
Novel Theranostic Approaches Targeting CCR4-Receptor, Current Status and Translational Prospectives: A Systematic Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
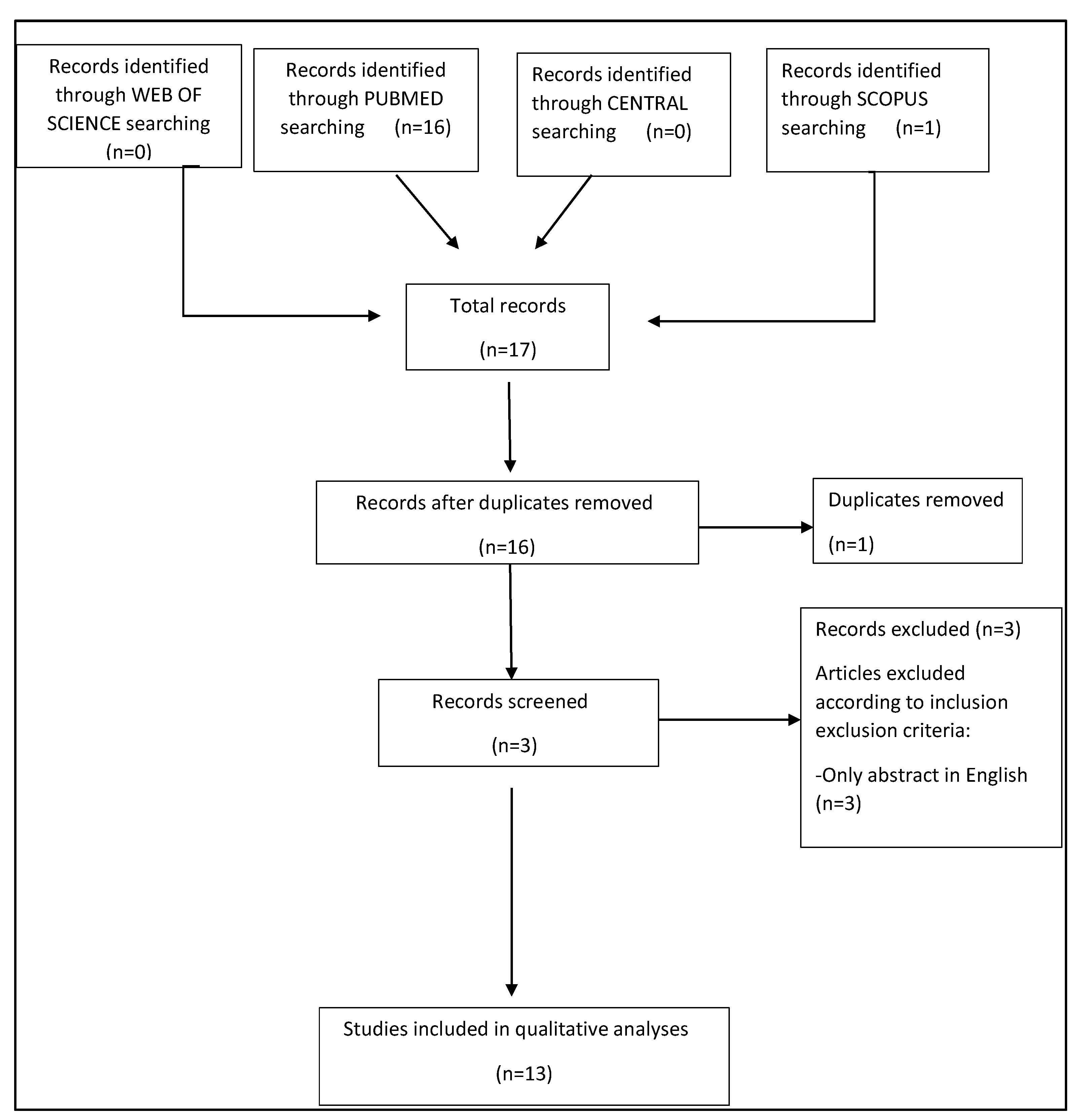
2.1. Search Strategy and Study Selection
2.2. Data Extraction and Methodological Quality Assessment
3. Results
3.1. Analysis of the Evidence
3.2. Study Characteristics and Methodological Quality Assessment
4. Discussion
4.1. CCR4
4.1.1. CCR4 Tissue Expression
4.1.2. CCR4 in Animal Studies
4.2. CCR4-Targeted Molecular Imaging
4.2.1. SPECT/CT CCR4-Target Imaging
4.2.2. PET CCR4-Target Imaging
4.3. Radiation-Enhanced Expression of Chemokine Receptor CCR4
4.4. Mogalizumab, Humanized Anti-CCR4 Monoclonal Antibody, and Its Applications
4.4.1. Adult T Cell Leukemia and Sézary Syndrome
4.4.2. Cutaneous Lymphomas
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cimini, A.; Ricci, M.; Chiaravalloti, A.; Filippi, L.; Schillaci, O. Theragnostic Aspects and Radioimmunotherapy in Pediatric Tumors. Int. J. Mol. Sci. 2020, 21, 3849. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Higuchi, T.; Pomper, M.G.; Rowe, S.P. Theranostics in Oncology-Thriving, Now More than Ever. Diagnostics 2021, 11, 805. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Wan, Q.; Cheng, Z.; Chen, Y. Radionuclide-Labeled Peptides for Imaging and Treatment of CXCR4- Overexpressing Malignant Tumors. Curr. Top. Med. Chem. 2019, 19, 17–32. [Google Scholar] [CrossRef]
- Filippi, L.; Frantellizzi, V.; Chiaravalloti, A.; Pontico, M.; De Feo, M.S.; Corica, F.; Montebello, M.; Schillaci, O.; De Vincentis, G.; Bagni, O. Prognostic and Theranostic Applications of Positron Emission Tomography for a Personalized Approach to Metastatic Castration-Resistant Prostate Cancer. Int. J. Mol. Sci. 2021, 22, 3036. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, E.; Johnson, S.A.; Seegers, W.H. Differentiation of certain platelet factors related to blood coagulation. Circ. Res. 1955, 3, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Yoshie, O.; Matsushima, K. CCR4 and its ligands: From bench to bedside. Int. Immunol. 2015, 27, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Chen, X.; Zeng, W.; Zhou, W.; Zhou, Q.; Wang, Z.; Jiang, W.; Xie, B.; Sun, L.Q. Radiation-Enhanced Expression of CCL22 in Nasopharyngeal Carcinoma is Associated With CCR4(+) CD8 T Cell Recruitment. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 126–139. [Google Scholar] [CrossRef]
- Sugaya, M. Clinical Guidelines and New Molecular Targets for Cutaneous Lymphomas. Int. J. Mol. Sci. 2021, 22, 11079. [Google Scholar] [CrossRef]
- Tanaka, N.; Mori, S.; Kiyotani, K.; Ota, Y.; Gotoh, O.; Kusumoto, S.; Nakano, N.; Suehiro, Y.; Ito, A.; Choi, I.; et al. Genomic determinants impacting the clinical outcome of mogamulizumab treatment for adult T-cell leukemia/lymphoma. Haematologica 2022, 107, 2418–2431. [Google Scholar] [CrossRef]
