
Exploration of an Inflection Point of Ventilation Parameters with Anaerobic Threshold Using Strucchange

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Protocol and Setup
2.3. Experimental Analysis
3. Results
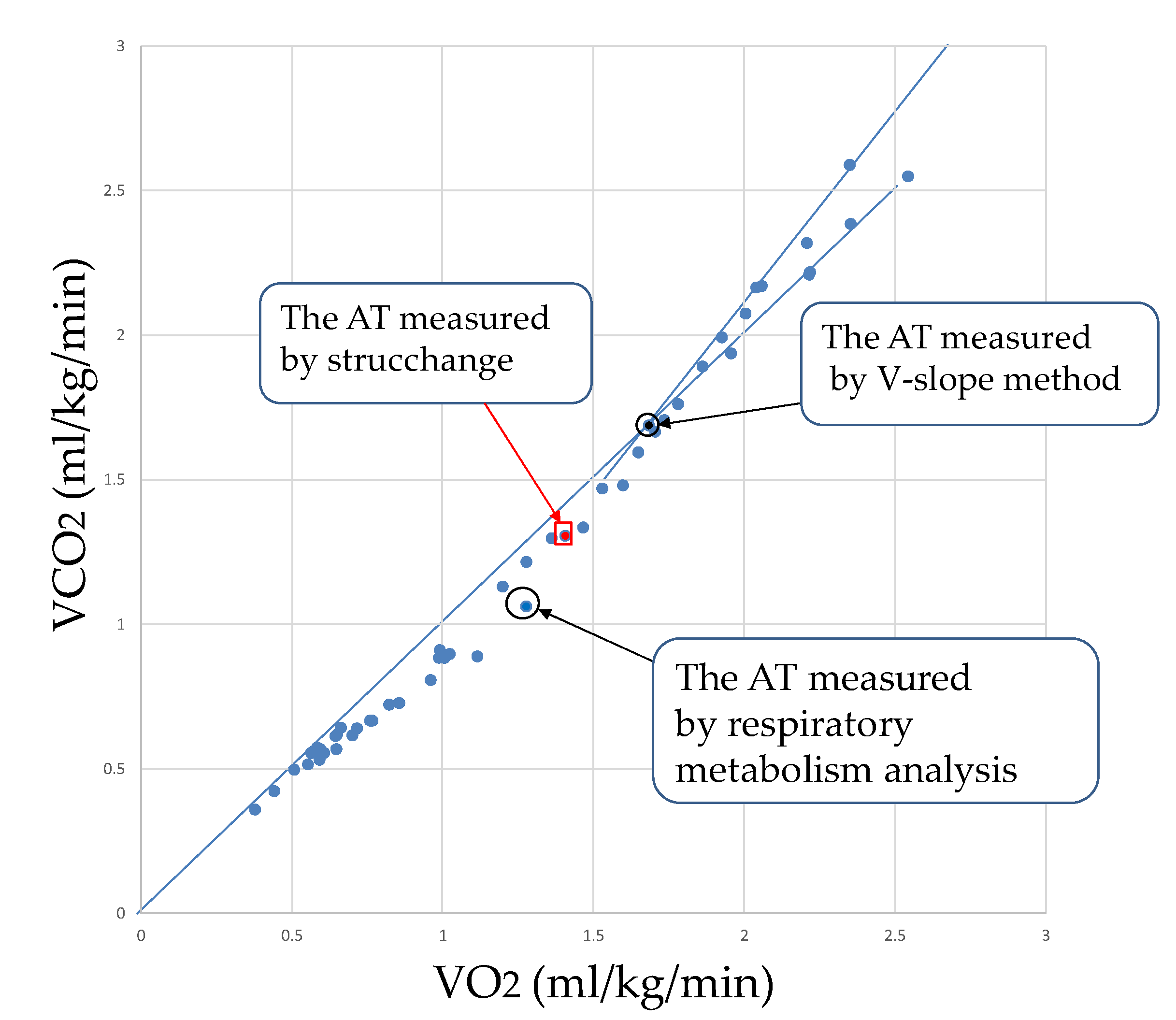
3.1. Results of V-Slope Method and Strucchange and Respiratory Metabolic Analysis
3.2. Results from Strucchange and Respiratory Metabolic Analysis
4. Discussion
4.1. Comparison between Strucchange and Respiratory Metabolic Analysis
4.2. Comparison of the V-Slope Method with Strucchange and Respiratory Metabolic Analysis
5. Conclusions
- (1)
- It was possible to detect the change point by strucchange in each ventilation index (VE, VCO2).
