
Accuracy of Estimated Bioimpedance Parameters with Octapolar Segmental Bioimpedance Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
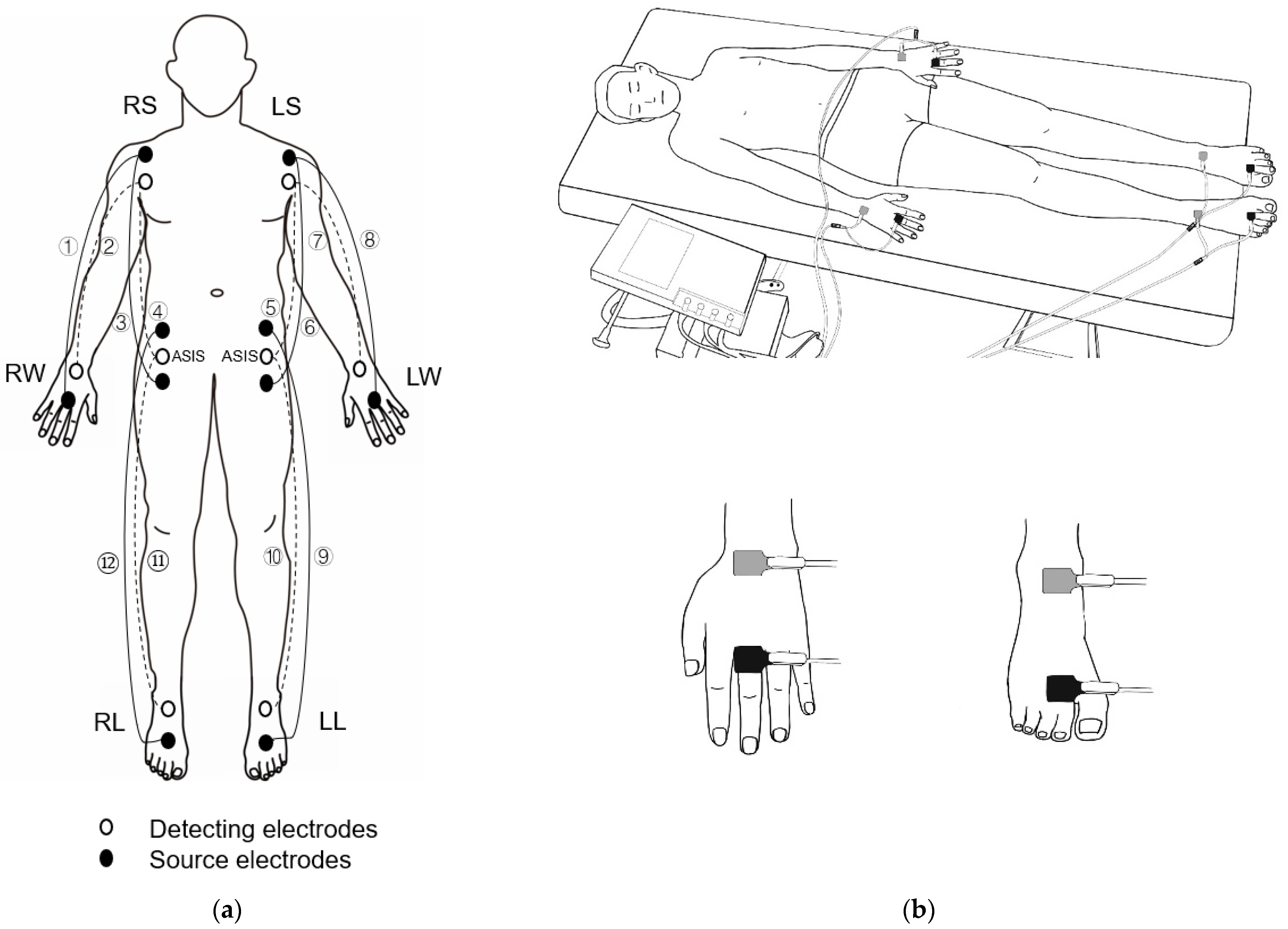
2.2. Measurement of the Direct Segmental Impedance Parameters
2.3. Assessments of Estimated Octapolar Segmental Impedance Parameters
2.4. Fat Mass and Fat-Free Mass from Dual-Energy X-ray Absorptiometry
2.5. Data Processing and Statistical Analysis
3. Results
Characteristics of the Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ward, L.C. Bioelectrical impedance analysis for body composition assessment: Reflections on accuracy, clinical utility, and standardisation. Eur. J. Clin. Nutr. 2019, 73, 194–199. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.C.; Heymsfield, S.B. Bioelectrical impedance analysis for diagnosing sarcopenia and cachexia: What are we really estimating? J. Cachexia Sarcopenia Muscle 2017, 8, 187–189. [Google Scholar] [CrossRef]
- Lukaski, H.C. Evolution of bioimpedance: A circuitous journey from estimation of physiological function to assessment of body composition and a return to clinical research. Eur. J. Clin. Nutr. 2013, 67, S2–S9. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef] [Green Version]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Lilienthal Heitmann, B.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Genton, L.; Norman, K.; Spoerri, A.; Pichard, C.; Karsegard, V.L.; Herrmann, F.R.; Graf, C.E. Bioimpedance-Derived Phase Angle and Mortality Among Older People. Rejuvenation Res. 2017, 20, 118–124. [Google Scholar] [CrossRef]
- Paton, N.I.; Elia, M.; Jennings, G.; Ward, L.C.; Griffin, G.E. Bioelectrical impedance analysis in human immunodeficiency virus-infected patients: Comparison of single frequency with multifrequency, spectroscopy, and other novel approaches. Nutrition 1989, 14, 658–666. [Google Scholar] [CrossRef]
- Paixão, E.; Gonzalez, M.C.; Nakano, E.Y.; Ito, M.K.; Pizato, N. Weight loss, phase angle, and survival in cancer patients undergoing radiotherapy: A prospective study with 10-year follow-up. Eur. J. Clin. Nutr. 2021, 75, 823–828. [Google Scholar] [CrossRef]
