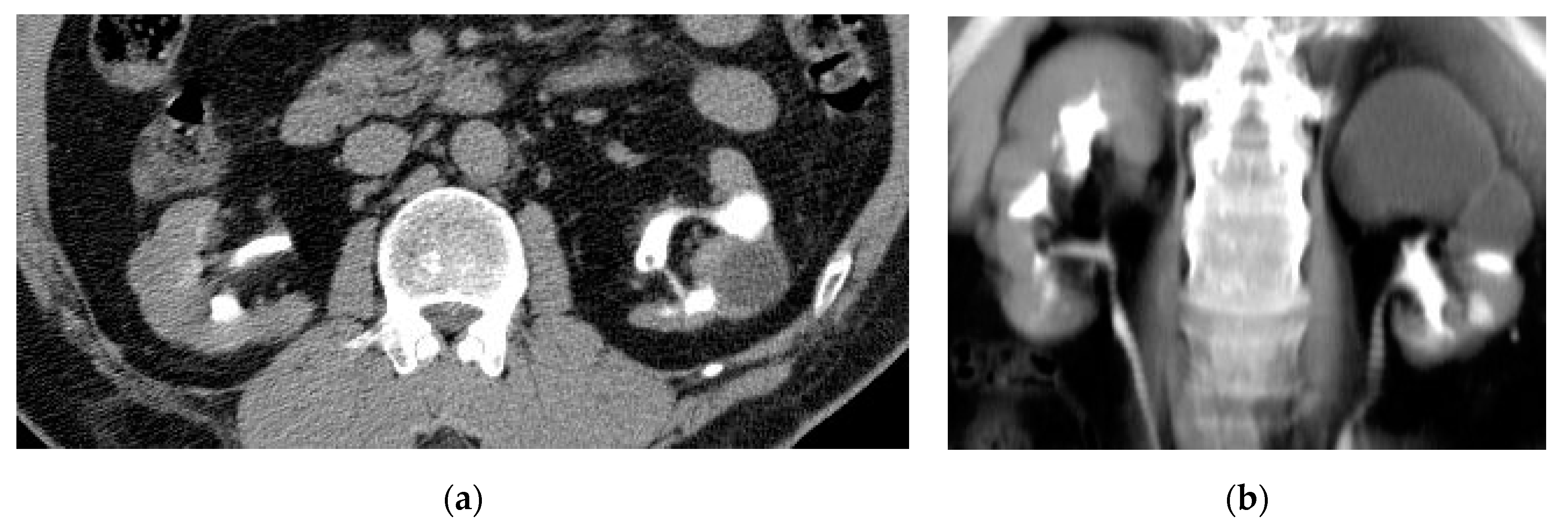
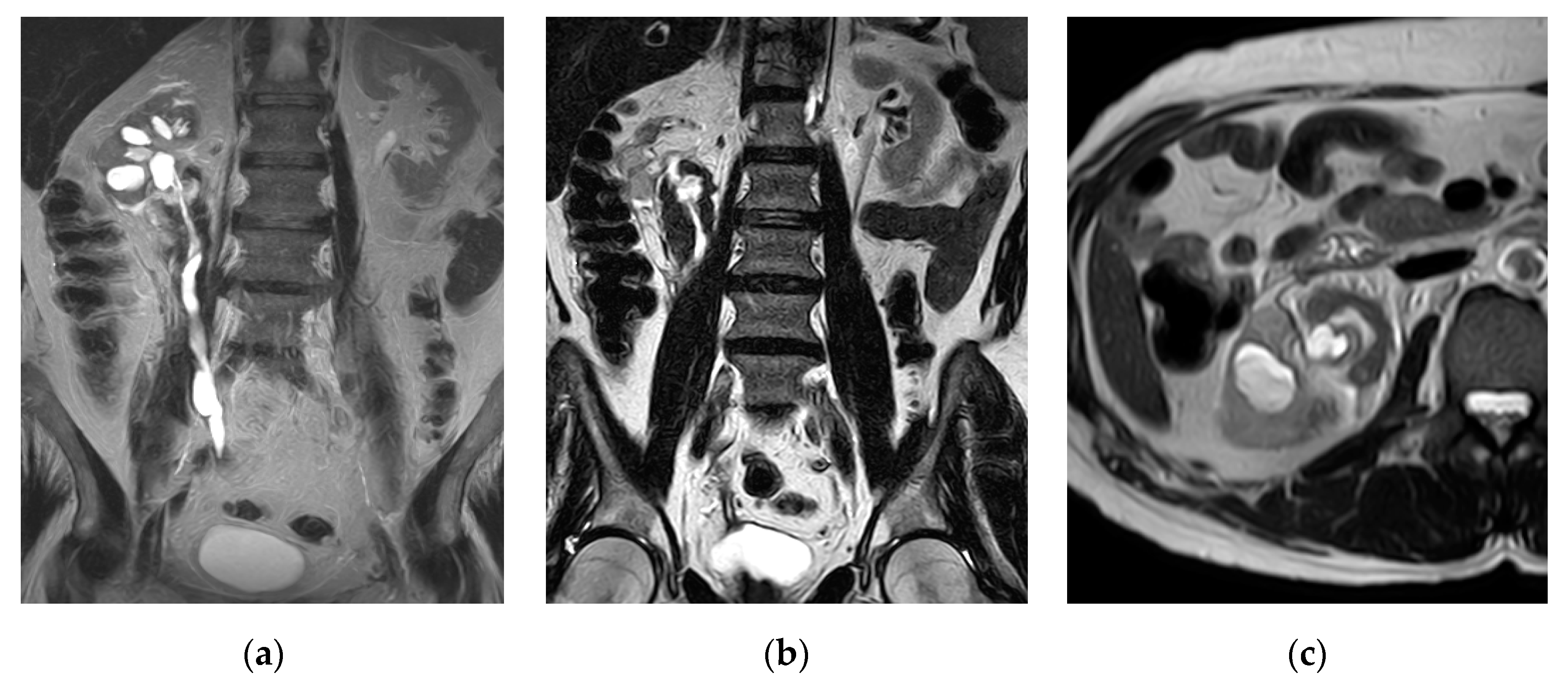
2.7. Urinary Tuberculosis
2.8. Urinary Bilharziasis
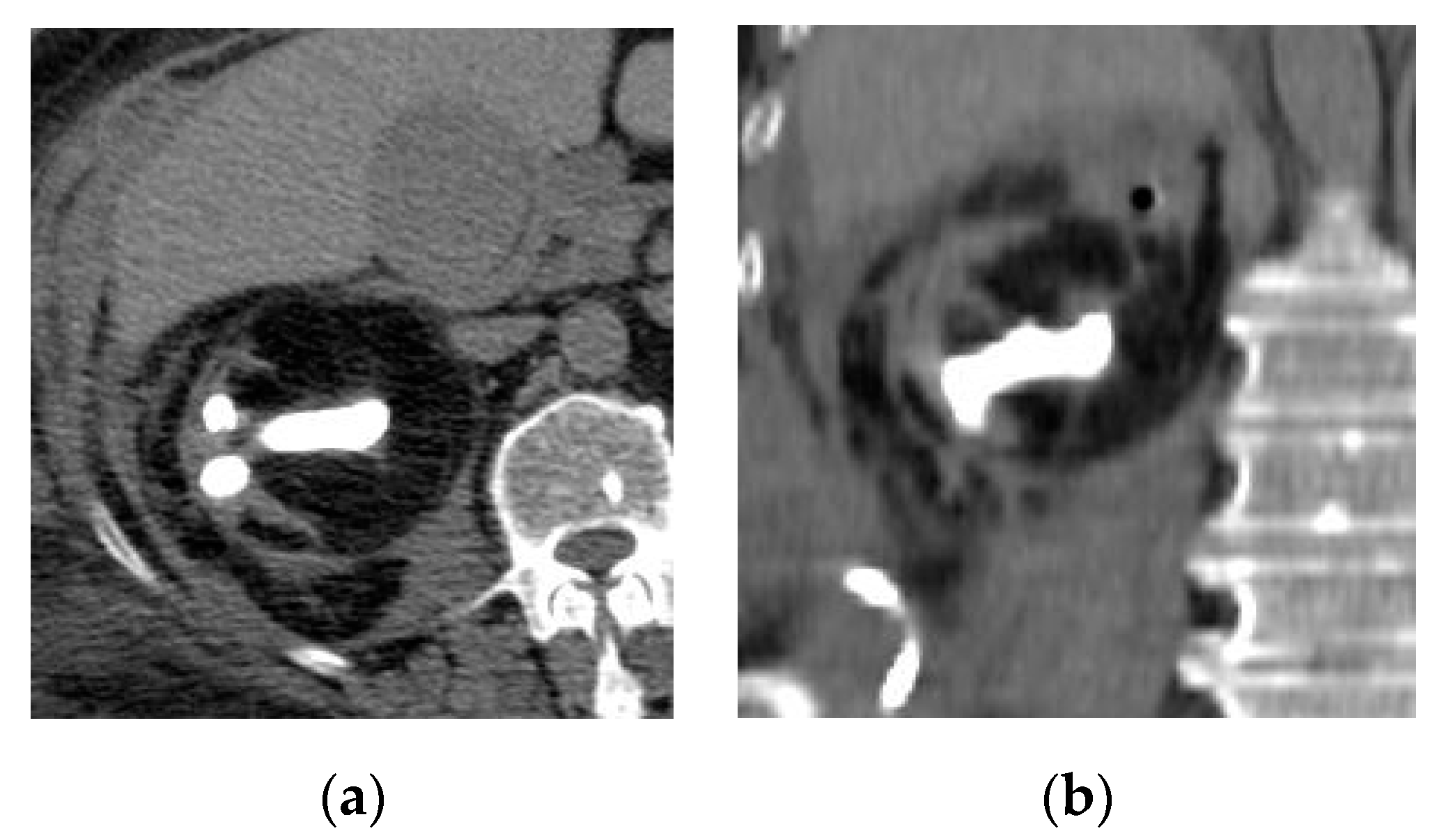
2.9. Corynebacterium Infection: Encrusted Pyelitis and Cystitis
2.10. Urinary Candidiasis:
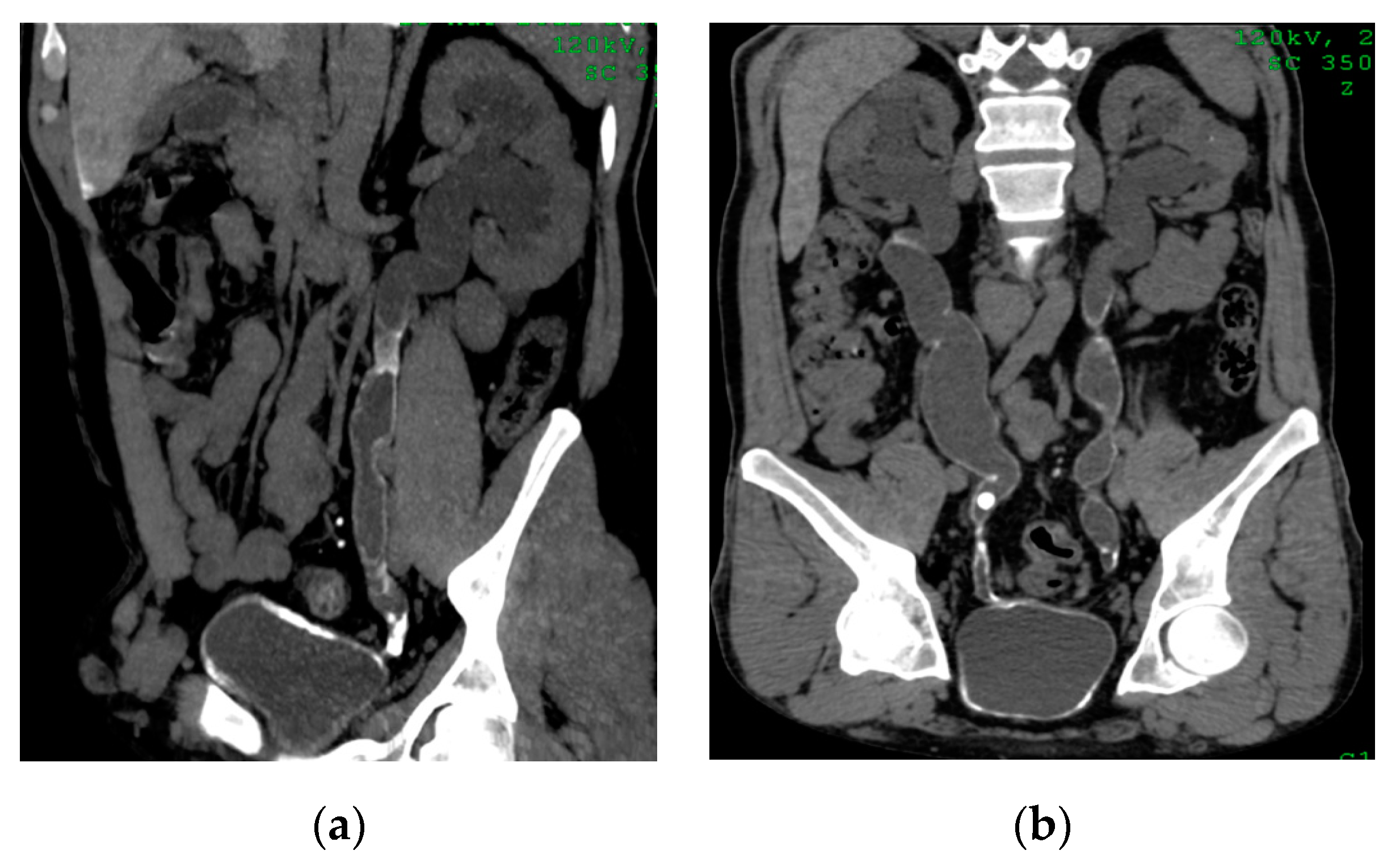
2.11. Ureteritis
2.12. Cystitis
2.13. Eosinophilic Cystitis
2.14. Cystitis and Fistula
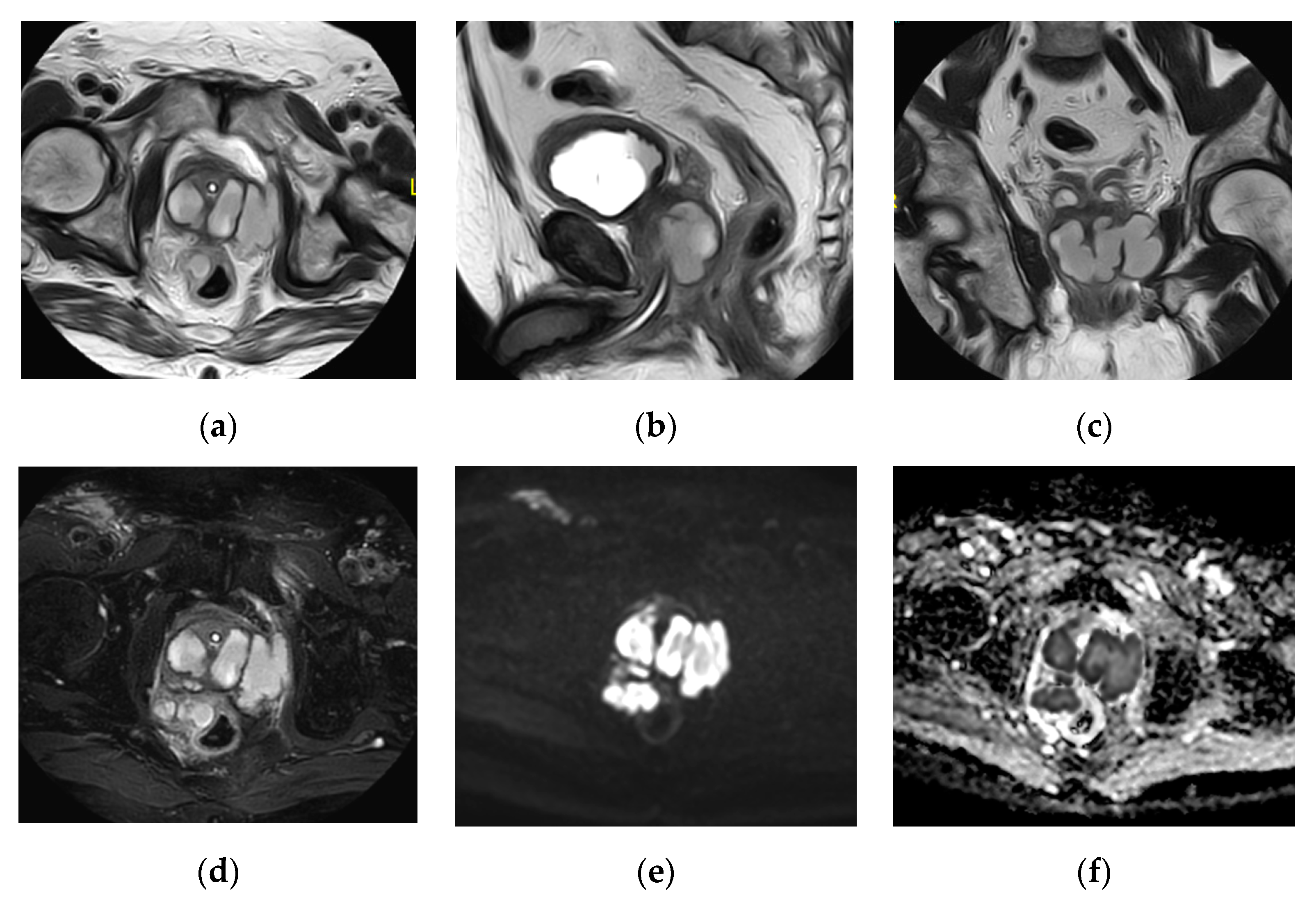
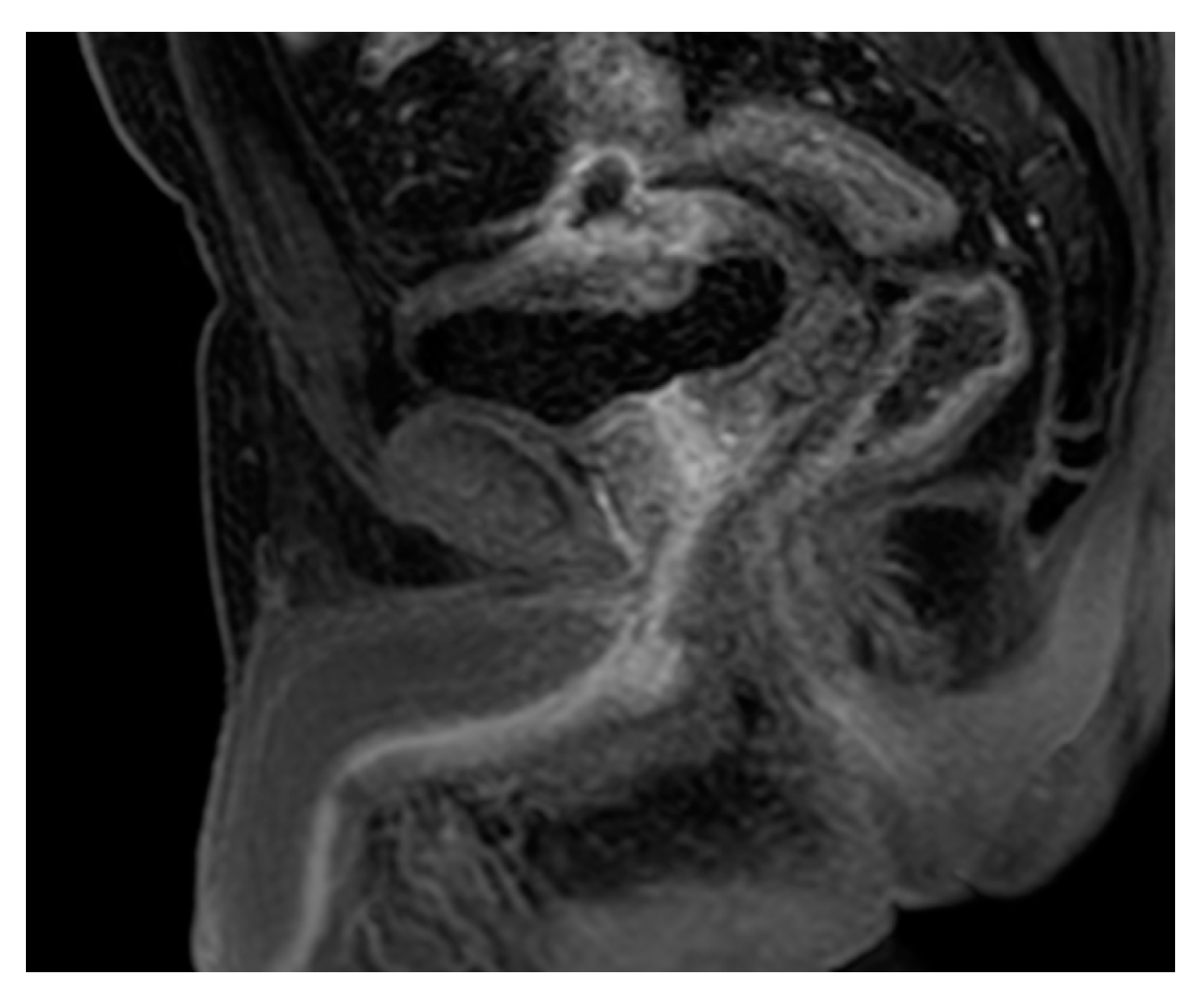
2.15. Acute Bacterial Prostatitis and Prostatic Abscess
2.16. Chronic Prostatitis
2.17. Urethritis
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nicola, R.; Menias, C.O. Urinary Obstruction, Stone Disease, and Infection. In Diseases of the Abdomen and Pelvis 2018–2021: Diagnostic Imaging—IDKD Book; Hodler, J., Kubik-Huch, R.A., von Schulthess, G.K., Eds.; Springer: Cham, Switzerland, 2018; pp. 223–228. [Google Scholar]
- O’Connor, O.J.; El-Diasty, T.; Abou-El-Ghar, M.; Maher, M.M. Common Uroradiological Referrals: Haematuria, Loin Pain, Renal Failure and Infection Haematuria, Loin Pain, Renal Failure and Infection. In Grainger and Allison’s Diagnostic Radiology, 6th ed.; Adam, A., Dixon, A., Gillard, J., Schaefer-Prokop, C., Grainger, R., Eds.; Elsevier Publishing: London, UK, 2015; pp. 832–858. [Google Scholar]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Dis.-A-Mon. DM 2003, 49, 53–70. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, L.E. The chronic indwelling catheter and urinary infection in long-term-care facility residents. Infect. Control Hosp. Epidemiol. 2001, 22, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Sarshar, M.; Behzadi, P.; Ambrosi, C.; Zagaglia, C.; Palamara, A.T.; Scribano, D. FimH and Anti-Adhesive Therapeutics: A Disarming Strategy against Uropathogens. Antibiotics 2020, 9, 397. [Google Scholar] [CrossRef]
- Scribano, D.; Sarshar, M.; Prezioso, C.; Lucarelli, M.; Angeloni, A.; Zagaglia, C.; Palamara, A.T.; Ambrosi, C. d-Mannose Treatment neither Affects Uropathogenic Escherichia coli Properties nor Induces Stable FimH Modifications. Molecules 2020, 25, 316. [Google Scholar] [CrossRef] [Green Version]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-antibiotic Antimicrobial Strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef]
