The Effect of Primary Duodenogastric Bile Reflux on the Presence and Density of Helicobacter pylori and on Gastritis in Childhood


Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Endoscopic Evaluation
2.3. Histopathologic Evaluation
2.4. Ethical Board Approval
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fein, M.; Fuchs, K.H.; Bohrer, T.; Freys, S.M.; Thiede, A. Fiberoptic technique for 14-hour bile reflux monitoring. Dig. Dis. Sci. 1996, 41, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Keane, F.B.; Dimagno, E.P.; Malagelada, J.R. Duodenogastric reflux in humans: Its relationship to fasting antroduodenal motility and gastric, pancreatic and biliary secretion. Gastroenterology 1981, 81, 726–731. [Google Scholar] [CrossRef]
- Miiller-Lissner, S.A.; Fimmel, C.J.; Sonnenberg, A.; Will, N.; Müller-Duysing, W.; Heinzel, F.; Müller, R.; Blum, A.L. Novel approach to quantity duodenogastric reflux in healthy volunteers and in patients with type I gastric ulcus. Gut 1983, 24, 515–517. [Google Scholar]
- Pazzi, P.; Scalia, S.; Stabellini, G.; Trevisani, L.; Alvisi, V.; Guarneri, M. Bile reflux gastritis in patients without prior gastric surgery: Therapeutic effects of ursodeoxycholic asid. Curr. Ther. Res. 1989, 45, 476–487. [Google Scholar]
- Watt, P.C.H.; Sloan, J.M.; Spencer, A.; Kennedy, T.L. Histology of the postoperative stomach before and after diversion of bile. Br. Med. J. (Clin. Res. Ed.) 1983, 287, 1410–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermans, D.; Sokal, E.M.; Collard, J.M.; Romagnoli, R.; Buts, J.P. Primary duodenogastric reflux in children and adolescents. Eur. J. Pediatr. 2003, 162, 598–602. [Google Scholar] [CrossRef]
- Ortiz, P.; Santibanez, G.; Briones, E.; Marín, V.; Palma, A. Duodenogastric reflux: Validation study of its endoscopic visualization. Rev. Med. Chile. 1998, 126, 279–283. [Google Scholar]
- Lee, E.L.; Feldman, M. Gastritis and gastropathies. In Sleisenger and Fordtran’s Gastrointestinal and Liver Diseases, 8th ed.; Feldman, M., Friedman, L., Brandt, L.J., Eds.; Saunders Elsevier: Philadelphia, PA, USA, 2006; pp. 1067–1083. [Google Scholar]
- Loffeld, R.J.; Liberov, B.; Dekkers, P.E. The changing prevalence of upper gastrointestinal endoscopic diagnoses: A single-centre study. Neth. J. Med. 2012, 70, 222–226. [Google Scholar]
- Shih, W.J.; Shih, G.; Milan, P.P.; Chang, C.Y.; Huang, W.S. Intrathoracic gastric activity on cholescintigraphy results in a large hiatus hernia with duodenogastric reflux. Clin. Nucl. Med. 2010, 35, 376–378. [Google Scholar] [CrossRef]
- Pellicano, R.; Ribaldone, D.G.; Fagoonee, S.; Astegiano, M.; Saracco, G.M.; Megraud, F. A 2016 panorama of Helicobacter pylori infection: Key messages for clinicians. Panminerva Med. 2016, 58, 304–317. [Google Scholar]
