
Comparison of a Wearable Accelerometer/Gyroscopic, Portable Gait Analysis System (LEGSYS+TM) to the Laboratory Standard of Static Motion Capture Camera Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
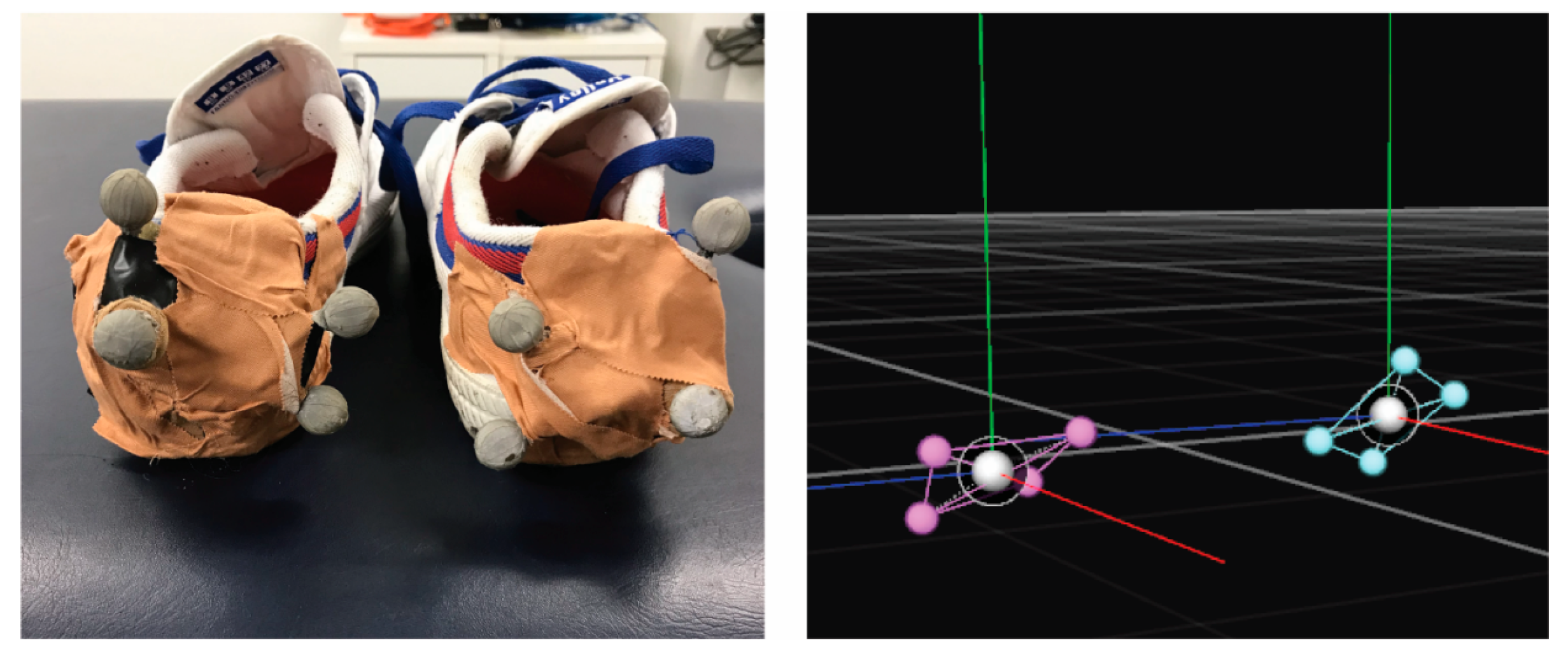
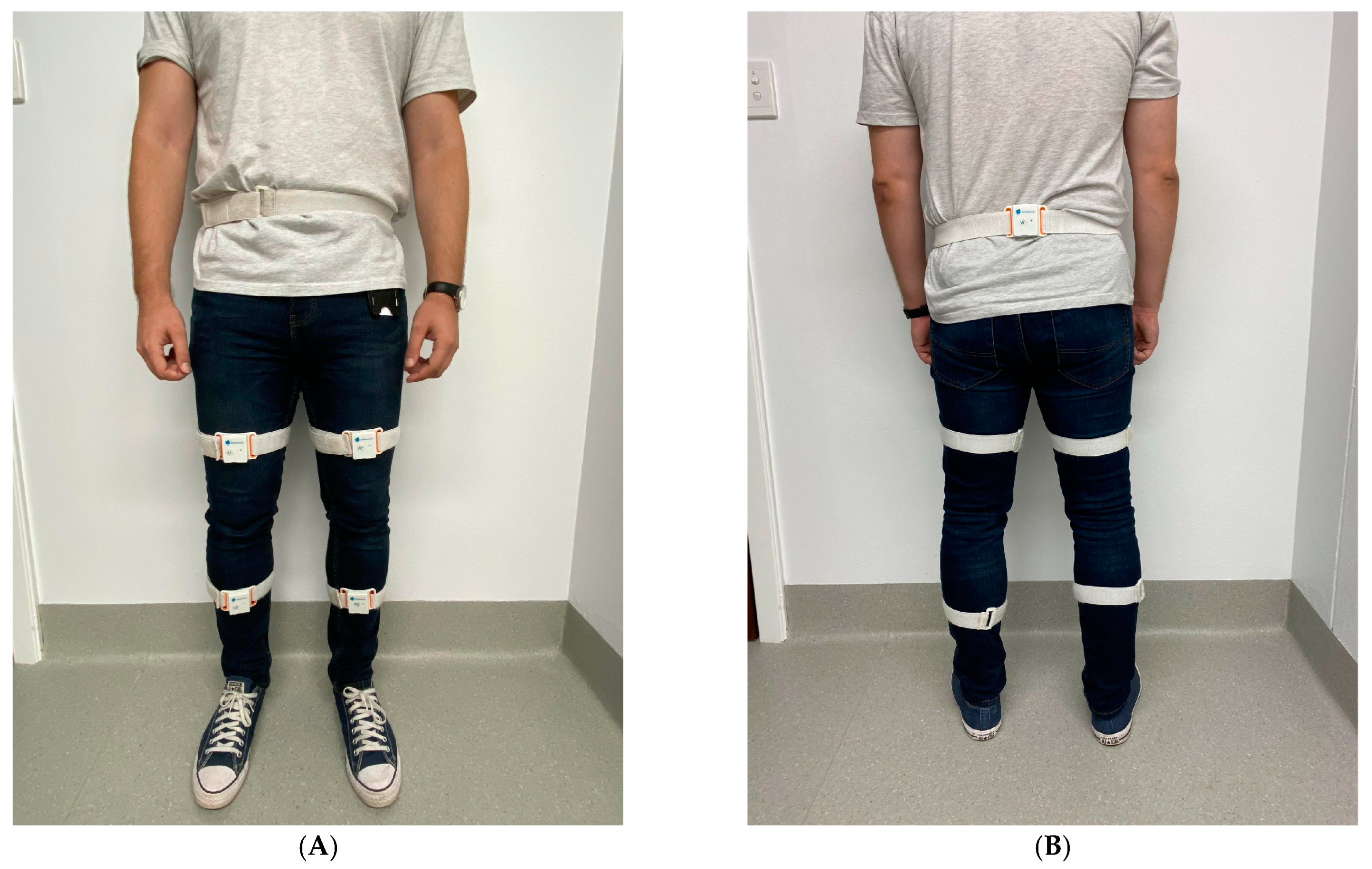
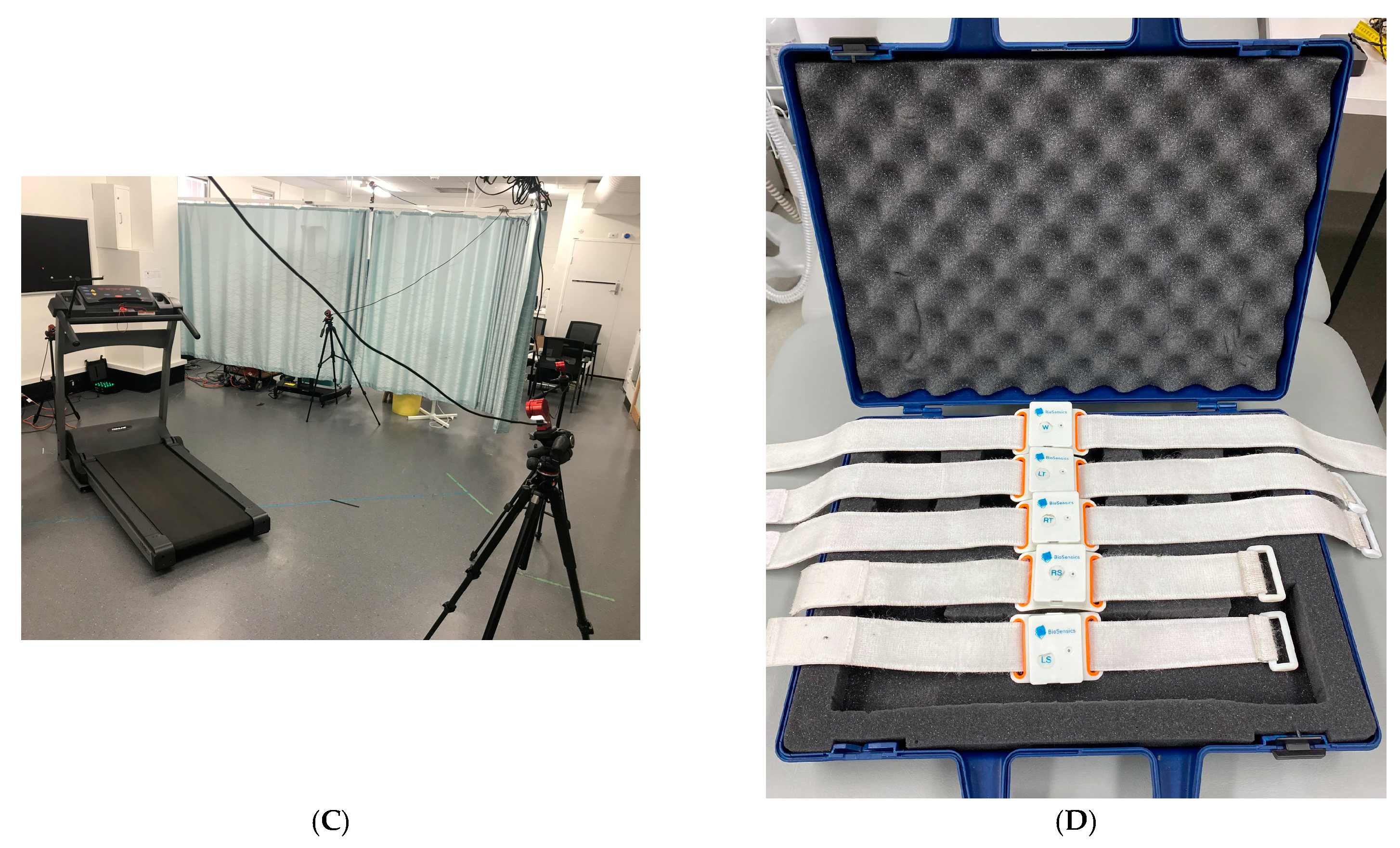
2.2. Experimental Setup
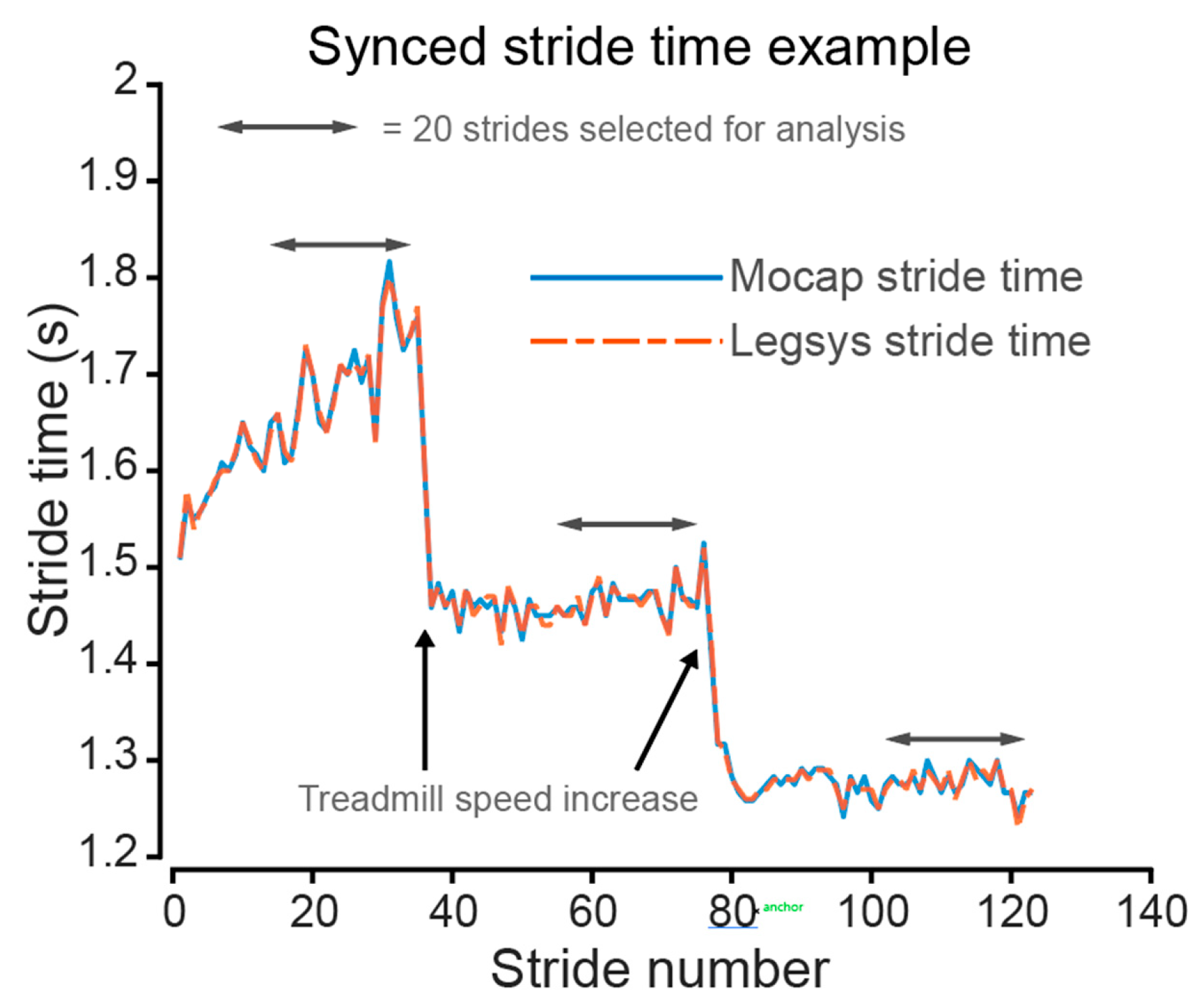
2.3. Stride Comparison between Systems
2.4. Statistical Analysis
3. Results
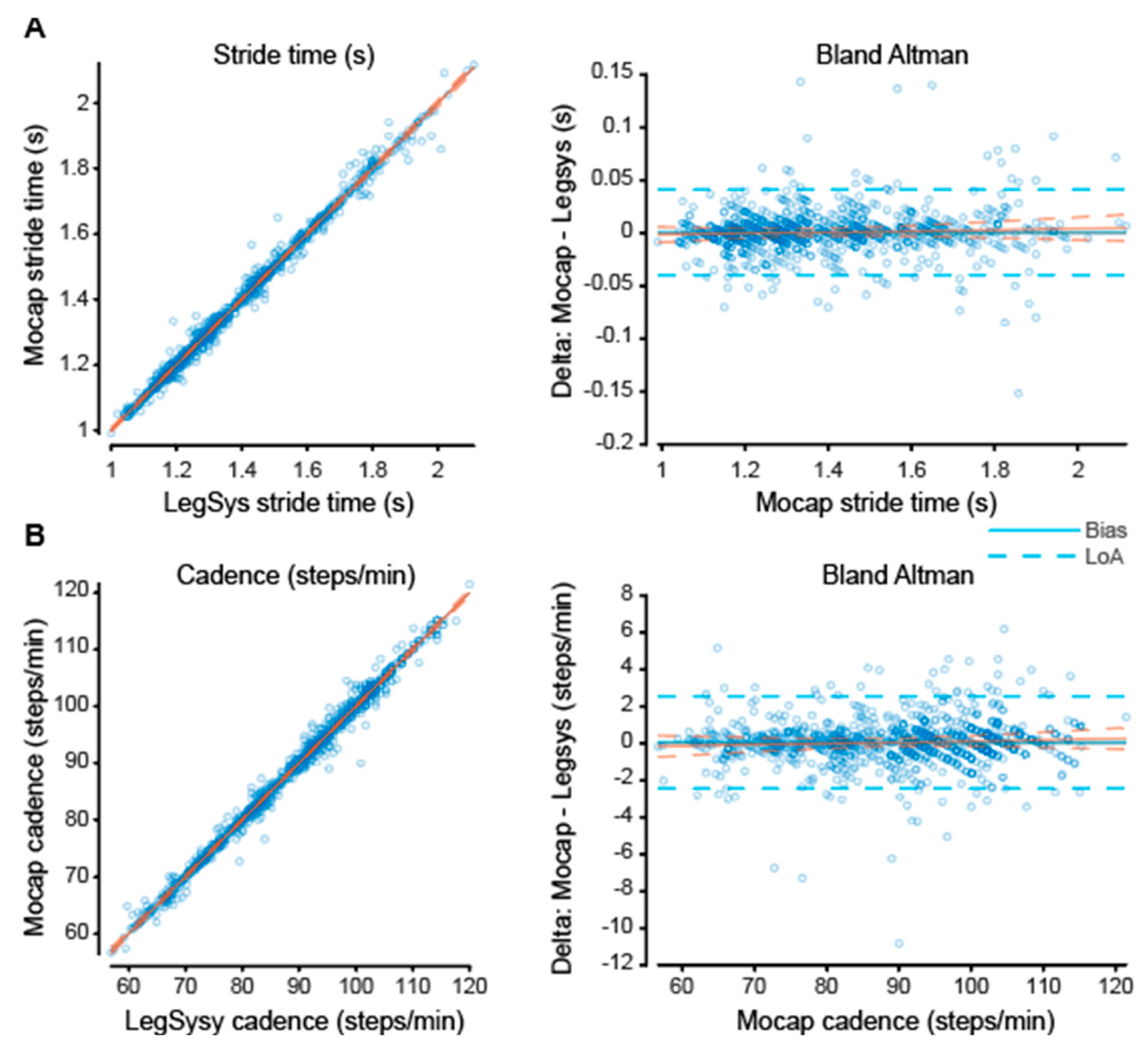
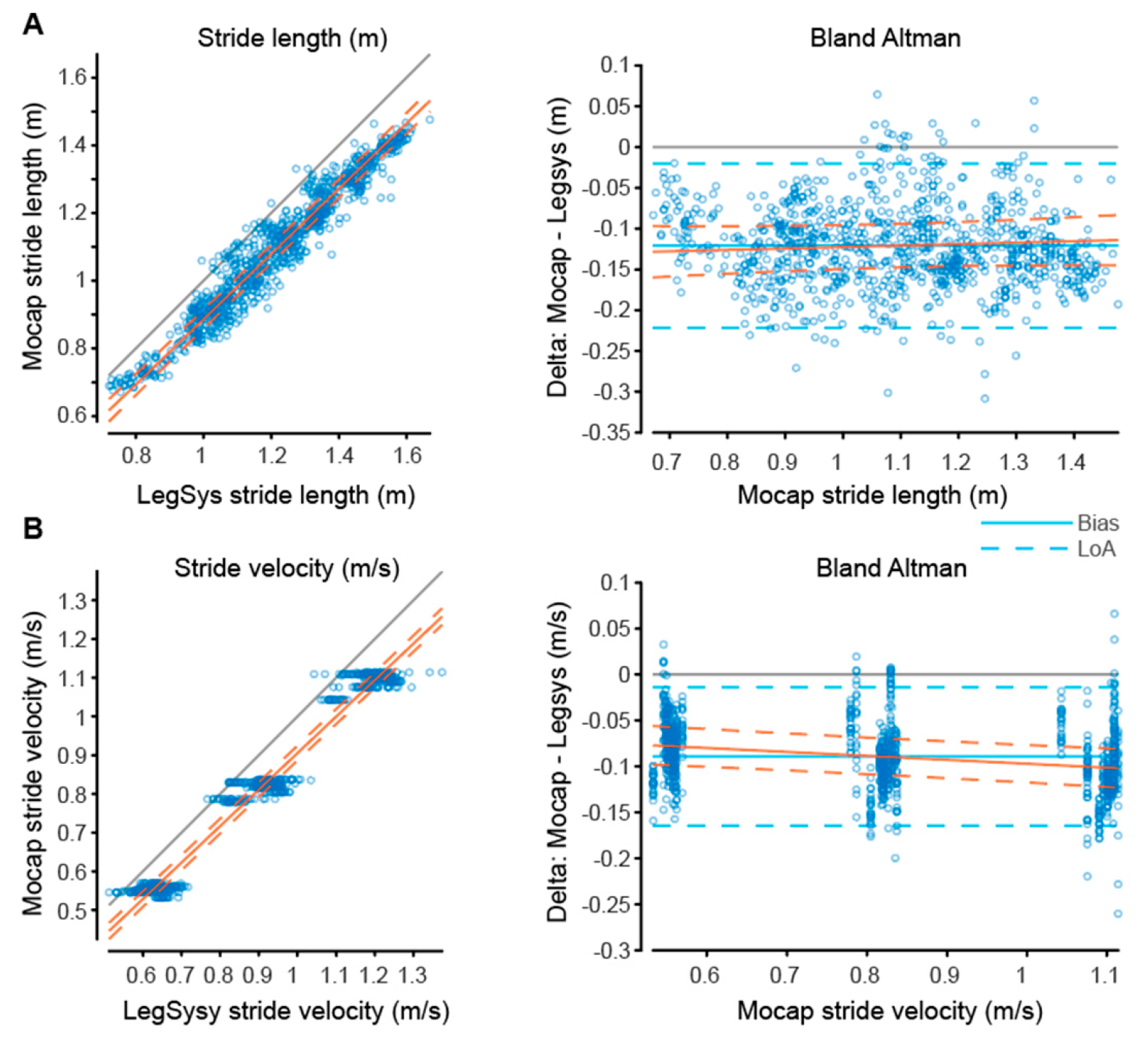
3.1. Stride Gait Parameters
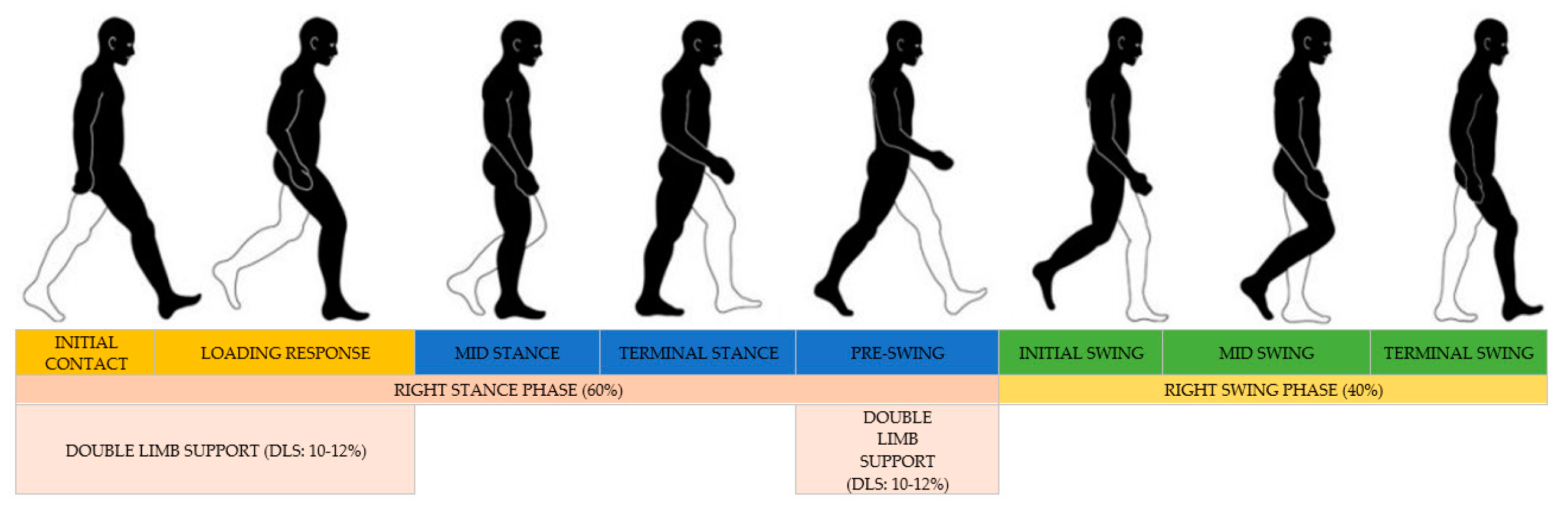
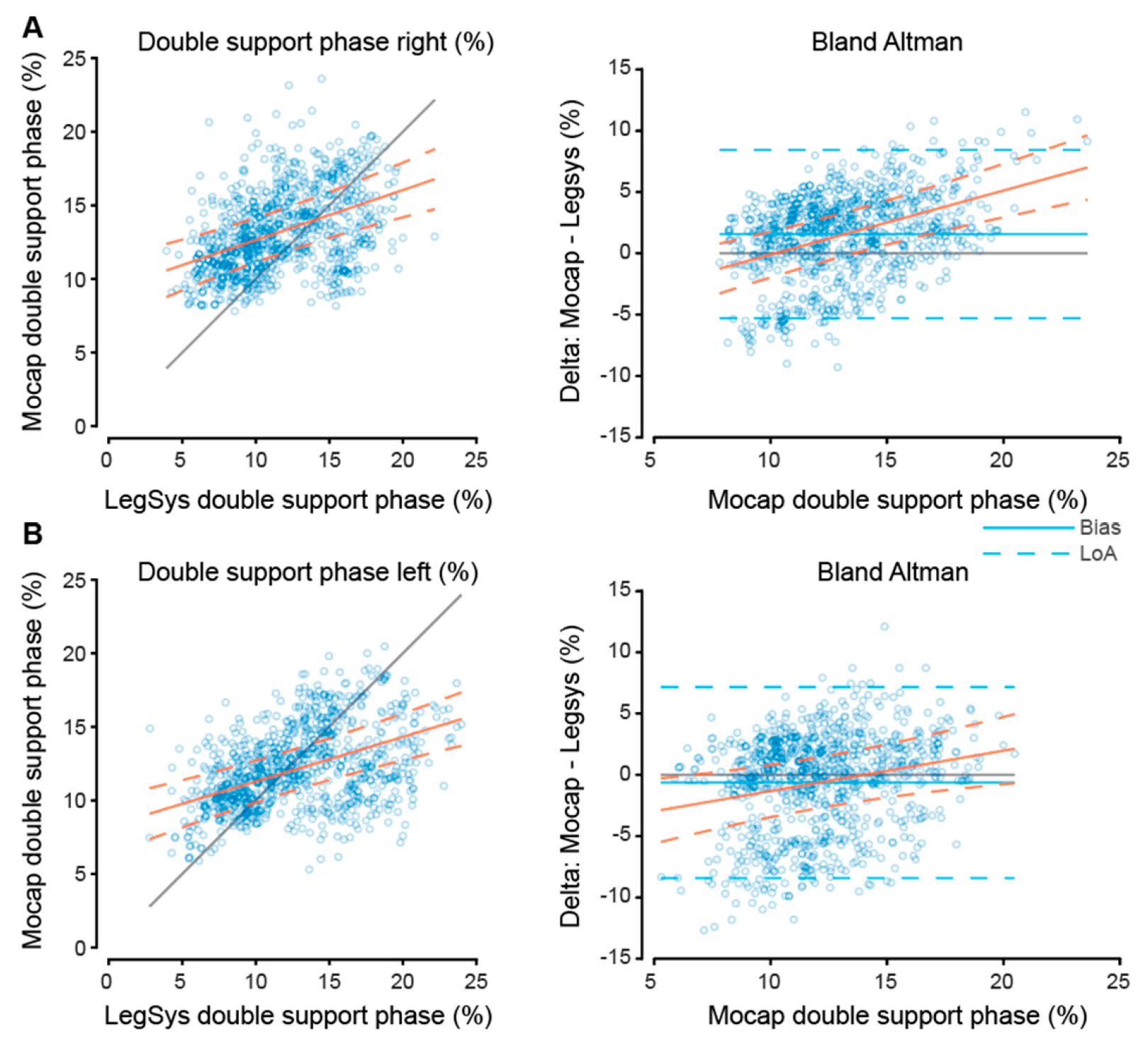
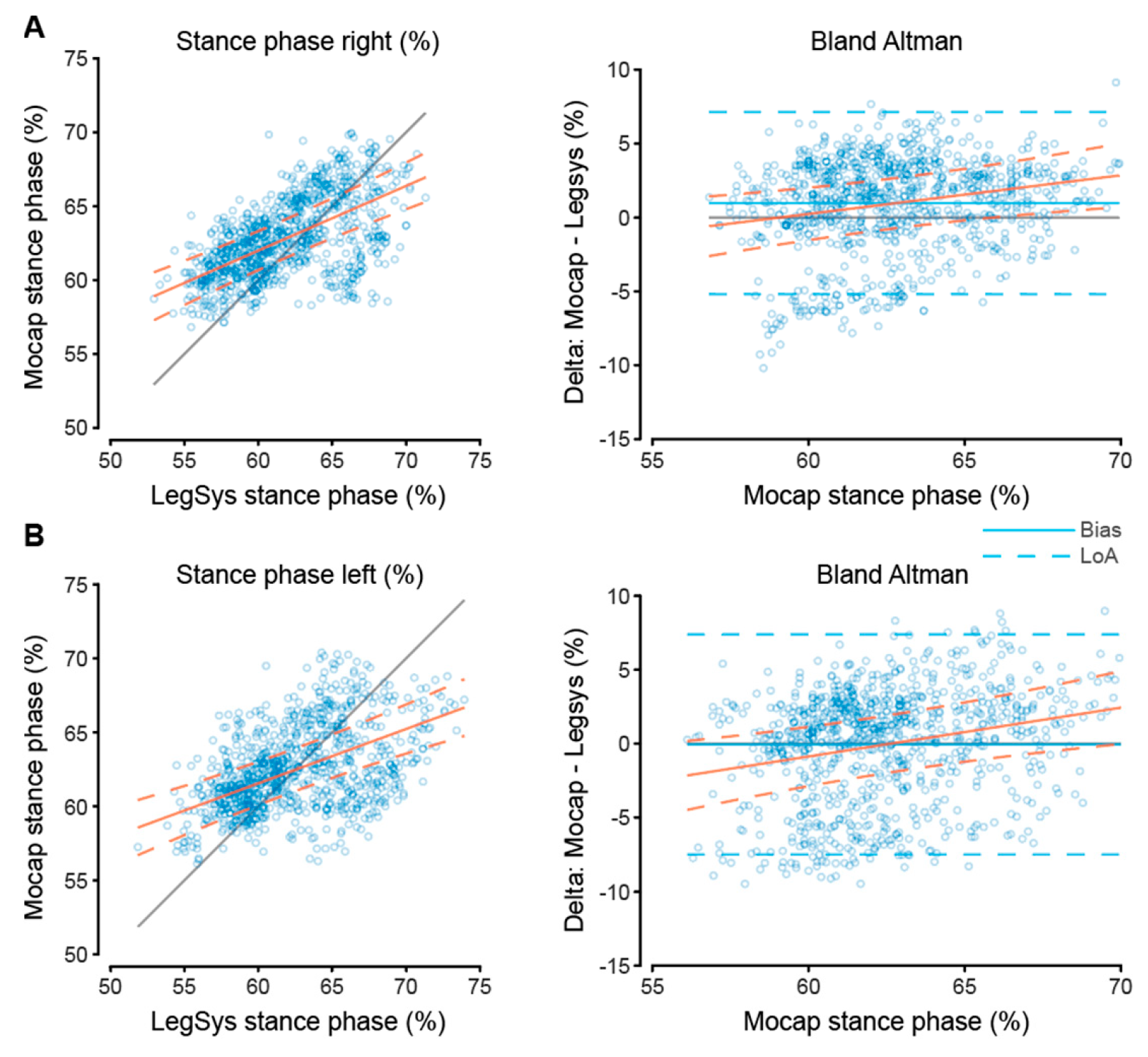
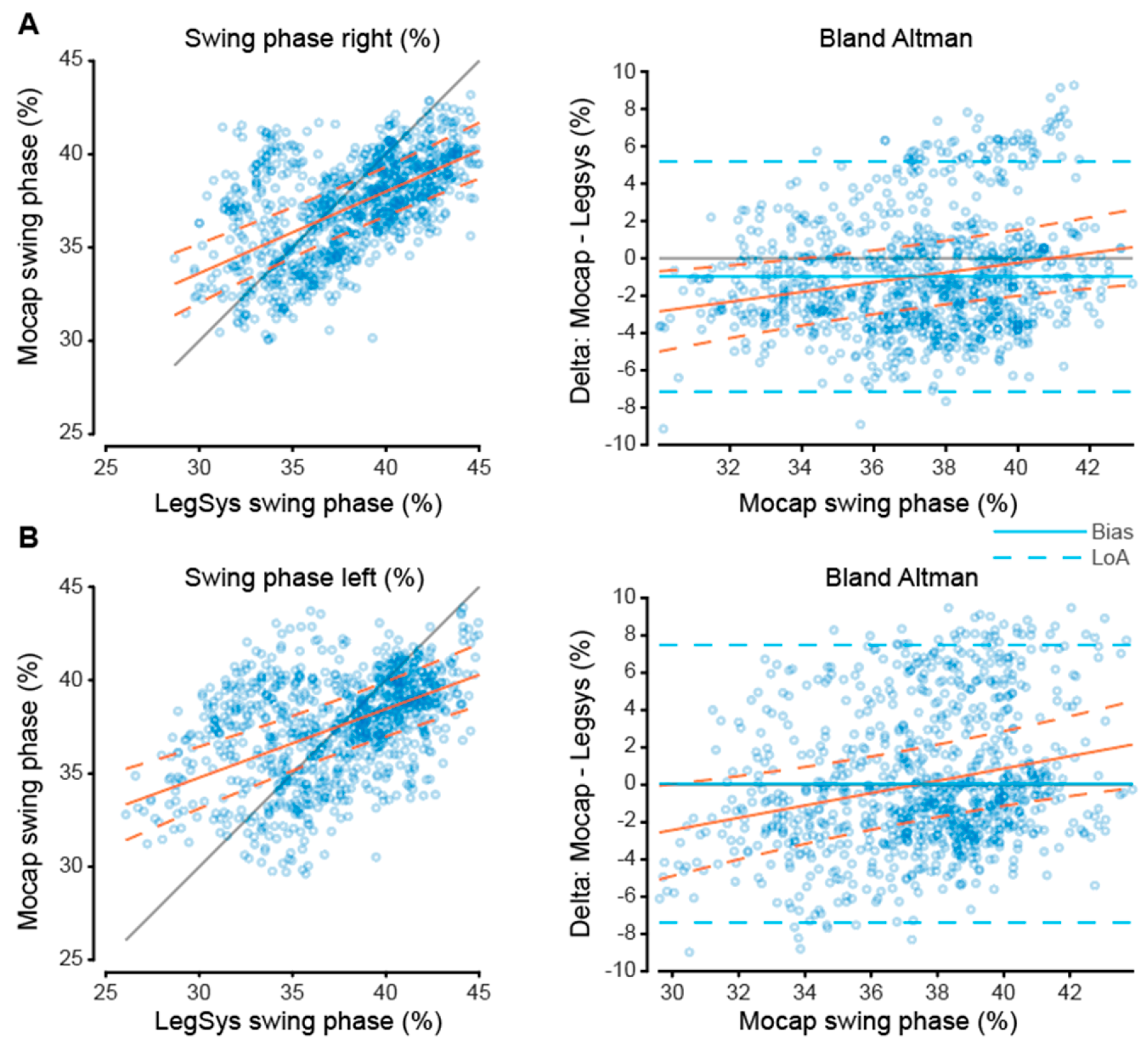
3.2. Phase Gait Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A




References
- Rydwik, E.; Bergland, A.; Forsén, L.; Frändin, K. Investigation into the reliability and validity of the measurement of elderly people’s clinical walking speed: A systematic review. Physiother Theory Pract. 2012, 28, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Moberg, L.; Svantesson, U.; Sundbom, A.; Johansson, H.; Emtner, M. Measuring walking speed in COPD: Test-retest reliability of the 30-metre walk test and comparison with the 6-minute walk test. Prim. Care Respir. J. 2011, 20, 434–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Filip, J.; Long, E. Short-distance walking speed tests in people with Parkinson disease: Reliability, responsiveness, and validity. Gait Posture 2014, 39, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Dajczman, E.; Wardini, R.; Kasymjanova, G.; Préfontaine, D.; Baltzan, M.A.; Wolkove, N. Six minute walk distance is a predictor of survival in patients with chronic obstructive pulmonary disease undergoing pulmonary rehabilitation. Can. Respir. J. 2015, 22, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Papaioannou, A.I.; Loukides, S.; Gourgoulianis, K.I.; Kostikas, K. Global assessment of the COPD patient: Time to look beyond FEV1? Respir. Med. 2009, 103, 650–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimenta, D.; Araújo, M.J.; Ortiga, R.; Vieira, A.L.; Rolo, R.; Ferreira, L. Predictive factors for readmission of patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease and respiratory failure. ERJ Open Res. 2020, 6, 40. [Google Scholar] [CrossRef]
