Presence of B19V in Patients with Thyroid Gland Disorders

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. B19V Serology by ELISA
2.3. Nested Polymerase Chain Reaction
2.4. Quantitative Real-Time PCR
2.5. Stastitical Analysis
3. Results
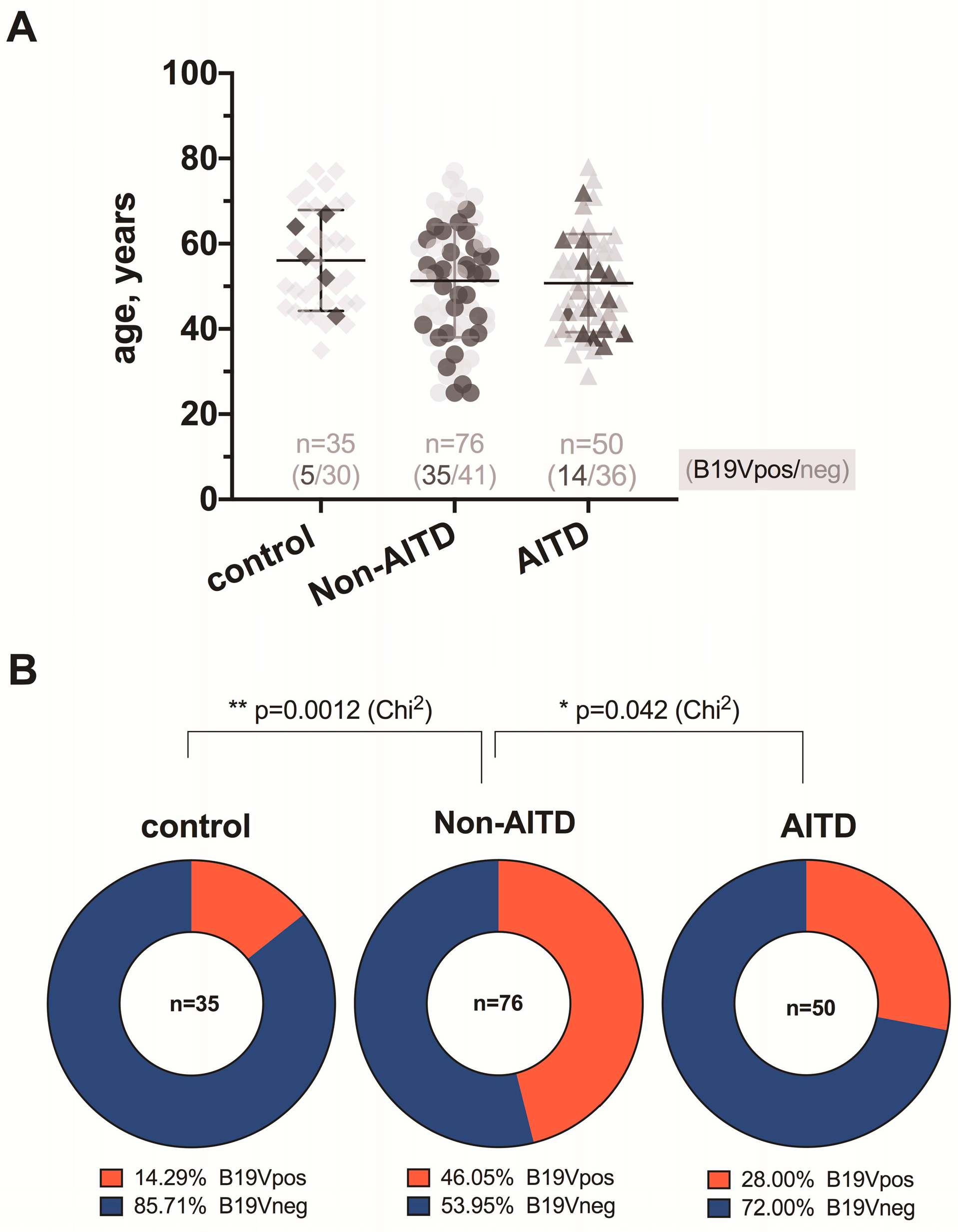
3.1. B19V Serology by ELISA
3.2. B19V NS Detection by Nested Polymerase Chain Reaction
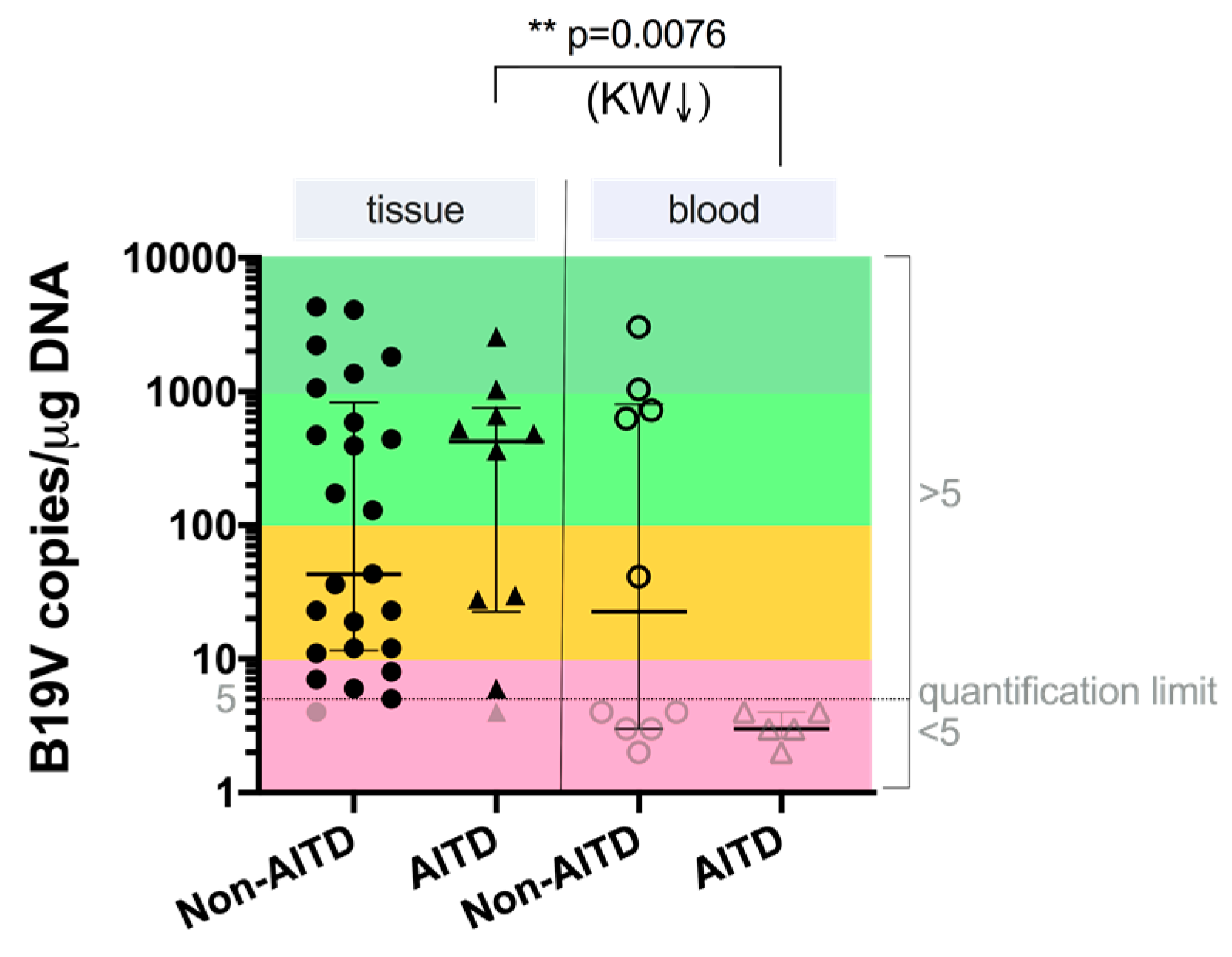
3.3. B19V Load by Quantitative Real-Time PCR
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ozawa, K.; Young, N. Characterization of capsid and noncapsid proteins of B19 parvovirus propagated in human erythroid bone marrow cell cultures. J. Virol. 1987, 61, 2627–2630. [Google Scholar] [PubMed]
- Pattison, J.R. B19 virus—A pathogenic human parvovirus. Blood Rev. 1987, 1, 58–64. [Google Scholar] [CrossRef]
- Anderson, L.J.; Tsou, C.; Parker, R.A.; Chorba, T.L.; Wulff, H.; Tattersall, P.; Mortimer, P.P. Detection of antibodies and antigens of human parvovirus B19 by enzyme-linked immunosorbent assay. J. Clin. Microbiol. 1986, 24, 522–526. [Google Scholar]
- Erdman, D.D.; Usher, M.J.; Tsou, C.; Caul, E.O.; Gary, G.W.; Kajigaya, S.; Young, N.S.; Anderson, L.J. Human parvovirus B19 specific IgG, IgA, and IgM antibodies and DNA in serum specimens from persons with erythema infectiosum. J. Med. Virol. 1991, 35, 110–115. [Google Scholar] [CrossRef]
