Cytomegalovirus Seropositivity and Suicidal Behavior: A Mini-Review

 , ,
, ,
Abstract
:1. Introduction
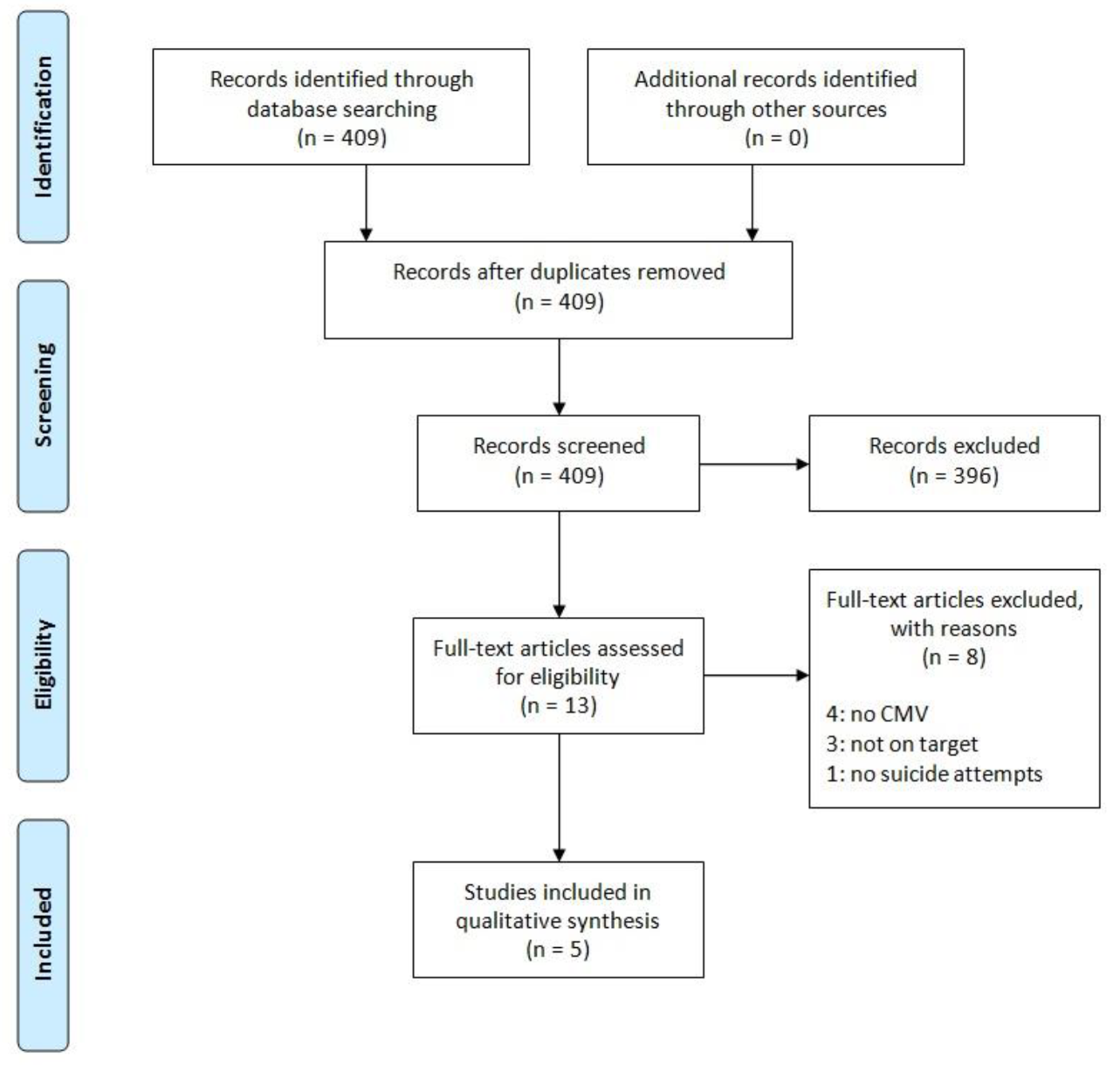
2. Materials and Methods
3. Results
3.1. Studies in Healthy Subjects
3.2. Studies in Psychiatric Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Niculescu, A.B.; Le-Niculescu, H.; Levey, D.F.; Phalen, P.L.; Dainton, H.L.; Roseberry, K.; Niculescu, E.M.; Niezer, J.O.; Williams, A.; Graham, D.L.; et al. Precision medicine for suicidality: From universality to subtypes and personalization. Mol. Psychiatry 2017, 22, 1250. [Google Scholar] [CrossRef] [PubMed]
- Belsher, B.E.; Smolenski, D.J.; Pruitt, L.D.; Bush, N.E.; Beech, E.H.; Workman, D.E.; Morgan, R.L.; Evatt, D.P.; Tucker, J.; Skopp, N.A. Prediction Models for Suicide Attempts and Deaths: A Systematic Review and Simulation. JAMA Psychiatry 2019, 76, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Oquendo, M.A.; Sullivan, G.M.; Sudol, K.; Baca-Garcia, E.; Stanley, B.H.; Sublette, M.E.; Mann, J.J. Toward a biosignature for suicide. Am. J. Psychiatry 2014, 171, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Leweke, F.M.; Gerth, C.W.; Koethe, D.; Klosterkötter, J.; Ruslanova, I.; Krivogorsky, B.; Torrey, E.F.; Yolken, R.H. Antibodies to infectious agents in individuals with recent onset schizophrenia. Eur. Arch. Psychiatr. Clin. Neurosci. 2004, 254, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Mohagheghi, M.; Eftekharian, M.M.; Taheri, M.; Alikhani, M.Y. Determining the IgM and IgG antibodies titer against HSV1, HSV2 and CMV in the serum of schizophrenia patients. Hum. Antibodies 2018, 26, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Tedla, Y.; Shibre, T.; Ali, O.; Tadele, G.; Woldeamanuel, Y.; Asrat, D.; Aseffa, A.; Mihret, W.; Abebe, M.; Alem, A.; et al. Serum antibodies to Toxoplasma gondii and Herpesvidae family viruses in individuals with schizophrenia and bipolar disorder: A case-control study. Ethiop. Med. J. 2011, 49, 211–220. [Google Scholar]
- Tanaka, T.; Matsuda, T.; Hayes, L.N.; Yang, S.; Rodriguez, K.; Severance, E.G.; Yolken, R.H.; Sawa, A.; Eaton, W.W. Infection and inflammation in schizophrenia and bipolar disorder. Neurosci. Res. 2017, 115, 59–63. [Google Scholar] [CrossRef]
- Prossin, A.R.; Yolken, R.H.; Kamali, M.; Heitzeg, M.M.; Kaplow, J.B.; Coryell, W.H.; McInnis, M.G. Cytomegalovirus Antibody Elevation in Bipolar Disorder: Relation to Elevated Mood States. Neural Plast. 2015, 2015, 939780. [Google Scholar] [CrossRef]
- Sweeten, T.L.; Posey, D.J.; McDougle, C.J. Brief report: Autistic disorder in three children with cytomegalovirus infection. J. Autism Dev. Disord. 2004, 34, 583–586. [Google Scholar] [CrossRef]
- Garofoli, F.; Lombardi, G.; Orcesi, S.; Pisoni, C.; Mazzucchelli, I.; Angelini, M.; Balottin, U.; Stronati, M. An Italian Prospective Experience on the Association Between Congenital Cytomegalovirus Infection and Autistic Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 1490–1495. [Google Scholar] [CrossRef]
