

A Clinical Perspective on Bespoke Sensing Mechanisms for Remote Monitoring and Rehabilitation of Neurological Diseases: Scoping Review

Abstract
:1. Introduction
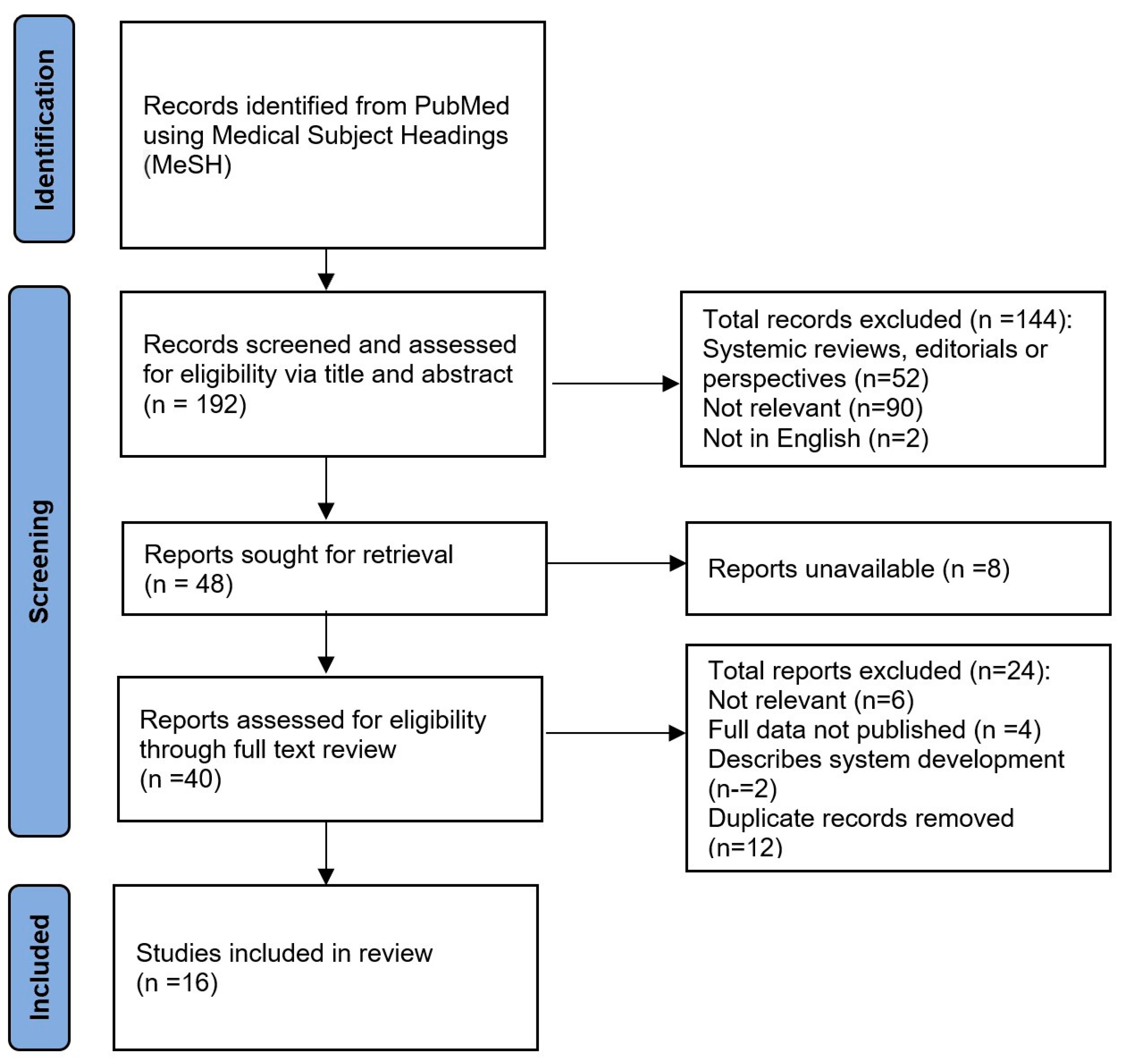
2. Methods
2.1. Search Method
- “Stroke” AND “Remote Sensing Technology”
- “Stroke” AND “Telerehabilitation”
- “Neurodegenerative Disease” AND “Remote Sensing Technology”
- “Neurodegenerative Disease” AND “Telerehabilitation”
- “Parkinson’s Disease” AND “Remote Sensing Technology”
- “Parkinson’s Disease” AND “Telerehabilitation”
- “Alzheimer Disease” AND “Remote Sensing Technology”
- “Alzheimer Disease” AND “Telerehabilitation”
- “Dementia” AND “Remote Sensing Technology”
- “Dementia” AND “Telerehabilitation”
- “Amyotrophic Lateral Sclerosis” AND “Remote Sensing Technology”
- “Amyotrophic Lateral Sclerosis” AND “Telerehabilitation”
- “Motor Neuron Disease” AND “Remote Sensing Technology”
- “Motor Neuron Disease” AND “Telerehabilitation”
2.2. Eligibility
2.3. Selection of Study
3. Results
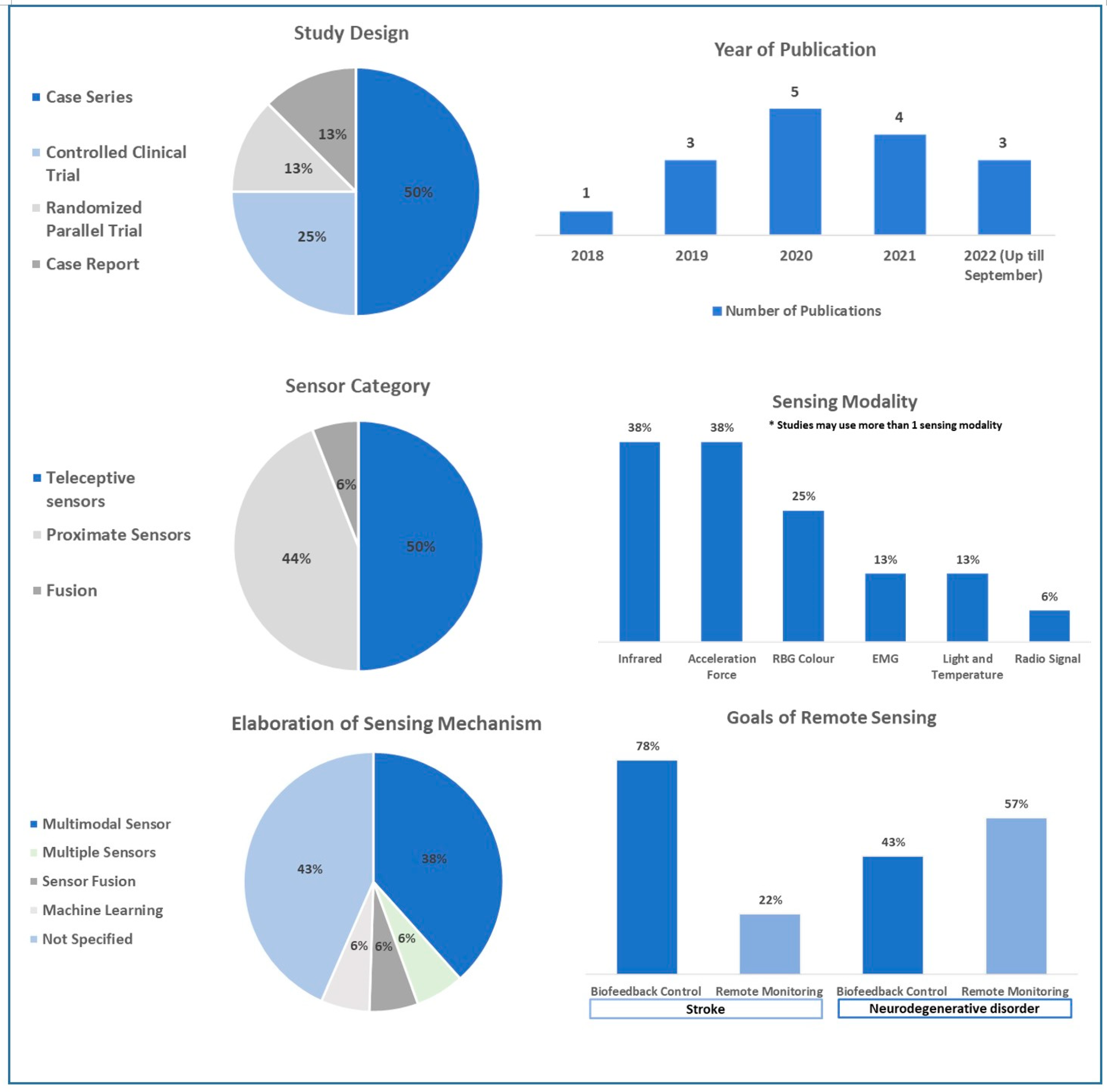
3.1. Characteristics of Included Study
3.2. Use of Sensors in Stroke
3.3. Use of Sensors in Neurodegenerative Disorders
3.4. Summary of Study Findings Regarding the Sensing Mechanism in Neurological Diseases
4. Discussion
4.1. Clinical Considerations for an Ideal Sensing Mechanism in Remote Rehabilitation
4.1.1. Commonly Used Clinical Parameters for Functional Assessment in Neurological Disease
4.1.2. Elaboration of Sensing Mechanisms to Process Data Tailored to Clinical Needs
Multimodal Sensors
Applying Multiple Unimodal Sensors
Sensor Fusion
Machine Learning Algorithms
4.1.3. Application of Feedback and Feedforward Control System to the Sensing Mechanism
4.2. Factors Affecting the Adoption of Sensing Mechanism
4.3. Limitations and Directions of Future Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 US Neurological Disorders Collaborators. Burden of Neurological Disorders Across the US From 1990–2017: A Global Burden of Disease Study. JAMA Neurol. 2021, 78, 165–176. [Google Scholar] [CrossRef]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020, 31, CD010255. [Google Scholar] [CrossRef]
- Chen, Y.; Abel, K.T.; Janecek, J.T.; Chen, Y.; Zheng, K.; Cramer, S.C. Home-based technologies for stroke rehabilitation: A systematic review. Int. J. Med. Inform. 2019, 123, 11–22. [Google Scholar] [CrossRef]
- Alarcón-Aldana, A.C.; Callejas-Cuervo, M.; Bo, A.P.L. Upper Limb Physical Rehabilitation Using Serious Videogames and Motion Capture Systems: A Systematic Review. Sensors 2020, 20, 5989. [Google Scholar] [CrossRef]
- Spencer, J.; Wolf, S.L.; Kesar, T.M. Biofeedback for Post-stroke Gait Retraining: A Review of Current Evidence and Future Research Directions in the Context of Emerging Technologies. Front. Neurol. 2021, 12, 637199. [Google Scholar] [CrossRef]
