Correlation of Biomarkers with Endoscopic Score: Ulcerative Colitis Endoscopic Index of Severity (UCEIS) in Patients with Ulcerative Colitis in Remission


 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
3.1. Baseline Characteristics of the Patients
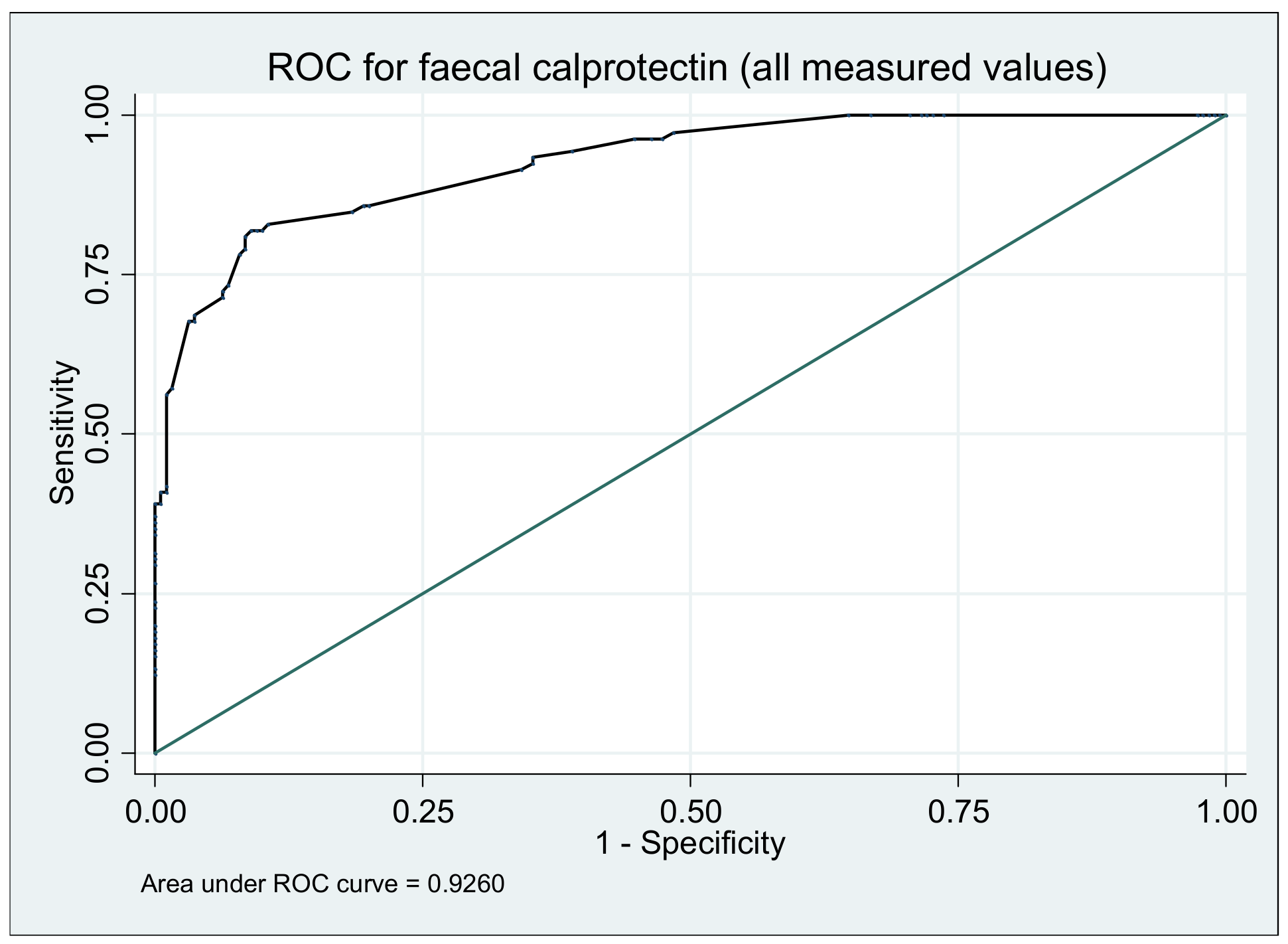
3.2. Fecal Calprotectin
3.2.1. Fecal Calprotectin Measurement
3.2.2. Relationship between Fecal Calprotectin and Endoscopic Activity
3.3. C-Reactive Protein
3.4. Haemoglobin
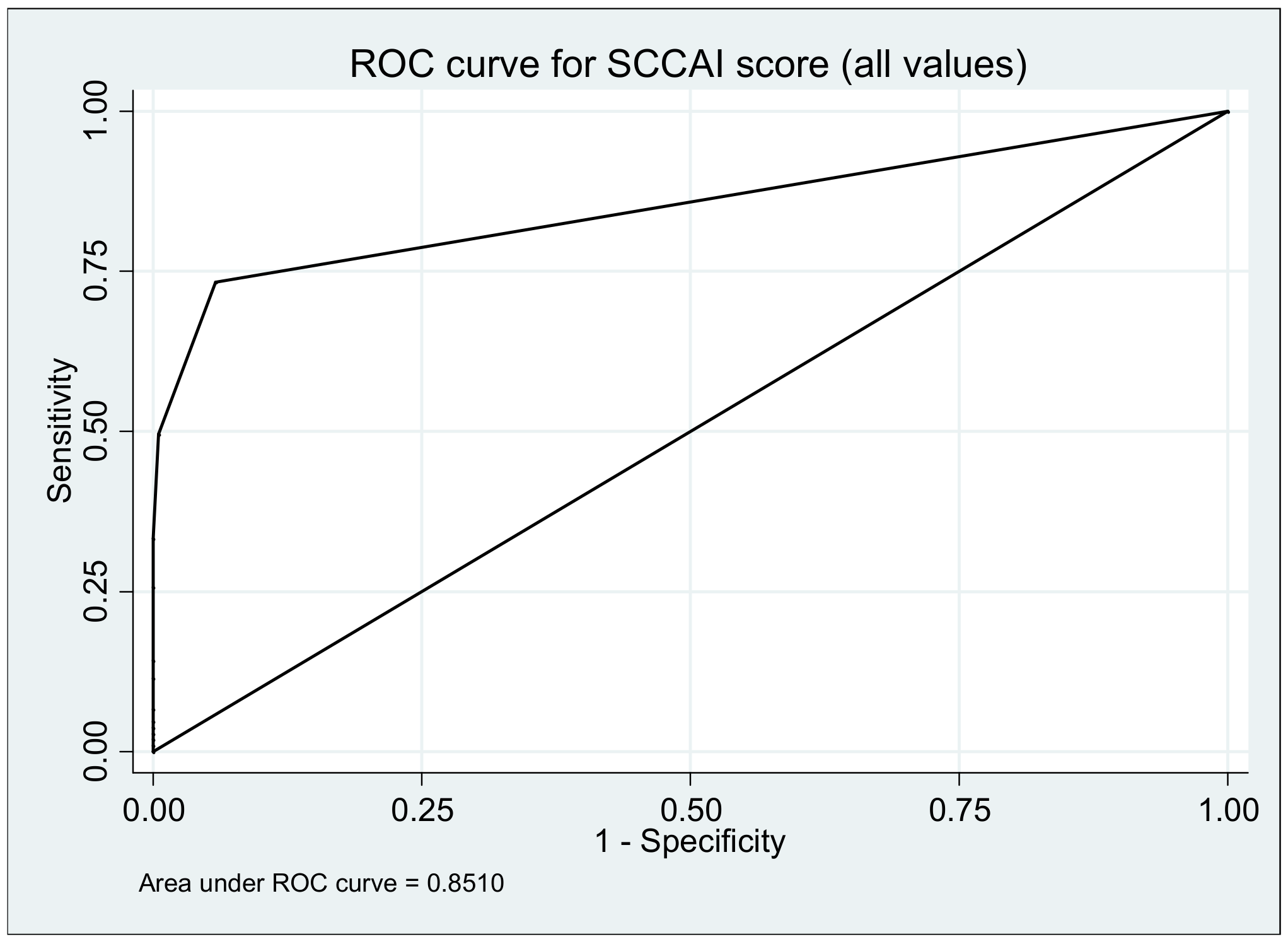
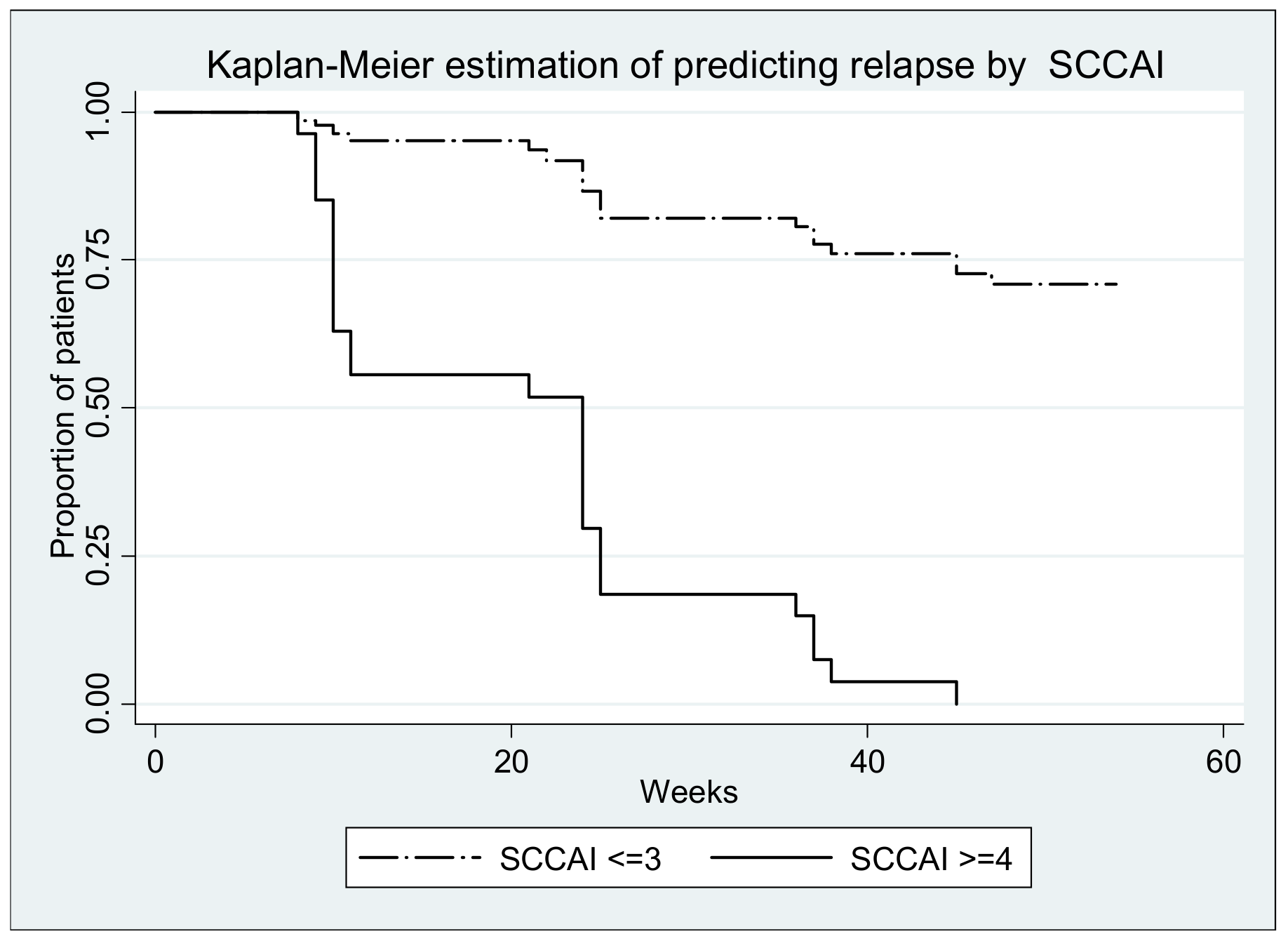
3.5. Simple Colitis Clinical Activity Index (SCCAI)
3.6. Ulcerative Colitis Endoscopic Index
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taghvaei, T.; Maleki, I.; Nagshvar, F.; Fakheri, H.; Hosseini, V.; Valizadeh, S.M.; Neishaboori, H. Fecal calprotectin and ulcerative colitis endoscopic activity index as indicators of mucosal healing in ulcerative colitis. Intern. Emerg. Med. 2015, 10, 321–328. [Google Scholar]
- Bunn, S.K.; Bisset, W.M.; Main, M.J.C.; Gray, E.S.; Olson, S.; Golden, B.E. Faecal calprotectin-Validation as a noninvasive measure of bowel inflammation in childhood inflammatory bowel disease (IBD). J. Pediatric Gastroenterol. Nutr. 2001, 33, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, F.; Akazawa, Y.; Matsushima, K.; Yamaguchi, N. Correlation of Fecal Markers with Magnifying Endoscopic Stratification in Patients with Ulcerative Colitis Who Are in Clinical Remission. Digestion 2018, 97, 82–89. [Google Scholar]
- Lee, S.; Kim, M.; Ye, B.D. Fecal calprotectin predicts complete mucosal healing and better correlates with the ulcerative colitis endoscopic index of severity than with the Mayo endoscopic subscore in patients with ulcerative colitis. BMC Gastroenterol. 