- Sochocka, M.; Zwolińska, K.; Leszek, J. The Infectious Etiology of Alzheimer’s Disease. Curr. Neuropharmacol. 2017, 15, 996–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgdorf, K.S.; Trabjerg, B.B.; Pedersen, M.G.; Nissen, J.; Banasik, K.; Pedersen, O.B.; Sørensen, E.; Nielsen, K.R.; Larsen, M.H.; Erikstrup, C.; et al. Large-scale study of Toxoplasma and Cytomegalovirus shows an association between infection and serious psychiatric disorders. Brain Behav. Immun. 2019. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Origoni, A.; Schweinfurth, L.A.B.; Stallings, C.; Savage, C.L.G.; Sweeney, K.; Katsafanas, E.; Wilcox, H.C.; Khushalani, S.; Yolken, R. Clinical and Serological Predictors of Suicide in Schizophrenia and Major Mood Disorders. J. Nerv. Ment. Dis. 2018, 206, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Wilcox, H.C.; Adamos, M.; Katsafanas, E.; Khushalani, S.; Origoni, A.; Savage, C.; Schweinfurth, L.; Stallings, C.; Sweeney, K.; et al. Suicide Attempts and Markers of Immune Response in Individuals with Serious Mental Illness. J. Psychiatr. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bate, S.L.; Dollard, S.C.; Cannon, M.J. Cytomegalovirus seroprevalence in the United States: The national health and nutrition examination surveys, 1988–2004. Clin. Infect. Dis. 2010, 50, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef]
- Gindes, L.; Teperberg-Oikawa, M.; Sherman, D.; Pardo, J.; Rahav, G. Congenital cytomegalovirus infection following primary maternal infection in the third trimester. BJOG 2008, 115, 830–835. [Google Scholar] [CrossRef]
- Gabrielli, L.; Bonasoni, M.P.; Santini, D.; Piccirilli, G.; Chiereghin, A.; Petrisli, E.; Dolcetti, R.; Guerra, B.; Piccioli, M.; Lanari, M.; et al. Congenital cytomegalovirus infection: Patterns of fetal brain damage. Clin. Microbiol. Infect. 2012, 18, E419–E427. [Google Scholar] [CrossRef] [Green Version]
- Lyutenski, S.; Götz, F.; Giourgas, A.; Majdani, O.; Bültmann, E.; Lanfermann, H.; Lenarz, T.; Giesemann, A.M. Does severity of cerebral MRI lesions in congenital CMV infection correlates with the outcome of cochlear implantation? Eur. Arch. Otorhinolaryngol. 2017, 274, 1397–1403. [Google Scholar] [CrossRef]
- Hawkins-Villarreal, A.; Moreno-Espinosa, A.L.; Eixarch, E.; Marcos, M.A.; Martinez-Portilla, R.J.; Salazar, L.; Garcia-Otero, L.; Lopez, M.; Borrell, A.; Figueras, F.; et al. Blood parameters in fetuses infected with cytomegalovirus according to the severity of brain damage and trimester of pregnancy at cordocentesis. J. Clin. Virol. 2019, 119, 37–43. [Google Scholar] [CrossRef]