- di Biase, L.; Di Santo, A.; Caminiti, M.L.; De Liso, A.; Shah, S.A.; Ricci, L.; Di Lazzaro, V. Gait Analysis in Parkinson’s Disease: An Overview of the Most Accurate Markers for Diagnosis and Symptoms Monitoring. Sensors 2020, 20, 3529. [Google Scholar] [CrossRef]
- Ferreira-Sánchez, M.D.R.; Moreno-Verdú, M.; Cano-de-la-Cuerda, R. Quantitative Measurement of Rigidity in Parkinson’s Disease: A Systematic Review. Sensors 2020, 20, 880. [Google Scholar] [CrossRef] [Green Version]
- Aşuroğlu, T.; Oğul, H. A deep learning approach for parkinson’s disease severity assessment. Health Technol. 2022, 12, 943–953. [Google Scholar] [CrossRef]
- Açıcı, K.; Erdaş, C.B.; Aşuroğlu, T.; Oğul, H. Handy: A Benchmark Dataset for Context-Awareness via Wrist-Worn Motion Sensors. Data 2018, 3, 24. [Google Scholar] [CrossRef] [Green Version]
- Eng, J.J.; Pastva, A.M. Advances in Remote Monitoring for Stroke Recovery. Stroke 2022, 53, 2658–2661. [Google Scholar] [CrossRef]
- Qiu, Q.; Cronce, A.; Patel, J.; Fluet, G.G.; Mont, A.J.; Merians, A.S.; Adamovich, S.V. Development of the Home based Virtual Rehabilitation System (HoVRS) to remotely deliver an intense and customized upper extremity training. J. Neuroeng. Rehabil. 2020, 17, 155. [Google Scholar] [CrossRef] [PubMed]
- Nam, C.; Zhang, B.; Chow, T.; Ye, F.; Huang, Y.; Guo, Z.; Li, W.; Rong, W.; Hu, X.; Poon, W. Home-based self-help telerehabilitation of the upper limb assisted by an electromyography-dr iven wrist/hand exoneuromusculoskeleton after stroke. J. Neuroeng. Rehabil. 2021, 18, 137. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.; Wang, J.; Li, Y.; Shen, L.; Chen, Z.; Long, J. A novel upper-limb tracking system in a virtual environment for stroke rehabilitation. J. Neuroeng. Rehabil. 2021, 18, 166. [Google Scholar] [CrossRef] [PubMed]
- Marin-Pardo, O.; Phanord, C.; Donnelly, M.R.; Laine, C.M.; Liew, S.-L. Development of a Low-Cost, Modular Muscle-Computer Interface for At-Home Telerehabilitation for Chronic Stroke. Sensors 2021, 21, 1806. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.M.; Lee, S.; Uhm, K.E.; Kurillo, G.; Han, J.J.; Lee, J. Upper Limb Three-Dimensional Reachable Workspace Analysis Using the Kinect Sensor in Hemiplegic Stroke Patients: A Cross-Sectional Observational Study. Am. J. Phys. Med. Rehabil. 2020, 99, 397–403. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, W.; Li, Q.; Ma, W. Medical Data Acquisition and Internet of Things Technology-Based Cerebral Stroke Disease Prevention and Rehabilitation Nursing Mobile Medical Management System. Comput. Math. Methods Med. 2022, 2022, 4646454. [Google Scholar] [CrossRef]
- Chen, S.C.; Lin, C.H.; Su, S.W.; Chang, Y.T.; Lai, C.H. Feasibility and effect of interactive telerehabilitation on balance in individuals with chronic stroke: A pilot study. J. Neuroeng. Rehabil. 2021, 18, 71. [Google Scholar] [CrossRef]