- Miyamoto, S.; Nagaya, N.; Satoh, T.; Kyotani, S.; Sakamaki, F.; Fujita, M.; Nakanishi, N.; Miyatake, K. Clinical Correlates and Prognostic Significance of Six-minute Walk Test in Patients with Primary Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 2000, 161, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zielińska, D.; Bellwon, J.; Rynkiewicz, A.; Elkady, M.A. Prognostic value of the six-minute walk test in heart failure patients undergoing cardiac surgery: A literature review. Rehabil. Res. Pract. 2013, 2013, 965494. [Google Scholar] [CrossRef]
- Amerinatanzi, A.; Zamanian, H.; Shayesteh Moghaddam, N.; Jahadakbar, A.; Elahinia, M. Application of the Superelastic NiTi Spring in Ankle Foot Orthosis (AFO) to Create Normal Ankle Joint Behavior. Bioengineering 2017, 4, 95. [Google Scholar] [CrossRef]
- Castell, M.-V.; Sánchez, M.; Julián, R.; Queipo, R.; Martín, S.; Otero, Á. Frailty prevalence and slow walking speed in persons age 65 and older: Implications for primary care. BMC Fam. Pract. 2013, 14, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero-Odasso, M.; Schapira, M.; Soriano, E.R.; Varela, M.; Kaplan, R.; Camera, L.A.; Mayorga, L.M. Gait Velocity as a Single Predictor of Adverse Events in Healthy Seniors Aged 75 Years and Older. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 1304–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, J.; Ho, S.C.; Yu, A.L.M. Walking Speed and Stride Length Predicts 36 Months Dependency, Mortality, and Institutionalization in Chinese Aged 70 And Older. J. Am. Geriatr. Soc. 1999, 47, 1257–1260. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T.; Gosselink, R.; Decramer, M. Short- and long-term effects of outpatient rehabilitation in patients with chronic obstructive pulmonary disease: A randomized trial. Am. J. Med. 2000, 109, 207–212. [Google Scholar] [CrossRef]
- Tutic, M.; Bloch, K.E.; Lardinois, D.; Brack, T.; Russi, E.W.; Weder, W. Long-term results after lung volume reduction surgery in patients with α1-antitrypsin deficiency. J. Thorac. Cardiovasc. Surg. 2004, 128, 408–413. [Google Scholar] [CrossRef] [Green Version]