- (2)
- We confirmed that the results of respiratory metabolic analysis and the confidence intervals by strucchange were almost identical in VE and VCO2. The RQ results differed significantly from the two aforementioned results due to possible errors in the analysis.
- (3)
- The V-slope method was objectively evaluated using inter-examiner reliability (ICC), but the results were unreliable.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hironori, T. Coronary artery disease trends in Japan. Jpn. Circ. J. 1994, 58, 166–172. [Google Scholar]
- Finegold, J.A.; Asaria, P.; Francis, D.P. Mortality from ischaemic heart disease by country, region, and age: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2013, 168, 934–945. [Google Scholar] [CrossRef] [Green Version]
- Wannamethee, S.G.; Shaper, A.G.; Walker, M. Physical activity and mortality in old men with diagnosed coronary heart disease. Circulation 2000, 102, 1358–1363. [Google Scholar] [CrossRef] [Green Version]
- Ades, P.A. Cardiac rehabilitation and secondary prevention of coronary heart disease. N. Engl. J. Med. 2001, 345, 892–902. [Google Scholar]
- Wasserman, K.; Whipp, B.J.; Koyal, S.N.; Beaver, W.L. Anaerobic threshold and respiratory gas exchange during exercise. J. Appl. Physiol. 1973, 35, 236–243. [Google Scholar] [CrossRef]
- Takeshima, N.; Tanaka, K.; Kobayashi, F.; Watanabe, T.; Kato, T. Effects of aerobic exercise conditioning at intensities corresponding to lactate threshold in the elderly. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 138–143. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, K.; Osada, N.; Noda, K.; Yamamoto, M.; Omiya, K.; Itoh, H.; Kamegai, M.; Murayama, M.; Sugai, J. Changes in hemodynamics and catecholamines during single-level exercise at the anaerobic threshold and 120% of the anaerobic threshold in normal subjects. J. Cardiol. 1994, 24, 61–69. [Google Scholar]
- James, N.W.; Adams, G.M.; Wilson, A.F. Determination of anaerobic threshold by ventilatory frequency. Int. J. Sports Med. 1989, 10, 192–196. [Google Scholar] [CrossRef]
- Kominami, K.; Nishijima, H.; Imahashi, K.; Katsuragawa, T.; Murakami, M.; Yonezawa, K.; Akino, M. Very early lactate threshold in healty young men as related to oxygen uptake kinetics. Medicine 2015, 94, e1559. [Google Scholar] [CrossRef]
- Mitsuru, T.; Yukiko, H.; Kiyokazu, S.; Koutaro, K.; Kiyoshi, O.; Kazunori, K. Relationship between Heart rate variability during exercise and ventilatory threshold. Jpn. J. Phys. Fit. Sports Med. 2001, 50, 185–192. [Google Scholar]
- Masanori, T.; Takayuki, F.; Junzo, T.; Yoshitaka, O. Determination of Anaerobic Threshold by the Breakpoint of Locomotor Respiratory Coupling. Acta Med. Hyogo 2011, 36, 99–106. [Google Scholar]
- Rika, K.; Akira, S. The Anaerobic Threshold (AT) determination experimental system and the movement of ventilation expire in limited respiration. IEICE Tech. Rep. 2016, 116, 7–12. [Google Scholar]
- Voorn, E.L.; Gerrits, K.H.; Koopman, F.S.; Nollet, F.; Beelen, A. Determining the Anaerobic Threshold in Postpolio Syndrome:Comparison With Current Guidelines for Training Intensity Prescription. Arch. Phys. Med. Rehabil. 2014, 95, 935–940. [Google Scholar] [CrossRef]
- Sue, D.Y.; Wasserman, K.; Moricca, R.B.; Casaburi, R. Metabolic acidosis during exercise in patients with chronic obstructive pulmonary disease. Chest 1988, 94, 931–938. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.A.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. Am. Physiol. Soc. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Package ‘Strucchange’. Available online: https://cran.r-project.org, (accessed on 17 November 2021).