- Brown, K.E.; Anderson, S.M.; Young, N.S. Erythrocyte P antigen: Cellular receptor for B19 parvovirus. Science 1993, 262, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Adamson-Small, L.A.; Ignatovich, I.V.; Laemmerhirt, M.G.; Hobbs, J.A. Persistent parvovirus B19 infection in non-erythroid tissues: Possible role in the inflammatory and disease process. Virus Res. 2014, 190, 8–16. [Google Scholar] [CrossRef]
- Chorba, T.; Coccia, P.; Holman, R.C.; Tattersall, P.; Anderson, L.J.; Sudman, J.; Young, N.S.; Kurczynski, E.; Saarinen, U.M.; Moir, R.; et al. The role of parvovirus B19 in aplastic crisis and erythema infectiosum (fifth disease). J. Infect. Dis. 1986, 154, 383–393. [Google Scholar] [CrossRef]
- Valentin, M.N.; Cohen, P.J. Pediatric parvovirus B19: Spectrum of clinical manifestations. Cutis 2013, 92, 179–184. [Google Scholar]
- Anderson, M.J.; Higgins, P.G.; Davis, L.R.; Willman, J.S.; Jones, S.E.; Kidd, I.M.; Pattison, J.R.; Tyrrell, D.A.J. Experimental parvoviral infection in humans. J. Infect. Dis. 1985, 152, 257–265. [Google Scholar] [CrossRef]
- Desailloud, R.; Hober, D. Viruses and thyroiditis: An update. Virol. J. 2009, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Kozireva, S.V.; Zestkova, J.V.; Mikazane, H.J.; Kadisa, A.L.; Kakurina, N.A.; Lejnieks, A.A.; Danilane, I.N.; Murovska, M.F. Incidence and clinical significance of parvovirus B19 infection in patients with rheumatoid arthritis. J. Rheumatol. 2008, 35, 1265–1270. [Google Scholar]
- Ferrari, S.M.; Fallahi, P.; Antonelli, A.; Benvenga, S. Environmental issues in thyroid diseases. Front. Endocrinol. (Lausanne) 2017, 8, 50. [Google Scholar] [CrossRef] [Green Version]
