Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Primary Outcomes
2.4. Secondary Outcomes
2.5. Systematic Search
- Study design
- Total study duration
- Risk of bias (randomization if any, sequence generation, allocation sequence concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting and other concerns about bias).
- Total number of participants
- Diagnostic criteria for neuropathy, clinical (pain, burning, or dysesthesias in a stocking distribution, abnormal ankle reflexes or abnormal sensory signs) or electrophysiological
- Age of participants.
- Sex of participants.
- Antiretroviral therapy.
- Characteristics of interventions (treatment vs. placebo or treatment vs. other treatment).
- Number of different intervention groups (Active treatment vs. placebo or other treatment).
- Characteristics of treatment or intervention (dose, route of administration, duration).
- Information about withdrawals.
- Outcome measures (Pain, adverse events, discontinuation due to side effects).
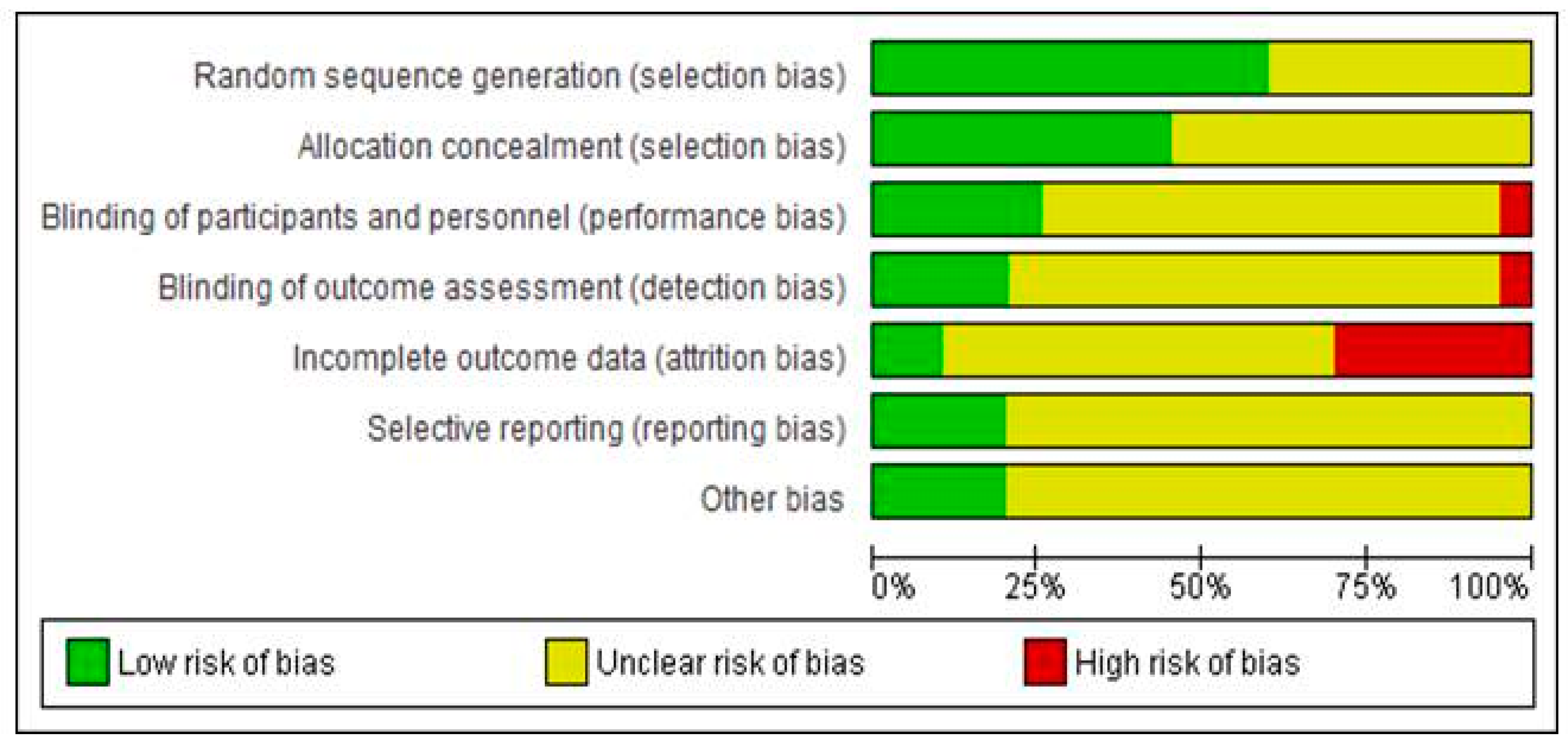
2.6. Assessment of Risk of Bias
- Random sequence generation (selection bias): The method of allocation sequence generation was assessed as: low risk of bias (random number table, computer random generator) and unclear risk of bias (when the method is not clearly stated)
- Allocation concealment (selection bias): The procedure followed for avoidance of allocation foresight or changing. We assessed methods as low risk of bias (telephone or central randomization, consecutively numbered, sealed, opaque envelopes) or unclear risk of bias (when method is not clearly stated).
- Blinding of participants and personnel (performance bias): Methods for blinding participants and personnel were assessed and judged as low risk of bias (when study described in detail the method of blinding) and unclear risk of bias (when study stated it was blinded but did not provide adequate description of how this was achieved or didn’t report this domain).
- Blinding of outcome assessment (detection bias): we assessed the methods used to blind the allocated interventions by outcome assessors. We assessed methods as low risk of bias (study states blinding of outcome assessments ensured) or unclear risk of bias (when method is not clearly stated) and high risk (no blinding of outcome assessment).
