
T-Cell Receptor Repertoire as a Predictor of Immune-Related Adverse Events in Renal Cell Carcinoma
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. RNA Extraction
2.3. Unbiased Amplification and Sequencing of TCR Genes
2.4. Data Analysis
2.5. Statistical Analysis and Graph Drawing
3. Results
3.1. Patient Characteristics
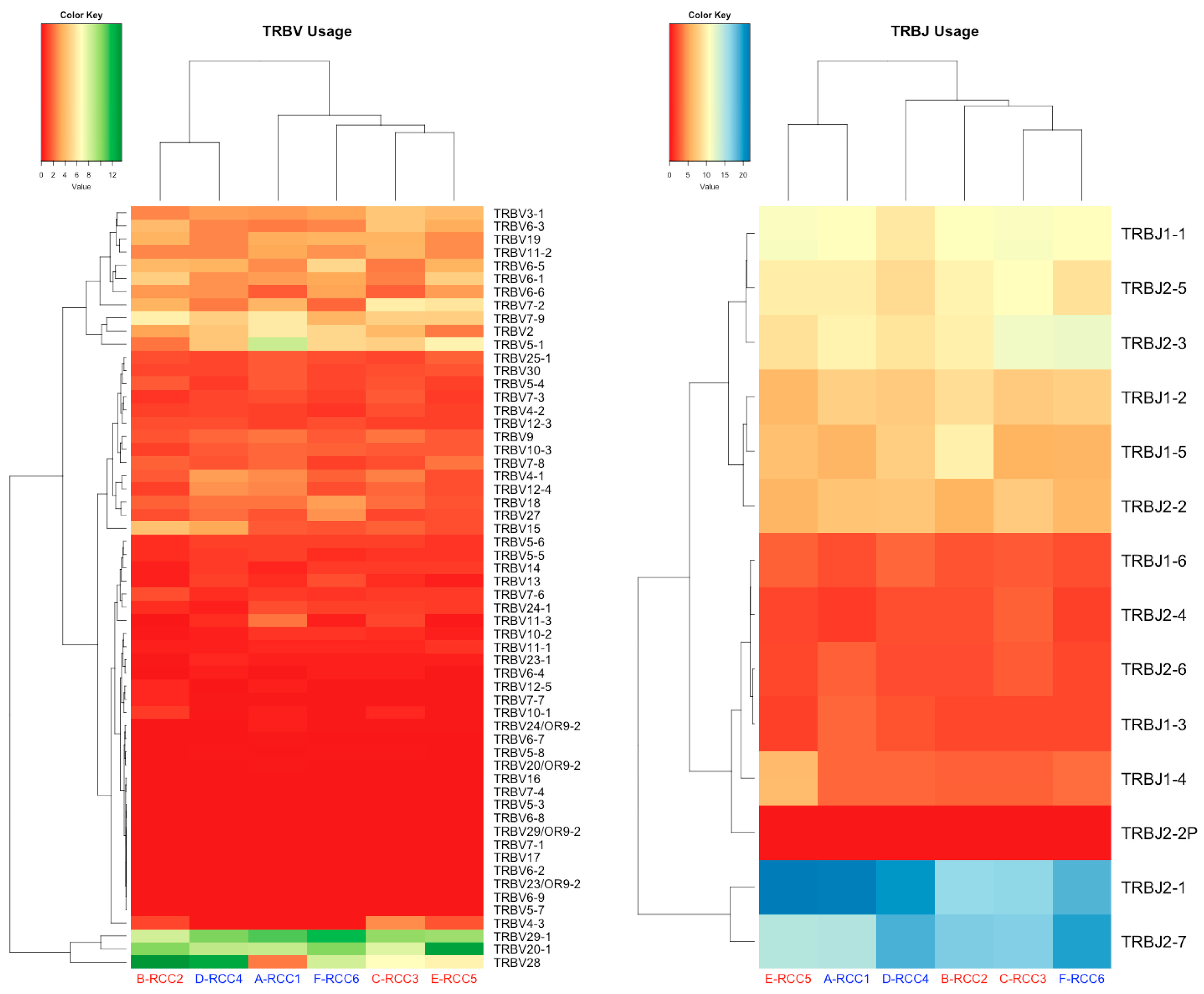
3.2. TCR Profile
3.3. Association between the irAE Grade and TCR Repertoire Diversity
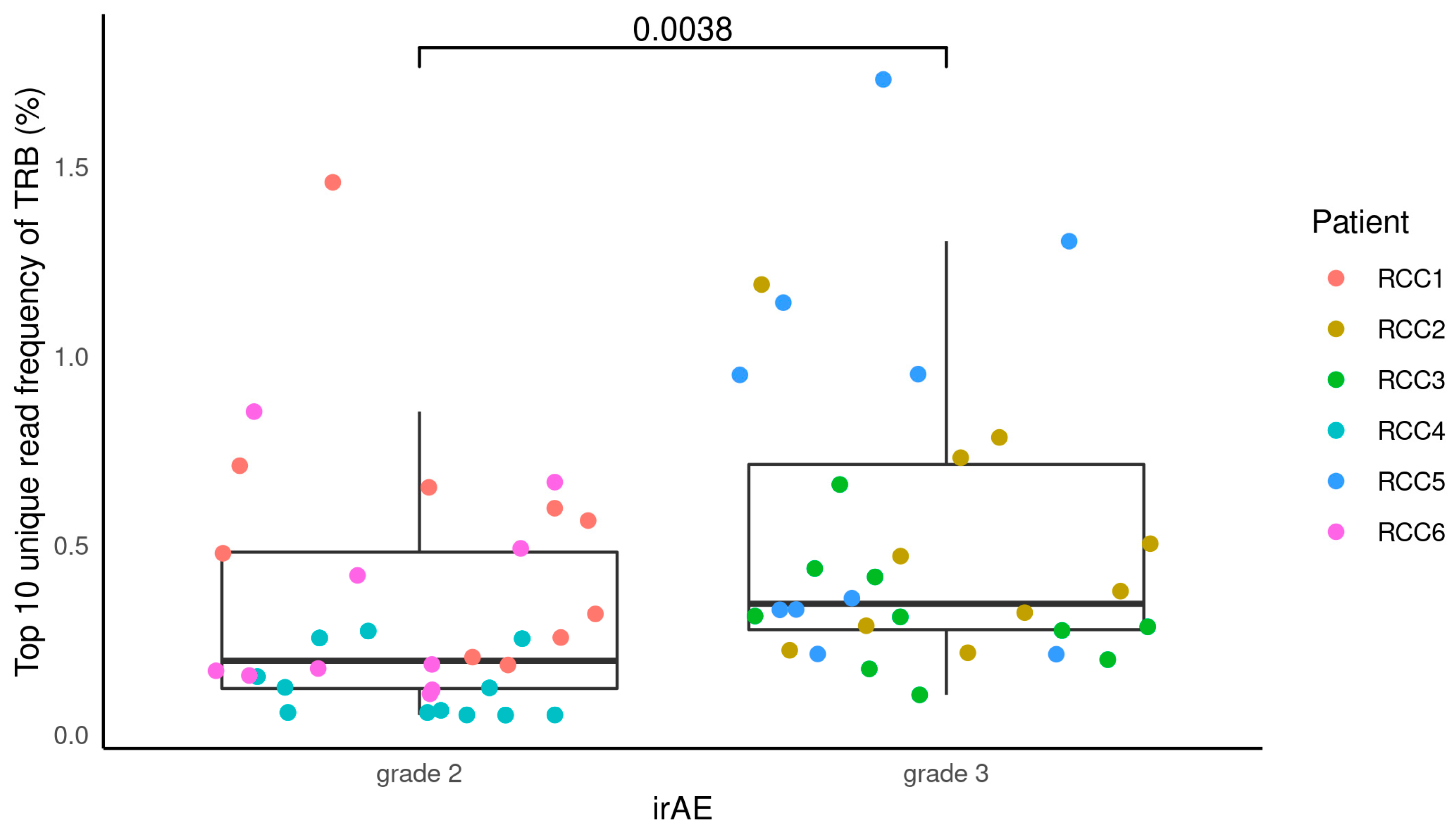
3.4. Association between the irAE Grade and TCR Repertoire Clonality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atkins, M.B.; Tannir, N.M. Current and emerging therapies for first-line treatment of metastatic clear cell renal cell carcinoma. Cancer Treat. Rev. 2018, 70, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef]
- Byun, D.J.; Wolchok, J.D.; Rosenberg, L.M.; Girotra, M. Cancer immunotherapy—Immune checkpoint blockade and associated endocrinopathies. Nat. Rev. Endocrinol. 2017, 13, 195–207. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernandez-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.; Alekseev, B.; Rha, S.Y.; Porta, C.; Eto, M.; Powles, T.; Grunwald, V.; Hutson, T.E.; Kopyltsov, E.; Mendez-Vidal, M.J.; et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N. Engl. J. Med. 2021, 384, 1289–1300. [Google Scholar] [CrossRef]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulieres, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef]
- Motzer, R.J.; Choueiri, T.K.; Powles, T.; Burotto, M.; Bourlon, M.T.; Hsieh, J.J.; Maruzzo, M.; Shah, A.Y.; Suarez, C.; Barrios, C.H.; et al. Nivolumab + cabozantinib (NIVO + CABO) versus sunitinib (SUN) for advanced renal cell carcinoma (aRCC): Outcomes by sarcomatoid histology and updated trial results with extended follow-up of CheckMate 9ER. J. Clin. Oncol. 2021, 39, 308. [Google Scholar] [CrossRef]
- Motzer, R.J.; Rini, B.I.; McDermott, D.F.; Aren Frontera, O.; Hammers, H.J.; Carducci, M.A.; Salman, P.; Escudier, B.; Beuselinck, B.; Amin, A.; et al. Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: Extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1370–1385. [Google Scholar] [CrossRef]