- Ogura, M.; Ishida, T.; Hatake, K.; Taniwaki, M.; Ando, K.; Tobinai, K.; Fujimoto, K.; Yamamoto, K.; Miyamoto, T.; Uike, N.; et al. Multicenter phase II study of mogamulizumab (KW-0761), a defucosylated anti-cc chemokine receptor 4 antibody, in patients with relapsed peripheral T-cell lymphoma and cutaneous T-cell lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 1157–1163. [Google Scholar] [CrossRef]
- Duvic, M.; Pinter-Brown, L.C.; Foss, F.M.; Sokol, L.; Jorgensen, J.L.; Challagundla, P.; Dwyer, K.M.; Zhang, X.; Kurman, M.R.; Ballerini, R.; et al. Phase 1/2 study of mogamulizumab, a defucosylated anti-CCR4 antibody, in previously treated patients with cutaneous T-cell lymphoma. Blood 2015, 125, 1883–1889. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Schottelius, M.; Lapa, C.; Osl, T.; Poschenrieder, A.; Hänscheid, H.; Lückerath, K.; Schreder, M.; Bluemel, C.; Knott, M.; et al. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J. Nucl. Med. 2016, 57, 248–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, A.; Xu, Y.; Xu, H.; Ren, J.; Meng, T.; Ni, Y.; Zhu, Q.; Zhang, W.B.; Pan, Y.B.; Jin, J.; et al. Lactate-induced M2 polarization of tumor-associated macrophages promotes the invasion of pituitary adenoma by secreting CCL17. Theranostics 2021, 11, 3839–3852. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Guo, H.; Bu, J.; Zhou, M.; Cheng, H.; He, F.; Wang, J.; Wang, X.; Zhang, Y.; Wang, Q.; et al. Rictor/mammalian target of rapamycin 2 regulates the development of Notch1 induced murine T-cell acute lymphoblastic leukemia via forkhead box O3. Exp. Hematol. 2014, 42, 1031–1040.e4. [Google Scholar] [CrossRef]
- Hanaoka, H.; Mukai, T.; Tamamura, H.; Mori, T.; Ishino, S.; Ogawa, K.; Iida, Y.; Doi, R.; Fujii, N.; Saji, H. Development of a 111In-labeled peptide derivative targeting a chemokine receptor, CXCR4, for imaging tumors. Nucl. Med. Biol. 2006, 33, 489–494. [Google Scholar] [CrossRef]
- Kuil, J.; Buckle, T.; Oldenburg, J.; Yuan, H.; Borowsky, A.D.; Josephson, L.; van Leeuwen, F.W. Hybrid peptide dendrimers for imaging of chemokine receptor 4 (CXCR4) expression. Mol. Pharm. 2011, 8, 2444–2453. [Google Scholar] [CrossRef]
- Lesniak, W.G.; Sikorska, E.; Shallal, H.; Behnam Azad, B.; Lisok, A.; Pullambhatla, M.; Pomper, M.G.; Nimmagadda, S. Structural characterization and in vivo evaluation of β-Hairpin peptidomimetics as specific CXCR4 imaging agents. Mol. Pharm. 2015, 12, 941–953. [Google Scholar] [CrossRef] [Green Version]
- Schottelius, M.; Osl, T.; Poschenrieder, A.; Hoffmann, F.; Beykan, S.; Hänscheid, H.; Schirbel, A.; Buck, A.K.; Kropf, S.; Schwaiger, M.; et al. [(177) Lu]pentixather: Comprehensive Preclinical Characterization of a First CXCR4-directed Endoradiotherapeutic Agent. Theranostics 2017, 7, 2350–2362. [Google Scholar] [CrossRef]