- Jung, H.J.; Choi, M.H.; Pai, K.S.; Kim, H.G. Diagnostic performance of contrastenhanced ultrasound for acute pyelonephritis in children. Sci. Rep. 2020, 10, 10715. [Google Scholar] [CrossRef]
- Demertzis, J.; Menias, C.O. State of the art: Imaging of renal infections. Emerg. Radiol. 2007, 14, 13–22. [Google Scholar] [CrossRef]
- Sriman, R.; Venkatesh, K.; Mathew, C.; Pankaj, M.; Shankar, R. Validity of diffusionweighted magnetic resonance imaging in the evaluation of acute pyelonephritis in comparison with contrast-enhanced computed tomography. Pol. J. Radiol. 2020, 85, e137–e143. [Google Scholar]
- Sallami, S.; Ghariani, R.; Hichri, A.; Zrayer, O. Imaging findings of urinary tuberculosis on computerized tomography versus excretory urography: Through 46 confirmedcases. La Tunis. Med. 2014, 92, 743–747. [Google Scholar]
- Gaudiano, C.; Tadolini, M.; Busato, F.; Vanino, E.; Pucci, S.; Corcioni, B.; Golfieri, R. Multidetector CT urography in urogenital tuberculosis: Use of reformatted images for the assessment of the radiological findings. A pictorial essay. Abdom. Radiol. (N. Y.) 2017, 42, 2314–2324. [Google Scholar] [CrossRef] [PubMed]
- Das, C.J.; Ahmad, Z.; Sharma, S.; Gupta, A.K. Multimodality imaging of renal inflammatory lesions. World J. Radiol. 2014, 6, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, A.; Sandler, C.M.; Goldman, S.M. Imaging in acute renal infection. BJU Int. 2000, 86 (Suppl. 1), 70–79. [Google Scholar] [CrossRef] [Green Version]
- Udare, A.; Abreu-Gomez, J.; Krishna, S.; McInnes, M.; Siegelman, E.; Schieda, N. Imaging Manifestations of Acute and Chronic Renal Infection That Mimics Malignancy: How to Make the Diagnosis Using Computed Tomography and Magnetic Resonance Imaging. Can. Assoc. Radiol. J. J. L’assoc. Can. Des. Radiol. 2019, 70, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.D.; Schieda, N.; Shanbhogue, A.K.; Dilauro, M.; Rosenkrantz, A.B.; Siegelman, E.S. MRI Evaluation of the Urothelial Tract: Pitfalls and Solutions. AJR Am. J. Roentgenol. 