
Evaluation of the Efficacy of Immune and Inflammatory Markers in the Diagnosis of Lacrimal-Gland Benign Lymphoepithelial Lesion
 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schneider, M.; Rizzardi, C. Lymphoepithelial Carcinoma of the Parotid Glands and Its Relationship with Benign Lymphoepithelial Lesions. Arch. Pathol. Lab. Med. 2008, 132, 278–282. [Google Scholar] [CrossRef]
- Chowdhury, Z.; Raphael, V.; Khonglah, Y.; Mishra, J.; Marbaniang, E.; Dey, B. Mélange of Lymphoepithelial Lesions of Salivary Glands from a Tertiary Care Center of North East India: Diagnostic Conundrums. J. Lab. Physicians 2021, 13, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, R.; Sun, M.; Wang, J.; Wang, N.; Zhang, X.; Ge, X.; Ma, J. The FcεRI signaling pathway is involved in the pathogenesis of lacrimal gland benign lymphoepithelial lesions as shown by transcriptomic analysis. Sci. Rep. 2021, 11, 21853. [Google Scholar] [CrossRef] [PubMed]
- Adzavon, Y.M.; Zhao, P.; Ma, J.; Zhang, X.; Zhang, X.; Zhang, M.; Liu, M.; Wang, L.; Chen, D.; Abisso, T.G.; et al. Macrophage migration inhibitory factor contributes to the pathogenesis of benign lymphoepithelial lesion of the lacrimal gland. Cell Commun. Signal. 2018, 16, 70. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, M.; Takahashi, H.; Ohara, M.; Suzuki, C.; Naishiro, Y.; Yamamoto, H.; Shinomura, Y.; Imai, K. A new conceptualization for Mikulicz’s disease as a systemic IgG4-Related disease. Mod. Rheumatol. 2006, 16, 335–340. [Google Scholar] [CrossRef]
- Sweeney, A.R.; Keene, C.D.; Cimino, P.; Chang, S.-H. IgG4-positive Cell Quantification Distinguishes Between Inflammatory and Noninflammatory Diseases of the Orbit. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Pistone, A.; Soyfoo, M. Granulomatosis with Polyangiitis Overlapping with IgG4-Related Disease. Case Rep. Rheumatol. 2022, 2022, 2360060. [Google Scholar] [CrossRef]
- Cruz, A.A.V.; Camacho, M.A.B.; Cunha, B.S.; Alkatan, H.M.; Xavier, N.F. Plasma cell IgG4 positivity in orbital biopsies of non-IgG4-related conditions. Saudi J. Ophthalmol. 2021, 35, 193–197. [Google Scholar] [CrossRef]
- Liu, R.; Wang, J.; Wang, N.; Li, J.; Ge, X.; Zhang, J.; Ma, J. Clinical Features and Prognoses of IgG4-Positive and IgG4-Negative Lacrimal Lymphomas. Front. Oncol. 2021, 11, 622847. [Google Scholar] [CrossRef]
- Li, J.; Ge, X.; Wang, X.; Liu, X.; Ma, J. Complement System in the Pathogenesis of Benign Lymphoepithelial Lesions of the Lacrimal Gland. PLoS ONE 2016, 11, e0148290. [Google Scholar] [CrossRef]