- Zhou, S.; Khanal, S.; Zhang, H. Risk of immune-related adverse events associated with ipilimumab-plus-nivolumab and nivolumab therapy in cancer patients. Ther. Clin. Risk Manag. 2019, 15, 211–221. [Google Scholar] [CrossRef]
- Scaviner, D.; Lefranc, M.P. The human T cell receptor alpha variable (TRAV) genes. Exp. Clin. Immunogenet. 2000, 17, 83–96. [Google Scholar] [CrossRef]
- Folch, G.; Lefranc, M.P. The human T cell receptor beta variable (TRBV) genes. Exp. Clin. Immunogenet. 2000, 17, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.M.; Bjorkman, P.J. T-cell antigen receptor genes and T-cell recognition. Nature 1988, 334, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.M. T cell receptor gene diversity and selection. Annu. Rev. Biochem. 1990, 59, 475–496. [Google Scholar] [CrossRef]
- Kato, T.; Iwasaki, T.; Uemura, M.; Nagahara, A.; Higashihara, H.; Osuga, K.; Ikeda, Y.; Kiyotani, K.; Park, J.H.; Nonomura, N.; et al. Characterization of the cryoablation-induced immune response in kidney cancer patients. Oncoimmunology 2017, 6, e1326441. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Y.; Yang, Q.F.; Yang, J.S.; Cao, R.B.; Liang, J.Y.; Liu, Y.T.; Zeng, Y.L.; Chen, S.; Xia, X.F.; Zhang, K.; et al. Characteristics and prognostic significance of profiling the peripheral blood T-cell receptor repertoire in patients with advanced lung cancer. Int. J. Cancer 2019, 145, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Tomiyama, E.; Koh, Y.; Matsushita, M.; Hayashi, Y.; Nakano, K.; Ishizuya, Y.U.; Wang, C.; Hatano, K.; Kawashima, A.; et al. A Potential Mechanism of Anticancer Immune Response Coincident with Immune-related Adverse Events in Patients with Renal Cell Carcinoma. Anticancer Res. 2020, 40, 4875–4883. [Google Scholar] [CrossRef]
- Kato, T.; Kiyotani, K.; Tomiyama, E.; Koh, Y.; Matsushita, M.; Hayashi, Y.; Nakano, K.; Ishizuya, Y.; Wang, C.; Hatano, K.; et al. Peripheral T cell receptor repertoire features predict durable responses to anti-PD-1 inhibitor monotherapy in advanced renal cell carcinoma. Oncoimmunology 2021, 10, 1862948. [Google Scholar] [CrossRef]
