
Serum microRNA Levels as a Biomarker for Diagnosing Non-Alcoholic Fatty Liver Disease in Chinese Colorectal Polyp Patients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
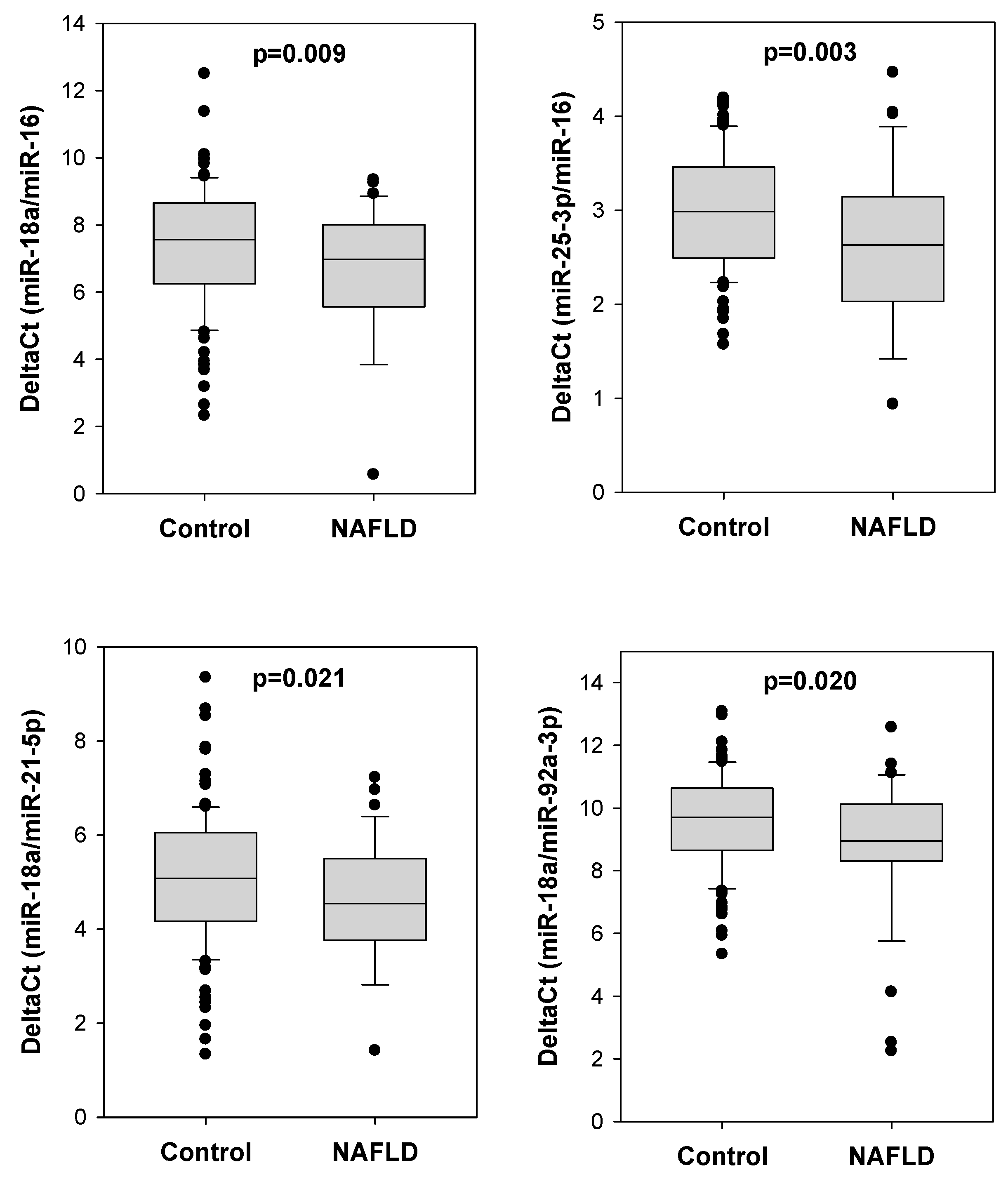
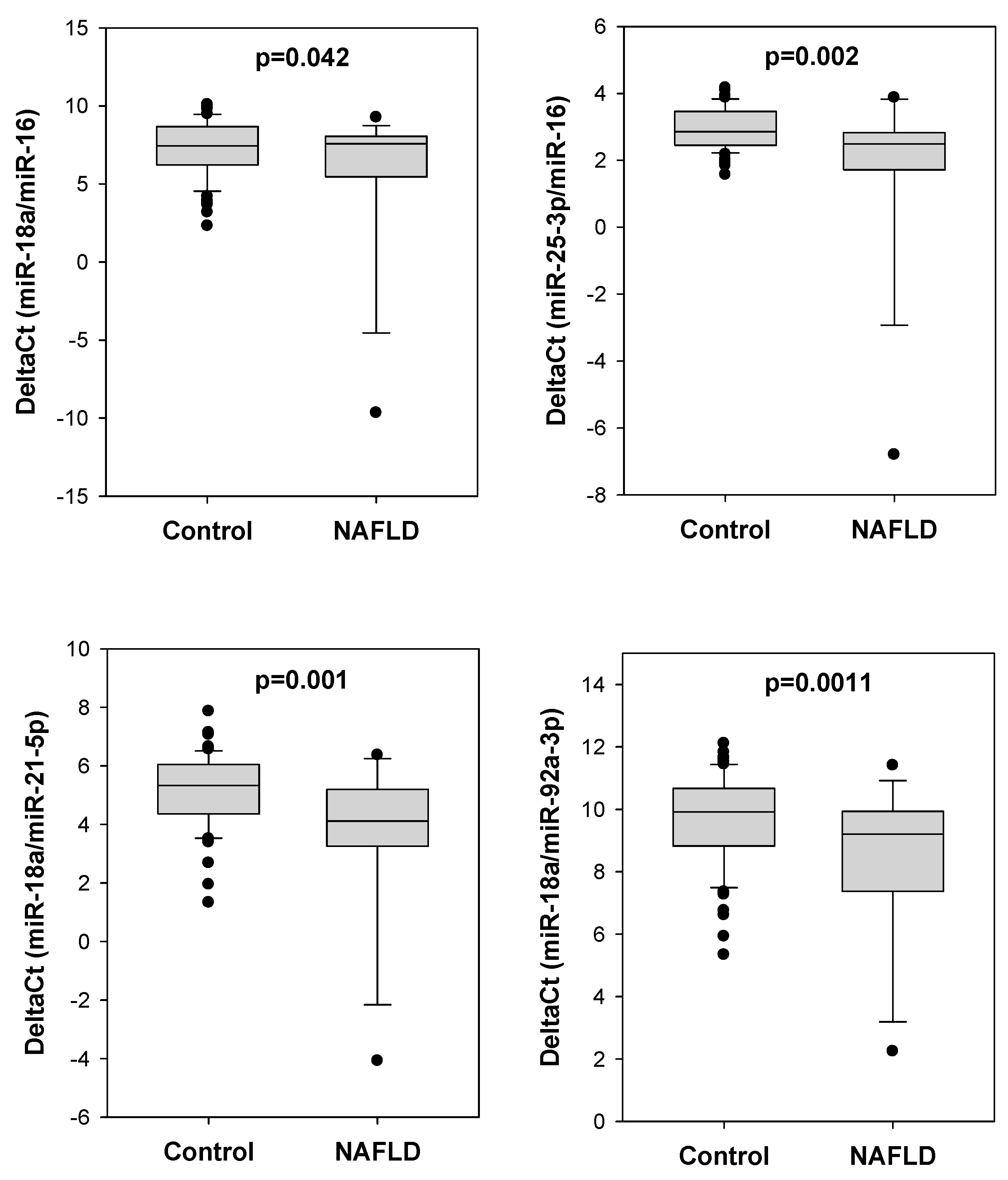
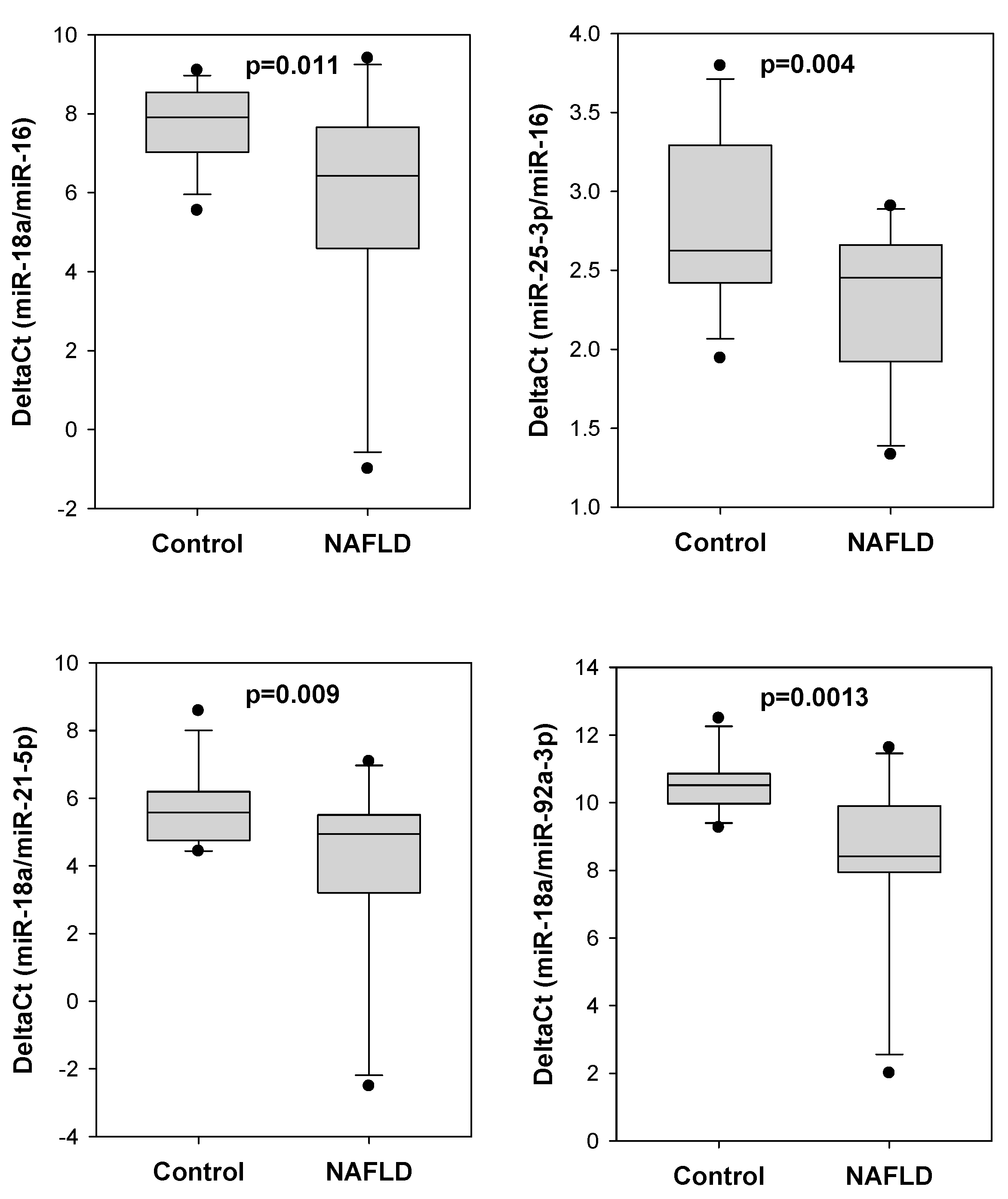
2.2. Comparison of Different miRNA Pairs between Polyp Patients with or without NAFLD
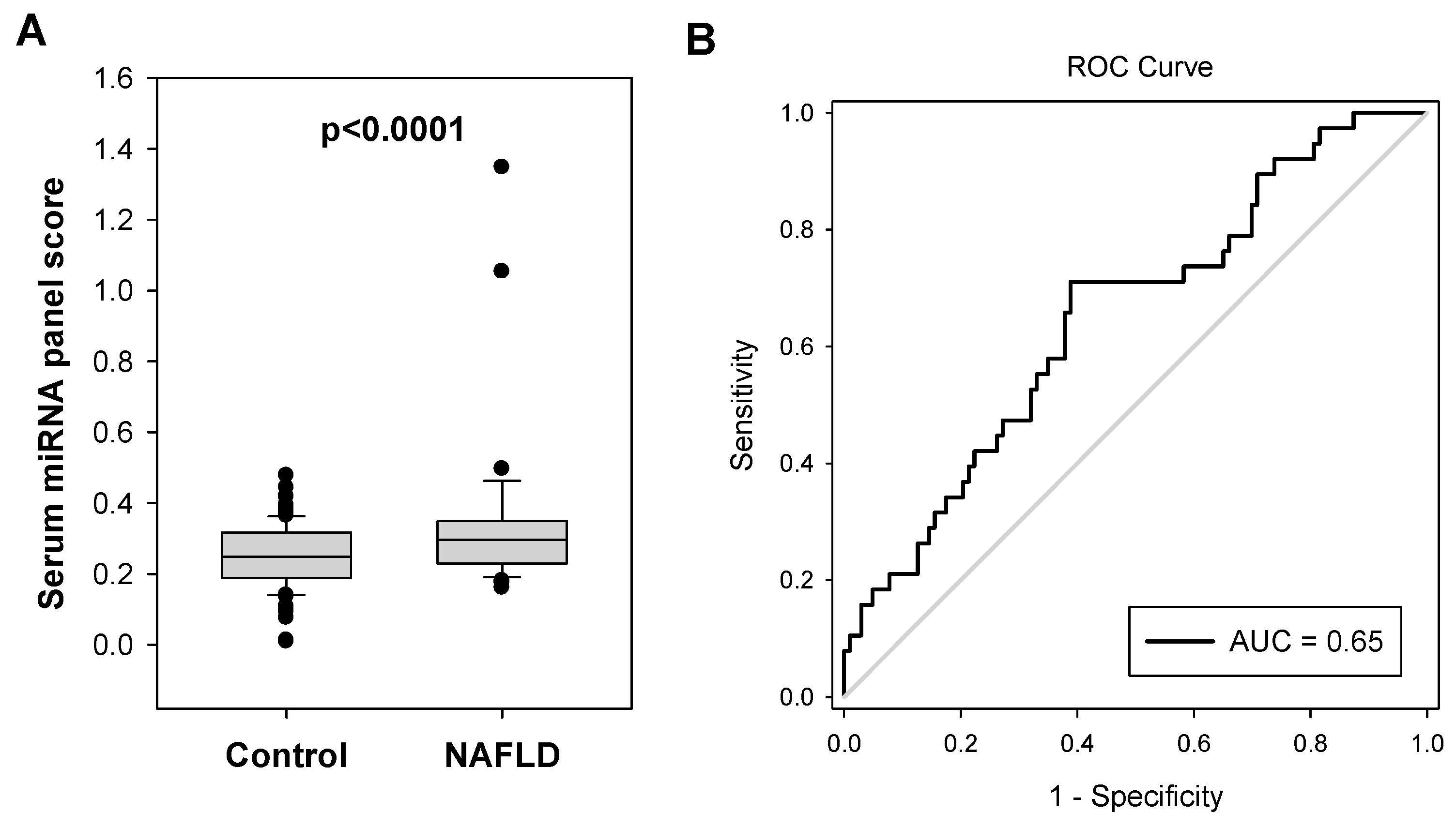
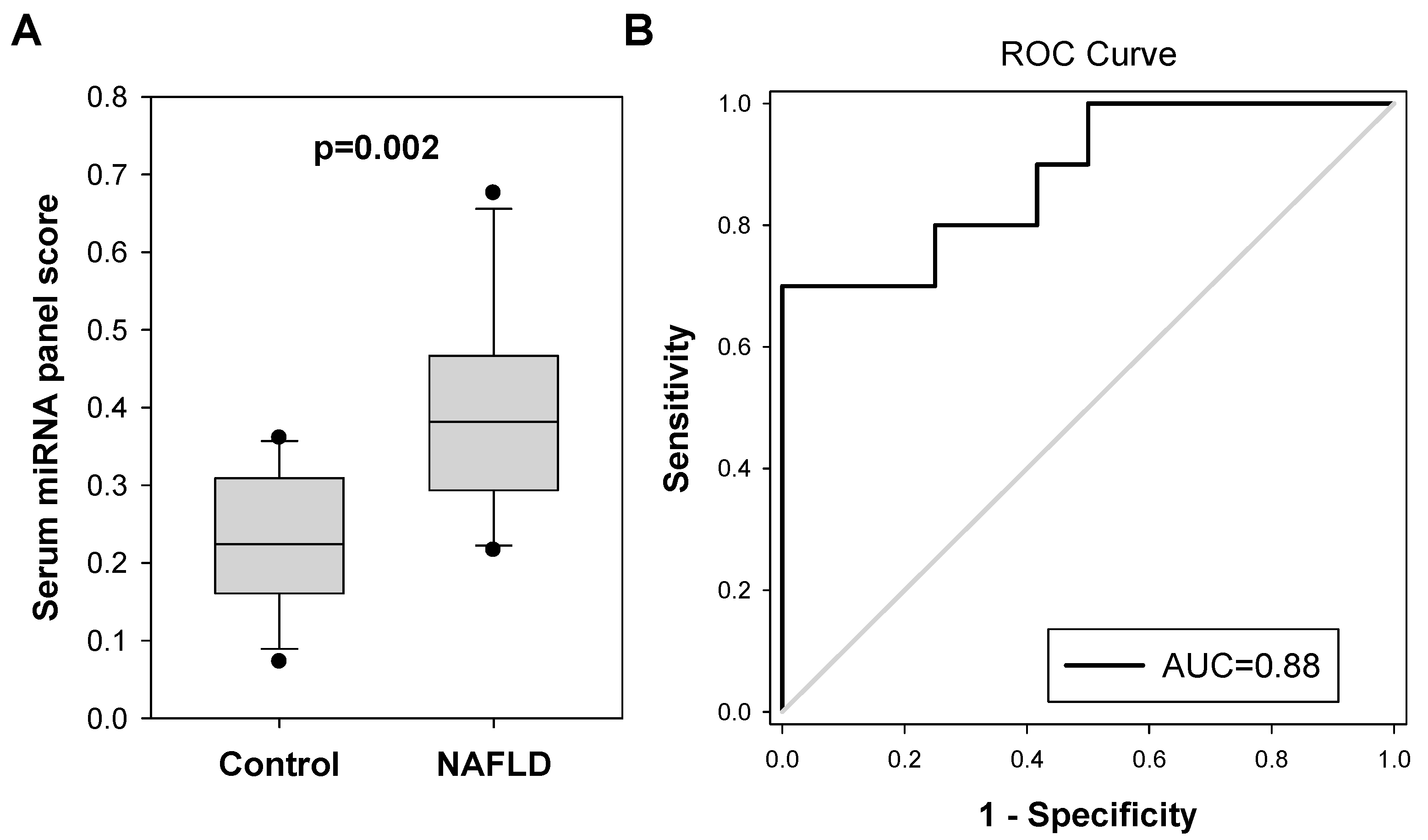
2.3. Diagnostic Performance of Serum miRNA Panel for NAFLD in Colorectal Polyp Patients
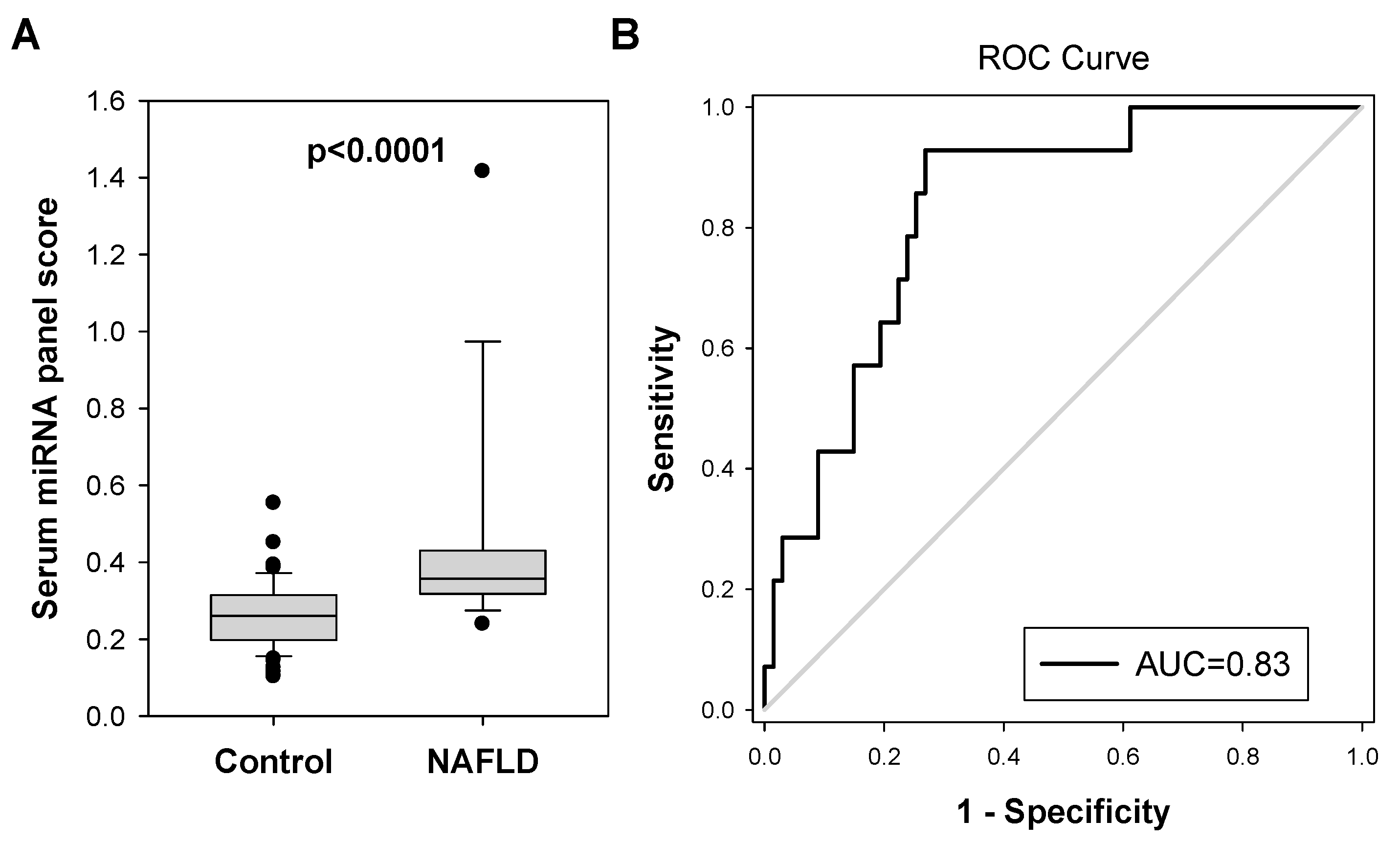
2.4. Validation of Serum miRNA Panel for Diagnosing Probable NAFLD in Another Small Cohort of Colorectal Polyp Patients
3. Discussion
4. Materials and Methods
4.1. Patient Specimens
4.2. Serum miRNA Extraction
4.3. Reverse Transcription (RT) and Quantitative Polymerase Chain Reaction (qPCR)
4.4. Statistical Analysis
4.5. Sample Size Calculation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pydyn, N.; Miekus, K.; Jura, J.; Kotlinowski, J. New therapeutic strategies in nonalcoholic fatty liver disease: A focus on promising drugs for nonalcoholic steatohepatitis. Pharm. Rep. 2020, 72, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Chan, H.L.Y.; Chien, R.N.; Chuang, W.L.; Fung, J.; Goh, G.B.; Hu, T.H.; Huang, J.F.; Jang, B.K.; Jun, D.W.; et al. Modelling NAFLD disease burden in four Asian regions-2019–2030. Aliment Pharm. 2020, 51, 801–811. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Streba, L.A.; Vere, C.C.; Rogoveanu, I.; Streba, C.T. Nonalcoholic fatty liver disease, metabolic risk factors, and hepatocellular carcinoma: An open question. World J. Gastroenterol. 