- Incomplete outcome data (attrition bias): we assessed the methods used to deal with incomplete data as low risk of bias (when <10% of participants did not complete the study or if a “baseline observation carried forward” was followed), unclear risk of bias (when a “last observation carried forward” methodology was followed) or high risk of bias (when a per protocol analysis was followed).
- Selective reporting (reporting bias): We assessed methods as low risk of bias (all of the study’s pre-specified outcomes were reported and a protocol is available), unclear risk (insufficient information and no available protocol) or high risk (not all of the study’s pre-specified criteria were reported).
2.7. Measures of Treatment Effect
2.8. Assessment of Heterogeneity
2.9. Sensitivity Analysis
2.10. Assessment of Reporting Biases
2.11. Data Synthesis
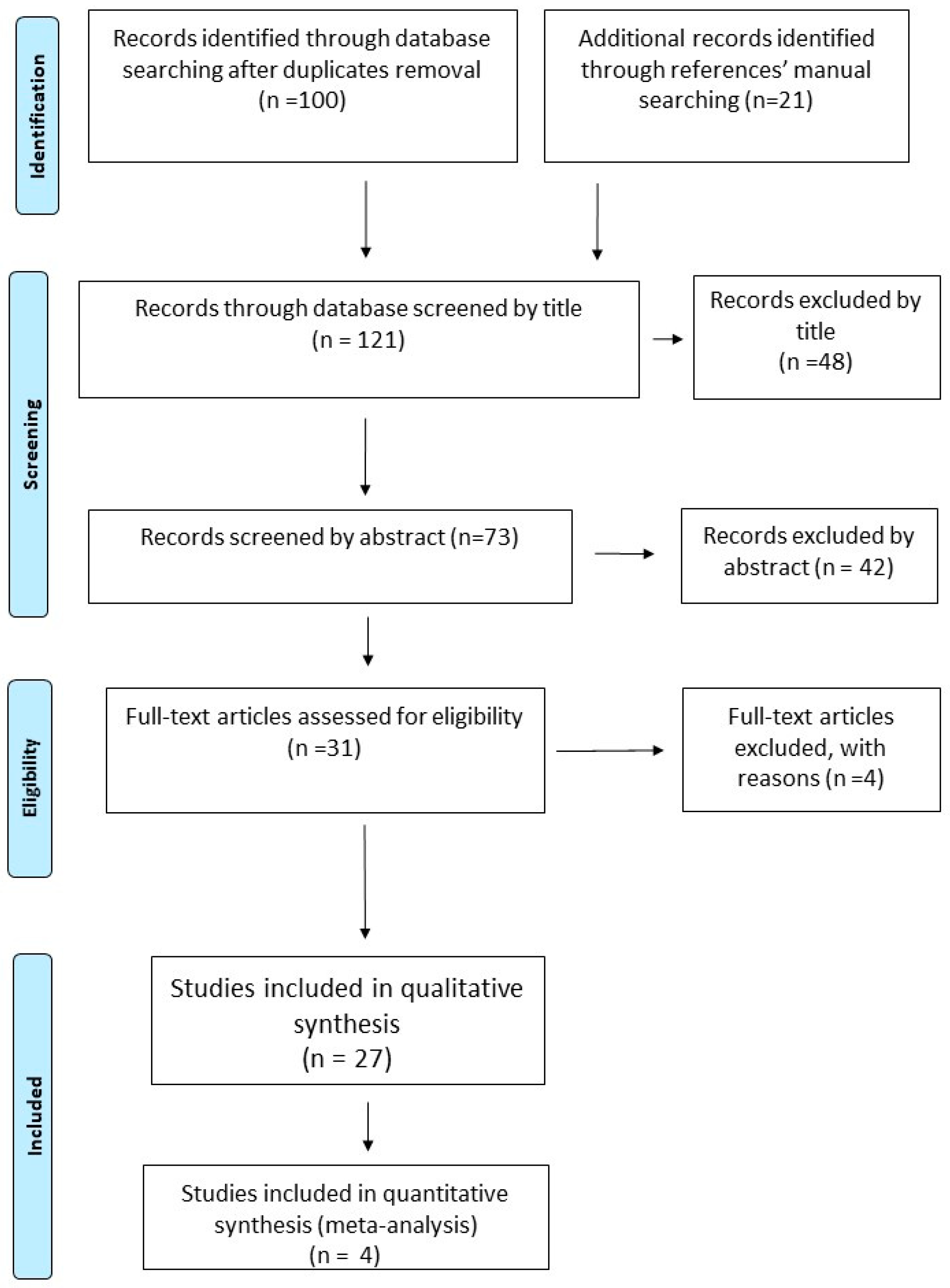
3. Results of the Search
3.1. Excluded Studies
3.2. Included Studies
Non-Pharmacologic Studies
3.3. Participants
3.4. Interventions
3.5. Outcomes
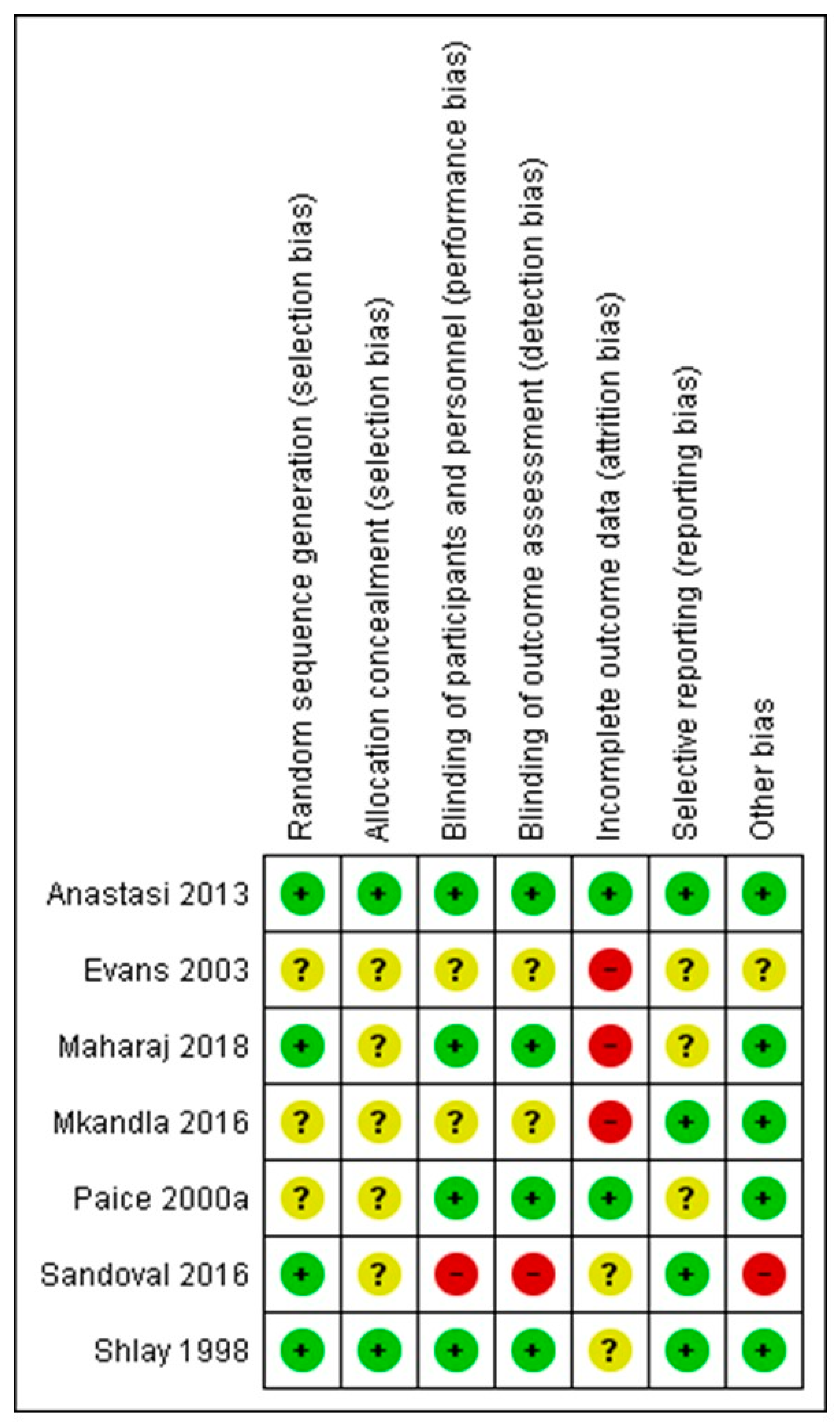
3.6. Risk of Bias of Included Non-Pharmacologic Studies
3.7. Aerobic Exercise (AE) and Progressive Resisted Exercises (PRE)
3.8. Acupuncture/Moxibustion (Acu/Moxa)
3.9. Lower Extremity Splinting (LES)
3.10. Cognitive Behaviour Therapy (CBT) vs. Supportive Psychotherapy (SP)
3.11. Vibratory Stimulus (VS)
4. Pharmacologic Interventions
4.1. Participants
4.2. Interventions
4.3. Outcomes
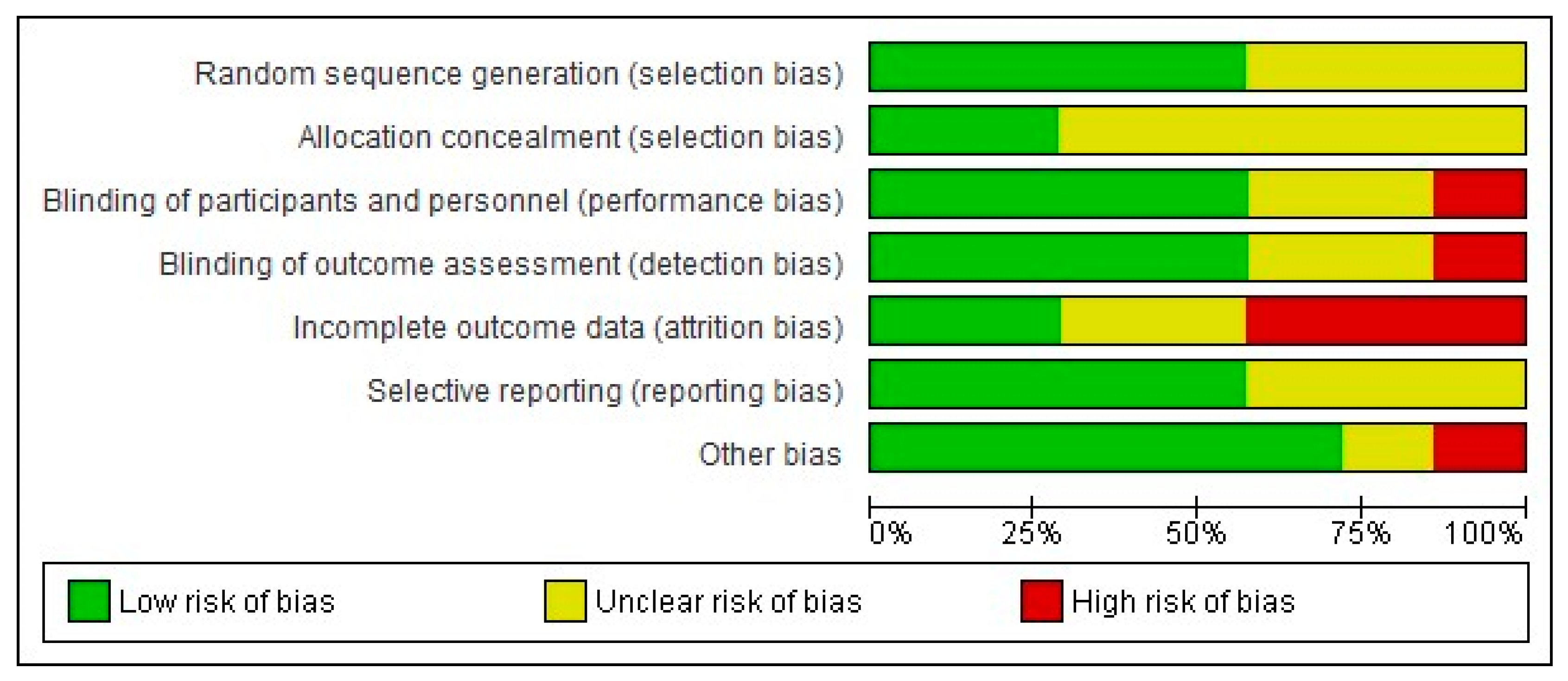
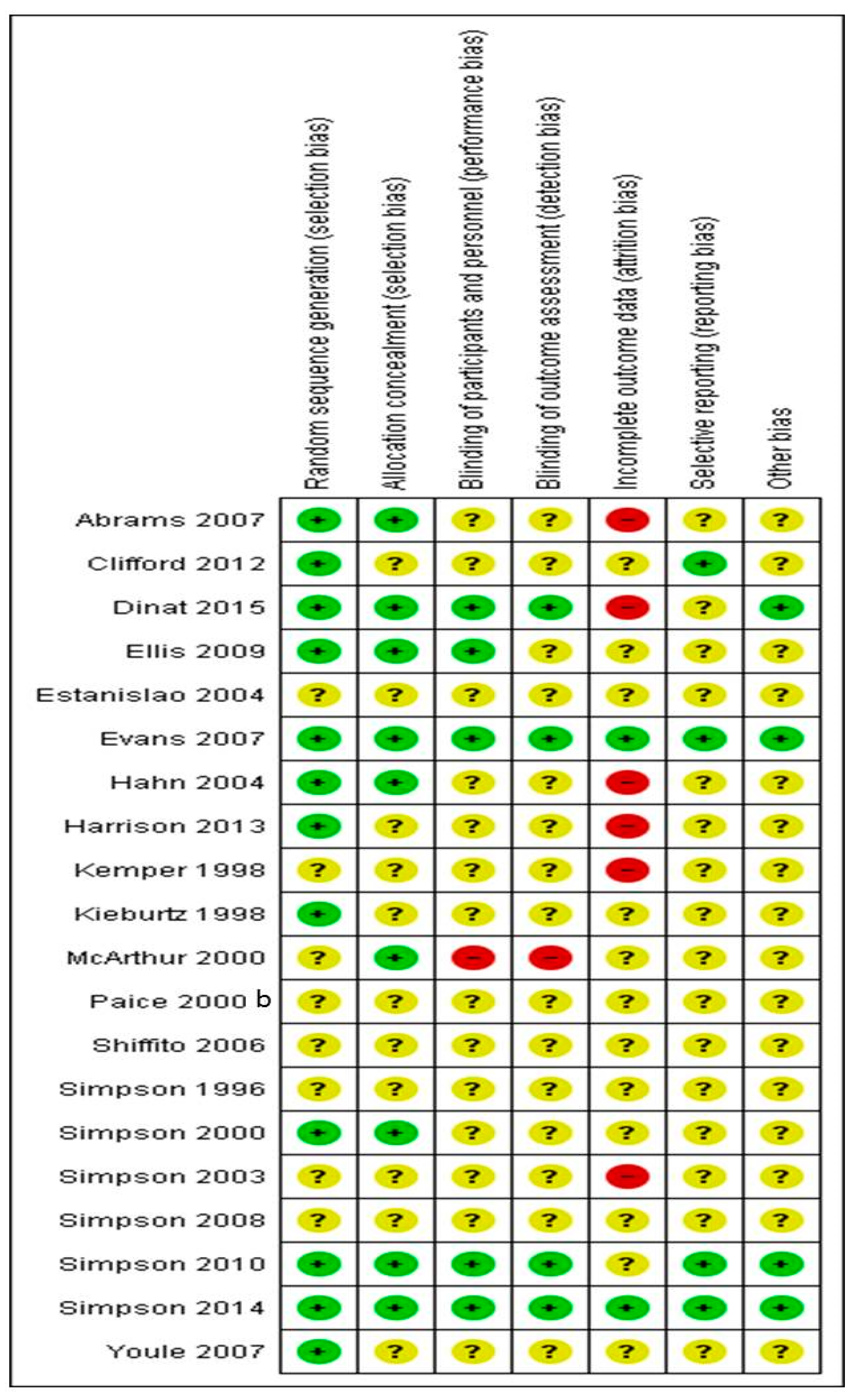
5. Risk of Bias in Included Studies
6. Allocation (Selection Bias)
7. Allocation Concealment (Selection Bias)
8. Blinding of Participants and Personnel (Performance Bias and Detection Bias)
9. Blinding of Outcome Assessment (Detection Bias)
10. Incomplete Outcome Data (Attrition Bias)
11. Selective Reporting (Reporting Bias)
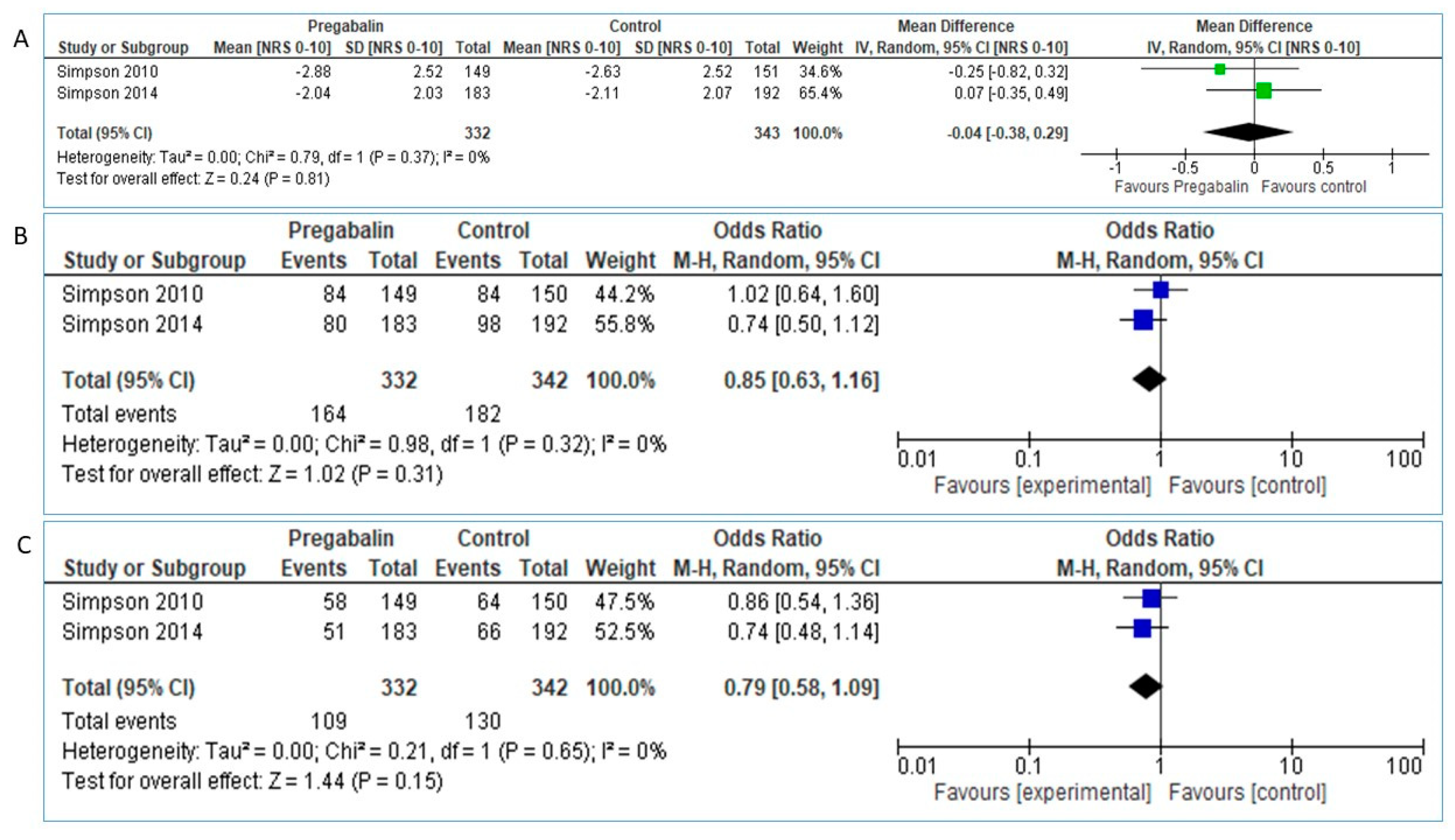
12. Pregabalin
12.1. Primary Efficacy Outcomes
12.2. Secondary Efficacy Outcomes
12.3. Safety
12.4. Smoked Cannabis
12.5. Primary Efficacy Outcomes
12.6. Secondary Efficacy Outcomes
12.7. Safety Outcomes
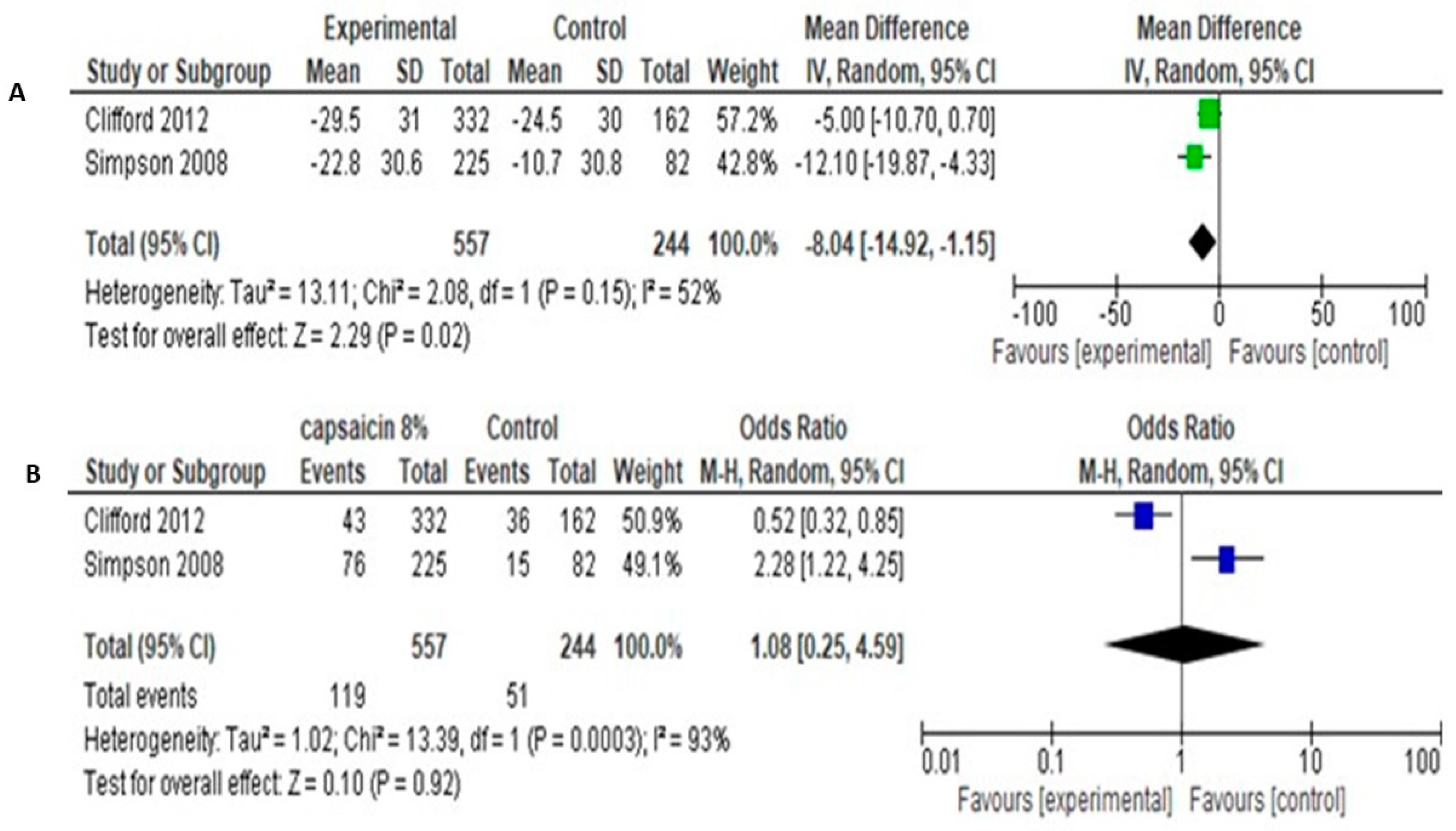
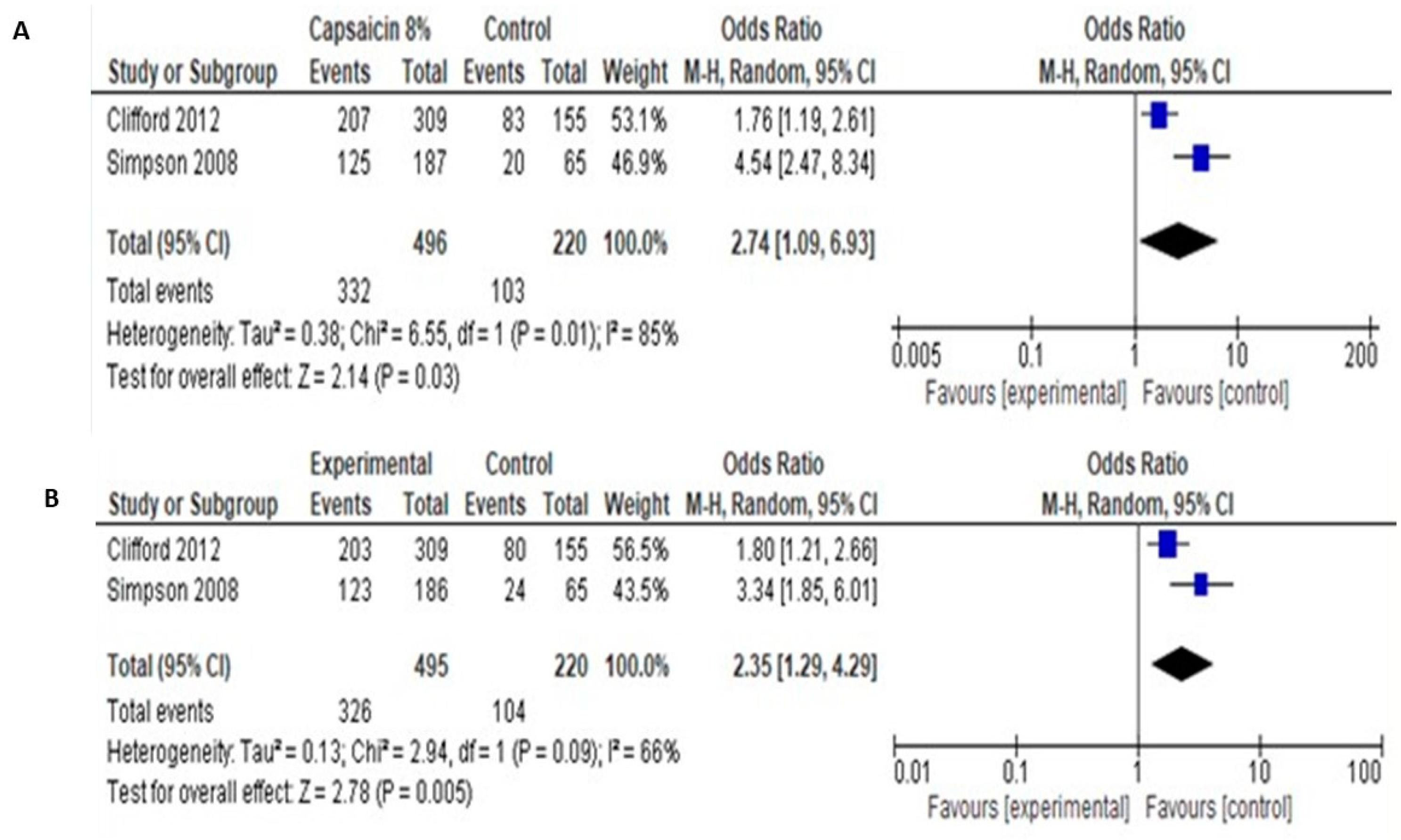
12.8. Capsaicin
13. Primary Efficacy Outcome
13.1. Lamotrigine
13.2. Amitryptiline and Mexiletine
13.3. Gabapentin (GBP)
13.4. Recombinant Human NGF (rhNGF)
13.5. Acetyl L-Carnitine
13.6. Lidocaine
13.7. Peptide T