- Lim, H.D.; Lane, J.R.; Canals, M.; Stone, M.J. Systematic Assessment of Chemokine Signaling at Chemokine Receptors CCR4, CCR7 and CCR10. Int. J. Mol. Sci. 2021, 22, 4232. [Google Scholar] [CrossRef]
- Spoerl, S.; Kremer, A.N.; Aigner, M.; Eisenhauer, N.; Koch, P.; Meretuk, L.; Löffler, P.; Tenbusch, M.; Maier, C.; Überla, K.; et al. Upregulation of CCR4 in activated CD8(+) T cells indicates enhanced lung homing in patients with severe acute SARS-CoV-2 infection. Eur. J. Immunol. 2021, 51, 1436–1448. [Google Scholar] [CrossRef]
- Asai, N.; Kubo, A.; Suzuki, S.; Murotani, K.; Numanami, H.; Yoshikawa, K.; Ueda, R.; Yamaguchi, E. CCR4 Expression in Tumor-Infiltrating Regulatory T Cells in Patients with Squamous Cell Carcinoma of the Lung: A Prognostic Factor for Relapse and Survival. Cancer Investig. 2019, 37, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, M.; Zhu, Y.; Zhang, X.; Yang, Y.; Wang, C. CCR4 Expression Is Associated With Poor Prognosis in Patients With Early Stage (pN0) Oral Tongue Cancer. J. Oral. Maxillofac. Surg. 2019, 77, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, X.; Wu, H.; Jin, Z.J.; Ma, D.; Yuen, S.; Jing, X.Q.; Shi, M.M.; Shen, B.Y.; Peng, C.H.; Zhao, R.; et al. Up-regulation of chemokine receptor CCR4 is associated with Human Hepatocellular Carcinoma malignant behavior. Sci. Rep. 2017, 7, 12362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ou, B.; Zhao, J.; Guan, S.; Feng, H.; Wangpu, X.; Zhu, C.; Zong, Y.; Ma, J.; Sun, J.; Shen, X.; et al. CCR4 promotes metastasis via ERK/NF-κB/MMP13 pathway and acts downstream of TNF-α in colorectal cancer. Oncotarget 2016, 7, 47637–47649. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Rexiati, M.; Yang, Y.; Wang, W.G.; Azhati, B.; Saimaiti, W.; Wang, Y.J. Expression of chemokine receptor 4 was associated with poor survival in renal cell carcinoma. Med. Oncol. 2014, 31, 882. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.M.; Feng, A.L.; Zhou, C.J.; Liang, X.H.; Mao, H.T.; Deng, B.P.; Yan, S.; Sun, J.T.; Du, L.T.; Liu, J.; et al. Aberrant expression of chemokine receptor CCR4 in human gastric cancer contributes to tumor-induced immunosuppression. Cancer Sci. 2011, 102, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Curiel, T.J.; Coukos, G.; Zou, L.; Alvarez, X.; Cheng, P.; Mottram, P.; Evdemon-Hogan, M.; Conejo-Garcia, J.R.; Zhang, L.; Burow, M.; et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat. Med. 2004, 10, 942–949. [Google Scholar] [CrossRef]
- Sather, B.D.; Treuting, P.; Perdue, N.; Miazgowicz, M.; Fontenot, J.D.; Rudensky, A.Y.; Campbell, D.J. Altering the distribution of Foxp3(+) regulatory T cells results in tissue-specific inflammatory disease. J. Exp. Med. 2007, 204, 1335–1347. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.; Wang, L.; Wells, A.D.; Dorf, M.E.; Ozkaynak, E.; Hancock, W.W. Recruitment of Foxp3+ T regulatory cells mediating allograft tolerance depends on the CCR4 chemokine receptor. J. Exp. Med. 2005, 201, 1037–1044. [Google Scholar] [CrossRef]