- Hong, J.W.; Kang, S.; Song, M.K.; Ahn, C.J.; Sa, H.S. Clinic serological factors associated with response to steroid treatment and recurrence in patients with IgG4-related ophthalmic disease. Br. J. Ophthalmol. 2018, 102, 1591–1595. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.-K.; Tsai, C.-C.; Kao, S.-C.; Liu, C.J.-L. Immunoglobulin G4-related ophthalmic disease. Taiwan J. Ophthalmol. 2018, 8, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Kubota, T.; Katayama, M.; Nishimura, R.; Moritani, S. Long-term outcomes of ocular adnexal lesions in IgG4-related ophthalmic disease. Br. J. Ophthalmol. 2020, 104, 345–349. [Google Scholar] [CrossRef]
- Goto, H.; Takahira, M.; Azumi, A.; Japanese Study Group for IgG4-Related Ophthalmic Disease. Diagnostic criteria for IgG4-related ophthalmic disease. Jpn. J. Ophthalmol. 2015, 59, 1–7. [Google Scholar] [CrossRef]
- Japanese Study Group of IgG4-related Ophthalmic Disease. A prevalence study of IgG4-related ophthalmic disease in Japan. Jpn. J. Ophthalmol. 2013, 57, 573–579. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, G.; Wang, M.; Tian, Y.; Chen, F.; Chen, B.; Wu, H. Novel Advances in the Study of IgG4-Related Disease in the Eye and Ocular Adnexa. Ophthalmic Res. 2022, 65, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Detiger, S.E.; Paridaens, D.M.; van Hagen, M.M.; Karim, F.M.; van Laar, J.A.M.; Verdijk, R.M.M. Tissue IgG2/IgG4 Ratio as an Additional Tool to Distinguish IgG4-Related Disease From Other Fibroinflammatory Disorders. Appl. Immunohistochem. Mol. Morphol. 2022, 30, 517–525. [Google Scholar] [CrossRef]
- Chan, A.S.Y.; Mudhar, H.; Shen, S.Y.; Lang, S.S.; Fernando, M.; Hilmy, M.H.; Guppy, N.J.; Rennie, I.; Dunkley, L.; Al Jajeh, I. Serum IgG2 and tissue IgG2 plasma cell elevation in orbital IgG4-related disease (IgG4-RD): Potential use in IgG4-RD assessment. Br. J. Ophthalmol. 2017, 101, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Arora, K.; Rivera, M.; Ting, D.; Deshpande, V. The histological diagnosis of IgG4-related disease on small biopsies: Challenges and pitfalls. Histopathology 2019, 74, 688–698. [Google Scholar] [CrossRef]
- Jia, C.; Tan, Y.; Zhao, M. The complement system and autoimmune diseases. Chronic Dis. Transl. Med. 2022, 8, 184–190. [Google Scholar] [CrossRef]
- Coss, S.L.; Zhou, D.; Chua, G.T.; Aziz, R.A.; Hoffman, R.P.; Wu, Y.L.; Ardoin, S.P.; Atkinson, J.P.; Yu, C.-Y. The complement system and human autoimmune diseases. J. Autoimmun. 2022, 102979. [Google Scholar] [CrossRef] [PubMed]