- Zouridakis, A.; Simos, Y.V.; Verginadis, I.I.; Charalabopoulos, K.; Ragos, V.; Dounousi, E.; Boudouris, G.; Karkabounas, S.; Evangelou, A.; Peschos, D. Correlation of bioelectrical impedance analysis phase angle with changes in oxidative stress on end-stage renal disease patients, before, during, and after dialysis. Ren. Fail. 2016, 38, 738–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: Phase angle and impedance ratio. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Popiołek-Kalisz, J.; Teter, M.; Kozak, G.; Powrózek, T.; Mlak, R.; Sobieszek, G.; Karakuła-Juchnowicz, H.; Małecka-Massalska, T. Potential bioelectrical impedance analysis (BIA) parameters in prediction muscle strength in women with anorexia nervosa. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2021, 22, 203–213. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Cavalcante, E.F.; Antunes, M.; Nabuco, H.; de Souza, M.F.; Teixeira, D.C.; Gobbo, L.A.; Silva, A.M.; Cyrino, E.S. Phase Angle Is Moderately Associated with Muscle Quality and Functional Capacity, Independent of Age and Body Composition in Older Women. J. Geriatr. Phys. Ther. 2019, 42, 281–286. [Google Scholar] [CrossRef]
- Scicchitano, P.; Iacoviello, M.; Passantino, A.; Guida, P.; De Palo, M.; Piscopo, A.; Gesualdo, M.; Caldarola, P.; Massari, F. The Prognostic Impact of Estimated Creatinine Clearance by Bioelectrical Impedance Analysis in Heart Failure: Comparison of Different eGFR Formulas. Biomedicines 2021, 9, 1307. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Ciccone, M.M.; Passantino, A.; Valle, R.; De Palo, M.; Sasanelli, P.; Sanasi, M.; Piscopo, A.; Guida, P.; Caldarola, P.; et al. Congestion and nutrition as determinants of bioelectrical phase angle in heart failure. Heart Lung J. Crit. Care 2021, 49, 724–728. [Google Scholar] [CrossRef]
- Scicchitano, P.; Massari, F. Bioimpedance vector analysis in the evaluation of congestion in heart failure. Biomark. Med. 2020, 14, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, A.; Pastori, G.; Codognotto, M.; Paoli, A. Equivalence of information from single frequency v. bioimpedance spectroscopy in bodybuilders. Br. J. Nutr. 2007, 97, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Cunha, P.M.; Tomeleri, C.M.; Nascimento, M.; Nunes, J.P.; Antunes, M.; Nabuco, H.; Quadros, Y.; Cavalcante, E.F.; Mayhew, J.L.; Sardinha, L.B.; et al. Improvement of cellular health indicators and muscle quality in older women with different resistance training volumes. J. Sports Sci. 2018, 36, 2843–2848. