Policies and Challenges on the Distribution of Specialists and Subspecialists in Rural Areas of Iran


 ,
,
Abstract
:1. Introduction
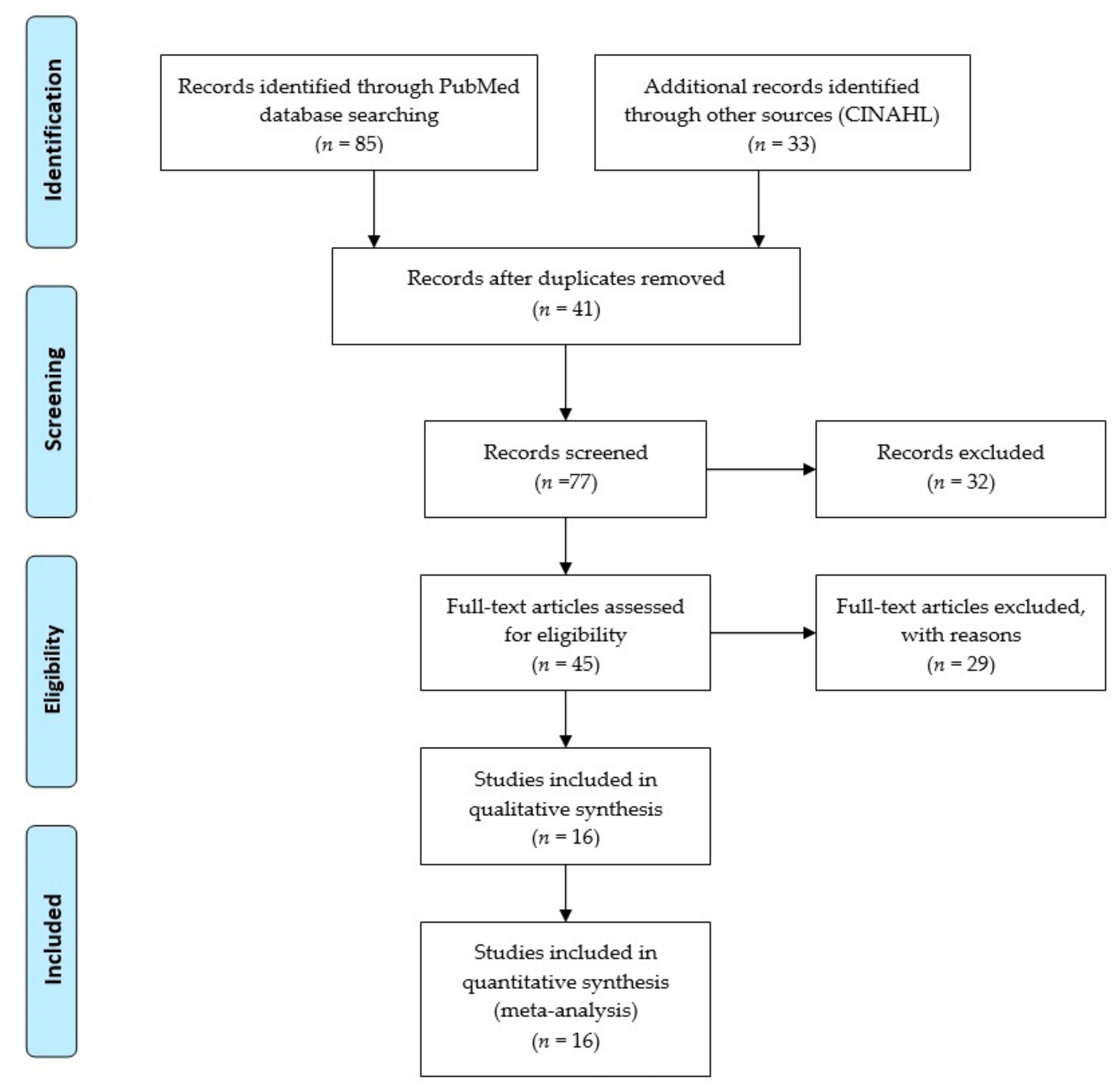
2. Methods
2.1. Data Sources and Study Selection
2.2. Quality Assessment
2.3. Exclusion Criteria
3. Results
3.1. Policies and Specialist Distribution for Pediatric Assistance
3.1.1. Problems in Specialist Consultation
3.1.2. Expenditure and Medical Policies to Supply Medication
3.1.3. Factors that Influence the Geographic Distribution of Iran Physicians
3.2. Health Status Degradation in Different Areas of Iran
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kwan, M.P.; Murray, A.T.; O’Kelly, M.E.; Tiefelsdorf, M. Recent advances in accessibility research: Representation, methodology and applications. J. Geogr. Syst. 2003, 5, 129–138. [Google Scholar] [CrossRef]
- Curtis, E.M.; van der Velde, R.; Moon, R.J.; van den Bergh, J.P.; Geusens, P.; de Vries, F.; van Staa, T.P.; Cooper, C.; Harvey, N.C. Epidemiology of fractures in the United Kingdom 1988–2012: Variation with age, sex, geography, ethnicity and socioeconomic status. Bone 2016, 87, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblatt, R.A.; Andrilla, C.H.A.; Catlin, M.; Larson, E.H. Geographic and specialty distribution of US physicians trained to treat opioid use disorder. Ann. Fam. Med. 2015, 13, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Belaid, L.; Dagenais, C.; Moha, M.; Ridde, V. Understanding the factors affecting the attraction and retention of health professionals in rural and remote areas: A mixed-method study in Niger. Hum. Resour. Health 2017, 15, 60. [Google Scholar] [CrossRef]
- Chen, L.C. Striking the right balance: Health workforce retention in remote and rural areas. Bull. World Health Organ. 2010, 88, 323. [Google Scholar] [CrossRef]
- Dieleman, M.; Harnmeijer, J.W. Improving Health Worker Performance: In Search of Promising Practices; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Okuji, M.M.; Okuji, D. Patient Protection and Affordable Care Act. In Dental Benefits and Practice Management: A Guide for Successful Practices; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Spooner, S.A. Telepediatrics: Telemedicine and child health. J. Telemed. Telecare 2005, 11, 269. [Google Scholar] [CrossRef]
- Basco, W.T.; Rimsza, M.E. Pediatrician workforce policy statement. Pediatrics 2013, 132, 390–397. [Google Scholar]
- LeBaron, S.W.M.; Schultz, S.H. Family medicine in Iran: The birth of a new specialty. Fam. Med. 2005, 37, 502. [Google Scholar]
- Golboni, F.; Nadrian, H.; Najafi, S.; Shirzadi, S.; Mahmoodi, H. Urban–rural differences in health literacy and its determinants in Iran: A community-based study. Aust. J. Rural Health 2018, 26, 98–105. [Google Scholar] [CrossRef]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- PRISMA. PRISMA—Transparent Reporting of Systematic Reviews and Meta-Analyses; PRISMA: Berlin, Germany, 2015. [Google Scholar]