2015, 21, 4103–4110. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.; Charlton, M. The globalization of nonalcoholic fatty liver disease: Prevalence and impact on world health. Hepatology 2016, 64, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Huck, M.B.; Bohl, J.L. Colonic Polyps: Diagnosis and Surveillance. Clin. Colon Rectal Surg. 2016, 29, 296–305. [Google Scholar] [CrossRef]
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef]
- Pan, J.; Cen, L.; Xu, L.; Miao, M.; Li, Y.; Yu, C.; Shen, Z. Prevalence and risk factors for colorectal polyps in a Chinese population: A retrospective study. Sci. Rep. 2020, 10, 6974. [Google Scholar] [CrossRef]
- Iyer, D.N.; Wan, T.M.H.; Man, J.H.W.; Sin, R.W.Y.; Li, X.; Lo, O.S.H.; Foo, D.C.C.; Pang, R.W.C.; Law, W.L.; Ng, L. Small RNA profiling of piRNAs in colorectal cancer identifies consistent overexpression of piR-24000 that correlates clinically with an aggressive disease phenotype. Cancers 2020, 12, 188. [Google Scholar] [CrossRef]
- Polite, B.N.; Dignam, J.J.; Olopade, O.I. Colorectal cancer and race: Understanding the differences in outcomes between African Americans and whites. Med. Clin. N. Am. 2005, 89, 771–793. [Google Scholar] [CrossRef]
- Siripongpreeda, B.; Mahidol, C.; Dusitanond, N.; Sriprayoon, T.; Muyphuag, B.; Sricharunrat, T.; Teerayatanakul, N.; Chaiwong, W.; Worasawate, W.; Sattayarungsee, P.; et al. High prevalence of advanced colorectal neoplasia in the Thai population: A prospective screening colonoscopy of 1404 cases. BMC Gastroenterol. 2016, 16, 101. [Google Scholar] [CrossRef]