2016, 207, W108–W116. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Kawamitsu, H.; Mitchell, D.G.; Ohno, Y.; Ku, Y.; Seo, Y.; Fujii, M.; Sugimura, K. ADC measurement of abdominal organs and lesions using parallel imaging technique. AJR Am. J. Roentgenol. 2006, 187, 1521–1530. [Google Scholar] [CrossRef]
- Matsuoka, A.; Minato, M.; Harada, M.; Kubo, H.; Bandou, Y.; Tangoku, A.; Nakano, K.; Nishitani, H. Comparison of 3.0-and 1.5-tesla diffusion-weighted imaging in the visibility of breast cancer. Radiat. Med. 2008, 26, 15–20. [Google Scholar] [CrossRef]
- Abreu-Gomez, J.; Udare, A.; Shanbhogue, K.P.; Schieda, N. Update on MR urography (MRU): Technique and clinical applications. Abdom. Radiol. (N. Y.) 2019, 44, 3800–3810. [Google Scholar] [CrossRef]
- Kraus, S.J. GENITOURINARY IMAGING IN CHILDREN. Pediatr. Clin. N. Am. 2001, 48, 1381–1424. [Google Scholar] [CrossRef]
- Majd, M.; Nussbaum Blask, A.R.; Markle, B.M.; Shalaby-Rana, E.; Pohl, H.G.; Park, J.S.; Chandra, R.; Rais-Bahrami, K.; Pandya, N.; Patel, K.M.; et al. Acute pyelonephritis: Comparison of diagnosis with 99mTc-DMSA, SPECT, spiral CT, MR imaging, and power Doppler US in an experimental pig model. Radiology 2001, 218, 101–108. [Google Scholar] [CrossRef]
- Johnson, J.R.; Russo, T.A. Acute Pyelonephritis in Adults. N. Engl. J. Med. 2018, 378, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Browne, R.F.; Zwirewich, C.; Torreggiani, W.C. Imaging of urinary tract infection in the adult. Eur. Radiol. 2004, 14 (Suppl. 3), E168–E183. [Google Scholar] [CrossRef]
- Patiño, A.; Martinez-Salazar, E.L.; Tran, J.; Sureshkumar, A.; Catanzano, T. Review of Imaging Findings in Urinary Tract Infections. Semin. Ultrasound Ct MR 2020, 41, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Rathod, S.B.; Kumbhar, S.S.; Nanivadekar, A.; Aman, K. Role of diffusion-weighted MRI in acute pyelonephritis: A prospective study. Acta Radiol. (Stockh. Swed. 1987) 2015, 56, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Faletti, R.; Cassinis, M.C.; Fonio, P.; Grasso, A.; Battisti, G.; Bergamasco, L.; Gandini, G. Diffusion-weighted imaging and apparent diffusion coefficient values versus contrast-enhanced MR imaging in the identification and characterization of acute pyelonephritis. Eur. Radiol. 