- Davis, N.L.; King, C.C.; Kourtis, A.P. Cytomegalovirus infection in pregnancy. Birth Defects Res. 2017, 109, 336–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenneson, A.; Cannon, M.J. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev. Med. Virol. 2007, 17, 253–276. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Grosse, S.D.; Ross, D.S. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev. Med. Virol. 2007, 17, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, E.; Revello, M.G.; Furione, M.; Zavattoni, M.; Lilleri, D.; Tassis, B.; Quarenghi, A.; Rustico, M.; Nicolini, U.; Ferrazzi, E.; et al. Prognostic markers of symptomatic congenital human cytomegalovirus infection in fetal blood. BJOG 2011, 118, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Micallef, S.; Galea, R. CMV encephalitis in an immune-competent patient. BMJ Case Rep. 2018. [Google Scholar] [CrossRef]
- Renard, T.; Daumas-Duport, B.; Auffray-Calvier, E.; Bourcier, R.; Desal, H. Cytomegalovirus encephalitis: Undescribed diffusion-weighted imaging characteristics. Original aspects of cases extracted from a retrospective study, and from literature review. J. Neuroradiol. 2016, 43, 371–377. [Google Scholar] [CrossRef]
- Goerig, N.L.; Frey, B.; Korn, K.; Fleckenstein, B.; Überla, K.; Schmidt, M.A.; Dörfler, A.; Engelhorn, T.; Eyüpoglu, I.; Rühle, P.F.; et al. Frequent occurrence of therapeutically reversible CMV-associated encephalopathy during radiotherapy of the brain. Neuro Oncol. 2016, 18, 1664–1672. [Google Scholar] [CrossRef] [Green Version]
- Sierra, A.; de Castro, F.; Del Rio-Hortega, J.; Iglesias-Rozas, J.R.; Garrosa, M.; Kettenmann, H. The “Big-Bang” for Modern Glial Biology: Translation and comments on Pío del Río-Hortega 1919 series of papers on microglia. Glia 2016, 64, 1801–1840. [Google Scholar] [CrossRef]
- Pandey, G.N.; Rizavi, H.S.; Zhang, H.; Bhaumik, R.; Ren, X. Abnormal protein and mRNA expression of inflammatory cytokines in the prefrontal cortex of depressed individuals who died by suicide. J. Psychiatry Neurosci. 2018, 43, 170192. [Google Scholar] [CrossRef] [Green Version]
- Al-Haddad, B.J.S.; Oler, E.; Armistead, B.; Elsayed, N.A.; Weinberger, D.R.; Bernier, R.; Burd, I.; Kapur, R.; Jacobsson, B.; Wang, C.; et al. The fetal origins of mental illness. Am. J. Obstet. Gynecol. 2019, 221, 549–562. [Google Scholar] [CrossRef]
- Zhang, Y.; Träskman-Bendz, L.; Janelidze, S.; Langenberg, P.; Saleh, A.; Constantine, N.; Okusaga, O.; Bay-Richter, C.; Brundin, L.; Postolache, T.T. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self-directed violence. J. Clin. Psychiatry. 2012, 73, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Okusaga, O.; Langenberg, P.; Sleemi, A.; Vaswani, D.; Giegling, I.; Hartmann, A.M.; Konte, B.; Friedl, M.; Groer, M.W.; Yolken, R.H.; et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with schizophrenia. Schizophr. Res. 2011, 133, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Burgdorf, K.S.; Simonsen, J.; Sundby, A.; Rostgaard, K.; Pedersen, O.B.; Sørensen, E.; Nielsen, K.R.; Bruun, M.T.; Frisch, M.; Edgren, G.; et al. Socio-demographic characteristics of Danish blood donors. PLoS ONE 2017, 12, e0169112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishii, T.; Hashimoto, E.; Ukai, W.; Kakutani, Y.; Sasaki, R.; Saito, T. Characteristics of attempted suicide by patients with schizophrenia compared with those with mood disorders: A case-controlled study in northern Japan. PLoS ONE 2014, 9, e96272. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Morinigo, J.D.; Fernandes, A.C.; Chang, C.K.; Hayes, R.D.; Broadbent, M.; Stewart, R.; David, A.S.; Dutta, R. Suicide completion in secondary mental healthcare: A comparison study between schizophrenia spectrum disorders and all other diagnoses. BMC Psychiatry 2014, 14, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keaton, S.A.; Madaj, Z.B.; Heilman, P.; Smart, L.; Grit, J.; Gibbons, R.; Postolache, T.T.; Roaten, K.; Achtyes, E.D.; Brundin, L. An inflammatory profile linked to increased suicide risk. J. Affect. Disord. 2019, 247, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Black, C.; Miller, B.J. Meta-analysis of cytokines and chemokines in suicidality: Distinguishing suicidal versus nonsuicidal patients. Biol. Psychiatry 2015, 78, 28–37. [Google Scholar] [CrossRef]
- Ganança, L.; Oquendo, M.A.; Tyrka, A.R.; Cisneros-Trujillo, S.; Mann, J.J.; Sublette, M.E. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology 2016, 63, 296–310. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.L.; Hsiao, E.Y.; Yan, Z.; Mazmanian, S.K.; Patterson, P.H. The placental interleukin-6 signaling controls fetal brain development and behavior. Brain Behav. Immun. 2017, 62, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Cheeran, M.C.; Lokensgard, J.R.; Schleiss, M.R. Neuropathogenesis of congenital cytomegalovirus infection: Disease mechanisms and prospects for intervention. Clin. Microbiol. Rev. 2009, 22, 99–126. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Ohgidani, M.; Kuwano, N.; Chrétien, F.; Lorin de la Grandmaison, G.; Onaya, M.; Tominaga, I.; Setoyama, D.; Kang, D.; Mimura, M.; et al. Suicide and microglia: Recent findings and future perspectives based on human studies. Front. Cell. Neurosci. 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study (Year) | Type of Study | Study Population | Case Population | Control Population | Analysis Method | Outcome |
|---|---|---|---|---|---|---|
| Burgdorf et al. [12] | Case control study | Data from 81,912 individuals from the Danish blood donor study. Total sample: 11,546 cases and controls | Blood donors who died by suicide or engaged in suicide attempts (n = 655) | Blood donors who did not die by suicide or engage in suicide attempts (n = 6503) | IgG anti cytomegalovirus (CMV). Solid phase ELISA | Seropositivity: 439/655 (67%) vs. 3886/6503 (59.7%), OR 1.31, 95% CI 1.10–1.56 |
| Zhang et al. [31] | Cross-sectional observational study | Suicide attempters from inpatients at Lund University Hospital, Sweden. | Patients admitted for suicide attempt (n = 54) | People randomly selected from the municipal population with no psychiatric condition or previous suicide attempt (n = 30) | IgG anti CMV, CMV titer. ELISA | Seropositivity: 33/53 (62.2%) vs. 16/29 (55.1%). |