- Yuan, Q.; Bromley, S.K.; Means, T.K.; Jones, K.J.; Hayashi, F.; Bhan, A.K.; Luster, A.D. CCR4-dependent regulatory T cell function in inflammatory bowel disease. J. Exp. Med. 2007, 204, 1327–1334. [Google Scholar] [CrossRef] [Green Version]
- Pease, J. CCR4 Chemokine Receptor. In xPharm: The Comprehensive Pharmacology Reference; Enna, S.J., Bylund, D.B., Eds.; Elsevier: New York, NY, USA, 2007; pp. 1–8. [Google Scholar] [CrossRef]
- Sato, F.; Omura, S.; Martinez, N.E.; Tsunoda, I. Chapter 3—Animal Models of Multiple Sclerosis. In Neuroinflammation, 2nd ed.; Minagar, A., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 37–72. [Google Scholar] [CrossRef]
- Mikaeili, A.; Erfani, M.; Sabzevari, O. Synthesis and evaluation of a (99m)Tc-labeled chemokine receptor antagonist peptide for imaging of chemokine receptor expressing tumors. Nucl. Med. Biol. 2017, 54, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Sano, K.; Masuda, R.; Hisada, H.; Oishi, S.; Shimokawa, K.; Ono, M.; Fujii, N.; Saji, H.; Mukai, T. A radiogallium-DOTA-based bivalent peptidic ligand targeting a chemokine receptor, CXCR4, for tumor imaging. Bioorg. Med. Chem. Lett. 2014, 24, 1386–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossain, C.; Jennings, T.; Duffy, R.; Knoblauch, K.; Gochoco, A.; Chervoneva, I.; Shi, W.; Alpdogan, S.O.; Porcu, P.; Pro, B.; et al. The histological prevalence and clinical implications of folliculotropism and syringotropism in mycosis fungoides. Chin. Clin. Oncol. 2019, 8, 6. [Google Scholar] [CrossRef]
- Amorim, G.M.; Niemeyer-Corbellini, J.P.; Quintella, D.C.; Cuzzi, T.; Ramos, E.S.M. Clinical and epidemiological profile of patients with early stage mycosis fungoides. Bras Derm. 2018, 93, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.T.; Bates, S.; Geskin, L. Current Status of HDAC Inhibitors in Cutaneous T-cell Lymphoma. Am. J. Clin. Dermatol. 2018, 19, 805–819. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.H.; Xu, C.; Li, L.L.; Zuo, Y.; Han, D.; He, X.Y.; Cheng, S.X. A targeting delivery system for effective genome editing in leukemia cells to reverse malignancy. J. Control. Release 2022, 343, 645–656. [Google Scholar] [CrossRef]
- Filippi, L.; Bagni, O.; Nervi, C. Aptamer-based technology for radionuclide targeted imaging and therapy: A promising weapon against cancer. Expert Rev. Med. Devices 2020, 17, 751–758. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1. Was There a Clear Question for the Study to Address? | 2. Was There a Comparison with an Appropriate Reference Standard? | 3. Did All Patients Get the Diagnostic Test and Reference Standard? | 4. Could the Results of the Test Have Been Influenced by the Results of the Reference Standard? | 5. Is the Disease Status of the Tested Population Clearly Described? | 6. Were the Methods for Performing the Test Described in Sufficient Detail? | 7. What Are the Results? | 8. How Sure Are We about the Results? Consequences and Cost of Alternatives Performed? | 9. Can the Results Be Applied to Your Patients/the Population of Interest? | 10. Can the Test be Applied to Your Patient or Population of Interest? | 11. Were All Outcomes Important to the Individual or Population Considered? | 12. What Would Be the Impact of Using This Test on Your Patients/Population? | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Li H et al., 2020 [7] | ☺ | ? | ? | ? | ☺ | ☺ | ☺ | ☺ | ☹ | ☹ | ☺ | It may have a positive outcome in therapeutic accuracy and prognosis in human patients |
| Sugaya et al., 2021 [8] | ☺ | ☺ | ☺ | ? | ☺ | ☺ | ☺ | ? | ☺ | ☺ | ☺ | It may lead to a better-targeted therapy |
| Tanaka et al., 2022 [9] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Immunotherapy with a more specific targeted receptor and better prognosis for the patient |
| Ogura et al., 2014 [10] | ☺ | ? | ☺ | ? | ☺ | ☺ | ☺ | ☺ | ☺ | ? | ☺ | Immunotherapy response rate monitorization |
| Duvic et al., 2015 [11] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | ☺ | ? | ☺ | ? | ☺ | Utility in targeted immunotherapy |
| Herrmann et al., 2016 [12] | ☺ | ☺ | ☺ | ? | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Promising results |
| Authors | Year | Type of Article | Nr of Pts | Main Cancer Tissue Expression | Main Molecule | Main Finding |
|---|---|---|---|---|---|---|
| Zhang et al. [13] | 2021 | Original article | In vitro | Pituitary adenoma | mTORC2/ CCL17 | The CCL17/CCR4/mTOCR1 axis may serve as a potential therapeutic target for pituitary adenoma. |
| Sugaya et al. [8] | 2021 | Review | 38 | Cutaneous T cell lymphoma | CD158k, JAK, PIK3, target of rapamycin, and microRNAs | Personalized therapy based on the detection of the genetic signatures of tumors and inhibition of the most suitable target molecules constitutes a future treatment strategy for MF/SS. |
| Li et al. [7] | 2020 | Original article | 1 | Nasopharyngeal Carcinoma | CCL22 | The radiation-enhanced release of CCL22 from NPC cells promotes migration of CCR4 + effector CD8 T cells, which might partially be associated with radiation therapy-mediated antitumor immunity. |
| Tanaka et al. [9] | 2022 | Original article | 64 | Lymphoma, T Cell, Peripheral and Cutaneous | Mogamulizumab | Patients with CCR4 alterations or without CCR7 alterations exhibited a more favorable clinical response to Mogamulizumab. |
| Hua et al. [14] | 2014 | Research | In vivo | T cell acute lymphoblastic leukemia (T-ALL) | Forkhead box O3/mTORC2 | The inactivation of mTORC2 causes the overexpression of forkhead box O3 and its downstream effectors and eases the progression of leukemia in T-ALL mice. |