- Wilkens, H.; Demertzis, S.; Konig, J.; Leitnaker, C.k.; Schafers, H.j.; Sybrecht, G.W. Lung volume reduction surgery versus conservative treatment in severe emphysema. Eur. Respir. J. 2000, 16, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Troosters, T.; Vilaro, J.; Rabinovich, R.; Casas, A.; Barbera, J.A.; Rodriguez-Roisin, R.; Roca, J. Physiological responses to the 6-min walk test in patients with chronic obstructive pulmonary disease. Eur. Respir. J. 2002, 20, 564–569. [Google Scholar] [CrossRef] [Green Version]
- Ten Haaf, D.S.M.; Nuijten, M.A.H.; Maessen, M.F.H.; Horstman, A.M.H.; Eijsvogels, T.M.H.; Hopman, M.T.E. Effects of protein supplementation on lean body mass, muscle strength, and physical performance in nonfrail community-dwelling older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2018, 108, 1043–1059. [Google Scholar] [CrossRef] [PubMed]
- Bytyçi, I.; Henein, M.Y. Stride Length Predicts Adverse Clinical Events in Older Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2670. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.N. Stride length regulation in Parkinson’s disease: The use of extrinsic, visual cues. Brain 2000, 123, 2077–2090. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Ability to modulate walking cadence remains intact in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1532–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Stride length regulation in Parkinson’s disease. Brain 1996, 119, 551–568. [Google Scholar] [CrossRef] [Green Version]
- Bayle, N.; Patel, A.S.; Crisan, D.; Guo, L.J.; Hutin, E.; Weisz, D.J.; Moore, S.T.; Gracies, J.-M. Contribution of Step Length to Increase Walking and Turning Speed as a Marker of Parkinson’s Disease Progression. PLoS ONE 2016, 11, e0152469. [Google Scholar] [CrossRef] [PubMed]
- Item-Glatthorn, J.F.; Maffiuletti, N.A. Clinical assessment of spatiotemporal gait parameters in patients and older adults. J. Vis. Exp. 2014, e51878. [Google Scholar] [CrossRef] [Green Version]