- Page, C.; Duverlie, G.; Sevestre, H.; Desailloud, R. Erythrovirus B19 and autoimmune thyroid diseases. Review of the literature and pathophysiological hypotheses. J. Med. Virol. 2015, 87, 162–169. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, W.; Liu, H.; Wang, D.; Wang, W.; Li, Y.; Wang, Z.; Wang, L.; Zhang, W.; Huang, G. Parvovirus B19 infection associated with Hashimoto’s thyroiditis in adults. J. Infect. 2010, 60, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Munakata, Y.; Saito, T.; Tani, J.I.; Nakagawa, Y.; Hoshikawa, S.; Ozaki, H.; Ito, S.; Yoshida, K. Intrathyroidal persistence of human parvovirus B19 DNA in a patient with Hashimoto’s thyroiditis. J. Infect. 2007, 55, e29–e31. [Google Scholar] [CrossRef] [PubMed]
- Saiki, R.K.; Gelfand, D.H.; Stoffel, S.; Scharf, S.J.; Higuchi, R.; Horn, G.T.; Mullis, K.B.; Erlich, H.A. Primer-directed enzymatic amplification of DNA with a thermostable DNA polymerase. Science 1988, 239, 487–491. [Google Scholar] [CrossRef]
- Barah, F.; Vallely, P.J.; Chiswick, M.L.; Cleator, G.M.; Kerr, J.R. Association of human parvovirus B19 infection with acute meningoencephalitis. Lancet 2001, 358, 729–730. [Google Scholar] [CrossRef]
- Page, C.; Hoffmann, T.W.; Benzerdjeb, N.; Duverlie, G.; Sevestre, H.; Desailloud, R. Detection of erythrovirus B19 in thyroidectomy specimens from Graves’ disease patients: A case-control study. J. Med. Virol. 2013, 85, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Chapenko, S.; Krumina, A.; Logina, I.; Rasa, S.; Chistjakovs, M.; Sultanova, A.; Viksna, L.; Murovska, M. Association of active human herpesvirus-6, -7 and parvovirus b19 infection with clinical outcomes in patients with myalgic encephalomyelitis/chronic fatigue syndrome. Adv. Virol. 2012, 2012, 205085. [Google Scholar] [CrossRef] [Green Version]