2017, 17, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, W.Y.; Buisson, A.; Andersen, M.J.; Lei, D.; Pekow, J.; Cohen, R.D.; Kahn, S.A.; Pereira, B.; Rubin, D.T. Fecal Calprotectin in Assessing Endoscopic and Histological Remission in Patients with Ulcerative Colitis. Dig. Dis. Sci. 2018, 63, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Theede, K.; Osterman, F.I. Level of Fecal Calprotectin Correlates With Endoscopic and Histologic Inflammation and Identifies Patients With Mucosal Healing in Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2015, 13, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Xie, T.; Zhang, T.; Ding, C.; Dai, X.; Li, Y.; Guo, Z.; Wei, Y.; Gong, J.; Zhu, W.; Li, J. Ulcerative Colitis Endoscopic Index of Severity (UCEIS) versus Mayo Endoscopic Score (MES) in guiding the need for colectomy in patients with acute severe colitis. Gastroenterol. Rep. 2018, 6, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Ikeya, K.; Hanai, H.; Watanabe, F. The Ulcerative Colitis Endoscopic Index of Severity More Accurately Re ects Clinical Outcomes and Long-term Prognosis than the Mayo Endoscopic Score. J. Crohns Colitis 2016, 10, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Bermejo, F.; Pérez-Calle, J.-L.; Taxonera, C.; Vera, I.; McNicholl, A.G.; Algaba, A.; López, P.; López-Palacios, N.; Calvo, M. Fecal Calprotectin and Lactoferrin for the Prediction of inflammatory bowel disease relapse. Inflamm. Bowel Dis. 2009, 15, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.; Day, A.S.; Turner, D.; Leach, S.; Mack, D.R.; Uusoue, K.; McLernon, R.; Hyams, J.; Leleiko, N.; Walters, T.D. Faecal calprotectin, lactoferrin, M2-pyruvate kinase and S100A12 in severe ulcerative colitis: A prospective multicentre comparison of predicting outcomes and monitoring response. Gut 2010, 59, 1207–1212. [Google Scholar]