- Wasserman, K. The anaerobic threshold measurement to evaluate exercise performance. Am. Rev. Respir. Dis. 1984, 129, 2P2. [Google Scholar] [CrossRef]
- Poole, D.C.; Rossiter, H.B.; Brooks, G.A.; Gladden, L.B. The anaerobic threshold:50+years of controversy. J. Physiol. 2020, 599, 737–767. [Google Scholar] [CrossRef]
- Karvonen, M.J.; Kentala, E.; Mustala, O. The effects of training on heart rate: A longitudinal study. Ann. Med. Exper. Fenn. 1957, 35, 307–315. [Google Scholar]
- Hughson, R.L.; Northey, D.R.; Xing, H.C.; Dietrich, B.H.; Cochrane, J.E. Alignment of ventilation and gas fraction for breath-by-breath respiratory gas exchange calculations in exercise. Comput. Biomed. Res. 1991, 24, 118–128. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Hirotaka, N.; Kazuo, K.; Kazuya, Y.; Hiroki, H.; Masayuki, S. Quantification and physiological significance of the rightward shift of the V-slope during incremental cardiopulmonary exercise testing. BMC Sports Sci. Med. Rehabil. 2017, 9, 9. [Google Scholar]
- Hirotaka, N.; Kazuyuki, K.; Kazuo, K.; Masatoshi, A.; Masayuki, S. New method for the mathematical derivation of the ventilator anaerobic threshold:a retrospective study. BMC Sports Sci. Med. Rehabil. 2019, 11, 10. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | BMI | Smoking History |
|---|---|---|
| A | 23.2 | Non-smoker |
| B | 19.8 | Non-smoker |
| C | 19.5 | Non-smoker |
| D | 19.7 | Non-smoker |
| E | 21.5 | Non-smoker |
| F | 22.8 | Non-smoker |
| G | 20 | Non-smoker |
| H | 24.9 | Non-smoker |
| I | 18.2 | Non-smoker |
| J | 21.8 | Non-smoker |
| K | 18.7 | Non-smoker |
| L | 21.4 | Non-smoker |
| M | 21.4 | Non-smoker |
| N | 18.2 | Non-smoker |
| O | 18.5 | Non-smoker |
| P | 19.8 | Non-smoker |
| Q | 20.5 | Non-smoker |
| mean | 21 | - |
| SD | 1.9 | - |
| Subject | Strucchange (95% CI) | Strucchange (Median) | Metabolic Measurement System | V-Slope Method |
|---|---|---|---|---|
| A | 110 | 110 | 100 | 110 |
| B | 100–110 | 110 | 110 | 110 |
| C | 80–90 | 90 | 90 | 100 |
| D | 70–80 | 70 | 80 | 120 |
| E | 80–90 | 80 | 80 | 125 |
| F | 120–130 | 120 | 120 | 120 |
| G | 120–130 | 130 | 120 | 140 |
| H | 90–100 | 90 | 90 | 125 |
| I | 70–90 | 80 | 90 | 95 |
| J | 120–130 | 130 | 120 | 120 |
| K | 90–100 | 100 | 100 | 150 |
| L | 100 | 100 | 100 | 110 |
| M | 90–100 | 100 | Not detected | 85 |
| N | 100–110 | 105 | Not detected | 117.5 |
| O | 100 | 100 | Not detected | 112.5 |
| P | 80–100 | 90 | Not detected | 137.5 |
| Q | 100–110 | 100 | Not detected | 97 |
| mean | - | 100.3 | 100 | 116.1 |