13.8. Prosaptide
13.9. Memantine
13.10. Duloxetine, Methadone
14. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Pillay, P.; Wadley, A.L.; Cherry, C.L.; Karstaedt, A.S.; Kamerman, P.R. Psychological Factors Associated With Painful Versus Non-Painful HIV-Associated Sensory Neuropathy. AIDS Behav. 2018, 22, 1584–1595. [Google Scholar] [CrossRef] [PubMed]
- Morgello, S.; Estanislao, L.; Simpson, D.; Geraci, A.; DiRocco, A.; Gerits, P.; Naseer, M. HIV-associated distal sensory polyneuropathy in the era of highly active antiretroviral therapy: The Manhattan HIV Brain Bank. Arch. Neurol. 2004, 61, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, K.A.; Armon, C.; Baron, A.; Moorman, A.C.; Wood, K.C.; Holmberg, S.D. Modification of the incidence of drug-associated symmetrical peripheral neuropathy by host and disease factors in the HIV outpatient study cohort. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005, 40, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Kamerman, P.R.; Moss, P.J.; Weber, J.; Wallace, V.C.; Rice, A.S.; Huang, W. Pathogenesis of HIV-associated sensory neuropathy: Evidence from in vivo and in vitro experimental models. J. Peripher. Nerv. Syst. JPNS 2012, 17, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, D.J.; McDonald, M.; Portenoy, R.K.; Rosenfeld, B.; Passik, S.; Breitbart, W. Pain syndromes and etiologies in ambulatory AIDS patients. Pain 1997, 70, 117–123. [Google Scholar] [CrossRef]
- Tagliati, M.; Grinnell, J.; Godbold, J.; Simpson, D.M. Peripheral nerve function in HIV infection: Clinical, electrophysiologic, and laboratory findings. Arch. Neurol. 1999, 56, 84–89. [Google Scholar] [CrossRef]
- Adoukonou, T.A.; Kouna-Ndouongo, P.; Kpangon, A.; Gnonlonfoun, D.; Kpacha, B.; Dovonou, A.; Houinato, D. Distal sensory polyneuropathy among HIV-infected patients at Parakou University Hospital, Benin, 2011. Med. Sante Trop. 2017, 27, 190–194. [Google Scholar] [CrossRef]
- Phillips, T.J.; Brown, M.; Ramirez, J.D.; Perkins, J.; Woldeamanuel, Y.W.; Williams, A.C.D.C.; Maier, C. Sensory, psychological, and metabolic dysfunction in HIV-associated peripheral neuropathy: A cross-sectional deep profiling study. Pain 2014, 155, 1846–1860. [Google Scholar] [CrossRef]
- Merlin, J.S.; Cen, L.; Praestgaard, A.; Turner, M.; Obando, A.; Alpert, C.; Frank, I. Pain and physical and psychological symptoms in ambulatory HIV patients in the current treatment era. J. Pain Symptom Manag. 2012, 43, 638–645. [Google Scholar] [CrossRef]