- Molenaar-de Backer, M.W.; Russcher, A.; Kroes, A.C.M.; Koppelman, M.H.G.M.; Lanfermeijer, M.; Zaaijer, H.L. Detection of parvovirus B19 DNA in blood: Viruses or DNA remnants? J. Clin. Virol. 2016, 84, 19–23. [Google Scholar] [CrossRef]
- Adamson, L.A.; Fowler, L.J.; Ewald, A.S.; Clare-Salzler, M.J.; Hobbs, J.A. Infection and persistence of erythrovirus B19 in benign and cancerous thyroid tissues. J. Med. Virol. 2014, 86, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Zhang, W.P.; Liu, H.X.; Wang, D.; Li, Y.F.; Wang, W.Q.; Wang, L.; He, F.R.; Wang, Z.; Yan, Q.G.; et al. Detection of human parvovirus B19 in papillary thyroid carcinoma. Br. J. Cancer 2008, 98, 611–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gravelsina, S.; Nora-Krukle, Z.; Svirskis, S.; Cunskis, E.; Murovska, M. Presence of B19V in Patients with Thyroid Gland Disorders. Medicina 2019, 55, 774. https://doi.org/10.3390/medicina55120774
Gravelsina S, Nora-Krukle Z, Svirskis S, Cunskis E, Murovska M. Presence of B19V in Patients with Thyroid Gland Disorders. Medicina. 2019; 55(12):774. https://doi.org/10.3390/medicina55120774
Chicago/Turabian StyleGravelsina, Sabine, Zaiga Nora-Krukle, Simons Svirskis, Egils Cunskis, and Modra Murovska. 2019. "Presence of B19V in Patients with Thyroid Gland Disorders" Medicina 55, no. 12: 774. https://doi.org/10.3390/medicina55120774