- Takashima, S.; Kato, J.; Hiraoka, S.; Nakarai, A.; Takei, D. Evaluation of Mucosal Healing in Ulcerative Colitis by Fecal Calprotectin Vs Fecal Immunochemical Test. Am. J. Gastroenterol. 2015, 110, 873–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, N.A.; Jones, G.; Plevris, N.; Patenden, R.; Arnott, I.D.; Lees, C.W. Association Between Level of Fecal Calprotectin and Progression of Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 2269–2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, N.; Cummins, E.; Royle, P.; Kandala, N.-B.; Shyangdan, D.; Arasaradnam, R.; Clar, C.; Johnston, R. Faecal calprotectin testing for differentiating amongst inflammatory and non-inflammatory bowel diseases: Systematic review and economic evaluation. Health Technol. Assess. 2013, 17, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Bennebroek, F.; Nieuwkerk, P.T.; Stokkers, P.C.F.; Ponsioen, C.Y.; Bockting, C.L.H.; Sanderman, R.; Sprangers, M.A.G. The Patient Simple Clinical Colitis Activity Index (P-SCCAI) can detect ulcerative colitis (UC) disease activity in remission: A comparison of the P-SCCAI with clinician-based SCCAI and biological markers. J. Crohn’s Colitis 2013, 7, 890–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walmsley, R.S.; Ayres, R.C.S.; Pounder, R.E.; Allan, R.N. A simple clinical colitis activity index. Gut 1998, 43, 29–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meenakshi, B.; Brensinger, C.M.; Tomov, V.T.; Hoang, T.B.; Sokach, C.E.; Siegel, C.A.; Lewis, J.D. An Optimized Patient-reported Ulcerative Colitis Disease Activity Measure Derived from the Mayo Score and the Simple Clinical Colitis Activity Index. Inflamm. Bowel Dis. 2014, 20, 1070–1078. [Google Scholar] [CrossRef] [Green Version]