2013, 23, 3501–3508. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, A.; Piccoli, G.B.; Priola, S.M.; Rognone, D.; Consiglio, V.; Garetto, I.; Rizzo, L.; Veltri, A. Diffusion-weighted magnetic resonance imaging: New perspectives in the diagnostic pathway of non-complicated acute pyelonephritis. Eur. Radiol. 2013, 23, 3077–3086. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, V.; Sharma, R. Emphysematous pyelonephritis (class IIIa) managed with antibiotics alone. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2015, 21, 363–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, A.; Sharma, R.; Bhalla, A.S.; Gamanagatti, S.; Seth, A. Diffusion-weighted MRI in inflammatory renal lesions: All that glitters is not RCC! Eur. Radiol. 2013, 23, 272–279. [Google Scholar] [CrossRef]
- Katabathina, V.S.; Kota, G.; Dasyam, A.K.; Shanbhogue, A.K.; Prasad, S.R. Adult renal cystic disease: A genetic, biological, and developmental primer. Radiographics 2010, 30, 1509–1523. [Google Scholar] [CrossRef] [Green Version]
- Stunell, H.; Buckley, O.; Feeney, J.; Geoghegan, T.; Browne, R.F.; Torreggiani, W.C. Imaging of acute pyelonephritis in the adult. Eur. Radiol. 2007, 17, 1820–1828. [Google Scholar] [CrossRef]
- Ifergan, J.; Pommier, R.; Brion, M.C.; Glas, L.; Rocher, L.; Bellin, M.F. Imaging in upper urinary tract infections. Diagn. Interv. Imaging 2012, 93, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirshberg, B.; Rheinboldt, M. MDCT Imaging of Acute Bladder Pathology. Curr. Probl. Diagn. Radiol. 2019, 49, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Eken, A.; Alma, E. Emphysematous cystitis: The role of CT imaging and appropriate treatment. Can. Urol. Assoc. J. J. L’assoc. Des. Urol. Can. 2013, 7, E754–E756. [Google Scholar] [CrossRef] [PubMed]
- Schönberg, S.O.; Budjan, J.; Hausmann, D. Urinary Obstruction, Stone Disease, and Infection. In Diseases of the Abdomen and Pelvis 2018–2021: Diagnostic Imaging—IDKD Book; Hodler, J., Kubik-Huch, R.A., von Schulthess, G.K., Eds.; Springer: Cham, Switzerland, 2018; pp. 247–255. [Google Scholar]