- Keltner, J.R.; Vaida, F.; Ellis, R.J.; Moeller-Bertram, T.; Fitzsimmons, C.; Duarte, N.A.; Simpson, D.M. Health-related quality of life ‘well-being’ in HIV distal neuropathic pain is more strongly associated with depression severity than with pain intensity. Psychosomatics 2012, 53, 380–386. [Google Scholar] [CrossRef]
- Uebelacker, L.A.; Weisberg, R.B.; Herman, D.S.; Bailey, G.L.; Pinkston-Camp, M.M.; Stein, M.D. Chronic Pain in HIV-Infected Patients: Relationship to Depression, Substance Use, and Mental Health and Pain Treatment. Pain Med. 2015, 16, 1870–1881. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.; Stein, D.J.; Jelsma, J. Pain in people living with HIV/AIDS: A systematic review. J. Int. AIDS Soc. 2014, 17, 18719. [Google Scholar] [CrossRef] [PubMed]
- Gabbai, A.A.; Castelo, A.; Oliveira, A.S. HIV peripheral neuropathy. Handb. Clin. Neurol. 2013, 115, 515–529. [Google Scholar] [PubMed]
- Aziz-Donnelly, A.; Harrison, T.B. Update of HIV-Associated Sensory Neuropathies. Curr. Treat. Options Neurol. 2017, 19, 36. [Google Scholar] [CrossRef]
- Phillips, T.J.; Cherry, C.L.; Cox, S.; Marshall, S.J.; Rice, A.S. Pharmacological treatment of painful HIV-associated sensory neuropathy: A systematic review and meta-analysis of randomised controlled trials. PLoS ONE 2010, 5, e14433. [Google Scholar] [CrossRef]
- Harrison, T.; Miyahara, S.; Lee, A.; Evans, S.; Bastow, B.; Simpson, D.; Clifford, D.B. Experience and challenges presented by a multicenter crossover study of combination analgesic therapy for the treatment of painful HIV-associated polyneuropathies. Pain Med. 2013, 14, 1039–1047. [Google Scholar] [CrossRef]
- Merlin, J.S.; Bulls, H.W.; Vucovich, L.A.; Edelman, E.J.; Starrels, J.L. Pharmacologic and non-pharmacologic treatments for chronic pain in individuals with HIV: A systematic review. AIDS Care 2016, 28, 1506–1515. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Brandenburg, N. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain Off. J. Am. Pain Soc. 2008, 9, 105–121. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Version 5.1 Cochrane Handbook for Systematic Reviews 2011 [cited March 2011 20/3/2019]. Available online: https://handbook-5-1.cochrane.org/ (accessed on 22 November 2019).