- Doaee, S.H.; Olyaeemanesh, A.; Emami, S.H.; Mobinizadeh, M.; Abooee, P.; Nejati, M.; Zolani, G.S. Development and implementation of health technology assessment: A policy study. Iran. J. Public Health 2013, 42 (Suppl. 1), 50. [Google Scholar]
- Matin, B.K.; Azami, S.R.; Mahmoudi, S.; Rezaei, S.; Shaahmadi, F.; Karyani, A.K. Determinants of pharmaceutical expenditures of urban households: A time series study in Kermanshah province (Iran). Electron. Phys. 2015, 7, 1470. [Google Scholar] [CrossRef] [PubMed]
- Bayati, M.; Feyzabadi, V.Y.; Rashidian, A. Geographical disparities in the health of Iranian women: Health outcomes, behaviors, and health-care access indicators. Int. J. Prev. Med. 2017, 8, 11. [Google Scholar] [PubMed]
- Haghdoost, A.; Abas, K.; Ashrafi, A.; Sadeghirad, B.; Shafieian, H.; Ghasemi, S.H. Geographical distribution of different groups of the medical community in the country and the examination of provincial inequalities. J. Med. Counc. Islam. Repub. Iran 2010. [Google Scholar]
- Parsaeian, M.; Farzadfar, F.; Zeraati, H.; Mahmoudi, M.; Rahimighazikalayeh, G.; Navidi, I.; Nikan, K.S.R.; Mohammad, K.; Jafari, K.M. Application of spatio-temporal model to estimate burden of diseases, injuries and risk factors in Iran 1990–2013. Arch. Iran. Med. 2014, 17, 28–32. [Google Scholar]
- Nourijelyani, K.; Aghamohammadi, A.; Sadaghiani, M.S.; Behniafard, N.; Abolhassani, H.; Pourjabar, S.; Rezvanizadeh, A.; Khadamy, J.; Imanzaeh, A.; Sedaghat, M.; et al. Physicians awareness on primary immunodeficiency disorders in Iran. Iran. J. Allergy Asthma Immunol. 2012, 11, 57–64. [Google Scholar]
- Aeenparast, A.; Farzadi, F.; Maftoon, F. Waiting time for specialist consultation in Tehran. Arch. Iran. Med. 2012, 15, 756–758. [Google Scholar]
- Rashidbeygi, M.; Sayehmiri, K. Knowledge and attitudes of physicians towards evidence based medicine in Ilam, Iran. Iran. Red Crescent Med. J. 2013, 15, 798. [Google Scholar] [CrossRef] [Green Version]
- Keley, E.T.; Ravaghi, H.; Salehi, M.; Nasiripour, A.A.; Abdi, Z.; Meshkini, A. Relationship between personal characteristics of specialist physicians and choice of practice location in Iran. Rural Remote Health 2016, 16, 3412. [Google Scholar]
- Ravaghi, H.; Taati, E.; Abdi, Z.; Meshkini, A.; Sarvarizadeh, S. Factors influencing the geographic distribution of physicians in Iran: A qualitative study. Rural Remote Health 2015, 15, 2967. [Google Scholar]
- Ghaderi, M.; Taghvaei, M.; Shafaghi, S. An analysis of management of regional development in Iran. Int. Rev. 2017, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Rasoolimanesh, S.M.; Jaafar, M.; Badarulzaman, N. Urban planning and management system in iran: A review and assessment. Middle East J. Sci. Res. 2013, 18, 220–229. [Google Scholar]
- Sefiddashti, S.E.; Ghazanfari, S. Ranking Islamic Republic of Iran’s Development Vision Countries in Term of Access to Healthcare Indicators. J. Health Adm. 2015, 17, 58–71. [Google Scholar]