- Yang, M.H.; Rampal, S.; Sung, J.; Choi, Y.H.; Son, H.J.; Lee, J.H.; Kim, Y.H.; Chang, D.K.; Rhee, P.L.; Rhee, J.C.; et al. The prevalence of colorectal adenomas in asymptomatic Korean men and women. Cancer Epidemiol. Biomark. Prev. 2014, 23, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Nakai, K.; Watari, J.; Tozawa, K.; Tamura, A.; Hara, K.; Yamasaki, T.; Kondo, T.; Kono, T.; Tomita, T.; Ohda, Y.; et al. Sex differences in associations among metabolic syndrome, obesity, related biomarkers, and colorectal adenomatous polyp risk in a Japanese population. J. Clin. Biochem. Nutr. 2018, 63, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Du, J.; Xu, Y.; Zhu, Z.; Cao, H. Helicobacter pylori infection associated with an increased risk of colorectal adenomatous polyps in the Chinese population. BMC Gastroenterol. 2019, 19, 14. [Google Scholar] [CrossRef]
- Colussi, D.; Fabbri, M.; Zagari, R.M.; Montale, A.; Bazzoli, F.; Ricciardiello, L. Lifestyle factors and risk for colorectal polyps and cancer at index colonoscopy in a FIT-positive screening population. United Eur. Gastroenterol. J. 2018, 6, 935–942. [Google Scholar] [CrossRef]
- Hwang, S.T.; Cho, Y.K.; Park, J.H.; Kim, H.J.; Park, D.I.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Won, K.H.; Jin, W. Relationship of non-alcoholic fatty liver disease to colorectal adenomatous polyps. J. Gastroenterol. Hepatol. 2010, 25, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, B.D.; Lukose, T.; Siegel, A.B.; Brown, R.S., Jr.; Verna, E.C. Increased risk of colorectal polyps in patients with non-alcoholic fatty liver disease undergoing liver transplant evaluation. J. Gastrointest. Oncol. 2015, 6, 459–468. [Google Scholar] [CrossRef]