- Brown, S.; Simpson, D.M.; Moyle, G.; Brew, B.J.; Schifitto, G.; Larbalestier, N.; Tobias, J.K. NGX-4010, a capsaicin 8% patch, for the treatment of painful HIV-associated distal sensory polyneuropathy: Integrated analysis of two phase III, randomized, controlled trials. AIDS Res. Ther. 2013, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Silver, M.; Blum, D.; Grainger, J.; Hammer, A.E.; Quessy, S. Double-blind, placebo-controlled trial of lamotrigine in combination with other medications for neuropathic pain. J. Pain Symptom Manag. 2007, 34, 446–454. [Google Scholar] [CrossRef]
- Nazarbaghi, S.; Amiri-Nikpour, M.R.; Eghbal, A.F.; Valizadeh, R. Comparison of the effect of topiramate versus gabapentin on neuropathic pain in patients with polyneuropathy: A randomized clinical trial. Electron. Physician 2017, 9, 5617–5622. [Google Scholar] [CrossRef] [PubMed]
- Penza, P.; Bricchi, M.; Scola, A.; Campanella, A.; Lauria, G. Electroacupuncture is not effective in chronic painful neuropathies. Pain Med. 2011, 12, 1819–1823. [Google Scholar] [CrossRef]
- Sandoval, R.; Roddey, T.; Giordano, T.P.; Mitchell, K.; Kelley, C. Randomized Trial of Lower Extremity Splinting to Manage Neuropathic Pain and Sleep Disturbances in People Living with HIV/AIDS. J. Int. Assoc. Provid. AIDS Care 2016, 15, 240–247. [Google Scholar] [CrossRef]
- Paice, J.A.; Shott, S.; Oldenburg, F.P.; Zeller, J.; Swanson, B. Efficacy of a vibratory stimulus for the relief of HIV-associated neuropathic pain. Pain 2000, 84, 291–296. [Google Scholar] [CrossRef]
- Mkandla, K.; Myezwa, H.; Musenge, E. The effects of progressive-resisted exercises on muscle strength and health-related quality of life in persons with HIV-related poly-neuropathy in Zimbabwe. AIDS Care 2016, 28, 639–643. [Google Scholar] [CrossRef]
- Maharaj, S.S.; Yakasai, A.M. Does a Rehabilitation Program of Aerobic and Progressive Resisted Exercises Influence HIV-Induced Distal Neuropathic Pain? Am. J. Phys. Med. Rehabil. 2018, 97, 364–369. [Google Scholar] [CrossRef]
- Evans, S.; Fishman, B.; Spielman, L.; Haley, A. Randomized trial of cognitive behavior therapy versus supportive psychotherapy for HIV-related peripheral neuropathic pain. Psychosomatics 2003, 44, 44–50. [Google Scholar] [CrossRef]
- Anastasi, J.K.; Capili, B.; McMahon, D.J.; Scully, C. Acu/Moxa for distal sensory peripheral neuropathy in HIV: A randomized control pilot study. J. Assoc. Nurses AIDS Care JANAC 2013, 24, 268–275. [Google Scholar] [CrossRef]
- Shlay, J.C.; Chaloner, K.; Max, M.B.; Flaws, B.; Reichelderfer, P.; Wentworth, D. Acupuncture and amitriptyline for pain due to HIV-related peripheral neuropathy: A randomized controlled trial. Terry Beirn Community Programs for Clinical Research on AIDS. Jama 1998, 280, 1590–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, D.M.; Schifitto, G.; Clifford, D.B.; Murphy, T.K.; Durso-De Cruz, E.; Glue, P.; Freeman, R. Pregabalin for painful HIV neuropathy: A randomized, double-blind, placebo-controlled trial. Neurology 2010, 74, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Rice, A.S.; Emir, B.; Landen, J.; Semel, D.; Chew, M.L.; Sporn, J. A randomized, double-blind, placebo-controlled trial and open-label extension study to evaluate the efficacy and safety of pregabalin in the treatment of neuropathic pain associated with human immunodeficiency virus neuropathy. Pain 2014, 155, 1943–1954. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.I.; Jay, C.A.; Shade, S.B.; Vizoso, H.; Reda, H.; Press, S.; Petersen, K.L. Cannabis in painful HIV-associated sensory neuropathy: A randomized placebo-controlled trial. Neurology 2007, 68, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.J.; Toperoff, W.; Vaida, F.; van den Brande, G.; Gonzales, J.; Gouaux, B.; Atkinson, J.H. Smoked medicinal cannabis for neuropathic pain in HIV: A randomized, crossover clinical trial. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2009, 34, 672–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, D.B.; Simpson, D.M.; Brown, S.; Moyle, G.; Brew, B.J.; Conway, B. A randomized, double-blind, controlled study of NGX-4010, a capsaicin 8% dermal patch, for the treatment of painful HIV-associated distal sensory polyneuropathy. J. Acquir. Immune Defic. Syndr. 2012, 59, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Brown, S.; Tobias, J.; Group N-CS. Controlled trial of high-concentration capsaicin patch for treatment of painful HIV neuropathy. Neurology 2008, 70, 2305–2313. [Google Scholar] [CrossRef]
- Paice, J.A.; Ferrans, C.E.; Lashley, F.R.; Shott, S.; Vizgirda, V.; Pitrak, D. Topical capsaicin in the management of HIV-associated peripheral neuropathy. J. Pain Symptom Manag. 2000, 19, 45–52. [Google Scholar] [CrossRef]
- Simpson, D.M.; Olney, R.; McArthur, J.C.; Khan, A.; Godbold, J.; Ebel-Frommer, K. A placebo-controlled trial of lamotrigine for painful HIV-associated neuropathy. Neurology 2000, 54, 2115–2119. [Google Scholar] [CrossRef]
- Simpson, D.M.; McArthur, J.C.; Olney, R.; Clifford, D.; So, Y.; Ross, D. Lamotrigine for HIV-associated painful sensory neuropathies: A placebo-controlled trial. Neurology 2003, 60, 1508–1514. [Google Scholar] [CrossRef]
- Dinat, N.; Marinda, E.; Moch, S.; Rice, A.S.; Kamerman, P.R. Randomized, Double-Blind, Crossover Trial of Amitriptyline for Analgesia in Painful HIV-Associated Sensory Neuropathy. PLoS ONE 2015, 10, e0126297. [Google Scholar] [CrossRef] [PubMed]
- Kieburtz, K.; Simpson, D.; Yiannoutsos, C.; Max, M.B.; Hall, C.D.; Ellis, R.J.; Clifford, D.B.; AIDS Clinical Trial Group 242 Protocol Team. A randomized trial of amitriptyline and mexiletine for painful neuropathy in HIV infection. Neurology 1998, 51, 1682–1688. [Google Scholar] [CrossRef] [PubMed]
- Kemper, C.A.; Kent, G.; Burton, S.; Deresinski, S.C. Mexiletine for HIV-infected patients with painful peripheral neuropathy: A double-blind, placebo-controlled, crossover treatment trial. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. Off. Publ. Int. Retrovirol. Assoc. 1998, 19, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.; Arendt, G.; Braun, J.S.; von Giesen, H.J.; Husstedt, I.W.; Maschke, M. A placebo-controlled trial of gabapentin for painful HIV-associated sensory neuropathies. J. Neurol. 2004, 251, 1260–1266. [Google Scholar] [CrossRef]
- McArthur, J.C.; Yiannoutsos, C.; Simpson, D.M.; Adornato, B.T.; Singer, E.J.; Hollander, H.; Navia, B.A.; AIDS Clinical Trials Group Team 291. A phase II trial of nerve growth factor for sensory neuropathy associated with HIV infection. Neurology 2000, 54, 1080–1088. [Google Scholar] [CrossRef]
- Youle, M.; Osio, M.; ALCAR Study Group. A double-blind, parallel-group, placebo-controlled, multicentre study of acetyl L-carnitine in the symptomatic treatment of antiretroviral toxic neuropathy in patients with HIV-1 infection. HIV Med. 2007, 8, 241–250. [Google Scholar] [CrossRef]
- Estanislao, L.; Carter, K.; McArthur, J.; Olney, R.; Simpson, D.; Lidoderm HIVNG. A randomized controlled trial of 5% lidocaine gel for HIV-associated distal symmetric polyneuropathy. J. Acquir. Immune Defic. Syndr. 2004, 37, 1584–1586. [Google Scholar] [CrossRef]
- Simpson, D.M.; Dorfman, D.; Olney, R.K.; McKinley, G.; Dobkin, J.; So, Y.; Friedman, B.; The Peptide T Neuropathy Study Group. Peptide T in the treatment of painful distal neuropathy associated with AIDS: Results of a placebo-controlled trial. Neurology 1996, 47, 1254–1259. [Google Scholar] [CrossRef]
- Evans, S.R.; Simpson, D.M.; Kitch, D.W.; King, A.; Clifford, D.B.; Cohen, B.A. A randomized trial evaluating Prosaptide for HIV-associated sensory neuropathies: Use of an electronic diary to record neuropathic pain. PLoS ONE 2007, 2, e551. [Google Scholar] [CrossRef] [Green Version]
- Schifitto, G.; Yiannoutsos, C.T.; Simpson, D.M.; Marra, C.M.; Singer, E.J.; Kolson, D.L. A placebo-controlled study of memantine for the treatment of human immunodeficiency virus-associated sensory neuropathy. J. Neurovirol. 2006, 12, 328–331. [Google Scholar] [CrossRef]
- Anastasi, J.K.; Capili, B.; Chang, M. HIV peripheral neuropathy and foot care management: A review of assessment and relevant guidelines. Am. J. Nurs. 2013, 113, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Gazda, S.; Brown, S.; Webster, L.R.; Lu, S.P.; Tobias, J.K. Long-term safety of NGX-4010, a high-concentration capsaicin patch, in patients with peripheral neuropathic pain. J. Pain Symptom Manag. 2010, 39, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Brown, S.; Tobias, J.K.; Vanhove, G.F.; Group N-CS. NGX-4010, a capsaicin 8% dermal patch, for the treatment of painful HIV-associated distal sensory polyneuropathy: Results of a 52-week open-label study. Clin. J. Pain 2014, 30, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.P. Peripheral neuropathy and light-preliminary report indicating prevalence of nanobacteria in HIV. J. Proteome Res. 2003, 2, 665–666. [Google Scholar] [CrossRef]
- Stockings, E.; Campbell, G.; Hall, W.D.; Nielsen, S.; Zagic, D.; Rahman, R.; Degenhardt, L. Cannabis and cannabinoids for the treatment of people with chronic noncancer pain conditions: A systematic review and meta-analysis of controlled and observational studies. Pain 2018, 159, 1932–1954. [Google Scholar] [CrossRef]
- Moore, R.A.; Derry, S.; Aldington, D.; Cole, P.; Wiffen, P.J. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Guolo, A.; Varin, C. Random-effects meta-analysis: The number of studies matters. Stat Methods Med. Res. 2017, 26, 1500–1518. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adverse events | No data | No data | 16/23 of the LES group: discomfort |
| Data | NRS 0–10 at 12 weeks Median (IQR): AE = 1.0 (1.0), PRE = 1.0 (1.0), control = 3.0 (1.0). AE vs. control, p < 0.001, effect size, r = 0.75. PRE vs. control p < 0.001, effect size r = 0.83 | QOL state of Health: F ratio = 4.24 SE = 0.05, CI:00–0.12 (p = 0.04), | Pain scale 0–100: Splint: −32.89 (23.23%), Sham: −14.52% (39.74%), p = 935 Pain reduction > 30% Splint 11/18 Liner 5/19 |