- Abolhallaje, M.; Mousavi, S.M.; Anjomshoa, M.; Nasiri, A.B.; Seyedin, H.; Sadeghifar, J.; Aryankhesal, A.; Vasokolaei, G.R.; Nasiri, M.B. Assessing health inequalities in Iran: A focus on the distribution of health care facilities. Glob. J. Health Sci. 2014, 6, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baigi, V.; Nedjat, S.; Hosseinpoor, A.R.; Sartipi, M.; Salimi, Y.; Fotouhi, A. Socioeconomic inequality in health domains in Tehran: A population-based cross-sectional study. BMJ Open 2018, 8, 1–6. [Google Scholar] [CrossRef]
- Lotfi, F.; Bayati, M.; Yusefi, A.R.; Ghaderi, S.; Barati, O. Inequality in distribution of health care resources in Iran: Human resources, health centers and hospital beds. Shiraz E Med. J. 2018, 19, e63700. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, S.; Ghazanfari, S.; Kazemi, Z.; Karyani, A.K. Access to healthcare facilities: Case study of Kermanshah province. J. Kermanshah Univ. Med. Sci. 2014, 18, 416–425. [Google Scholar]
- Laverack, G. The challenge of behaviour change and health promotion. Challenges 2017, 8, 25. [Google Scholar] [CrossRef] [Green Version]
- Ciccia, A.H.; Roizen, N.; Garvey, M.; Bielefeld, R.; Short, E.J. Identification of neurodevelopmental disabilities in underserved children using telehealth (INvesT): Clinical trial study design. Contemp. Clin. Trials 2015, 45, 226–232. [Google Scholar] [CrossRef]
- Simacek, J.; Dimian, A.F.; McComas, J.J. Communication intervention for young children with severe neurodevelopmental disabilities via telehealth. J. Autism Dev. Disord. 2017, 47, 744–767. [Google Scholar] [CrossRef]
- Kim, J.A. Telehealth in the developing world. Healthc. Inform. Res. 2010, 16, 140–141. [Google Scholar] [CrossRef]
- Eng, T.R. The e-Health Landscape—A Terrain Map of Emerging Information and Communication Technologies in Health and Health Care; The Robert Wood Johnson Foundation: Princet, NJ, USA, 2004. [Google Scholar]
- Singh, M.; Das, R.R. Utility of telemedicine for children in India. Indian J. Pediatr. 2010, 77, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Karp, W.B.; Grigsby, R.K.; McSwiggan-Hardin, M.; Pursley-Crotteau, S.; Adams, L.N.; Bell, W.; Stachura, M.E.; Kanto, W.P. Use of telemedicine for children with special health care needs. Pediatrics 2000, 105, 843–847. [Google Scholar] [CrossRef] [PubMed]
- Mars, M. Telemedicine and advances in urban and rural healthcare delivery in Africa. Prog. Cardiovasc. Dis. 2013, 56, 326–335. [Google Scholar] [CrossRef]
- Myers, K.; Stoep, A.V.; Zhou, C.; McCarty, C.A.; Katon, W. Effectiveness of a telehealth service delivery model for treating attention-deficit/hyperactivity disorder: A community-based randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 263–274. [Google Scholar] [CrossRef] [Green Version]
- Marcin, J.P.; Ellis, J.; Mawis, R.; Nagrampa, E.; Nesbitt, T.S.; Dimand, R.J. Using telemedicine to provide pediatric subspecialty care to children with special health care needs in an underserved rural community. Pediatrics 2004, 113, 1–6. [Google Scholar] [CrossRef]
- Lobe, T.E. Telemedicine and the future of healthcare for our children. Pediatrics 2004, 113, 130. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year | Study Type | Objectives | Policies | Challenges |
|---|---|---|---|---|---|