- Chen, W.; Wang, M.; Jing, X.; Wu, C.; Zeng, Y.; Peng, J.; Cai, X. High risk of colorectal polyps in men with non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 2051–2065. [Google Scholar] [CrossRef]
- Li, Y.; Liu, S.; Gao, Y.; Ma, H.; Zhan, S.; Yang, Y.; Xin, Y.; Xuan, S. Association between NAFLD and Risk of Colorectal Adenoma in Chinese Han Population. J. Clin. Transl. Hepatol. 2019, 7, 99–105. [Google Scholar] [CrossRef]
- Keku, T.O.; Lund, P.K.; Galanko, J.; Simmons, J.G.; Woosley, J.T.; Sandler, R.S. Insulin resistance, apoptosis, and colorectal adenoma risk. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2076–2081. [Google Scholar] [CrossRef]
- Yu, X.; Xie, L.; Zhou, Y.; Yuan, X.; Wu, Y.; Chen, P. Patients with non-alcoholic fatty liver disease may be a high-risk group for the development of colorectal polyps: A cross-sectional study. World Acad. Sci. J. 2020, 2, 1. [Google Scholar] [CrossRef]
- Hernandez-Rodas, M.C.; Valenzuela, R.; Videla, L.A. Relevant Aspects of Nutritional and Dietary Interventions in Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, K.; Sakai, Y.; Terashima, T.; Shimode, T.; Seki, A.; Orita, N.; Takeshita, Y.; Shimakami, T.; Takatori, H.; Arai, K.; et al. Decline in serum albumin concentration is a predictor of serious events in nonalcoholic fatty liver disease. Medicine 2021, 100, e26835. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Rowe, I.A.; Parker, R. Liver biopsy for the selection of patients with nonalcoholic steatohepatitis for clinical trials. Gastroenterology 2015, 148, 262. [Google Scholar] [CrossRef]