| Outcome measures | Per protocol analysis Pain intensity and distress NRS 0–10 | HR-QOL: ED-5D mobility, EQ-5D self-care, EQ-5D usual activity, EQ-5D pain or Discomfort, EQ-5D anxiety/depression, EQ-5D state of health level | Neuropathic Pain Scale 0–100 The Pittsburgh Sleep Quality Index (PSQI) 0–21 |
| Intervention | Aerobic exercise (AE) vs. Progressive resisted exercises (PRE) vs. control. Sessions of 30 min, 3 times/week for 12 weeks | Progressive resisted exercises (PRE) vs. control. Sessions of 30 min, 2 times/week for 12 wee | Walkabout splints or sham (liners only) during night sleep |
| ARV therapy | >6 six months | cART control/PRE: 6–12 months 32/26, 13–24 months 11/9, >25 months 37/45 | Splints:20/23 Sham: 20/22 |
| Sex F/M | AE = 27/18, PRE = 23/21, Control = 27/24 | PRE: 57/23 Control: 56/24 | Splints: 9/14 Sham: 10/12 |
| Age | AE:38.29 (8.06) PRE:35.98 (8.53) Control: 36.13 (8.10) | 42.2 (8.5) | Splints: 50.65 (8.04) Sham: 46.09 (8.13) |
| Diagnostic criteria | Referred as diagnosed with HIVDSN | Referred as diagnosed with HIVDSN | Referred as diagnosed with HIVDSN |
| Duration | 12 weeks | 12 weeks | 6 weeks |
| Design | RCT parallel design | RCT parallel design | RCT parallel design |
| Participants randomized (completed) | 154 (136) | 160 (64) | 46 (35) |
| Reference | Maharaj et al. 2018 [30] | Mkandla et al. 2016 [29] | Sandoval et al. 2016 [7] |
| Adverse events | Mild bruising | No data | No data |
| Data | Acu/moxa: 0.85 (SE = 0.12) Sham/control 1.10 (SE = 0.09) p = 0.05 | BPI average pain intensity Cognitive: −2.6 (3.2) Supportive psychotherapy: −1.3(2.1) (p > 0.05) | Vibration therapy: −67.3% (33.4%) Sham therapy: −55% (32%), p = 0.92 |
| Outcome measures | Daily symptom diary (SD) that incorporated the GPS (0–1.77) Subjective Peripheral Neuropathy Screen (SPNS) | BPI average pain intensity The Brief Symptom Inventory Self-report Beck Depression Inventory Hamilton Depression Rating Scale The Karnofsky Performance Scale | Current-pain item in the Brief Pain Inventory 0 = 10 |
| Intervention | Acu/Moxa vs Sham/control | Cognitive behavioural intervention or supportive psychotherapy once weekly | Vibration therapy for 45 min vs. sham therapy for 45 min |
| ARV therapy | Stable regimen for >8 weeks | No data | No data |
| Sex F/M | Acu/Moxa: 5/20 Sham/Con: 6/19 | 13/48 | 12/28 |
| Age | Acu/Moxa: 47.8 (7.2) Sham/control: 47.6 (7.5) | 46.5 (7.9) | 41.0 (6.0) |
| Diagnostic criteria | Referred as diagnosed with HIVDSN | Referred as diagnosed with HIVDSN | Symmetrical numbness, paraesthesia, or burning, pain ‘now’ score of 4 or greater on BPI 0–10 |
| Duration | 15 weeks | 6 weeks | 45 min |
| Design | RCT Parallel design | RCT Parallel design | RCT Parallel design |
| Participants randomized (completed) | 50 (50) | 61 (33) | 40 (40) |
| Reference | Anastasi 2013 et al. [32] | Evans et al. 2003 [31] | Paice et al. 2000a [28] |
| Adverse events | 35% of patients stopped drug treatment |
| Data | GPS mean change (14 weeks): SAR (n = 105 −0.29. control (n = 82), −0.19, mean difference −0.08 (CI: −0.21 to 0.06), p = 0.26 Amitriptyline (n = 49) −0.26, placebo (n = 52) −30, mean difference 0.00 (CI −0.18–0.19) p = 0.99 |
| Outcome measures | Primary: Change in GPS between baseline and end of 14 weeks. Secondary: A neurologic summary score, 39-item, qual-ity-of-life assessment tool. |
| Intervention | SAR or control points twice weekly during a 6-week induction phase, followed by weekly treatment during an 8-week maintenance phase. For the amitriptyline comparison, the patients,14-week course of either amitriptyline or placebo capsules 25–75 mg daily |
| ARV therapy | Antiretroviral therapy was allowed |
| Sex F/M | SAR:15/106 Control: 10/108 Amitriptyline 5/66 Placebo 8/57 |
| Age | Mean (SD): SAR 40.9 (6.8) Control points 41.7 (8.3) Amitriptyline 40.1 (7.1) Placebo 39.9 (5.9) |
| Diagnostic criteria | HIV-related lower extremity peripheral neuropathy, diagnosed by a physician based on history and clinical examination |
| Duration | 14 weeks |
| Design | 2 × 2 factorial design plus 2 groups active-placebo parallel design |
| Participants randomized (completed) | Factorial Option N = 125 Acupuncture Option N = 114 Amitriptyline Option N = 11 |
| Reference | Shlay et al. 1998 [33] |
| Adverse events | Discontinuation due to AEs: Pregabalin dizziness (4 subjects), somnolence (2 subjects), confusion state (2 subjects), disorientation (2 subjects). Placebo hypoesthesia (1 subject), bladder pain (1 subject), nausea and vomiting (1 subject), pain (1 subject) | Total AE: Pregabalin = 323, Placebo = 255 Serious AE: Pregabalin = 7, Placebo = 7 Severe AE: Pregabalin = 11, Placebo = 8 Incidence of any AE: Dizziness, Pregabalin = 25 Placebo = 10, Headache Pregabalin = 25, Placebo = 26, Somnolence, Pregabalin = 13, Placebo = 4 |
| Data | Pregabalin: −2.88, Placebo: −2.63 (difference −0.25, p = 0.3914) 50% responder rate: Pregabalin 38.9%, Placebo 42.8% (p = 0.50) 30% responder rate: Pregabalin 56.3%, Placebo 55.9% (p = 0.90) | Primary: Change from baseline in LS mean (SE) NRS pain score, Pregabalin: −2.04 (0.15), Placebo: −2.11 (0.15), MD = 0.07 [95% CI = −0.30 to 0.45], p = 0.709. Number of patients with >30% response: Pregabalin: 88/183 (48.1%), Placebo: 98/192 (51.0%) OR = 0.84, [95% CI = 0.52 to 1.36], p = 0.490 |
| Outcome measures | Primary: Pain reduction, NRS 0−10. Number of patients with >30% and 50% pain reduction. Secondary: Anxiety, Depression, PGIC | Primary: Pain reduction, NRS 0−10. Number of patients with >30% pain reduction Secondary: PGIC/CGIC, BPI-sf, NPSI. NRS-Sleep scale, MOS Daytime activity and sleep parameters. WPAI-SHP, and SF-36, Hospital Anxiety and Depression Scale HADS |
| Intervention | Pregabalin started at 150 mg/daily, titrated up to 600 mg daily at 2 weeks, stable for next 12 weeks | Pregabalin starting at 150/day, titrated up to 600 mg/day (tolerance and efficacy), during 4 weeks titration period, then maintenance doses for 12 weeks follow up period |
| ARV therapy | Stable doses for >3 months before entry | Stable ARV treatment >8 weeks before the study |
| Sex F/M | 57/245 | Pregabalin: 121/62 Placebo 116/76 |
| Age | Mean (SD) Placebo: 46.8 (7.5) Pregabalin: 48.2 (8.1) | Mean (SD) Pregabalin: 41.2 (9.0) Placebo: 42.3 (8.4) |
| Diagnostic criteria | clinical | 2 of the 3 following signs: reduced or absent Achilles tendon reflexes, superficial and vibratory sensation in the lower extremities, daily pain (>40 mm on the VAS [range 0–100] scale |
| Duration | 14 weeks | 16 weeks |
| Design | Randomized parallel group | Randomized parallel group |
| Participants randomized (completed) | 302 (299) | 377 (375) |
| Reference | Simpson et al. 2010 [34] | Simpson et al. 2014 [35] |
| Adverse events | Cannabis: Severe dizziness: 1 episode Anxiety: 1 episode Placebo: Anxiety: 1 episode. Confusion, dizziness, nausea significantly more frequent in cannabis group (p < 0.01). No withdrawals due to adverse events | Greater frequency of concentration difficulties, fatigue, sleepiness or sedation, increased duration of sleep, reduced salivation, and thirst in cannabis week than placebo week |
| Data | Primary outcome 1. >30% pain change Cannabis, 13/25 patients, placebo: 6/25 patients (52% vs. 24%, difference 28%, 95% CI 2%–54%, 2. Median change in pain (VAS): Cannabis −34% (IQR −71, −16) placebo −17% (IQR −29, +8) dif 18%, p = 0.03. Secondary: Painful area brush and von Frey hair stimuli: Cannabis median −34%, −52% vs. Placebo −11%, +3% respectively p = 0.05 | Primary: Median difference in pain reduction = 3.3 favouring cannabis, Effect size = 0.60, p = 0.020 (ITT). First week: DDS Median change: cannabis −4.1, placebo +0.1 p = 0.029. Proportion of patients with >30 DDS pain reduction: cannabis week 0.46 (95%CI 0.28,0.65), placebo week 0.18 (0.03, 0.32), p = 0.043 VAS median change (range) Cannabis −17 (−58, 52) placebo −4 (−56, 28), (p < 0.001) |
| Outcome measures | Primary: 1. Proportion of patients with >30% reduction in pain from baseline to end of treatment 2. The percent change in pain from baseline (VAS) Secondary: 1. Percent change after 1st and last cigarette in pain, and secondary hyperalgesia 2. Change in total mood disturbance (Profile of Mood States) | Primary: 1. Change in self-reported pain magnitude assessed by the DDS (0- to 20-point scale). 2. Change in VAS scale (0–10) Secondary: Disability, mood, and quality of life (Sickness Impact Profile (SIP), Profile of Mood States (POMS) the Brief Symptom Inventory (BSI) |
| Intervention | Cannabis cigarettes smoking (3.56% delta-9-THC) or placebo cannabis cigarettes (0% delta-9-THC), 3 times daily for 5 consecutive days | 4 smoking sessions/day for 5 consecutive days with active (Δ-9 ΤHC 1–8%, titrated to effect) or matching placebo cigarettes, 2 weeks washout followed by another 4 smoking sessions/day for another 5 days (placebo or active) |
| ARV therapy | Stable regimen for at least 8 weeks prior to randomization: Cannabis: 18/27 Placebo: 26/28 | Prescribed: 93% Exposed to potentially neurotoxic dideoxy- nucleoside reverse transcriptase inhibitors: 72% |
| Sex F/M | Cannabis 5/22 Placebo 2/26 | 0/34 |
| Age | Mean (SD) Cannabis 50 (6) Placebo: 47 (7) | 48.8 (6.8) |
| Diagnostic criteria | Symmetric distal pain or dysesthesias > 2 weeks, absent or depressed ankle reflexes, or pin, vibration, touch, temperature sensory loss | Reduced distal tendon reflexes, distal sensory loss or electro-physiological abnormalities (distal leg sensory nerve conduction studies), plus symptoms of pain and paraesthesias |
| Duration | 5 days | 5 days, 2 weeks washout cross over to another 5 days |
| Design | Randomized parallel group | Single group, double-blind, placebo-controlled crossover |
| Participants randomized (completed) | 55 (50) | 34 (28) |
| Reference | Abrams et al. 2007 [36] | Ellis et al. 2009 [37] |