- Sung, P.S. Increased double limb support times during walking in right limb dominant healthy older adults with low bone density. Gait Posture 2018, 63, 145–149. [Google Scholar] [CrossRef]
- Cubit, K.A.; Meyer, C. Aging in Australia. Gerontologist 2011, 51, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Alvarez, A.; Trivino, G. Linguistic description of the human gait quality. Eng. Appl. Artif. Intell. 2013, 26, 13–23. [Google Scholar] [CrossRef]
- Umberger, B.R. Stance and swing phase costs in human walking. J. R. Soc. Interface 2010, 7, 1329–1340. [Google Scholar] [CrossRef]
- Stockel, T.; Jacksteit, R.; Behrens, M.; Skripitz, R.; Bader, R.; Mau-Moeller, A. The mental representation of the human gait in young and older adults. Front. Psychol. 2015, 6, 943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najafi, B.; Khan, T.; Wrobel, J. Laboratory in a box: Wearable sensors and its advantages for gait analysis. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar]
- Iragorri, N.; Spackman, E. Assessing the value of screening tools: Reviewing the challenges and opportunities of cost-effectiveness analysis. Public Health Rev. 2018, 39, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muro-de-la-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarnita, D.; Geonea, I.; Petcu, A.; Tarnita, D.N. Numerical Simulations and Experimental Human Gait Analysis Using Wearable Sensors. New Trends Med. Serv. Robot. 2017, 289–304. [Google Scholar] [CrossRef]
- He, Y.; Wu, D.; Zhou, M.; Zheng, Y.; Wang, T.; Lu, C.; Zhang, L.; Liu, H.; Liu, C. Wearable Strain Sensors Based on a Porous Polydimethylsiloxane Hybrid with Carbon Nanotubes and Graphene. ACS Appl. Mater. Interfaces 2021, 13, 15572–15583. [Google Scholar] [CrossRef]
- Rouhani, H.; Favre, J.; Crevoisier, X.; Aminian, K. Measurement of Multi-segment Foot Joint Angles During Gait Using a Wearable System. J. Biomech. Eng. 2012, 134, 061006. [Google Scholar] [CrossRef]
- Tarniţă, D.; Calafeteanu, D.; Matei, I.; Tarnita, D. Experimental Measurement of Flexion-Extension in Normal and Osteoarthritic Knee during Sit-to-Stand Movement. Appl. Mech. Mater. 2014, 658, 520–525. [Google Scholar] [CrossRef]