- Miciuleviciene, J.; Calkauskas, H.; Jonaitis, L.; Kiudelis, G.; Tamošiūnas, V.; Praškevičius, A.; Kupčinskas, L.; Berg, D. Helicobacter pylori genotypes in Lithuanian patients with chronic gastritis and duodenal ulcer. Medicina 2008, 44, 449–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, H.J.; Wyatt, J.I.; Dixon, M.F.; Axon, A.T. Campylobacter like organisms and reflux gastritis. J. Clin. Pathol. 1986, 39, 531–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemela, S.; Karttunen, T.; Heikkla, J.; Mäentausta, O.; Lehtola, J. Relationship of Campylobacter pylori and duodenogastric reflux. Dig. Dis. Sci. 1989, 34, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Netzer, P.; Gut, A.; Brundler, R.; Gaia, C.; Halter, F.; Inauen, W. Influence of pantoprazole on oesophageal motility, and bile and acid reflux in patients with oesophagitis. Aliment. Pharmacol. Ther. 2001, 15, 1375–1384. [Google Scholar] [CrossRef]
- Ladas, S.D.; Katsogridakis, J.; Malamou, H.; Giannopoulou, H.; Kesse-Elia, M.; Raptis, S.A. Helicobacter pylori mayinduce bile reflux: Link between H pylori and bile-induced injury to gastric epithelium. Gut 1996, 38, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Gorrea, P. Classification and grading of gastritis. The updated Sydney system. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Gorrea, P. Histological classification of gastritis and Helicobacter pylori infection: An agreement at last. The International Workshop on the Histopathology of Gastritis? Helicobacter 1997, 2, S17–S24. [Google Scholar] [CrossRef]
- Barakat, E.A.; Abbas, N.F.; El-Kholi, N.Y. Primary bile reflux gastritis versus Helicobacterpylori gastritis: A comparative study. Egypt. J. Intern. Med. 2018, 30, 23–27. [Google Scholar] [CrossRef]
- Vere, C.C.; Cazacu, S.; Comănescu, V.; Mogoantă, L.; Rogoveanu, I.; Ciurea, T. Endoscopical and histological features in bile reflux gastritis. Rom. J. Morphol. Emberyol. 2005, 46, 269–274. [Google Scholar]
- Kellosalo, J.; Alavaikko, M.; Laitinen, S. Effect of biliary tract procedures on duodenogastric reflux and the gastric mucosa. Scand. J. Gastroenterol. 1991, 26, 1272–1278. [Google Scholar] [CrossRef]
- Mercan, E.; Duman, U.; Tihan, D.; Dilektasli, E.; Senol, K. Cholecystectomy and duodenogastric reflux: Interacting effects over the gastric mucosa. SpringerPlus 2016, 5, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yang, X.; Gu, W.; Shu, X.; Zhang, T.; Jiang, M. Histological features of the gastric mucosa in children with primary bile reflux gastritis. World J. Surg. Oncol. 2012, 10, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.W.; Mo, J.Z.; Zhi, L.M.; Chen, X.Y.; Shi, Y.; Xiao, S.D. The influence of longterm bile reflux on rat gastric mucosa. Chin. J. Dig. 2006, 26, 295–299. [Google Scholar]
- Chang, W.K.; Lin, C.K.; Chuan, D.C.; Chao, Y.C. Duodenogastric reflux: Proposed new endoscopic classification in symptomatic patients. J. Med. Sci. 2016, 36, 1–5. [Google Scholar]
- Taşkin, V.; Sedele, M.; Saka, O.; Kantarçeken, B. The effect of duodenogastric reflux on Helicobacter pylori presence and gastrichistopathologic changes. Turk. J. Gastroenterol. 2003, 14, 239–242. [Google Scholar] [PubMed]