- Kitaura, K.; Shini, T.; Matsutani, T.; Suzuki, R. A new high-throughput sequencing method for determining diversity and similarity of T cell receptor (TCR) alpha and beta repertoires and identifying potential new invariant TCR alpha chains. BMC Immunol. 2016, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Kitaura, K.; Yamashita, H.; Ayabe, H.; Shini, T.; Matsutani, T.; Suzuki, R. Different Somatic Hypermutation Levels among Antibody Subclasses Disclosed by a New Next-Generation Sequencing-Based Antibody Repertoire Analysis. Front. Immunol. 2017, 8, 389. [Google Scholar] [CrossRef] [PubMed]
- Shankar, B.; Zhang, J.; Naqash, A.R.; Forde, P.M.; Feliciano, J.L.; Marrone, K.A.; Ettinger, D.S.; Hann, C.L.; Brahmer, J.R.; Ricciuti, B.; et al. Multisystem Immune-Related Adverse Events Associated with Immune Checkpoint Inhibitors for Treatment of Non-Small Cell Lung Cancer. JAMA Oncol. 2020, 6, 1952–1956. [Google Scholar] [CrossRef] [PubMed]
- Maher, V.E.; Fernandes, L.L.; Weinstock, C.; Tang, S.; Agarwal, S.; Brave, M.; Ning, Y.-m.; Singh, H.; Suzman, D.; Xu, J.; et al. Analysis of the Association between Adverse Events and Outcome in Patients Receiving a Programmed Death Protein 1 or Programmed Death Ligand 1 Antibody. J. Clin. Oncol. 2019, 37, 2730–2737. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.; Yan, F.; Singla, N.; Levonyack, N.; Formella, J.; Christie, A.; Kapur, P.; Bowman, A.I.; Hammers, H.J.; Hannan, R.; et al. Immune-related adverse events are associated with improved outcomes in ICI-treated renal cell carcinoma patients. J. Clin. Oncol. 2019, 37, 645. [Google Scholar] [CrossRef]
- Verzoni, E.; Carteni, G.; Cortesi, E.; Giannarelli, D.; De Giglio, A.; Sabbatini, R.; Buti, S.; Rossetti, S.; Cognetti, F.; Rastelli, F.; et al. Real-world efficacy and safety of nivolumab in previously-treated metastatic renal cell carcinoma, and association between immune-related adverse events and survival: The Italian expanded access program. J. Immunother. Cancer 2019, 7, 99. [Google Scholar] [CrossRef]