- Steinkeler, J.A.; Sun, M.R.M. Imaging of Infections of the Urinary and Male Reproductive Tracts. Semin. Roentgenol. 2017, 52, 83–89. [Google Scholar] [CrossRef]
- Bobba, R.K.; Arsura, E.L.; Sarna, P.S.; Sawh, A.K. Emphysematous cystitis: An unusual disease of the Genito-Urinary system suspected on imaging. Ann. Clin. Microbiol. Antimicrob. 2004, 3, 20. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.J.; Tseng, C.C. Emphysematous pyelonephritis: Clinicoradiological classification, management, prognosis, and pathogenesis. Arch. Intern. Med. 2000, 160, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Grayson, D.E.; Abbott, R.M.; Levy, A.D.; Sherman, P.M. Emphysematous infections of the abdomen and pelvis: A pictorial review. Radiographics 2002, 22, 543–561. [Google Scholar] [CrossRef]
- Wong-You-Cheong, J.J.; Woodward, P.J.; Manning, M.A.; Davis, C.J. From the archives of the AFIP: Inflammatory and nonneoplastic bladder masses: Radiologic-pathologic correlation. Radiographics 2006, 26, 1847–1868. [Google Scholar] [CrossRef]
- Schull, A.; Monzani, Q.; Bour, L.; Barry-Delongchamps, N.; Beuvon, F.; Legmann, P.; Cornud, F. Imaging in lower urinary tract infections. Diagn. Interv. Imaging 2012, 93, 500–508. [Google Scholar] [CrossRef] [Green Version]
- Vijayaraghavan, S.B.; Kandasamy, S.V.; Arul, M.; Prabhakar, M.; Dhinakaran, C.L.; Palanisamy, R. Spectrum of high-resolution sonographic features of urinary tuberculosis. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2004, 23, 585–594. [Google Scholar] [CrossRef]
- Muttarak, M.; ChiangMai, W.N.; Lojanapiwat, B. Tuberculosis of the genitourinary tract: Imaging features with pathological correlation. Singap. Med. J. 2005, 46, 568–574. [Google Scholar]
- Dyer, R.B.; Chen, M.Y.; Zagoria, R.J. Classic signs in uroradiology. Radiographics 2004, 24 (Suppl. 1), S247–S280. [Google Scholar] [CrossRef]