- Salgueiro, C.; Urrútia, G.; Cabanas-Valdés, R. Influence of Core-Stability Exercises Guided by a Telerehabilitation App on Trunk Performance, Balance and Gait Performance in Chronic Stroke Survivors: A Preliminary Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 5689. [Google Scholar] [CrossRef]
- Rogerson, L.; Burr, J.; Tyson, S. The feasibility and acceptability of smart home technology using the Howz system for people with stroke. Disabil. Rehabil. Assist. Technol. 2020, 15, 148–152. [Google Scholar] [CrossRef]
- Abujrida, H.; Agu, E.; Pahlavan, K. Machine learning-based motor assessment of Parkinson’s disease using postural sway, gait and lifestyle features on crowdsourced smartphone data. Biomed. Phys. Eng. Express 2020, 6, 035005. [Google Scholar] [CrossRef]
- Dominey, T.; Kehagia, A.A.; Gorst, T.; Pearson, E.; Murphy, F.; King, E.; Carroll, C. Introducing the Parkinson’s KinetiGraph into Routine Parkinson’s Disease Care: A 3-Year Single Centre Experience. J. Park. Dis. 2020, 10, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Lipsmeier, F.; Taylor, K.I.; Postuma, R.B.; Volkova-Volkmar, E.; Kilchenmann, T.; Mollenhauer, B.; Bamdadian, A.; Popp, W.L.; Cheng, W.Y.; Zhang, Y.P.; et al. Reliability and validity of the Roche PD Mobile Application for remote monitoring of early Parkinson’s disease. Sci. Rep. 2022, 12, 12081. [Google Scholar] [CrossRef] [PubMed]
- Cikajlo, I.; Hukić, A.; Dolinšek, I.; Zajc, D.; Vesel, M.; Krizmanič, T.; Blažica, B.; Biasizzo, A.; Novak, F.; Peterlin, P.K. Can telerehabilitation games lead to functional improvement of upper extremities in individuals with Parkinson’s disease? Int. J. Rehabil. Res. 2018, 41, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Vahia, I.V.; Kabelac, Z.; Hsu, C.Y.; Forester, B.P.; Monette, P.; May, R.; Hobbs, K.; Munir, U.; Hoti, K.; Katabi, D. Radio Signal Sensing and Signal Processing to Monitor Behavioral Symptoms in Dementia: A Case Study. Am. J. Geriatr. Psychiatry 2020, 28, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, I.; Stavropoulos, T.G.; Meditskos, G.; Andreadis, S.; Kompatsiaris, I.; Tsolaki, M. Long-Term Impact of Intelligent Monitoring Technology on People with Cognitive Impairment: An Observational Study. J. Alzheimers Dis. 2019, 70, 757–792. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Zmora, R.; Mitchell, L.L.; Finlay, J.M.; Peterson, C.M.; McCarron, H.; Jutkowitz, E. Six-Month Effectiveness of Remote Activity Monitoring for Persons Living With Dementia and Their Family Caregivers: An Experimental Mixed Methods Study. Gerontologist 2019, 59, 78–89. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- National Institute of Aging. Available online: https://www.nia.nih.gov/health/vascular-dementia (accessed on 18 November 2022).