| SD | - | 16.1 | 14.8 | 16.4 |
| Subject | Strucchange (95% CI) | Strucchange (Median) | Metabolic Measurement System | V-Slope Method |
|---|---|---|---|---|
| A | 110–120 | 110 | 100 | 110 |
| B | 110–130 | 120 | 110 | 110 |
| C | 90 | 90 | 90 | 100 |
| D | 70–80 | 80 | 80 | 120 |
| E | 80–90 | 80 | 80 | 125 |
| F | 120–130 | 130 | 120 | 120 |
| G | 120–130 | 130 | 120 | 140 |
| H | 90–100 | 90 | 90 | 125 |
| I | 100–110 | 110 | 90 | 95 |
| J | 120–130 | 130 | 120 | 120 |
| K | 100–115 | 105 | 100 | 150 |
| L | 120–130 | 125 | 100 | 110 |
| M | 100–115 | 105 | Not detected | 85 |
| N | 100–110 | 105 | Not detected | 117.5 |
| O | 90–100 | 95 | Not detected | 112.5 |
| P | 100–115 | 110 | Not detected | 137.5 |
| Q | 95–110 | 105 | Not detected | 97 |
| mean | - | 107.0 | 100 | 116.1 |
| SD | - | 15.9 | 14.8 | 16.4 |
| Subject | Strucchange (95% CI) | Strucchange (Median) | Metabolic Measurement System | V-Slope Method |
|---|---|---|---|---|
| A | 110–120 | 110 | 100 | 110 |
| B | 110–120 | 120 | 110 | 110 |
| C | 100–110 | 110 | 90 | 100 |
| D | 90–100 | 100 | 80 | 120 |
| E | 100–110 | 100 | 80 | 125 |
| F | 100–110 | 110 | 120 | 120 |
| G | 80–90 | 90 | 120 | 140 |
| H | 60–100 | 70 | 90 | 125 |
| I | 70–80 | 70 | 90 | 95 |
| J | 100–110 | 110 | 120 | 120 |
| K | 70–80 | 70 | 100 | 150 |
| L | 50–65 | 55 | 100 | 110 |
| M | 60–75 | 65 | No detected | 85 |
| N | 20 | 20 | No detected | 117.5 |
| O | 75–85 | 80 | No detected | 112.5 |
| P | 70–80 | 75 | No detected | 137.5 |
| Q | 50–75 | 60 | No detected | 97 |
| mean | - | 83.2 | 100 | 116.1 |
| SD | - | 24.8 | 14.8 | 16.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aida, T.; Shionoya, A.; Nonaka, H.; Hayami, K.; Uchiyama, H.; Nagamori, M.; Ohhashi, S.; Kobayashi, M.; Takayama, T.; Kimura, S. Exploration of an Inflection Point of Ventilation Parameters with Anaerobic Threshold Using Strucchange. Sensors 2022, 22, 2682. https://doi.org/10.3390/s22072682
Aida T, Shionoya A, Nonaka H, Hayami K, Uchiyama H, Nagamori M, Ohhashi S, Kobayashi M, Takayama T, Kimura S. Exploration of an Inflection Point of Ventilation Parameters with Anaerobic Threshold Using Strucchange. Sensors. 2022; 22(7):2682. https://doi.org/10.3390/s22072682
Chicago/Turabian StyleAida, Takenori, Akira Shionoya, Hirofumi Nonaka, Kouji Hayami, Hisashi Uchiyama, Masahiro Nagamori, Satoshi Ohhashi, Mai Kobayashi, Tsugumi Takayama, and Shinji Kimura. 2022. "Exploration of an Inflection Point of Ventilation Parameters with Anaerobic Threshold Using Strucchange" Sensors 22, no. 7: 2682. https://doi.org/10.3390/s22072682