- Thoumas, D.; Darmallaicq, C.; Pfister, C.; Savoye-Collet, C.; Sibert, L.; Grise, P.; Lemaitre, L.; Benozio, M. Imaging characteristics of alkaline-encrusted cystitis and pyelitis. AJR Am. J. Roentgenol. 2002, 178, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Hertig, A.; Duvic, C.; Chretien, Y.; Jungers, P.; Grünfeld, J.P.; Rieu, P. Encrusted pyelitis of native kidneys. J. Am. Soc. Nephrol. JASN 2000, 11, 1138–1140. [Google Scholar] [PubMed]
- Orlowski, H.L.P.; McWilliams, S.; Mellnick, V.M.; Bhalla, S.; Lubner, M.G.; Pickhardt, P.J.; Menias, C.O. Imaging Spectrum of Invasive Fungal and Fungal-like Infections. Radiographics 2017, 37, 1119–1134. [Google Scholar] [CrossRef]
- Wasnik, A.P.; Elsayes, K.M.; Kaza, R.K.; Al-Hawary, M.M.; Cohan, R.H.; Francis, I.R. Multimodality imaging in ureteric and periureteric pathologic abnormalities. AJR Am. J. Roentgenol. 2011, 197, W1083–W1092. [Google Scholar] [CrossRef]
- Tonolini, M.; Ippolito, S. Cross-sectional imaging of complicated urinary infections affecting the lower tract and male genital organs. Insights Imaging 2016, 7, 689–711. [Google Scholar] [CrossRef] [Green Version]
- Teegavarapu, P.S.; Sahai, A.; Chandra, A.; Dasgupta, P.; Khan, M.S. Eosinophilic cystitis and its management. Int. J. Clin. Pract. 2005, 59, 356–360. [Google Scholar] [CrossRef]
- van den Ouden, D. Diagnosis and management of eosinophilic cystitis: A pooled analysis of 135 cases. Eur. Urol. 2000, 37, 386–394. [Google Scholar] [CrossRef]
- Itano, N.M.; Malek, R.S. Eosinophilic cystitis in adults. J. Urol. 2001, 165, 805–807. [Google Scholar] [CrossRef]
- Verhagen, P.C.; Nikkels, P.G.; de Jong, T.P. Eosinophilic cystitis. Arch. Dis. Child. 2001, 84, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Najjar, S.F.; Jamal, M.K.; Savas, J.F.; Miller, T.A. The spectrum of colovesical fistula and diagnostic paradigm. Am. J. Surg. 2004, 188, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.N.; Nyberg, L., Jr.; Nickel, J.C. NIH consensus definition and classification of prostatitis. JAMA 1999, 282, 236–237. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Huang, X.; Wang, H.; Liu, H.; Ren, F.; Zhang, Z.; Yang, Y.; Yin, H.; Huan, Y. Prostatic abscess and seminal vesicle abscess: MRI findings and quantitative analysis of apparent diffusion coefficient values. Radiol. Infect. Dis. 2015, 2, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Barozzi, L.; Valentino, M.; Menchi, I.; Pavlica, P. Clinical uroradiology: The standardisation of terminology for lower urinary tract function and dysfunction. La Radiol. Med. 2010, 115, 272–286. [Google Scholar] [CrossRef]
- Del Gaizo, A.; Silva, A.C.; Lam-Himlin, D.M.; Allen, B.C.; Leyendecker, J.; Kawashima, A. Magnetic resonance imaging of solid urethral and peri-urethral lesions. Insights Imaging 2013, 4, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Kawashima, A.; Sandler, C.M.; Wasserman, N.F.; LeRoy, A.J.; King, B.F., Jr.; Goldman, S.M. Imaging of urethral disease: A pictorial review. Radiographics 2004, 24 (Suppl. 1), S195–S216. [Google Scholar] [CrossRef]





























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infectious Conditions | Cross-Sectional Imaging Signs |
|---|---|
| Acute pyelonephritis | Wedge shaped hypo-enhancing areas or striated nephrogram pattern. Perinephric fat stranding and thickening of Gerota’s fascia. |
| Renal abscesses | Round or geographic non-enhancing central fluid collection and enhancing rim. Perinephric fat stranding and thickening of Gerota’s fascia. |
| Emphysematous UTIs | Gas in the renal parenchyma, collecting system, bladder lumen and sometimes in the perirenal and perivesical tissue. |
| Pyonephrosis | Dilated thick-walled hyperenhancing collecting system, distended with high attenuation pus-filled fluid, fluid—fluid layering at T2WI, and thinning of the renal cortex. |
| Chronic pyelonephritis | Renal scarring, cortical atrophy, calyceal clubbing, thickening and dilatation of the calyceal system and overall renal asymmetry. |
| Xanthogranulomatous Pyelonephritis | Non-functioning enlarged kidney, obstructing stone within a non-dilated renal pelvis, expansion of the calyces, and inflammatory changes in the perinephric fat. |
| Urinary tuberculosis | Calyx stem stenosis with proximal ball-shaped hydrocalyx, cavity communicating with a deformed calyx, putty kidney, ureteric strictures and shortening with beaded appearance, thick-walled contracted bladder. |