- Kawa, S. The Immunobiology of Immunoglobulin G4 and Complement Activation Pathways in IgG4-Related Disease. Curr. Top. Microbiol. Immunol. 2017, 401, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; He, D.; Zhao, L.; Liang, S.; Liang, D.; Xu, F.; Zhang, M.; Zhu, X.; Chen, H.; Xie, H.; et al. Role of complement system in patients with biopsy-proven immunoglobulin G4–related kidney disease. Hum. Pathol. 2018, 81, 220–228. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biochemical Indicators | LGBLEL (n = 90) | Control (n = 30) | t Value | P Value |
|---|---|---|---|---|
| ESR (0–20 mm/h) | 17.34 ± 14.10 | 12.04 ± 6.68 | 2.654 | 0.0093 |
| CRP (0–5 mg/L) | 2.01 ± 2.89 | 1.03 ± 1.26 | 2.462 | 0.0155 |
| ACE (33.3 ± 10.2 U/mL) | 33.36 ± 19.92 | 32.59 ± 40.12 | 0.132 | 0.8953 |
| ASO (0–200 IU/mL) | 97.49 ± 118.50 | 88.17 ± 62.35 | 0.5318 | 0.5962 |
| RF (0–20 IU/mL) | 15.48 ± 28.46 | 5.88 ± 3.84 | 3.0400 | 0.0031 |
| C3 (900–1800 mg/L) | 973.77 ± 255.43 | 1115.49 ± 159.23 | 3.374 | 0.0012 |
| IgM (0.4–2.3 g/L) | 1.35 ± 1.89 | 1.26 ± 0.61 | 0.3793 | 0.7052 |
| IgG (751–1560 mg/dL) | 1588.37 ± 530.49 | 1117.86 ± 233.73 | 6.325 | <0.0001 |
| IgG1 (381–930 mg/dl) | 722.04 ± 293.96 | 631.63 ± 156.42 | 2.139 | 0.035 |
| IgG2 (242–700 mg/dl) | 631.17 ± 241.82 | 468.73 ± 161.64 | 4.114 | <0.0001 |
| IgG3 (22-176 mg/dl) | 59.22 ± 39.41 | 50.27 ± 28.68 | 1.339 | 0.1851 |
| IgG4 (4–87 mg/dl) | 174.64 ± 204.74 | 28.82 ± 23.02 | 6.561 | <0.0001 |
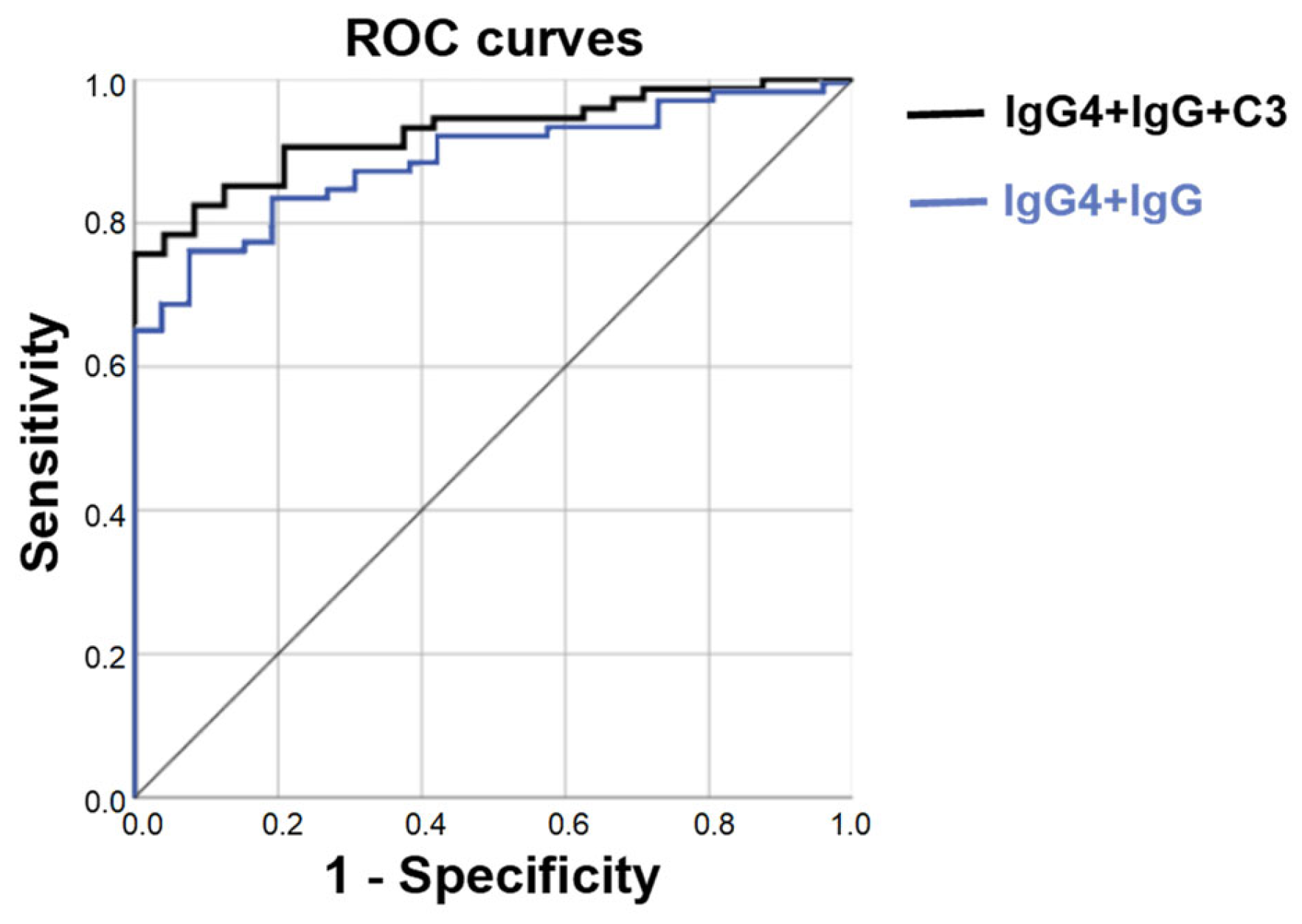
| Indicators | Wald-Value | p Value | Correlation | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| C3 | 4.957 | 0.026 | 0.995 | 0.991 | 0.999 |
| IgG | 7.575 | 0.006 | 1.006 | 1.002 | 1.010 |
| IgG4 | 7.873 | 0.005 | 1.034 | 1.010 | 1.058 |
| Constant | 1.369 | 0.242 | 0.061 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luan, F.; Liu, R.; Li, J.; Ge, X.; Wang, N.; Guo, Q.; Tao, Y.; Ma, J. Evaluation of the Efficacy of Immune and Inflammatory Markers in the Diagnosis of Lacrimal-Gland Benign Lymphoepithelial Lesion. Curr. Issues Mol. Biol. 2023, 45, 2013-2020. https://doi.org/10.3390/cimb45030129
Luan F, Liu R, Li J, Ge X, Wang N, Guo Q, Tao Y, Ma J. Evaluation of the Efficacy of Immune and Inflammatory Markers in the Diagnosis of Lacrimal-Gland Benign Lymphoepithelial Lesion. Current Issues in Molecular Biology. 2023; 45(3):2013-2020. https://doi.org/10.3390/cimb45030129
Chicago/Turabian StyleLuan, Fuxiao, Rui Liu, Jing Li, Xin Ge, Nan Wang, Qihan Guo, Yong Tao, and Jianmin Ma. 2023. "Evaluation of the Efficacy of Immune and Inflammatory Markers in the Diagnosis of Lacrimal-Gland Benign Lymphoepithelial Lesion" Current Issues in Molecular Biology 45, no. 3: 2013-2020. https://doi.org/10.3390/cimb45030129