- Itoh, M.; Wada, K.; Tan, S.; Kitano, Y.; Kai, J.; Makino, I. Antibacterial action of bile acids against Helicobacter pylori and changes in its ultrastructural morphology: Effect of unconjugated dihydroxy bile acid. J. Gastroenterol. 1999, 34, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Sobala, G.M.; O’Connor, H.J.; Dewar, E.P.; King, R.F.; Axon, A.T.; Dixon, M.F. Bile reflux and intestinal metaplasia in gastric mucosa. J. Clin. Pathol. 1993, 46, 235–240. [Google Scholar] [CrossRef]
- Szarszewski, A.; Korzon, M.; Kamiñska, B.; Lass, P. Duodenogastric reflux: Clinical and therapeutic aspects. Arch. Dis. Child. 1999, 81, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Tewari, S.N.; Cerezo, L.; Price, G. The prevelance of Campylobacter pylori gastritis: A study of symptomatic nonulcer dyspepsia and bile gastritis. J. Clin. Gastroenterol. 1989, 11, 271–277. [Google Scholar] [CrossRef]
- Matsuhisa, T.; Tsukui, T. Relation between reflux of bile acids into the stomach and gastric mucosal atrophy, intestinal metaplasia in biopsy specimens. J. Clin. Biochem. Nutr. 2012, 50, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Huajun, L.; Zhongyan, Z.; Yunfang, L.; Xiumei, Y.; Kaiyu, H.; Weiguo, H. Efficacy and safety of ursodeoxycholic acid in the treatment of children with bile reflux gastritis. Mod. Pract. Med. 2011, 23, 192–194. [Google Scholar]


{kind=link}
| Number | % | ||
|---|---|---|---|
| Gender | Male | 128 | 36 |
| Female | 233 | 64 | |
| Duodenogastric bile reflux | Yes | 45 | 13 |
| No | 316 | 87 | |
| Helicobacter pylori | Yes | 231 | 64 |
| No | 130 | 36 | |
| Helicobacter pylori density | 1 | 112 | 31 |
| 2 | 80 | 22 | |
| 3 | 39 | 11 | |
| Gastritis | Yes | 282 | 78 |
| No | 79 | 22 | |
| Gastritis severity | Mild | 135 | 37 |
| Moderate | 112 | 31 | |
| Severe | 35 | 10 | |
| Duodenogastric Bile Reflux | ||||
|---|---|---|---|---|
| Yes | No | p | ||
| Age | 13.9 ± 3.1 | 11.3 ± 4.7 | <0.001 | |
| Gender | Male | 15 (33%) | 113 (36%) | 0.750 |
| Female | 30 (67%) | 203 (64%) | ||
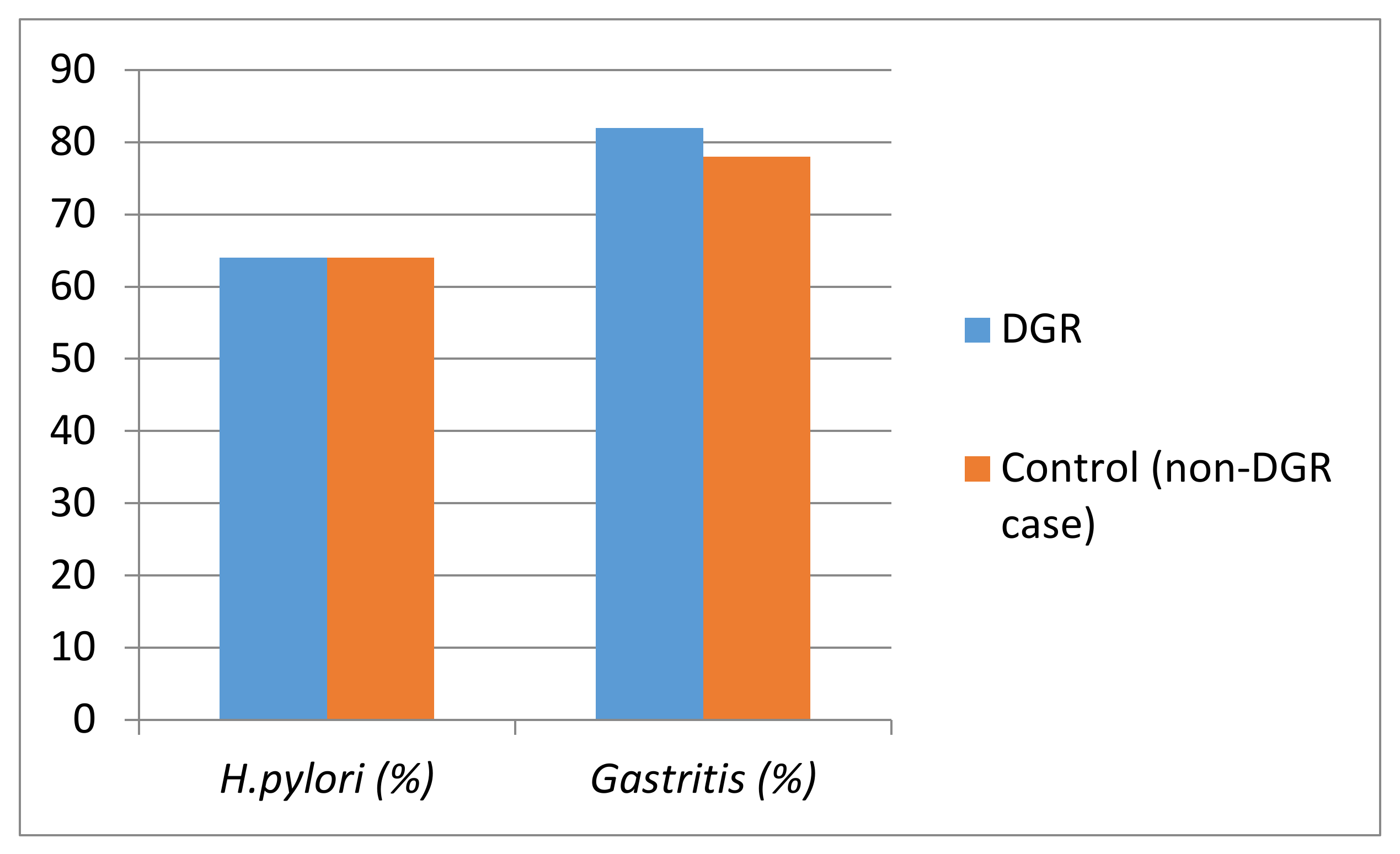
| Presence of Helicobacter pylori | Yes | 29 (64%) | 202 (64%) | 0.946 |
| No | 16 (36%) | 114 (36%) | ||
| Density of Helicobacter pylori | 1 | 13 (29%) | 99 (31%) | 0.244 |
| 2 | 8 (18%) | 72 (23%) | ||
| 3 | 8 (18%) | 31 (10%) | ||
| Gastritis | Yes | 37 (82%) | 245 (78%) | 0.476 |
| No | 8 (18%) | 71 (23%) | ||
| Gastritis severity | Mild | 19 (51%) | 116 (47%) | 0.829 |
| Moderate | 13 (35%) | 99 (40%) | ||
| Severe | 5 (14%) | 30 (12%) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agin, M.; Kayar, Y. The Effect of Primary Duodenogastric Bile Reflux on the Presence and Density of Helicobacter pylori and on Gastritis in Childhood. Medicina 2019, 55, 775. https://doi.org/10.3390/medicina55120775
Agin M, Kayar Y. The Effect of Primary Duodenogastric Bile Reflux on the Presence and Density of Helicobacter pylori and on Gastritis in Childhood. Medicina. 2019; 55(12):775. https://doi.org/10.3390/medicina55120775
Chicago/Turabian StyleAgin, Mehmet, and Yusuf Kayar. 2019. "The Effect of Primary Duodenogastric Bile Reflux on the Presence and Density of Helicobacter pylori and on Gastritis in Childhood" Medicina 55, no. 12: 775. https://doi.org/10.3390/medicina55120775