- Zijlstra, A.; Goosen, J.H.M.; Verheyen, C.C.P.M.; Zijlstra, W. A body-fixed-sensor based analysis of compensatory trunk movements during unconstrained walking. Gait Posture 2008, 27, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Dozza, M.; Peterka, R.; Chiari, L.; Wall, C., 3rd. Vibrotactile biofeedback improves tandem gait in patients with unilateral vestibular loss. Ann. N. Y. Acad. Sci. 2009, 1164, 279–281. [Google Scholar] [CrossRef] [Green Version]
- Adkin, A.L.; Bloem, B.R.; Allum, J.H.J. Trunk sway measurements during stance and gait tasks in Parkinson’s disease. Gait Posture 2005, 22, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, S.; Benbasat, A.Y.; Scarborough, D.M.; Krebs, D.E.; Paradiso, J.A. Gait Analysis Using a Shoe-Integrated Wireless Sensor System. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 413–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Williams Andrews, A. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef]
- Graham, J.E.; Fisher, S.R.; Bergés, I.-M.; Kuo, Y.-F.; Ostir, G.V. Walking speed threshold for classifying walking independence in hospitalized older adults. Phys. Ther. 2010, 90, 1591–1597. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Comfortable and maximum walking speed of adults aged 20–79 years: Reference values and determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pijnappels, M.; Bobbert, M.F.; van Dieën, J.H. Changes in walking pattern caused by the possibility of a tripping reaction. Gait Posture 2001, 14, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Rácz, K.; Kiss, R.M. Marker displacement data filtering in gait analysis: A technical note. Biomed. Signal Process. Control 2021, 70, 102974. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Movement; Wiley: New York, NY, USA, 2009. [Google Scholar]
- Wilkinson, G.N.; Rogers, C.E. Symbolic Description of Factorial Models for Analysis of Variance. J. R. Stat. Society. Ser. C Appl. Stat. 1973, 22, 392–399. [Google Scholar] [CrossRef]
- Zou, G.Y. Confidence interval estimation for the Bland-Altman limits of agreement with multiple observations per individual. Stat. Methods Med. Res. 2013, 22, 630–642. [Google Scholar] [CrossRef]