- Martini, D.J.; Goyal, S.; Liu, Y.; Evans, S.T.; Olsen, T.A.; Case, K.; Magod, B.L.; Brown, J.T.; Yantorni, L.; Russler, G.A.; et al. Immune-Related Adverse Events as Clinical Biomarkers in Patients with Metastatic Renal Cell Carcinoma Treated with Immune Checkpoint Inhibitors. Oncologist 2021, 26, e1742–e1750. [Google Scholar] [CrossRef]
- Yoest, J.M. Clinical features, predictive correlates, and pathophysiology of immune-related adverse events in immune checkpoint inhibitor treatments in cancer: A short review. Immunotargets Ther. 2017, 6, 73–82. [Google Scholar] [CrossRef]
- Passat, T.; Touchefeu, Y.; Gervois, N.; Jarry, A.; Bossard, C.; Bennouna, J. Physiopathological mechanisms of immune-related adverse events induced by anti-CTLA-4, anti-PD-1 and anti-PD-L1 antibodies in cancer treatment. Bull. Cancer 2018, 105, 1033–1041. [Google Scholar] [CrossRef]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Berner, F.; Bomze, D.; Diem, S.; Ali, O.H.; Fassler, M.; Ring, S.; Niederer, R.; Ackermann, C.J.; Baumgaertner, P.; Pikor, N.; et al. Association of Checkpoint Inhibitor-Induced Toxic Effects with Shared Cancer and Tissue Antigens in Non-Small Cell Lung Cancer. JAMA Oncol. 2019, 5, 1043–1047. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | RCC1 | RCC2 | RCC3 | RCC4 | RCC5 | RCC6 |
|---|---|---|---|---|---|---|
| Age, years | 73 | 73 | 71 | 27 | 70 | 69 |
| Sex | Female | Female | Male | Female | Male | Male |
| Smoking | Yes | Yes | Yes | No | Yes | Yes |
| Stage | ||||||
| T | 3a | 1b | 3a | 3a | 3a | 1b |
| N | 0 | 0 | 1 | 1 | 0 | 0 |
| M | 1 | 1 | 1 | 0 | 0 | 1 |
| IMDC risk | intermediate | intermediate | poor | intermediate | intermediate | poor |
| Pathology | Clear-cell RCC | Clear-cell RCC | Clear-cell RCC | MiT-family translocation | Clear-cell RCC | Clear-cell RCC |
| Treatment lines | First-line | First-line | First-line | Adjuvant | Adjuvant | Adjuvant |
| irAE | ||||||
| Grade | 2 | 3 | 3 | 2 | 3 | 2 |