| Doaee, S.H. [14] | 2013 | Policy study | Health technology assessments (HTAs) | Generating localization for fundamental HTAs in the Iranian health system. In medical universities, for M.sc, Ph.D. degrees, design policy in the HTA subject | There is no clear government policy to move forward with HTA objectives in Iran |
| Karami Matin [15] | 2015 | Analytical descriptive study | Finding the key factors that affect the expenditures of pharmaceutical products by municipal houses | For poor people, designing and developing primary and supplemental insurance coverage can be a suitable solution to avoid barriers of drug availability for patients with chronic diseases | Health policymakers in Iran are not ready to take steps to ensure physical and financial access to drugs |
| Bayati, M. [16] | 2017 | Original study | Framework for women’s health determinants | At a provincial level, determinants like health behavior, health knowledge, and lifestyle availability were imbalanced in women’s health at a provincial level | Too many provincial disparities of Iranian women were found. Health policymakers should address these disparities in determinants |
| Haghdoost, A. [17] | 2010 | Survey | Geographical distribution of specialists and medical experts and the inequalities in Iran provinces | The country is more specialized in different medical subgroups, and other provinces still require specialist medical personnel | Specialist group geographical distribution is unbalanced across the country, and there seems to be a significant shortage in deprived areas. |
| Parsaeian, M. [18] | 2014 | Original study | Provide remedies to overcome the burden of disease and geographical inequalities of Iran | Relating various available data sources and generating reliable and precise evidence for Iranian burden of diseases and its risk factors | Not identified |
| Nourijelyani, K. [19] | 2012 | Experimental | Assessment of the Iranian general practitioners (GPs) knowledge and pediatricians about primary immunodeficiency diseases (PIDs) | Reconsidering educating schedules and training classes is necessary to improve physician’s knowledge about PIDs. | There is an impressive absence of awareness of PIDs among doctors |
| Aeenparast, A. [20] | 2012 | Cross-sectional | Determine the waiting time in doctor workplaces in Tehran, Iran | The normal waiting time in this research was less than seven days for specialists and just about seven days for subspecialists | The Iranian health system has not set up a complete referral framework, and with this circumstance, waiting times may strongly affect patient health |
| Rashidbeygi, M. [21] | 2013 | Experimental | Finding the knowledge of physicians towards evidence-based medicine (EBM) | Information and frame of mind of young doctors were progressively founded on EBM and contrasted with old doctors | A huge contrast in the information mean score of doctors demonstrates that EBM is still new in Iran |