- Walmsley, R.; Roy, O. Simple Clinical Colitis Activity Index (SCCAI) and future patient-centered telemedical care of Ulcerative Colitis patients. Med. Res. Arch. 2017, 5, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Walsha, A.J.; Ghoshb, A.; Braing, A.O.; Buchel, O.; Burger, D.; Thomas, S.; White, L.; Collins, G.S.; Keshav, S.; Travis, S.P.L. Comparing disease activity indices in ulcerative colitis. JCC 2014, 8, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Walsh, A.J.; Bryant, R.V.; Travis, S.P.L. Current best practice for disease activity assessment in IBD. Nat. Publ. Gr. 2016, 13, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Mumolo, M.G.; Ceccarelli, L.; Bellini, M.; Romano, M.R.; Sterpi, C.; Ricchiuti, A.; Marchi, S.; Bottai, M. Calprotectin is a stronger predictive marker of relapse in ulcerative colitis than in Crohn’s disease. Gut 2005, 54, 364–368. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years, Median, Range) | 47 (21–77) |
|---|---|
| Gender (% male) | 55.9 |
| Smoking (% smokers) | 11.9 |
| Montreal classification of extent of UC (%) | |
| E1 | 18.6 |
| E2 | 40.7 |
| E3 | 40.7 |
| Concomitant medication at baseline % | |
| 5-ASA (Mesalazine) | 98.3 |
| Azathioprine | 44.1 |
| Corticosteroids | 10.2 |
| Infliximab | 32.2 |
| Adalimumab | 17.0 |
| Time of remission of disease until inclusion in the study (months; median range) | 30 (4–84) |
| Parameters | OR (95% CI) | p (Z Test) | ROC Area (95% CI) | p (Chi2) |
|---|---|---|---|---|
| FC | 1.05 (1.03–1.06) | ≤0.0001 | 0.93 (0.90–0.96) | 0.0005 |
| CRP | 1.74 (1.51–2.00) | ≤0.0001 | 0.87 (0.84–1.00) | 0.0047 |
| HB | 2.30 (1.81–2.93) | ≤0.0001 | 0.75 (0.69–0.82) | ≤0.0001 |
| SCCAI score | 14.04 (6.88–28.66) | ≤0.00001 | 0.85 (0.81–0.90) | ≤0.0001 |