- de Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Arjunan, A.; Peel, N.M.; Hubbard, R.E. Gait Speed and Frailty Status in Relation to Adverse Outcomes in Geriatric Rehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 859–864. [Google Scholar] [CrossRef]
- Jung, H.-W.; Jang, I.-Y.; Lee, C.K.; Yu, S.S.; Hwang, J.K.; Jeon, C.; Lee, Y.S.; Lee, E. Usual gait speed is associated with frailty status, institutionalization, and mortality in community-dwelling rural older adults: A longitudinal analysis of the Aging Study of Pyeongchang Rural Area. Clin. Interv. Aging 2018, 13, 1079–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aich, S.; Pradhan, P.M.; Chakraborty, S.; Kim, H.-C.; Kim, H.-T.; Lee, H.-G.; Kim, I.H.; Joo, M.-i.; Jong Seong, S.; Park, J. Design of a Machine Learning-Assisted Wearable Accelerometer-Based Automated System for Studying the Effect of Dopaminergic Medicine on Gait Characteristics of Parkinson’s Patients. J. Healthc. Eng. 2020, 2020, 1823268. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Gorelick, M.; Kramers-de Quervain, I.; Bizzini, M.; Munzinger, J.P.; Tomasetti, S.; Stacoff, A. Concurrent validity and intrasession reliability of the IDEEA accelerometry system for the quantification of spatiotemporal gait parameters. Gait Posture 2008, 27, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Rantalainen, T.; Pirkola, H.; Karavirta, L.; Rantanen, T.; Linnamo, V. Reliability and concurrent validity of spatiotemporal stride characteristics measured with an ankle-worn sensor among older individuals. Gait Posture 2019, 74, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Peruzzi, A.; Della Croce, U.; Cereatti, A. Estimation of stride length in level walking using an inertial measurement unit attached to the foot: A validation of the zero velocity assumption during stance. J. Biomech. 2011, 44, 1991–1994. [Google Scholar] [CrossRef]
- Hollman, J.H.; Childs, K.B.; McNeil, M.L.; Mueller, A.C.; Quilter, C.M.; Youdas, J.W. Number of strides required for reliable measurements of pace, rhythm and variability parameters of gait during normal and dual task walking in older individuals. Gait Posture 2010, 32, 23–28. [Google Scholar] [CrossRef]