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Ribeiro, A.S.; Cavaglieri, C.R.; Deminice, R.; Schoenfeld, B.J.; Schiavoni, D.; Dos Santos, L.; de Souza, M.F.; Antunes, M.; Venturini, D.; et al. Correlations between resistance training-induced changes on phase angle and biochemical markers in older women. Scand. J. Med. Sci. Sports 2018, 28, 2173–2182. [Google Scholar] [CrossRef]
- Langer, R.D.; Silva, A.M.; Borges, J.H.; Cirolini, V.X.; Páscoa, M.A.; Guerra-Júnior, G.; Gonçalves, E.M. Physical training over 6 months is associated with improved changes in phase angle, body composition, and blood glucose in healthy young males. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2019, 31, e23275. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Bosaeus, M.; Karlsson, T.; Holmäng, A.; Ellegård, L. Accuracy of quantitative magnetic resonance and eight-electrode bioelectrical impedance analysis in normal weight and obese women. Clin. Nutr. 2014, 33, 471–477. [Google Scholar] [CrossRef]
- Jeon, K.C.; Kim, S.Y.; Jiang, F.L.; Chung, S.; Ambegaonkar, J.P.; Park, J.H.; Kim, Y.J.; Kim, C.H. Prediction Equations of the Multifrequency Standing and Supine Bioimpedance for Appendicular Skeletal Muscle Mass in Korean Older People. Int. J. Environ. Res. Public Health 2020, 17, 5847. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Heymsfield, S.B. Bioelectrical impedance analysis in the assessment of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Biological indexes considered in the derivation of the bioelectrical impedance analysis. Am. J. Clin. Nutr. 1996, 64 (Suppl. 3), 397S–404S. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.C. Segmental bioelectrical impedance analysis: An update. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Jaffrin, M.Y.; Morel, H. Measurements of body composition in limbs and trunk using a eight contact electrodes impedance meter. Med. Eng. Phys. 2019, 31, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Mally, K.; Dittmar, M. Comparison of three segmental multifrequency bioelectrical impedance techniques in healthy adults. Ann. Hum. Biol. 2012, 39, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, A.; Pastori, G.; Guizzo, M.; Rebeschini, M.; Naso, A.; Cascone, C. Equivalence of information from single versus multiple frequency bioimpedance vector analysis in hemodialysis. Kidney Int. 2005, 67, 301–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinsley, G.M.; Harty, P.S.; Moore, M.L.; Grgic, J.; Silva, A.M.; Sardinha, L.B. Changes in total and segmental bioelectrical resistance are correlated with whole-body and segmental changes in lean soft tissue following a resistance training intervention. J. Int. Soc. Sports Nutr. 2019, 16, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm-Leen, E.R.; Hall, Y.N.; Horwitz, R.I.; Chertow, G.M. Phase Angle, frailty and Mortality in older adults. Curr. Opin. Clin. Nutr. Metab. Care. 2017, 20, 330–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, A.M.; Matias, C.N.; Nunes, C.L.; Santos, D.A.; Marini, E.; Lukaski, H.C.; Sardinha, L.B. Lack of agreement of in vivo raw bioimpedance measurements obtained from two single and multi-frequency bioelectrical impedance devices. Eur. J. Clin. Nutr. 2019, 73, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, R.F.; de Azevedo, Z.M.; Fonseca, V.M.; Peixoto, M.V.; dos Anjos, L.A.; Gaspar-Elsas, M.I.; Moore, D.C.; Ramos, E.G. Distribution of bioelectrical impedance vector values in multi-ethnic infants and pre-school children. Clin. Nutr. 2012, 31, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Chumlea, W.C.; Roche, A.F. Estimation of body composition from bioelectric impedance of body segments. Am. J. Clin. Nutr. 1989, 50, 221–226. [Google Scholar] [CrossRef]
- Organ, L.W.; Bradham, G.B.; Gore, D.T.; Lozier, S.L. Segmental bioelectrical impedance analysis: Theory and application of a new technique. J. Appl. Physiol. 1994, 77, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Nescolarde, L.; Lukaski, H.; De Lorenzo, A.; de-Mateo-Silleras, B.; Redondo-Del-Río, M.P.; Camina-Martín, M.A. Different displacement of bioimpedance vector due to Ag/AgCl electrode effect. Eur. J. Clin. Nutr. 2016, 70, 1401–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiffman, C.A. Adverse effects of near current-electrode placement in non-invasive bio-impedance measurements. Physiol. Meas. 2013, 34, 1513–1529. [Google Scholar] [CrossRef]