| UCEIS score | 34.50 (12.06–98.74) | ≤0.00001 | 0.89 (0.84–0.94) | 0.11 |
| Parameters | HR (95% CI) | p (Z Test) |
|---|---|---|
| Gender (Women vs. Male) | 0.81 (0.54–1.19) | 0.281 |
| Age (over 60 yrs vs. under 60 yrs) | 1.01 (1.00–1.02) | 0.045 |
| Extent of ulcerative colitis (E2-E3 vs. E1) | 2.31 (1.69–3.14) | ≤0.0001 |
| Smoking (Smoker& ex-smoker vs. Non-smoker) | 1.10 (0.94–1.28) | 0.224 |
| Fecal Calprotectin (0–12 months) | 1.001 (1.0010–1.0015) | ≤0.0001 |
| C reactive protein (0–12 months) | 1.10 (1.08–1.12) | ≤0.0001 |
| Hb concentration (0–12 months) | 1.39 (1.32–1.47) | ≤0.0001 |
| Simple Clinical Colitis Activity Index (SCCAI) over time (0–12 months | 1.39 (1.32–1.47) | ≤0.0001 |
| Ulcerative Colitis Endoscopic Index (UCEIS) over time (0–12 months) | 1.70 (1.53–1.90) | ≤0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, C.S.; Filip, P.V.; Diaconu, S.L.; Matei, C.; Furtunescu, F. Correlation of Biomarkers with Endoscopic Score: Ulcerative Colitis Endoscopic Index of Severity (UCEIS) in Patients with Ulcerative Colitis in Remission. Medicina 2021, 57, 31. https://doi.org/10.3390/medicina57010031
Pop CS, Filip PV, Diaconu SL, Matei C, Furtunescu F. Correlation of Biomarkers with Endoscopic Score: Ulcerative Colitis Endoscopic Index of Severity (UCEIS) in Patients with Ulcerative Colitis in Remission. Medicina. 2021; 57(1):31. https://doi.org/10.3390/medicina57010031
Chicago/Turabian StylePop, Corina Silvia, Petruta Violeta Filip, Sorina Laura Diaconu, Clara Matei, and Florentina Furtunescu. 2021. "Correlation of Biomarkers with Endoscopic Score: Ulcerative Colitis Endoscopic Index of Severity (UCEIS) in Patients with Ulcerative Colitis in Remission" Medicina 57, no. 1: 31. https://doi.org/10.3390/medicina57010031