| Rash | Yes | No | No | Yes | No | Yes |
| Hepatitis | Yes | No | No | No | No | Yes |
| Diarrhea/colitis | No | Yes | No | Yes | Yes | No |
| Hypothyroidism | No | Yes | No | No | No | No |
| Adrenal insufficiency | No | No | Yes | No | Yes | No |
| TRB Genes | Grade 2 | Grade 3 | ||||
|---|---|---|---|---|---|---|
| Usage Pattern | Frequency (%) | Patient | Usage Pattern | Frequency (%) | Patient | |
| TRBV | TRBV28 | 12.70 | RCC4 | TRBV28 | 13.58 | RCC2 |
| TRBV29-1 | 11.75 | RCC6 | TRBV17 | 12.98 | RCC5 | |
| TRBV29-1 | 11.03 | RCC1 | TRBV20-1 | 10.20 | RCC2 | |
| TRBV29-1 | 10.42 | RCC4 | TRBV7-3 | 9.93 | RCC3 | |
| TRBV20-1 | 10.27 | RCC6 | TRBV7-1 | 9.74 | RCC5 | |
| TRBJ | TRBJ2-1 | 21.50 | RCC1 | TRBJ2-1 | 21.84 | RCC5 |
| TRBJ2-1 | 20.11 | RCC4 | TRBJ2-7 | 17.13 | RCC2 | |
| TRBJ2-7 | 19.46 | RCC6 | TRBJ2-7 | 17.01 | RCC3 | |
| TRBJ2-7 | 18.62 | RCC4 | TRBJ2-1 | 16.47 | RCC3 | |
| TRBJ2-1 | 18.43 | RCC6 | TRBJ2-1 | 16.32 | RCC2 | |
| Diversity Index | Grade 2 | Grade 3 | p Value |
|---|---|---|---|
| Shannon–Weaver index | 9.39 (8.92–9.50) | 8.91 (8.03–10.34) | 0.70 |
| inverse Simpson’s index | 2607 (1751–6672) | 1159.2 (806.0–5394.4) | 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, T.; Nagata, M.; Ikehata, Y.; Nagashima, Y.; Nagaya, N.; Lu, Y.; Horie, S. T-Cell Receptor Repertoire as a Predictor of Immune-Related Adverse Events in Renal Cell Carcinoma. Curr. Issues Mol. Biol. 2023, 45, 8939-8949. https://doi.org/10.3390/cimb45110561
Kobayashi T, Nagata M, Ikehata Y, Nagashima Y, Nagaya N, Lu Y, Horie S. T-Cell Receptor Repertoire as a Predictor of Immune-Related Adverse Events in Renal Cell Carcinoma. Current Issues in Molecular Biology. 2023; 45(11):8939-8949. https://doi.org/10.3390/cimb45110561
Chicago/Turabian StyleKobayashi, Takuro, Masayoshi Nagata, Yoshihiro Ikehata, Yuki Nagashima, Naoya Nagaya, Yan Lu, and Shigeo Horie. 2023. "T-Cell Receptor Repertoire as a Predictor of Immune-Related Adverse Events in Renal Cell Carcinoma" Current Issues in Molecular Biology 45, no. 11: 8939-8949. https://doi.org/10.3390/cimb45110561