- Siniscalchi, A.; Gallelli, L.; Labate, A.; Malferrari, G.; Palleria, C.; De Sarro, G. Post-stroke Movement Disorders: Clinical Manifestations and Pharmacological Management. Curr. Neuropharmacol. 2012, 10, 254–262. [Google Scholar] [CrossRef] [Green Version]
- Winters, J.M.; Wang, Y.; Winters, J.M. Wearable sensors and telerehabilitation. IEEE Eng. Med. Biol. Mag. 2003, 22, 56–65. [Google Scholar] [CrossRef]
- de Quirós, M.B.; Douma, E.; Akker-Scheek, I.V.D.; Lamoth, C.J.C.; Maurits, N.M. Quantification of Movement in Stroke Patients under Free Living Conditions Using Wearable Sensors: A Systematic Review. Sensors 2022, 22, 1050. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Tardieu, G.; Shentoub, S.; Delarue, R. A la recherche d’une technique de measure de la spasticité. Revue de Neurologie (Paris). [Research on a technique for measurement of spasticity]. Rev. Neurol. 1954, 91, 143–144. [Google Scholar] [PubMed]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R. Movement Disorder Society UPDRS Revision Task Force. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Downs, S. The Berg Balance Scale. J. Physiother. 2015, 61, 46. [Google Scholar] [CrossRef] [Green Version]
- Aşuroğlu, T.; Açıcı, K.; Erdaş, C.B.; Toprak, M.K.; Erdem, H.; Oğul, H. Parkinson’s disease monitoring from gait analysis via foot-worn sensors. Biocybern. Biomed. Eng. 2018, 38, 760–772. [Google Scholar] [CrossRef]
- Ries, J.D. Rehabilitation for Individuals with Dementia: Facilitating Success. Curr. Geriatr. Rep. 2018, 7, 59–70. [Google Scholar] [CrossRef]
- Telenius, E.W.; Engedal, K.; Bergland, A. Inter-rater reliability of the Berg Balance Scale, 30 s chair stand test and 6 m walking test, and construct validity of the Berg Balance Scale in nursing home residents with mild-to-moderate dementia. BMJ Open 2015, 5, e008321. [Google Scholar] [CrossRef] [PubMed]
- Bossers, W.J.; van der Woude, L.H.; Boersma, F.; Scherder, E.J.A.; van Heuvelen, M.J.G. The Groningen Meander Walking Test: A dynamic walking test for older adults with dementia. Phys. Ther. 2014, 94, 262–272. [Google Scholar] [CrossRef] [Green Version]
- Suttanon, P.; Hill, K.D.; Dodd, K.J.; Said, C.M. Retest reliability of balance and mobility measurements in people with mild to moderate Alzheimer’s disease. Int. Psychogeriatr. 2011, 23, 1152–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, H.; Mizoguchi, Y.; Tadakuma, K.; Ming, A.; Ishikawa, M.; Shimojo, M. Development of intelligent robot hand using proximity, contact and slip sensing. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation (ICRA), Anchorage, AK, USA, 3–7 May 2010; Volume 777–784, p. 5509243. [Google Scholar] [CrossRef]
- Wang, H.; Wang, L.; Xiang, Y.; Zhao, N.; Li, X.; Chen, S.; Lin, C.; Li, G. Assessment of elbow spasticity with surface electromyography and mechanomyography based on support vector machine. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 3860–3863. [Google Scholar] [CrossRef]
- Yokoyama, H.; Kanashima, T.; Okuyama, M.; Abe, T.; Noma, H.; Azuma, T.; Sohgawa, M. Touch Sensing by Multi-axial Force Measurement Using High-Resolution Tactile Sensor with Microcantilevers. IEEJ Trans. Sens. Micromach. 2014, 134, 58–63. [Google Scholar] [CrossRef]
- Oubre, B.; Daneault, J.F.; Jung, H.T.; Whritenour, K.; Miranda, J.G.V.; Park, J.; Ryu, T.; Kim, Y.; Lee, S.I. Estimating Upper-Limb Impairment Level in Stroke Survivors Using Wearable Inertial Sensors and a Minimally-Burdensome Motor Task. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 601–611. [Google Scholar] [CrossRef] [PubMed]
- MacIver, M. Neuroethology: From Morphological Computation to Planning. In The Cambridge Handbook of Situated Cognition; Robbins, P., Aydede, M., Eds.; Cambridge University Press: New York, NY, USA, 2009; pp. 480–504. [Google Scholar]
- Krausz, N.E.; Hargrove, L.J. A Survey of Teleceptive Sensing for Wearable Assistive Robotic Devices. Sensors 2019, 19, 5238. [Google Scholar] [CrossRef] [Green Version]
- Lee, J. Patient-Specific Predictive Modeling Using Random Forests: An Observational Study for the Critically Ill. JMIR Med. Inform. 2017, 5, e3. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.-C.; Chen, S.-F.; Lin, C.-H.; Shih, C.-J.; Lin, A.-C.; Yuan, W.; Li, Y.-C.; Kuo, T.-Y. Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units. Sensors 2021, 21, 1864. [Google Scholar] [CrossRef] [PubMed]
- Panwar, M.; Biswas, D.; Bajaj, H.; Jöbges, M.; Turk, R.; Maharatna, K.; Acharyya, A. Rehab-Net: Deep Learning Framework for Arm Movement Classification Using Wearable Sensors for Stroke Rehabilitation. IEEE Trans. Biomed. Eng. 2019, 66, 3026–3037. [Google Scholar] [CrossRef]
- Balestra, N.; Sharma, G.; Riek, L.M.; Busza, A. Automatic Identification of Upper Extremity Rehabilitation Exercise Type and Dose Using Body-Worn Sensors and Machine Learning: A Pilot Study. Digit. Biomark. 2021, 5, 158–166. [Google Scholar] [CrossRef]