| Adverse events | NGX-4010: 161/225 control: 45/82 Dropouts due to adverse events: NGX-4010, n = 2; control, n = 1. | % of patients with >1 AE: 93% NGX-4010, 83% control group. | Drop out: Capsaicin cream n = 5 (burning) |
| Data | NRPS scores from baseline to week 12, Mean (SD): NGX 4080 −22.8% (30.6), control −10.7% (30.8), p = 0.0026 >30% change in pain: NGX 4080 76/225, control 15/82 | Change from baseline to weeks 2–12, mean (SE): NGX 4010 −1.8 (0.1) Control, −1.4 (0.2), p > 0.05. >30% pain reduction: NGX-4010 43/332, control 36/162 p > 0.05 | BPI at study endpoint Mean (SD); capsaicin 5.50 (2.68) Control 3.10 (2.12), p = 0.042 |
| Outcome measures | Primary: % change in the pain NPRS score, from baseline to weeks 2 to 12. Secondary: Change from baseline pain for weeks 2–4 and 2–8; proportion of patients with a >30% mean decrease “average pain; percent change from baseline in the “worst pain for the past 24 h” and “pain now”. Change from baseline to week 12 assessed with GPS sf McGill, BPI, PGIC and CGIC | Primary: percent change in NPRS scores from baseline during weeks 2–12, patients with a >30% average pain reduction, the percentage of patients improved on PGIC and CGIC, changes from screening in sfMcGill Pain Questionnaire and SF-36v2 | Change in BPI, Quality of Life Index (QLI), Profile of Mood States (POMS), Sickness Impact Profile (SIP) |
| Intervention | NGX-4010 (capsaicin 640 mcg/cm2, 8% w/w) Patch or control patch (patch (3.2 mcg/cm2, 0.04% w/w) applied for 30, 60, or 90 min, up to 4 patches each | NGX-4010 (capsaicin 640 mg/cm2, 8% w/w; or control capsaicin (3.2 mg/cm2, 0.04% w/w) patch, for 30 or 60 min to both feet (up to 1120 cm2) | Topical capsaicin (0.075%) plus usual therapy, or placebo plus usual therapy, 4 times daily for 4 weeks |
| ARV therapy | No ART or on stable doses for >8 weeks | Exposure NGX-4010: 25/332, control: 8/162 | No use of didenine or didectosine |
| Sex F/M | NGX 4010: 18/207 Control 3/79 | NGX 4010: 42/332 Control 20/162 | 1/25 |
| Age | Mean (SD): NGX-4010 47.7 (8.4) Control 48.4 (7.6) | Mean (SD) NGX-4010 49.7 (8.5) Control 49.7 (8.7) | Mean (SD): 40.3 (6.0) |
| Diagnostic criteria | Pain, burning, dysesthetic discomfort in both feet, diminished ankle reflexes, and diminution of vibration, pain, or temperature sensation in the distal legs | Diagnosed with HIV-DSP for >2 months and an average baseline numeric pain rating scale (NPRS) score of 3–9 | Diagnosed HIV-related DSPN |
| Duration | 12 weeks | 12 weeks | 4 weeks |
| Design | Randomized-controlled parallel group | Randomized-controlled parallel group | Randomized-controlled parallel group |
| Participants randomized (completed) | 307 (274 completed, 302 analysed) | 494(234) | 26 (14) |
| Reference | Simpson et al., 2008 [39] | Clifford et al., 2012 [38] | Paice 2000b |
| Adverse events | Drop out: Lamotrigine, rash n = 5, gastrointestinal infection n = 1 | Rash: Lamotrigine 21/150 Control 9/77 Infection 17/150, control 7/77, Nausea: Lamotrigine 17/150, control 8/77 Diarrhea Lamotrigine: 16/150, control 7/77 Headache: Lamotrigine 16/150, control 8/77 |
| Data | Mean difference (SE) pain scores between baseline and week 14: Lamotrigine −0.55 (0.14), control −0.18 (0.09), p = 0.03. No difference in global pain score (p = 0.37), worst pain score (p = 0.17), or change in use of concomitant analgesics (p = 0.99) at week 14 between the two groups | Neurotoxic striatum, mean change: Lamotrigine: −0.03, control −0.007, p < 0.05 Non neurotoxic striatum, mean change: Lamotrigine −0.022, control −0.0025, p > 0.05 |
| Outcome measures | Primary: Pain reduction measured by GPS. Safety and Tolerability Secondary: The slope of change of weekly mean pain scores over course of trial. Patient-rated global pain relief, change in worst pain, use of concomitant analgesic medications | Primary efficacy measure: the mean change in average pain (GPS up to the maintenance phase (PP analysis) Secondary efficacy endpoints: analysis of slope of weekly average GPS, the mean change in pain (VAS, McGill Pain Questionnaire), the percentage of patients with >30% VAS change |
| Intervention | Lamotrigine or patching placebo titrated up to 150 mg × 2 up to 7 weeks, then stable for 7 more weeks | Lamotrigine or matching placebo titrated up to 600 mg daily for 7 weeks, then stable dose for 4 weeks |
| ARV therapy | No neurotoxic antiretroviral therapy for >8 weeks before randomization or a history of a stable dose for at least 8 weeks before randomization | No prior exposure to ddX ART, stop them >8 weeks or at stable dose for >8 weeks before randomization. |
| Sex F/M | Lamotrigine: 1/8. Control 4/16 (completers) | Lamotrigine 15/150 Control 11/77 |
| Age | Lamotrigine 44.6 (8.4) Control 44.4 (10.6) (completers) | Mean (range) Neurotoxic stratum: Lamotrigine 44 (32–65), placebo 42 (29–67) No neurotoxic striatum: Lamotrigine45 (26–63), placebo 46 (33–64) |
| Diagnostic criteria | Symptoms of burning or dysesthetic pain in both feet for at least 2 weeks, rated on the GPS as at least “mild” all of the time or moderate” for a total of at least 2 hours a day, and either absent or diminished ankle reflexes or distal diminution of either vibration sensation or pain and temperature sensation | Symptoms of neuropathic pain in both distal lower extremities plus either diminished reflexes at the ankles distal diminution of sensations of vibration, pain, or temperature in the legs. |
| Duration | 14 weeks | 12 weeks |
| Design | Randomized parallel group | Randomized parallel group |
| Participants randomized (completed) | 42 (28) | 227 (172) |
| Reference | [40] and [41] | Simpson et al. 2003 |
| Adverse events | Dry mouth: Amitript = 9, placebo n = 1; Drowsiness: Amitriptyline n = 7, placebo n = 1; Chest pain: Placebo n = 1 | Amitriptyline (sedation n = 10, confusion n = 1, less common events n = 4), Mexiletine (nausea and vomiting n = 10, urinary retention n = 3, dizziness n = 1, other n = 8) Placebo (confusion n = 21, urinary retention n = 1, other n = 3) | Drug stop: Mexiletine, 1 rush, 2 gastrointestinal side effects. 1, ECG changes |
| Data | Primary: ARV users: amitriptyline: −2.7, SD −3.3; placebo: −2.1, SD −2.8; t(60) = −1.13, p = 0.26 ARV naïve: amitriptyline: −2.8, SD −3.3; placebo: −2.8, SD −3.4; t(60) = 0.05, p = 0.96 | Amitriptyline group (n = 39): Mean −0.31 (SD 0.31). Mexiletine group (n = 44): Mean −0.23 (SD 0.41). Placebo group (n = 43): −0.20 (SD 0.30), p = 0.38. The mean reduction in pain intensity with Amitriptyline, relative to placebo: −0.11 | Mean pain scores (SD): First Mexiletine 30.8 (16.1), then placebo: 34.0 (29.6) p = 0.78. First placebo 54.2 (19.5) then Mexiletine 45.7 (27.3), p = 0.45 |
| Outcome measures | Per protocol analysis Primary: Likert [0–10]: Difference in pain intensity between baseline and at six weeks. Secondary: Dose escalation and maximum dosage of amitriptyline Side effects and adverse events. The use of rescue medication | Primary: GPS [0–1.77]: Change in mean pain intensity from baseline to week 8. Safety: clinical adverse events, and laboratory test abnormalities, dosage modification caused by adverse events Secondary: Changes in mood, quality of life, requirement for additional analgesic agents | Primary: Pain reduction, VAS 0–100 Secondary: adverse events |
| Intervention | Amitriptyline vs. placebo (6 weeks, median dose = 50 mg) | Amitriptyline + placebo Mexiletine, placebo Amitriptyline + Mexiletine, placebo Amitriptyline + placebo Mexiletine. 4 weeks titration, 4 weeks stable dose, up to 600 mg Mexiletine and 100 mg Amitriptyline | Mexiletine up to 600 mg/day vs. placebo for 6 weeks, 1 week washout then Placebo vs. Mexiletine |
| ARV therapy | Stable therapy for>6 months (ARV user group), or therapy naïve (ARV-naïve group). ARV-naïve (n = 61) ARV-user (n = 61) | Current use: n = 49, Discontinued 8-26 weeks prior to study: n = 35, Never used/discontinued > 26 weeks prior to study: n = 61 | No early use of ddI, ddC within one year |
| Sex F/M | 87/35 | 6/139 | 2/20 |
| Age | Mean (SD) 38 (8.9) | Median: Amitriptyline39 Mexiletine 40 | Mean:35 |
| Diagnostic criteria | Brief Peripheral Neuropathy Screening Tool | Symmetrical pain, burning or tingling at least mild all the time or moderate for >2 h/day and diminished ankle reflexes or distal diminution of vibratory sense or diminished pain and temperature sensation | Pain >4/10 in VAS, decrease in pinprick or vibratory sense, decrease or absent ankle jerks |
| Duration | 15 weeks | 8 weeks | 6 weeks, one week washout then another 6 weeks |
| Design | Randomized cross-over | Randomized parallel | Randomized cross-over |
| Participants randomized (completed) | 124 (122) | 145 (126) | 22 (19) |
| Reference | Dinat et al., 2015 [43] | Kieburtz et al., 1998 [44] | Kemper et al., 1998 [45] |
| Adverse events | GBP-group: 80% patients dizziness and significantly more frequent than placebo patients p < 0.05. Dizziness, gait ataxia and nausea were more frequent in the GBP-group, but not statistically significant compared with placebo patients | Side effects: 22 patients low dose NGF. 56 patients NGF, 25 patients placebo group. Most frequent injection site pain or myalgias on all groups |
| Data | GBP: median baseline week VAS = 5.1, median 4th week VAS = 2.85, −44.1%, p < 0.05 Placebo: median baseline week VAS = 4.7, median 4th week VAS = 3.3, −29.8%, p = 0.646). Comparison of the changes between GBP and placebo-group: no significant differences for the pain or the sleep interference score. | The mean adjusted change: Placebo, −0.06 [range −0.14 to +0.01 log units] 0.1 μg/kg rhNGF: 0.18 (−0.25 to −0.1 log units] 0.3 μg/kg rhNGF: 0.21 [−0.29 to −0.14log units] |
| Outcome measures | Primary outcome: Pain change (10-cm VAS of SF-MPQ). Primary endpoint: Difference in weekly median pain score between the 4th week and the baseline week. Secondary: median sleep interference score, measured by VAS (0 = excellent sleep, 10 cm = no sleep) | Primary endpoint: Change in pain intensity (GPS) from baseline to week 18. Secondary: Global assessments of neuropathic pain |