- Scheltinga, M.R.; Jacobs, D.O.; Kimbrough, T.D.; Wilmore, D.W. Alterations in body fluid content can be detected by bioelectrical impedance analysis. J. Surg. Res. 1991, 50, 461–468. [Google Scholar] [CrossRef]
- Hansen, E.S.; Baigent, C.; Reck, S.I.; Connor, M. Bioelectrical Impedance as a Technique for Estimating Postmortem Interval. J. Forensic Sci. 2018, 63, 1186–1190. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Men (n = 73) | Women (n = 63) | Total (n = 136) | |
|---|---|---|---|
| Age (year) | 76.5 ± 4.1 | 75.1 ± 4.0 | 75.9 ± 4.1 |
| Weight (kg) | 65.4 ± 7.1 | 54.1 ± 6.1 *** | 60.2 ± 8.7 |
| Height (cm) | 166.5 ± 4.8 | 152.2 ± 5.0 *** | 159.9 ± 8.6 |
| BMI (kg/m2) | 23.6 ± 2.2 | 23.4 ± 2.2 | 23.5 ± 2.2 |
| FFM (kg) | 49.9 ± 4.3 | 36.9 ± 3.6 *** | 43.9 ± 7.6 |
| FM (kg) | 15.5 ± 5.1 | 17.3 ± 3.9 * | 16.3 ± 4.7 |
| FFMI (kg/m2) | 18.0 ± 1.1 | 15.9 ± 1.1 *** | 17.0 ± 1.5 |
| FMI (kg/m2) | 5.6 ± 1.8 | 7.4 ± 1.6 *** | 6.5 ± 2.0 |
| %BF | 23.3 ± 6.2 | 31.6 ± 4.8 *** | 27.2 ± 6.9 |
| Zmeasured (Ω) | 458 ± 41.5 | 537 ± 47.9 *** | 495 ± 59.3 |
| Rmeasured (Ω) | 456 ± 41.5 | 535 ± 47.9 *** | 492 ± 59.4 |
| Xcmeasured (Ω) | 47.7 ± 5.3 | 48.4 ± 5.4 | 48.0 ± 5.4 |
| PhAmeasured (°) | 6.0 ± 0.6 | 5.2 ± 0.6 *** | 5.6 ± 0.7 |
| Male (n = 73) | Female (n = 63) | |||||
|---|---|---|---|---|---|---|
| Measured † | Estimated ‡ | Ratio | Measured | Estimated | Ratio | |
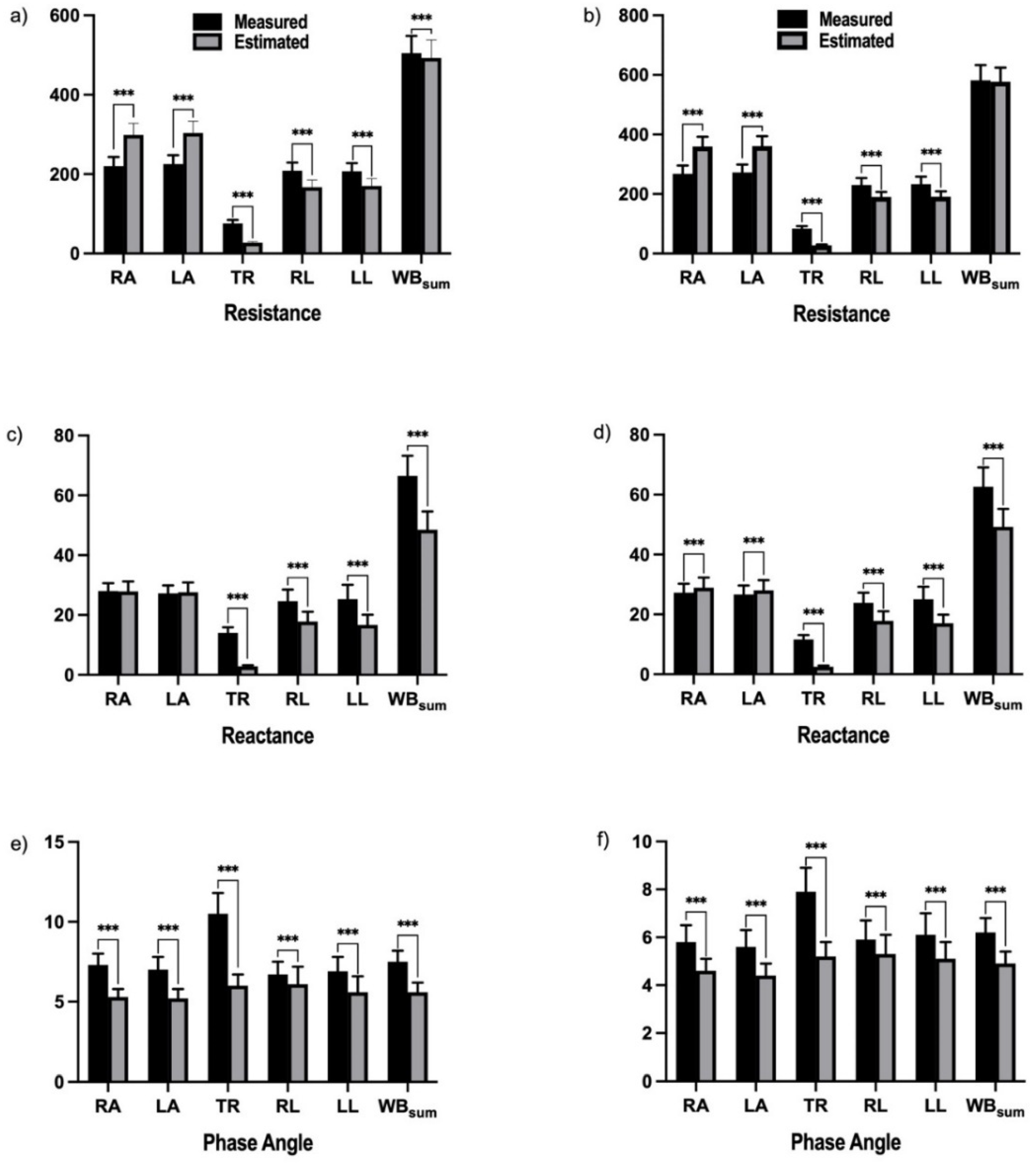
| Resistance (R, Ω) | ||||||
| RA | 220 ± 22.8 | 299 ± 29.5 *** | 1.36 ± 0.06 | 268 ± 28.3 | 360 ± 33.0 *** | 1.36 ± 0.06 |
| LA | 225 ± 22.5 | 304 ± 29.1 *** | 1.35 ± 0.06 | 272 ± 26.4 | 361 ± 33.1 *** | 1.33 ± 0.06 |
| TR | 76 ± 8.6 | 27 ± 2.7 *** | 0.36 ± 0.03 | 84 ± 8.7 | 27 ± 2.7 *** | 0.33 ± 0.03 |
| RL | 209 ± 20.7 | 167 ± 18.1 *** | 0.80 ± 0.07 | 230 ± 23.0 | 190 ± 16.4 *** | 0.83 ± 0.05 |
| LL | 207 ± 20.5 | 170 ± 18.8 *** | 0.82 ± 0.07 | 233 ± 25.0 | 191 ± 17.8 *** | 0.82 ± 0.05 |
| WBestimate | 505 ± 43.8 | 493 ± 45.5 *** | 0.98 ± 0.05 | 582 ± 51.8 | 577 ± 46.7 | 0.99 ± 0.05 |