- Sudharani, K.; Sarma, T.C.; Satya Prasad, K. Brain stroke detection using K-Nearest Neighbor and Minimum Mean Distance technique. In Proceedings of the 2015 International Conference on Control, Instrumentation, Communication and Computational Technologies (ICCICCT), Kumaracoil, India, 18–19 December 2015; pp. 770–776. [Google Scholar] [CrossRef]
- Kandukuri, K.; Sandhya, A. Heart Stroke Detection Using KNN Algorithm. ECS Trans. 2022, 107, 18385. [Google Scholar] [CrossRef]
- Xing, W.; Bei, Y. Medical Health Big Data Classification Based on KNN Classification Algorithm. IEEE Access 2020, 8, 28808–28819. [Google Scholar] [CrossRef]
- Liang, J.; Qin, Z.; Ni, J.; Lin, X.; Shen, X. Practical and Secure SVM Classification for Cloud-Based Remote Clinical Decision Services. IEEE Trans. Comput. 2021, 70, 1612–1625. [Google Scholar] [CrossRef]
- Cai, S.; Chen, Y.; Huang, S.; Wu, Y.; Zheng, H.; Li, X.; Xie, L. SVM-Based Classification of sEMG Signals for Upper-Limb Self-Rehabilitation Training. Front. Neurorobotics 2019, 13, 31. [Google Scholar] [CrossRef] [Green Version]
- Hamaguchi, T.; Saito, T.; Suzuki, M.; Ishioka, T.; Tomisawa, Y.; Nakaya, N.; Abo, M. Support Vector Machine-Based Classifier for the Assessment of Finger Movement of Stroke Patients Undergoing Rehabilitation. J. Med. Biol. Eng. 2020, 40, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Seidler, R.D.; Noll, D.C.; Thiers, G. Feedforward and feedback processes in motor control. Neuroimage 2004, 22, 1775–1783. [Google Scholar] [CrossRef]
- Marangunić, N.; Granić, A. Technology acceptance model: A literature review from 1986 to 2013. Univers. Access Inf. Soc. 2015, 14, 81–95. [Google Scholar] [CrossRef]
- Keogh, A.; Dorn, J.F.; Walsh, L.; Calvo, F.; Caulfield, B. Comparing the Usability and Acceptability of Wearable Sensors Among Older Irish Adults in a Real-World Context: Observational Study. JMIR mHealth uHealth 2020, 8, e15704. [Google Scholar] [CrossRef]
- Biddiss, E.; Beaton, D.; Chau, T. Consumer design priorities for upper limb prosthetics. Disabil. Rehabil. Assist. Technol. 2007, 2, 346–357. [Google Scholar] [CrossRef]
- AshaRani, P.V.; Jue Hua, L.; Roystonn, K.; Siva Kumar, F.; Peizhi, W.; Ying Jie, S.; Shafie, S.; Chang, S.; Jeyagurunathan, A.; Boon Yiang, C. Readiness and Acceptance of eHealth Services for Diabetes Care in the General Population: Cross-sectional Study. J. Med. Internet Res. 2021, 23, e26881. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors, Published Year | Study Design | Study Sample | Device Name | Site | Sensor Type | Sensing Modality | Measured Clinical Parameters | Dataset (Repository) | Machine Learning Prediction | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Rogerson L et al., 2019 [19] | CS | 19 stroke patients | Howz system (Commercialized) | NA | Ambient sensor, door sensor, and smart plug | Temperature, light | Mean number of times participant was active during the day, door sensor activation, alerts (due to low activity or late start) | Mean number of times participant was active during the day = 47.1 ± 55, Mean number of times door sensor was activated per day = 5 ± 2.4, number of alerts = 1.1 ± 1.2 (Public) | NA | Howz system for monitoring and feedback activities were feasible and acceptable for stroke survivors. No technological problems or adverse events were noted. The system was nonobtrusive, easy to use, and provided peace of mind that help would be at hand if needed. |
| Lee YM et al., 2020 [15] | CS | 41 stroke patients | Microsoft Kinect (Commercialized) | NA | RGB camera, depth sensor, infrared sensor | RGB, depth, infrared | Upper extremity 3D Kinect-based reachable workspace, FMA, MI-UE, QuickDASH | Total upper limb FMA (n = 34) = 50.8 ± 19.5, MI-UE (n = 41) = 79.8 ± 20.1, QuickDASH = 32.5 ± 23.8. Correlation: total RSA and FMA total (R2 = 0.68, p < 0.01), total RSA and MI-UE (R2 = 0.65, p < 0.01), total RSA and QuickDASH (R2 = 0.42, p < 0.01) (Public) | NA | A Kinect-based reachable workspace could be a useful alternative outcome measure of upper limb impairment and disability. The total relative surface area of the paretic side correlated with FMA, MI, and QuickDASH scores. |
| Qiu Q et al., 2020 [11] | CS | 15 stroke patients | LMC | NA | Infrared LEDs, infrared cameras | Infrared | Upper extremity FMA, hand kinematics (HOR, HOA, WPR, WPA, HRR, HRA) | Mean increase of upper extremity FMA = 5.2 (SE = 0.69, p < 0.001). Improved ROM: 15.83% for HOR, 27.50% for WPR, and 37.20% for HRR. Less error during tracing task (15.76% in HOA, 18.70% in WPA and 18.75% in HRA) (Private) | NA | HoVRS provides data for customizing upper limb rehabilitation in their home setting with minimal in person instruction or assistance. Improvements in upper limb function and six measurements of hand kinematics are noted with use of the system. |