| Intervention | Gabapentin dosage and matching placebo titrated over 2 weeks up to 1200 mg/d. In the case of sufficient, effect the dosage was increased up to 2400 mg/d over further 2 weeks | 0.1 mg/kg rhNGF s.c. 2 times/week, 0.3 mg/kg rhNGF s.c. 2 times/week, placebo s.c. 2 times/week |
| ARV therapy | 7 patients with concomitant antiretroviral treatment of d4T and/or ddI (GBP n = 4; placebo n = 3) and 3 patients, who had had neurotoxic antiretroviral drugs (d4T and/or ddI) in the period of 3 months before he study (GBP n = 2; placebo n = 1) | Subjects stratified regarding ddI, ddC, or d4T use: current use, use stopped 8–26 weeks before randomization stopped >26 weeks before randomization, never used |
| Sex F/M | 6/20 | 8/262 |
| Age | Median (range) GBP: 46 (27–59) Placebo: 44 (35–61) | Mean (SD): 44.0 (8.7) |
| Diagnostic criteria | Based on history, clinical and neurophysiological examination (paraesthesia, dysesthesia or pain), abnormal sensory signs (elevated vibratory threshold or pin hyperalgesia), decreased or absent ankle reflexes. | Clinical, based on criteria set by the American Academy of Neurology |
| Duration | 4 weeks | 18 weeks |
| Design | Randomized, double blind, parallel group | Randomized, double blind, parallel group |
| Participants randomized (completed) | 26 (24) | 270 (235) |
| Reference | Hahn et al. 2004 [46] | McArthur et al., 2002 [47] |
| Adverse events | 23 patients with 1 or more AE; ALCAR n = 1 (20.9%) Placebo: n = 14 (29.8%) Events related to study medication ALCAR group: paraesthesia, 1 subject; pain, anorexia, dry mouth and neuropathy, 1 patient. Placebo group:4 patients diarrhoea, nausea, pruritus and rash) | Lidocaine gel: local rash, blisters, and dryness, n = 3 |
| Data | Primary: VAS reduction Mean (SD) ALCAR–1.32 (1.84) Placebo–0.61 (1.55), p = 0.07 2. Secondary: TSS change Mean (SD): ALCAR -1.32 (2.45) Placebo −0.88 (1.90), p = 0.19 Proportion of patients with >30% improvement in TSS: 30.2% Placebo: 18.2%, p = 0.21 | Primary outome: Pain scores at end of phase A: Mean (SD) Lidocaine 1.09 (0.24) Placebo 1.15 (0.32), difference at end of Phase A: Lidocaine 0.03 (0.23), placebo 0.08 (0.16), p = 0.314 Pain scores at end of phase B: Mean (SD) Lidocaine 1.16 (0.33) Placebo 1.10 (0.32), difference at end of Phase B: Lidocaine 0.11 (0.23), placebo 0.00 (0.13), p = 0.744 |
| Outcome measures | Primary: Pain change (VAS) between baseline and 14 days. Secondary: Total Symptom Score (TSS), (CGI-C), MPQ, need for rescue analgesics | Primary outcome: Difference in GPS pain scores during the 2nd week of each period. Secondary analyses:(1) differential response of first treatment, (2) global pain relief (3) effect of exposure to nucleoside analogue on the response to lidocaine gel |
| Intervention | ALCAR 1000 mg/day or placebo i.m., 2 times/day for 14 days | Active gel (5% lidocaine gel) or vehicle placebo gel, applied once daily for 2 weeks. They were then crossed over to the second 2-week treatment period on the alternate drug |
| ARV therapy | Stable ATN (onset within 6–12 months of commencing NRTI therapy, symptoms stable for 42 months, and no other neuropathic aetiological factors or DSP-associated therapies) | Current stable use: 21 not used for the previous 8 weeks: 41 |
| Sex F/M | 18/72 | No data |
| Age | 44.4 (9.8) | 45 |
| Diagnostic criteria | Electrophysiological diagnosis | Presence of pain or paraesthesias in both feet for at least 2 weeks, rated on the GPS as at least mild all the time or moderate for a > 2 h/day and diminished or absent ankle reflexes, or pain, temperature, or vibration sensation in the legs |
| Duration | 14 days | 6 weeks: 2 weeks Phase A, 2 weeks washout, 2 weeks Phase B |
| Design | Randomized controlled parallel group | Randomized controlled cross-over study |
| Participants randomized (completed) | 90 (87) | 64 (56) |
| Reference | Youle et al. 2007 [48] | Estanislao et al. 2004 [49] |
| Adverse events | No differences between groups. One patient in placebo group: mild epistaxis | PRO: 4 AE (cellulitis, altered mental status, higella enteritis, pancreatitis) PBO: 1 AE (Kaposi sarcoma) |
| Data | Primary (PP analysis): Pain score differences between baseline and week 12, Mean (SD): Peptide T: −0.24 (0.45) Placebo: −0.39 (0.54), p = 0.3 | GPS changes mean (SD): PRO 2 mg/day −0.12(0.23) PRO 4 mg/day −0.24(0.35) PRO 8 mg/day −0.15(0.32) PRO 16mg/day −0.18(0.34) PBO −0.18(0.32), p.0.05 between all comparisons |
| Outcome measures | Primary: Reduction in pain severity (GPS) at week 12 Secondary: were neurologic examination, nerve conduction studies, global evaluation, electrophysiologic measurements, cognitive function and immunological function | Primary efficacy endpoint: change from baseline to 6 week endpoint GPS weekly average. Secondary endpoints: defined as >0.35 units of pain improvement from baseline on the GPS, change in HIV viral load |
| Intervention | Peptide T 6mg intranasally/ day or placebo intranasally for 12 weeks | 2, 4, 8, or 16 mg/d PRO or PBO administered via S.C. injection for 6 weeks |
| ARV therapy | No use of use of zidovudine (ZDV, AZT) for less than three months before entry, no use of didanosine (ddI) and/or zalcitabine (ddC) within eight weeks of entry Current use of Zidovudine: Peptide T, n = 28 Placebo, n = 35 | Stable use or non-use of dideoxynucleoside reverse transcriptase inhibitors for >4 months. ddC, d4T, or ddI use at Entry: 52/229 |
| Sex F/M | Peptide T:38/2 Placebo 39/2 | 19/210 |
| Age | Median: Peptide T = 40.4 Placebo = 40.9 | Median, Q1, Q3: 47,43,53 |
| Diagnostic criteria | (1) Distal pain, paraesthesia, or numbness, of the lower extremities. (2) Neurologic signs, (reduction in pain, temperature, touch, or vibratory sensation in a stocking and glove distribution; absent or reduced ankle reflexes. (3) Electrophysiologic signs of generalized, distal, sensory and motor, axonal polyneuropathy | Clinical criteria developed by the American Academy of Neurology (1991) |
| Duration | 12 weeks | 6 weeks |
| Design | Randomized, placebo-controlled, parallel design study | Randomized, placebo-controlled, 4 arm parallel design study |
| Participants randomized (completed) | 81 (75) | 237 (196) |
| Reference | Simpson et al. 1996 [50] | Evans et al. 2007 [51] |
| Adverse events | No differences between groups | Adverse events: Duloxetine, n = 5 Methadone, n = 17 Conbination, n = 17 Placebo, n = 6 Severe adverse events: Duloxetine nausea (n = 1), vomiting (n = 1), renal dysfunction (n = 1). Severe adverse events on placebo: pain (n = 1), fatigue (n = 1). |
| Data | Primary, Pain change Mean (SD) Memantine = −1.82 (2.77) Placebo = −2.36 (3.35), p = 0.87 Change of the paresthesia score, mean (SD): Memantine = −0.91 (3.58) Placebo = −1.14 (3.35), p = 0.92 | Primary: 4th week pain scores (median Q1, Q3) A. Dul/Placebo:7 (4, 8) B. Placebo/Placebo: 6 (4, 8) C. Placebo/Meth: 6.5 (5, 8) D. Dul/Meth: 5.5 (4, 7). Comparisons A vs. B, p = 1, C vs. B, p = 1, D vs. B, p = 0.25, D vs. A, p = 0.11, D vs. C, p = 0.06 |
| Outcome measures | Primary: change in pain and paraesthesia indices on a 01–10 scale, from baseline to week 16, between memantine and placebo arms. | Primary outcome measure: mean 24 h pain intensity (MPI) measured on 0–10 NRS. Secondary Outcome: night-time pain intensity |
| Intervention | Memantine starting at 10 mg/day, titrated up to 40 mg in 4 weeks (or up to the maximum tolerated dose, stable up to week 16. | Patient assigned to one of 4 to one of four treatment sequences, including Duloxetine, Methadone, Duloxetine-Methadone or placebo, 4 weeks each with one week washout. Duloxetine/matching placebo titrated to 60mg. Methadone/matching placebo titrated to 10 mg t.i.d. |
| ARV therapy | Memantine: 2/24 Placebo 20/21 | Stable use or non-use of antiretrovirals for 30 days prior to entry |
| Sex F/M | Memantine2/22 Placebo: 4/17 | 2/13 |
| Age | Median (min, max): Memantine group: 44 (33, 63) Placebo group: 46 (31, 59) | 13/15 over 50 years |
| Diagnostic criteria | Presence of symmetric loss or reduction of vibratory, pinprick, or temperature sensation in a stocking and glove distribution and predominantly symmetric pain or paraesthesia | Presence of symmetrical pain, burning, or dysesthesias in a stocking distribution for at least 6 months with abnormal ankle reflexes or at least one abnormal sensory sign (elevated vibratory thresholds, stocking loss of pinprick or temperature, or cutaneous allodynia) |
| Duration | 16 weeks | 20 weeks |
| Design | Randomized, double blind, placebo-controlled, parallel study | Randomized, double blind, placebo-controlled, four-period crossover study |
| Participants randomized (completed) | 45 | 15 (8) |
| Reference | Shiffito et al. 2006 [52] | Harrison et al. 2013 [53] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaniti, A.; Sardeli, C.; Fyntanidou, V.; Papakonstantinou, P.; Dalakakis, I.; Mylonas, A.; Sapalidis, K.; Kosmidis, C.; Katsaounis, A.; Giannakidis, D.; et al. Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis. Medicina 2019, 55, 762. https://doi.org/10.3390/medicina55120762
Amaniti A, Sardeli C, Fyntanidou V, Papakonstantinou P, Dalakakis I, Mylonas A, Sapalidis K, Kosmidis C, Katsaounis A, Giannakidis D, et al. Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis. Medicina. 2019; 55(12):762. https://doi.org/10.3390/medicina55120762
Chicago/Turabian StyleAmaniti, Aikaterini, Chrysanthi Sardeli, Varvara Fyntanidou, Panagiota Papakonstantinou, Ioannis Dalakakis, Antonios Mylonas, Konstantinos Sapalidis, Christoforos Kosmidis, Athanasios Katsaounis, Dimitrios Giannakidis, and et al. 2019. "Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis" Medicina 55, no. 12: 762. https://doi.org/10.3390/medicina55120762