| WBmeasure | 456 ± 41.5 | 493 ± 45.5 *** | 1.08 ± 0.04 | 535 ± 47.9 | 577 ± 46.7 *** | 1.08 ± 0.04 |
| Reactance (Xc, Ω) | ||||||
| RA | 28.0 ± 2.6 | 27.9 ± 3.3 | 1.00 ± 0.07 | 27.2 ± 3.0 | 8.9 ± 3.4 *** | 0.33 ± 0.08 |
| LA | 27.2 ± 2.7 | 27.6 ± 3.3 | 1.02 ± 0.08 | 26.6 ± 3.0 | 8.0 ± 3.4 *** | 0.30 ± 0.08 |
| TR | 14.0 ± 1.9 | 2.8 ± 0.4 *** | 0.21 ± 0.03 | 11.6 ± 1.5 | 2.5 ± 0.4 *** | 0.22 ± 0.03 |
| RL | 24.6 ± 3.9 | 17.8 ± 3.3 *** | 0.73 ± 0.13 | 23.8 ± 3.4 | 17.8 ± 3.2 *** | 0.75 ± 0.08 |
| LL | 25.3 ± 4.8 | 16.7 ± 3.4 *** | 0.66 ± 0.10 | 25.0 ± 4.2 | 17.0 ± 2.9 *** | 0.69 ± 0.10 |
| WBestimate | 66.5 ± 6.7 | 48.5 ± 6.1 *** | 0.73 ± 0.07 | 62.6 ± 6.5 | 49.5 ± 6.0 *** | 0.79 ± 0.06 |
| WBmeasure | 47.7 ± 5.3 | 48.5 ± 6.1 | 1.02 ± 0.07 | 48.4 ± 5.4 | 49.2 ± 6.0 * | 1.02 ± 0.06 |
| Phage Angle (°) | ||||||
| RA | 7.3 ± 0.7 | 5.3 ± 0.5 *** | 0.74 ± 0.05 | 5.8 ± 0.7 | 4.6 ± 0.5 *** | 0.79 ± 0.06 |
| LA | 7.0 ± 0.8 | 5.2 ± 0.6 *** | 0.76 ± 0.06 | 5.6 ± 0.7 | 4.4 ± 0.5 *** | 0.80 ± 0.06 |
| TR | 10.5 ± 1.3 | 6.0 ± 0.7 *** | 0.58 ± 0.09 | 7.9 ± 1.0 | 5.2 ± 0.6 *** | 0.66 ± 0.09 |
| RL | 6.7 ± 0.8 | 6.1 ± 1.1 *** | 0.91 ± 0.17 | 5.9 ± 0.8 | 5.3 ± 0.8 *** | 0.90 ± 0.10 |
| LL | 6.9 ± 0.9 | 5.6 ± 1.0 *** | 0.81 ± 0.11 | 6.1 ± 0.9 | 5.1 ± 0.7 *** | 0.84 ± 0.11 |
| WBestimate | 7.5 ± 0.7 | 5.6 ± 0.6 *** | 0.75 ± 0.07 | 6.2 ± 0.6 | 4.9 ± 0.5 *** | 0.79 ± 0.06 |
| WBmeasure | 6.0 ± 0.6 | 5.6 ± 0.6 *** | 0.94 ± 0.07 | 5.2 ± 0.6 | 4.9 ± 0.5 *** | 0.94 ± 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, F.; Tang, S.; Eom, J.-J.; Song, K.-H.; Kim, H.; Chung, S.; Kim, C.-H. Accuracy of Estimated Bioimpedance Parameters with Octapolar Segmental Bioimpedance Analysis. Sensors 2022, 22, 2681. https://doi.org/10.3390/s22072681
Jiang F, Tang S, Eom J-J, Song K-H, Kim H, Chung S, Kim C-H. Accuracy of Estimated Bioimpedance Parameters with Octapolar Segmental Bioimpedance Analysis. Sensors. 2022; 22(7):2681. https://doi.org/10.3390/s22072681
Chicago/Turabian StyleJiang, Fanglin, Saizhao Tang, Jin-Jong Eom, Keon-Hyoung Song, Hyeoijin Kim, Sochung Chung, and Chul-Hyun Kim. 2022. "Accuracy of Estimated Bioimpedance Parameters with Octapolar Segmental Bioimpedance Analysis" Sensors 22, no. 7: 2681. https://doi.org/10.3390/s22072681