| Chen SC et al., 2021 [17] | CCT | 30 stroke patients (15 Kinect, 15 controls) | Microsoft Kinect (Commercialized) | NA | RGB camera, depth sensor, infrared sensor | RGB, depth, infrared | BBS, TUG, Modified Falls Efficacy Scale, MI, and FAC | Improvement in BBS in both groups (control group: p = 0.01, effect size = 0.49; experimental group: p = 0.01, effect size = 0.70). TUG scores in experimental group improved (p = 0.005, effect size = 0.70) (Private) | NA | Kinect-based interactive telerehabilitation system with remote therapist supervision has superior or equal efficiency compared to one-on-one physiotherapy. Compliance and safety of this interactive telerehabilitation system is observed. |
| Nam C et al., 2021 [12] | CS | 11 stroke patients | NA | Wrist, hand | WH-ENMS | EMG | FMA, ARAT, WMFT, Motor FIM, MAS, EMG activation level, and the Co-contraction Index (CI) of the target muscles | Significant improvements (p < 0.05, paired sample t test) in the mean FMA full score (33.4 vs. 44.5), ARAT (19.3 vs. 26.7), WMFT score (39.2 vs. 45.9), WMFT time (51.6 vs. 45.7) before and after training. Significant decrease (p < 0.05, Wilcoxon’s signed rank test) in mean MAS scores at elbow (2.18 vs. 1.49), wrist (1.95 vs. 1.18) and finger (1.98 vs. 1.40) before and after training. Significant decreases in the EMG activation levels of the APB and FCR-FD and EMG co-contraction index of measured muscle pairs; and significant reductions in the number of movements and maximal trunk displacements. (Private) | NA | WH-ENMS-assisted home- based self-help rehabilitation was feasible and effective for improving upper limb function. Significantimprovements in the voluntary motor control and muscle coordination of the upper limb, increased smoothness and reduced compensatory trunk movement during arm reaching coordinated with distal movements, and release of muscular spasticity at the elbow, wrist, and fingers. |
| Cha K et al., 2021 [13] | RPT | 27 stroke patients | VRRS, LMC | NA | RGB camera (VRRS), infrared LEDs, and cameras (LMC) | RGB, infrared | FMA, virtual body ownership, agency, location of the body, and usability | FMA pre- and post-training: Conventional therapy (23.44 vs. 28.11, p = 0.000, D-value = 4.67), LMC (27.67 vs. 33.56, p = 0.001, D-value = 5.89), VRSS (20.78 vs. 31.22, p = 0.000, D-value = 10.44). Significant difference (F = 5.426, p = 0.005) with a large effect size (ƞ2 = 0.361) in D-value between VRSS and conventional therapy. Significant difference (F = 5.426, p = 0.021) with a large effect size (ƞ2 = 0.221) in the D-value between VRSS and LMC. Significant differences between VRRS and LP in body ownership (3.2 vs. 1.3, p = 0.044), agency (6.8 vs. 4.2, p = 0.049), usability (69.7 vs. 55.8, p = 0.038) (Private) | NA | VRRS improved the users’ senses of body ownership, agency, and location of the body. Users preferred using the VRRS to using the LMC. VRRS promotes rehabilitation; FMA scores improved in all groups in experiment 2, the mean D-values of the FMA scores of the group using VRRS was significantly higher than the control groups. |
| Marin-Pardo O et al., 2021 [14] | CR | 1 stroke patient | Tele-REINVE-NT | Forearm | EMG | Surface EMG | EMG signals, game performance, user experience, patient-reported change in motor function | No statistically significant changes for extensor (rho = 0.27, p = 0.164) or flexor (rho = −0.34, p = 0.071) muscle activity, game performance (rho = 0.29, p = 0.06). (Public) | NA | Muscle-computer interface system had no adverse events and patient did not perceive discomfort, pain, or fatigue. Normalization of co-contraction was not statistically significant. Patient reported positive changes in motor function and improved quality of life. |
| Song Y et al., 2022 [16] | CCT | 32 stroke patients, 6 healthy control-s | Mobile medical managem-ent system based on IOT technology | Upper arm | Accelerometer | Acceleration force | Brunnstrom staging | When the noise intensity was 5%, 10%, 20%, 40%, and 60%, the MSE of the optimized median filtering algorithm were 54:17 ± 4:52, 103:52 ± 8:63, 215:42 ± 17:95, 1302:17 ± 108:51, and 4865:22 ± 455:26, respectively, and MSE of the median filtering algorithm before optimization were 2:17 ± 0:34, 15:41 ± 1:48, 21:52 ± 1:99, 52:42 ± 4:87, and 116:92 ± 8:63, respectively. PSNR of the optimized median filtering algorithm was significantly higher than that before optimization. Maximum prediction accuracy of 89.83% in the test set was achieved with 23 neurons. (Private) | BP neural network. Training time (2.5 s) and root MSE (0.29) of the model were lowest when Traingda was used. Training time and root MSE of traingda were significantly lower than traingd and traingdm functions. Training steps of traingda function were significantly different from those of traingd and traingdm functions. When transfer in the hidden layer and the input layer is tansig, the error percentage (7.56%) and root MSE (0.25) of model are minimum. | MSE of the signal showed a significant upward trend. Brunnstrom staging results were compared with the prediction results of the mobile monitoring system. Prediction results of Brunnstrom stages I and II were completely consistent with the clinical staging results. 3 samples or 9.37% showed different normal prediction results and clinical stage results in stages III–VI, and the prediction accuracy was 90.63%. There is certain application value for the rehabilitation of stroke patients. |