- Bedossa, P.; Dargere, D.; Paradis, V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003, 38, 1449–1457. [Google Scholar] [CrossRef]
- Wang, Z.; Lu, Y.; Han, J. Peripheral blood microRNAs: A novel tool for diagnosing disease? Intractable Rare Dis. Res. 2012, 1, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Xin, S.; Zhan, Q.; Chen, X.; Xu, J.; Yu, Y. Efficacy of serum miRNA test as a non-invasive method to diagnose nonalcoholic steatohepatitis: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 186. [Google Scholar] [CrossRef]
- Vulf, M.; Shunkina, D.; Komar, A.; Bograya, M.; Zatolokin, P.; Kirienkova, E.; Gazatova, N.; Kozlov, I.; Litvinova, L. Analysis of miRNAs Profiles in Serum of Patients With Steatosis and Steatohepatitis. Front. Cell Dev. Biol. 2021, 9, 736677. [Google Scholar] [CrossRef]
- Kim, T.H.; Lee, Y.; Lee, Y.S.; Gim, J.A.; Ko, E.; Yim, S.Y.; Jung, Y.K.; Kang, S.; Kim, M.Y.; Kim, H.; et al. Circulating miRNA is a useful diagnostic biomarker for nonalcoholic steatohepatitis in nonalcoholic fatty liver disease. Sci. Rep. 2021, 11, 14639. [Google Scholar] [CrossRef]
- Quintas, G.; Caiment, F.; Rienda, I.; Perez-Rojas, J.; Pareja, E.; Castell, J.V.; Jover, R. Quantitative Prediction of Steatosis in Patients with Non-Alcoholic Fatty Liver by Means of Hepatic MicroRNAs Present in Serum and Correlating with Hepatic Fat. Int. J. Mol. Sci. 2022, 23, 9298. [Google Scholar] [CrossRef] [PubMed]