- Riva, F.; Bisi, M.C.; Stagni, R. Gait variability and stability measures: Minimum number of strides and within-session reliability. Comput. Biol. Med. 2014, 50, 9–13. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Limits of Agreement (Low) | Limits of Agreement (High) | Bias | |
|---|---|---|---|
| Stride Measures | |||
| Stride Time (s) | −0.04 | 0.04 | 0.001 |
| Stride Length (m) | −0.22 | −0.02 | −0.12 |
| Stride Velocity (m/s) | −0.16 | −0.01 | −0.09 |
| Cadence (steps/min) | −2.43 | 2.55 | 0.06 |
| Phase Measures | |||
| Left Swing Phase | −7.39 | 7.49 | 0.05 |
| Right Swing Phase | −7.14 | 5.19 | −0.97 |
| Left Stance Phase | −7.49 | 7.39 | −0.05 |
| Right Stance Phase | −5.19 | 7.14 | 0.97 |
| Left Double Stance Phase | −8.43 | 7.18 | −0.63 |
| Right Double Stance Phase | −5.29 | 8.43 | 1.57 |
| Intercept (Upper CI, Lower CI) | Intercept p-Value | LEGSYS+ Slope (Upper CI, Lower CI) | LEGSYS+ Slope p-Value | R2 | |
|---|---|---|---|---|---|
| Stride Measures | |||||
| Stride Time (s) | 0.005 (−0.003, 0.01) | 0.24 | 0.99 (0.99, 1) | p < 0.001 | 0.99 |
| Stride Length (m) | −0.08 (−0.1, −0.05) | 4.70 × 10−11 | 0.96 (0.95, 0.97) | p < 0.001 | 0.96 |
| Stride Velocity (m/s) | −0.04 (−0.05, −0.02) | 3.65 × 10−9 | 0.94 (0.93, 0.95) | p < 0.001 | 0.98 |
| Cadence (steps/min) | 0.31 (−0.25, 0.88) | 0.28 | 0.99 (0.99, 1) | p < 0.001 | 0.99 |
| Phase Measures | |||||
| Left Swing Phase | 23.77 (22.07, 25.44) | 3.33 × 10−123 | 0.37 (0.33, 0.41) | 1.20 × 10−58 | 0.40 |
| Right Swing Phase | 20.49 (18.85, 22.14) | 3.62 × 10−102 | 0.44 (0.40, 0.48) | 1.40 × 10−80 | 0.46 |
| Left Stance Phase | 39.52 (36.84, 42.20) | 7.30 × 10−132 | 0.37 (0.33, 0.41) | 1.20 × 10−58 | 0.40 |
| Right Stance Phase | 35.74 (33.16, 38.31) | 4.37 × 10−120 | 0.44 (0.40, 0.48) | 1.40 × 10−80 | 0.46 |
| Left Double Stance Left Phase | 8.25 (7.43, 9.07) | 5.43 × 10−73 | 0.30 (0.26, 0.34) | 1.75 × 10−47 | 0.39 |
| Right Double Stance Phase | 9.24 (8.4, 10.07) | 1.27 × 10−84 | 0.34 (0.29, 0.39) | 1.33 × 10−37 | 0.33 |
| Intercept (Upper CI, Lower CI) | Intercept p-Value | LEGSYS+ Slope (Upper CI, Lower CI) | LEGSYS+ Slope p-Value | R2 | Standard Error of Mean (SEM) | SDC | |
|---|---|---|---|---|---|---|---|
| Stride Measures | |||||||