| Salgueiro C et al., 2022 [18] | CCT | 30 stroke patients (15 G-Walk and 15 control-s) | G-Walk accelerom-eter system from BTS Bioengine-ering (Commercialized) | Trunk, entire lower limb | Accelerometer | Acceleration force | STIS2.0, S-FIST, S-PASS, BBS, the number of falls and gait parameters measured by the G-Walk accelerometer system | Improvements in S-TIS 2.0 balance pre- and post-intervention: control (4.27 vs. 4.31, p = 0.534), experimental group (4.73 vs. 6.71, p = 0.001), p = 0.007. Significant differences pre- and post-intervention intergroup S-TIS 2.0 total: control (7.33 vs. 7.46, p = 0.606), experimental group (7.60 vs. 10.36, p = 0.000), p = 0.032. BBS pre- and post-intervention, improved in both control (41.27 vs. 42.54, p = 0.009) and experimental groups (43.2 vs. 44.93, p = 0.029). (Public) | NA | The authors used an accelerometer to measure gait parameters. Performing core-strengthening exercises guided by a telerehabilitation application vs. conventional therapy seems to improve trunk function and sitting balance in chronic post-stroke. |
| Authors/ Published Year | Study Design | Study Sample | Device Name | Site | Sensor Type | Sensing Modality | Measured Clinical Parameters | Dataset (Repository) | Machine Learning Prediction | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Cikajlo I et al., 2018 [23] | CS | 26 patients with PD | Microsoft Kinect (Commercialized) | NA | RGB camera, depth sensor, infrared sensor | RGB, depth, infrared | Box and Blocks Test, UPDRS and daily activity Jebsen’s test, writing a letter, moving light objects, Nine-Hole Peg Test, PDQ-39 | Statistically significant improvements in Box and Blocks Test (mean: 47 vs. 52, p = 0.002, Cohen’s d = 0.40), UPDRS III (mean: 27 vs. 29, p = 0.001, d = 0.22), and daily activity Jebsen’s test; writing a letter (mean: 24.0 vs. 20.6, p = 0.003, d = 0.23); and moving light objects (mean: 4.4 vs. 3.9, p = 0.006, d = 0.46). (Private) | NA | Telerehabilitation exergaming system which tracked participants’ movements and adapted the difficulty level of games in real-time is feasible but may require technical assistance. This resulted in clinically meaningful significant improvements. Nine-Hole Peg Test did not significantly improve. Participants claimed problems with mobility but less with ADLs and emotional well-being. (PDQ-39) |
| Gaugler JE et al., 2019 [26] | CCT | 132 patients with AD or a related dementia | RAM System (GreatCall system) (Commercialized) | NA | Ambient sensor | Information not available | Qualitative outcomes of SSCQ, self-efficacy, burden, role captivity, role overload, and CES-D | At baseline and 6 months post RAM: SSCQ controls (24.26 vs. 23.73) treatment (24.17 vs. 23.33); Self-Efficacy controls (27.62 vs. 27.59) treatment (27.94 vs. 28.39); Burden: controls (37.01 vs. 40.93) treatment (37.59 vs. 40.40); Role Captivity: controls (6.35 vs. 6.56) treatment (6.13 vs. 6.74); Role Overload: controls (7.41 vs. 7.42) treatment (7.95 vs. 7.51); CES-D: controls (32.51 vs. 35.95) treatment (33.01 vs. 38.90). (Private) | NA | The system identifies significant behavioral changes by monitoring patterns in ADLs, generating an alert. Compared to controls without RAM, the RAM system did not significantly affect caregiving outcomes over a 6-month period. Themes of caregiver characteristics, care recipient characteristics and living arrangements were identified by qualitative analysis. |
| Lazarou I et al., 2019 [25] | RPT | 18 patients (12 with MCI and 6 with AD) | Xtion Pro, Plugwise, Wireless Sensor Tag System, Presence sensors, Withings Aura, Jawbone | Wrist | Ambient sensor, accelerometer | Infrared, depth, temperature, humidity/moisture, light, pressure, acceleration force | Standard neuropsychological assessment, GDS, PSS, and NPI | Improvement in experimental group RAVLT total: M(SD) 38.67(13.53) to M(SD) = 45.83(15.94), p = 0.03). Significant difference in experimental group MMSE M(SD) = 28.33(1.86) compared to non-pharmacological interventions group M(SD) = 25.33(1.51) and regular care M(SD) = 25.17(2.79). Significant difference in RAVLT-learning between experimental group (M(SD) = 9.00(4.05) and non-pharmacological interventions group (M(SD) = 4.00(1.90). Significant difference in PSS of experimental group (M(SD) = 3.83(8.2) and regular care (M(SD) = 15.33(3.50). (Private) | NA | The experimental group received tailored non-pharmacological interventions according to system observations and showed improvement in the majority of neuropsychological tests (TEA, elevator time test, TRAIL-B, RBMT-recall, BDI) and statistically significant improvement in cognitive function, sleep quality, and daily activity compared to both control groups (tailored non-pharmacological interventions based on self-reported symptoms vs. neither system installation nor interventions) |