| Renal replacement lipomatosis | Total atrophy of the renal parenchyma with complete fibrofatty replacement associated with stag horn stone. Stretched calyces without hyronephrosis. |
| Urinary Bilharziasis | Contracted, fibrotic, thick calcified bladder wall with ureteric stenosis and calcifications. |
| Urinary candidiasis | Rolled appearance when it contains air bubbles between the layers of fungal colonies. If air bubbles are not present, it appears as non-enhancing solid mass. |
| Ureteritis | Diffuse mucosal urothelial thickening, often with associated periureteric fat stranding. |
| Encrusted pyelitis and cystitis | Linear hyperdense calcifications along the thickened urothelium. |
| Acute infectious cystitis | Diffuse bladder wall thickening, especially if oedematous at T2 weighted image, urothelial hyperenhancement, perivesical fat stranding. |
| Mural bladder abscess | Intramural/exophytic non-enhancing fluid collection, irregular wall, often thick peripheral enhancement, usually affecting the upper bladder aspect. |
| Prostatic abscess | Non enhancing fluid collection with peripheral or septal enhancement and non-enhancing central fluid. Possible extraprostatic extension |
| Acute urethritis | Thickened urethra and surrounding soft tissues, high T2 weighted signal intensity, corresponding intense contrast enhancement. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Ghar, M.A.; Farg, H.; Sharaf, D.E.; El-Diasty, T. CT and MRI in Urinary Tract Infections: A Spectrum of Different Imaging Findings. Medicina 2021, 57, 32. https://doi.org/10.3390/medicina57010032
El-Ghar MA, Farg H, Sharaf DE, El-Diasty T. CT and MRI in Urinary Tract Infections: A Spectrum of Different Imaging Findings. Medicina. 2021; 57(1):32. https://doi.org/10.3390/medicina57010032
Chicago/Turabian StyleEl-Ghar, Mohamed Abou, Hashim Farg, Doaa Elsayed Sharaf, and Tarek El-Diasty. 2021. "CT and MRI in Urinary Tract Infections: A Spectrum of Different Imaging Findings" Medicina 57, no. 1: 32. https://doi.org/10.3390/medicina57010032