| Stride Time (s) | −0.007 (−0.016, 0.001) | 0.095 | 0.006 (−0.0003, 0.01) | 0.06 | 0.003 | 0.02 | 0.06 |
| Stride Length (m) | −0.14 (−0.16, −0.12) | 1.70 × 10−30 | 0.02 (0.003, 0.03) | 0.02 | 0.37 | 0.04 | 0.11 |
| Stride Velocity (m/s) | −0.05 (−0.07, −0.04) | 3.82 × 10−16 | −0.04 (−0.05, −0.03) | 2.15 × 10−20 | 0.36 | 0.03 | 0.09 |
| Cadence (steps/min) | −0.53 (−1.09, 0.03) | 0.066 | 0.007 (0.0003, 0.01) | 0.04 | 0.003 | 1.27 | 3.52 |
| Phase Measures | |||||||
| Left Swing Phase | −12.32 (−15.37, −9.27) | 6.06 × 10−15 | 0.33 (0.25, 0.41) | 4.21 × 10−17 | 0.41 | 3.00 | 8.33 |
| Right Swing Phase | −10.70 (−13.41, −7.99) | 2.46 × 10−14 | 0.26 (0.19, 0.33) | 2.16 × 10−13 | 0.33 | 2.61 | 7.25 |
| Left Stance Phase | −20.66 (−25.51, −15.80) | 2.30 × 10−16 | 0.33 (0.25, 0.41) | 4.21 × 10−17 | 0.41 | 3.00 | 8.33 |
| Right Stance Phase | −15.44 (−19.85, −11.03) | 1.21 × 10−11 | 0.26 (0.19, 0.33) | 2.16 × 10−13 | 0.33 | 2.61 | 7.25 |
| Left Double Stance Phase | −4.62 (−6.18, −3.06) | 8.09 × 10−9 | 0.33 (0.23, 0.42) | 9.23 × 10−14 | 0.38 | 3.18 | 8.82 |
| Right Double Stance Phase | −5.32 (−6.63, −4.01) | 5.83 × 10−15 | 0.52 (0.45, 0.59) | 9.51 × 10−44 | 0.41 | 2.94 | 8.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Homes, R.; Clark, D.; Moridzadeh, S.; Tosovic, D.; Van den Hoorn, W.; Tucker, K.; Midwinter, M. Comparison of a Wearable Accelerometer/Gyroscopic, Portable Gait Analysis System (LEGSYS+TM) to the Laboratory Standard of Static Motion Capture Camera Analysis. Sensors 2023, 23, 537. https://doi.org/10.3390/s23010537
Homes R, Clark D, Moridzadeh S, Tosovic D, Van den Hoorn W, Tucker K, Midwinter M. Comparison of a Wearable Accelerometer/Gyroscopic, Portable Gait Analysis System (LEGSYS+TM) to the Laboratory Standard of Static Motion Capture Camera Analysis. Sensors. 2023; 23(1):537. https://doi.org/10.3390/s23010537
Chicago/Turabian StyleHomes, Ryan, Devon Clark, Sina Moridzadeh, Danijel Tosovic, Wolbert Van den Hoorn, Kylie Tucker, and Mark Midwinter. 2023. "Comparison of a Wearable Accelerometer/Gyroscopic, Portable Gait Analysis System (LEGSYS+TM) to the Laboratory Standard of Static Motion Capture Camera Analysis" Sensors 23, no. 1: 537. https://doi.org/10.3390/s23010537