| Controls from municipal population of Lund, Sweden. Total sample: 84 cases and controls | CMV IgG titer: 99.5 (±86.9) vs. 91.3 (±92.0) |
| Study (Year) | Type of Study | Study Population | Case Population | Control Population | Analysis Method | Outcome |
|---|---|---|---|---|---|---|
| Dickerson et al. 2018 [13] | Prospective study with 16y FU | Individuals with previous diagnosis of schizophrenia spectrum disorder, bipolar disorder or major depressive disorder. Total sample: 1292 individuals | Individuals with serious mental illness who died by suicide (n = 16) | Individuals with serious mental illness who did not die by suicide (n = 1276) | IgG anti-CMV titer. Solid phase ELISA. Antibody levels expressed as a ratio between the test sample divided by that of a standard control sample. | CMV IgG titer: 3.35 (±3.07) vs. 1.59 (±1.90). Association found between increasing levels of antibodies and Hazard Ratios. |
| Dickerson et al. 2017 [14] | Cross-sectional study | Individuals with previous diagnosis of schizophrenia spectrum disorder, bipolar disorder or major depressive disorder. Total sample: 162 patients | Individuals with serious mental illness with previous suicide attempts (n = 72) | Individuals with serious mental illness without a previous suicide attempt (n = 90) | Anti-CMV IgG and IgM titer. Solid phase ELISA. | Association between suicide attempts and IgM anti CMV measured as a continuous variable (coefficient 0.151). Increased odds of suicide for levels of IgM anti CMV ≥ 75th and 90th percentiles (OR 3.02 and 6.31 respectively). No association with IgG. |
| Okusaga et al. 2011 [32] | Cross-sectional study | Patients diagnosed with schizophrenia through SCID, recruited in the Munich area of Germany. Total sample: 950 patients | 351 individuals with schizophrenia with previous suicide attempts. | 599 individuals with schizophrenia with no previous suicide attempt. | IgG anti-CMV. Solid phase ELISA. | Seropositivity for CMV not associated with a history of suicide attempt. No further data provided. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paolini, M.; Lester, D.; Hawkins, M.; Hawkins-Villarreal, A.; Erbuto, D.; Fiorillo, A.; Pompili, M. Cytomegalovirus Seropositivity and Suicidal Behavior: A Mini-Review. Medicina 2019, 55, 782. https://doi.org/10.3390/medicina55120782
Paolini M, Lester D, Hawkins M, Hawkins-Villarreal A, Erbuto D, Fiorillo A, Pompili M. Cytomegalovirus Seropositivity and Suicidal Behavior: A Mini-Review. Medicina. 2019; 55(12):782. https://doi.org/10.3390/medicina55120782
Chicago/Turabian StylePaolini, Marco, David Lester, Michael Hawkins, Ameth Hawkins-Villarreal, Denise Erbuto, Andrea Fiorillo, and Maurizio Pompili. 2019. "Cytomegalovirus Seropositivity and Suicidal Behavior: A Mini-Review" Medicina 55, no. 12: 782. https://doi.org/10.3390/medicina55120782