- Landrier, J.F.; Derghal, A.; Mounien, L. MicroRNAs in Obesity and Related Metabolic Disorders. Cells 2019, 8, 859. [Google Scholar] [CrossRef] [PubMed]
- Fang, R.; Zhu, Y.; Hu, L.; Khadka, V.S.; Ai, J.; Zou, H.; Ju, D.; Jiang, B.; Deng, Y.; Hu, X. Plasma MicroRNA Pair Panels as Novel Biomarkers for Detection of Early Stage Breast Cancer. Front. Physiol. 2018, 9, 1879. [Google Scholar] [CrossRef] [PubMed]
- Boeri, M.; Verri, C.; Conte, D.; Roz, L.; Modena, P.; Facchinetti, F.; Calabro, E.; Croce, C.M.; Pastorino, U.; Sozzi, G. MicroRNA signatures in tissues and plasma predict development and prognosis of computed tomography detected lung cancer. Proc. Natl. Acad. Sci. USA 2011, 108, 3713–3718. [Google Scholar] [CrossRef] [PubMed]
- Hennessey, P.T.; Sanford, T.; Choudhary, A.; Mydlarz, W.W.; Brown, D.; Adai, A.T.; Ochs, M.F.; Ahrendt, S.A.; Mambo, E.; Califano, J.A. Serum microRNA biomarkers for detection of non-small cell lung cancer. PloS ONE 2012, 7, e32307. [Google Scholar] [CrossRef]
- Matthaei, H.; Wylie, D.; Lloyd, M.B.; Dal Molin, M.; Kemppainen, J.; Mayo, S.C.; Wolfgang, C.L.; Schulick, R.D.; Langfield, L.; Andruss, B.F.; et al. miRNA biomarkers in cyst fluid augment the diagnosis and management of pancreatic cysts. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2012, 18, 4713–4724. [Google Scholar] [CrossRef]
- Sheinerman, K.S.; Umansky, S. Universal screening test based on analysis of circulating organ-enriched microRNAs: A novel approach to diagnostic screening. Expert Rev. Mol. Diagn. 2015, 15, 329–338. [Google Scholar] [CrossRef]