| Vahia IV et al., 2020 [24] | CR | 1 patient with AD | The Emerald device (Commercialized) | NA | Radio signal sensor | Radio signals | Positional data, motion episodes (a segment of uninterrupted motion of ≥6 feet in one direction) | Mean motion episodes per day across all days = 82.7 (SD = 35.8). Significant (paired t test, p < 0.05) increase in motion episodes on days with family visits (93.8 (SD = 30.4) vs. non visit days 80.9 (SD = 36.3). Average 13.7% increase in motion episodes on visit days compared to the prior day and a 29.9% increase compared to the subsequent day. (Private) | NA | “The Emerald device” helps to identify behavioral symptoms of dementia on a day-to-day basis, while staff logs on patient behavior did not generate comparable temporally detailed information on behavior. The device transmitted 96.2% of data with no adverse events. Data may help identify and preempt triggers for BPSD. |
| Abujrida H et al., 2020 [20] | CS | 152 patients with PD, 304 healthy controls | NA | NA | Smartphone sensor (accelerometer, gyroscope, pedometer) | Acceleration, angular velocity | Statistical, time, wavelet, and frequency domain features, and other lifestyle features | Gait features which decrease prediction error (MSE) in classification: (1) Entropy rate for walking balance severity (2) Lifestyle features and multiple gyroscope features for shaking/tremor, and (3) Accelerometer and gyroscope features for FoG Entropy rate and minMaxDiff (differences in step swing captured with accelerometer peaks) correlate linearly with gait severities. (Public) | Highest accuracy and AUC were (1) Random forest and entropy rate, 93% and 0.97, respectively, for walking balance; (2) Bagged trees and MinMaxDiff, 95% and 0.92 respectively, for shaking/tremor; (3) Bagged trees and entropy rate, 98% and 0.98 respectively, for FoG; and (4) Random forest and MinMaxDiff, 95% and 0.99 respectively, for distinguishing PD patients from HC False positive rate of classification is significantly higher if lifestyle features are not included. | Feature importance calculation based on machine learning is a better measure of feature significance Through machine learning classification of smartphone sensor data of PD gait anomalies collected in the home environment, the stage and severity of PD can be inferred. |
| Dominey T et al., 2020 [21] | CS | 166 patients with PD | Parkinson’s KinetiGraph (PKG™) (Commercialized) | Wrist | Accelerometer | Acceleration force | Bradykinesia, dyskinesia, percentage of time with tremor, and percentage of time immobile | Most frequently reported findings in both follow-up and new patients were bradykinesia (63% and 72%, respectively) and sleep disturbance (58% and 41%, respectively). Treatment recommendations were made in 152/166 (92%) patients. Treatment recommendations were implemented for 83/114 (73%) patients, with advanced therapy in 6/9 (67%), additional motor agent in 34/71 (48%) and additional non-motor agent in 16/28 (57%). (Private) | NA | PKG™ indices with detection threshold for undertreatment were determined. The most common treatment changes relating to dopamine replacement and advice on sleep hygiene and bowel management. The study highlighted opportunities and challenges associated with incorporating digital data into care traditionally delivered via in-person contact. |
| Lipsmeier F et al., 2022 [22] | CS | 316 subjects with PD | NA | Wrist | Smartphone/Smartwatch | Acceleration force | Bradykinesia, bradyphrenia and speech, tremor, gait, and balance | All pre-specified sensor features exhibited good-to-excellent test-retest reliability (median intraclass correlation coefficient = 0.9), and correlated with corresponding UPDRS items (rho: 0.12–0.71). Strongest correlations between sensor features and corresponding clinical items are observed with bradykinesia sensor features (Hand Turning and Finger Tapping), postural and rest tremor sensor features. Weakest correlations were found with the Balance and Draw A Shape tests. 15/17 sensor features discriminated participants with UPDRS scores of 0 vs. 1. 13/17 sensor features discriminated participants with H&Y stage I vs. II. (Private) | NA | The study demonstrated the preliminary reliability and validity of remote at-home quantification of motor sign severity with Roche PD Mobile application to assess motor signs in early PD and related movement disorders. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, J.M.; Lim, J.H. A Clinical Perspective on Bespoke Sensing Mechanisms for Remote Monitoring and Rehabilitation of Neurological Diseases: Scoping Review. Sensors 2023, 23, 536. https://doi.org/10.3390/s23010536
Yen JM, Lim JH. A Clinical Perspective on Bespoke Sensing Mechanisms for Remote Monitoring and Rehabilitation of Neurological Diseases: Scoping Review. Sensors. 2023; 23(1):536. https://doi.org/10.3390/s23010536
Chicago/Turabian StyleYen, Jia Min, and Jeong Hoon Lim. 2023. "A Clinical Perspective on Bespoke Sensing Mechanisms for Remote Monitoring and Rehabilitation of Neurological Diseases: Scoping Review" Sensors 23, no. 1: 536. https://doi.org/10.3390/s23010536