| Liu et al. [3] | 2019 | Review | In vitro | CCR4 expressing tumors | CXCR4 peptides | The potential of CCR4 as a theranostic agent. |
| Hanaoka et al. [15] | 2006 | Research | In vitro | Pancreatic cancer | 111In-DTPA-Ac-TZ14011 | 111In-DTPA-Ac-TZ14011 would be a potential agent for the imaging of CXCR4 expression in metastatic tumors in vivo |
| Kuil et al. [16] | 2011 | Research | In vitro | CCR4 expressing tumors | Hybrid peptide dendrimers/ cyclic Ac-TZ14011 peptide | Biodistribution studies revealed that the additional peptides in the dimer and tetramer reduced nonspecific muscle uptake. |
| Lesniak et al. [17] | 2015 | Research | In vivo | CXCR4 expressing subcutaneous U87 tumors | [111In]POL-D and [111In]POL-PD | POL3026 is a promising template to develop new imaging agents that target CXCR4. |
| Schottelius et al. [18] | 2017 | Research | In vivo | Multiple Myeloma | [68Ga]pentixafor/ [177Lu]pentixather | High clinical potential for [68Ga]pentixafor/[177Lu]pentixather in CCR4 expressing tumors. |
| Herrmann et al. [12] | 2016 | Research | 3 | Multiple Myeloma | 177Lu-pentixather/ 90Y-pentixather | CXCR4-targeted radiotherapy with pentixather appears to be a promising novel treatment option in combination with cytotoxic chemotherapy and autologous stem cell transplantation, especially for patients with advanced multiple myeloma. |
| Ogura et al. [10] | 2014 | Clinical Trial, Phase II | 38 | Lymphoma, T Cell, Peripheral and Cutaneous | Mogamulizumab | Mogamulizumab showed meaningful antitumor activity in patients with relapsed PTCL and CTCL. |
| Duvic et al. [11] | 2015 | Clinical Trial, Phase II | 41 | Cutaneous T cell lymphoma | Mogamulizumab | No dose-limiting toxicity was observed with the use of Mogamulizumab. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorica, J.; De Feo, M.S.; Corica, F.; Sidrak, M.M.A.; Conte, M.; Filippi, L.; Schillaci, O.; De Vincentis, G.; Frantellizzi, V. Novel Theranostic Approaches Targeting CCR4-Receptor, Current Status and Translational Prospectives: A Systematic Review. Pharmaceuticals 2023, 16, 313. https://doi.org/10.3390/ph16020313
Gorica J, De Feo MS, Corica F, Sidrak MMA, Conte M, Filippi L, Schillaci O, De Vincentis G, Frantellizzi V. Novel Theranostic Approaches Targeting CCR4-Receptor, Current Status and Translational Prospectives: A Systematic Review. Pharmaceuticals. 2023; 16(2):313. https://doi.org/10.3390/ph16020313
Chicago/Turabian StyleGorica, Joana, Maria Silvia De Feo, Ferdinando Corica, Marko Magdi Abdou Sidrak, Miriam Conte, Luca Filippi, Orazio Schillaci, Giuseppe De Vincentis, and Viviana Frantellizzi. 2023. "Novel Theranostic Approaches Targeting CCR4-Receptor, Current Status and Translational Prospectives: A Systematic Review" Pharmaceuticals 16, no. 2: 313. https://doi.org/10.3390/ph16020313