| Keley, E. [22] | 2016 | Cross-sectional | The connection between doctors’ attributes and their desire to practice in rural areas was analyzed | It appears that expanding the enrollment of specialists from a rural background in residency projects may overcome the issue of uneven dissemination of specialist physicians in Iran | Not identified |
| Ravaghi, H. [23] | 2015 | Qualitative | Investigate the factors affecting the distribution of expert doctors in Iran | The territorial distribution and supply of specialists of Iran have been improved in light of the executed policies in recent years | Students with a rural background and steady measures for doctors working in deprived regions were suggested |
| First Author | Year | Study Type | Objectives | Policies | Challenges |
|---|---|---|---|---|---|
| Ghaderi, M. [24] | 2017 | Survey | Impact factors on the management of regional development in Iran | Produce solutions to reduce regional imbalances | Policies proposed in this study increase imbalances and threaten disorder for all of Iran |
| Rasoolimanesh, S. [25] | 2013 | Qualitative | Assessment of the existing urban planning system of Iran | Findings cause poor urban plan management | Poor implementation |
| S. Emamgolipor Sefiddashti [26] | 2017 | Cross-sectional | Ranking the countries based on access to health sector indicators | Produce a report on the need for specialists in Iranian provinces | Healthcare expenditure not yet successful in Iran |
| Abolhallaje, M. [27] | 2014 | Cross-sectional | In terms of access to health care, ranking the towns of the provinces was done | Policymakers should come forward to bridge the gap between the distribution of health services in Markazi | The large gap for healthcare provision in towns of Markazi province, Iran |
| Baigi, V. [28] | 2018 | Survey | Assessment of socioeconomic inequality in various health domains and self-rated health (SRH) | Socioeconomic inequalities were found in various health domains in favor of improved socioeconomic status groups | Not identified |
| Lotfi, F. [29] | 2018 | Retrospective | Examining the equality of resource distribution between Iran provinces in 2014 | Proposing suggestions to policymakers to focus more on resource distribution-based health requirements of patients | Not identified |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirmoeini, S.M.; Marashi Shooshtari, S.S.; Battineni, G.; Amenta, F.; Tayebati, S.K. Policies and Challenges on the Distribution of Specialists and Subspecialists in Rural Areas of Iran. Medicina 2019, 55, 783. https://doi.org/10.3390/medicina55120783
Mirmoeini SM, Marashi Shooshtari SS, Battineni G, Amenta F, Tayebati SK. Policies and Challenges on the Distribution of Specialists and Subspecialists in Rural Areas of Iran. Medicina. 2019; 55(12):783. https://doi.org/10.3390/medicina55120783
Chicago/Turabian StyleMirmoeini, Seyed Masoud, Seyed Sina Marashi Shooshtari, Gopi Battineni, Francesco Amenta, and Seyed Khosrow Tayebati. 2019. "Policies and Challenges on the Distribution of Specialists and Subspecialists in Rural Areas of Iran" Medicina 55, no. 12: 783. https://doi.org/10.3390/medicina55120783