- Srinivasan, S.; Treacy, R.; Herrero, T.; Olsen, R.; Leonardo, T.R.; Zhang, X.; DeHoff, P.; To, C.; Poling, L.G.; Fernando, A.; et al. Discovery and Verification of Extracellular miRNA Biomarkers for Non-invasive Prediction of Pre-eclampsia in Asymptomatic Women. Cell Rep. Med. 2020, 1, 10003. [Google Scholar] [CrossRef]
- Cermelli, S.; Ruggieri, A.; Marrero, J.A.; Ioannou, G.N.; Beretta, L. Circulating microRNAs in patients with chronic hepatitis C and non-alcoholic fatty liver disease. PloS ONE 2011, 6, e23937. [Google Scholar] [CrossRef]
- Gori, M.; Arciello, M.; Balsano, C. MicroRNAs in nonalcoholic fatty liver disease: Novel biomarkers and prognostic tools during the transition from steatosis to hepatocarcinoma. BioMed Res. Int. 2014, 2014, 741465. [Google Scholar] [CrossRef]
- Liang, T.; Liu, C.; Ye, Z. Deep sequencing of small RNA repertoires in mice reveals metabolic disorders-associated hepatic miRNAs. PloS ONE 2013, 8, e80774. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Yang, Z.; Kusumanchi, P.; Han, S.; Liangpunsakul, S. Critical Role of microRNA-21 in the Pathogenesis of Liver Diseases. Front. Med. 2020, 7, 7. [Google Scholar] [CrossRef]
- Sun, C.; Huang, F.; Liu, X.; Xiao, X.; Yang, M.; Hu, G.; Liu, H.; Liao, L. miR-21 regulates triglyceride and cholesterol metabolism in non-alcoholic fatty liver disease by targeting HMGCR. Int. J. Mol. Med. 2015, 35, 847–853. [Google Scholar] [CrossRef]
- Yamada, H.; Suzuki, K.; Ichino, N.; Ando, Y.; Sawada, A.; Osakabe, K.; Sugimoto, K.; Ohashi, K.; Teradaira, R.; Inoue, T.; et al. Associations between circulating microRNAs (miR-21, miR-34a, miR-122 and miR-451) and non-alcoholic fatty liver. Clin. Chim. Acta Int. J. Clin. Chem. 2013, 424, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.; Leary, P.J.; Govaere, O.; Barter, M.J.; Charlton, S.H.; Cockell, S.J.; Tiniakos, D.; Zatorska, M.; Bedossa, P.; Brosnan, M.J.; et al. Increased serum miR-193a-5p during non-alcoholic fatty liver disease progression: Diagnostic and mechanistic relevance. JHEP Rep. Innov. Hepatol. 2022, 4, 100409. [Google Scholar] [CrossRef] [PubMed]
- Cisilotto, J.; do Amaral, A.E.; Rosolen, D.; Rode, M.P.; Silva, A.H.; Winter, E.; da Silva, T.E.; Fischer, J.; Matiollo, C.; Rateke, E.C.M.; et al. MicroRNA profiles in serum samples from Acute-On-Chronic Liver Failure patients and miR-25-3p as a potential biomarker for survival prediction. Sci. Rep. 2020, 10, 100. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiang, D.; Hu, X.; Ruan, Q.; Wang, L.; Bao, Z. Identification and study of differentially expressed miRNAs in aged NAFLD rats based on high-throughput sequencing. Ann. Hepatol. 2020, 19, 302–312. [Google Scholar] [CrossRef]
- Pratama, M.Y.; Pascut, D.; Tamini, S.; Minocci, A.; Tiribelli, C.; Grugni, G.; Sartorio, A. Circulating microRNA Associated to Different Stages of Liver Steatosis in Prader-Willi Syndrome and Non-Syndromic Obesity. J. Clin. Med. 2020, 9, 1123. [Google Scholar] [CrossRef]
- Pescador, N.; Perez-Barba, M.; Ibarra, J.M.; Corbaton, A.; Martinez-Larrad, M.T.; Serrano-Rios, M. Serum circulating microRNA profiling for identification of potential type 2 diabetes and obesity biomarkers. PloS ONE 2013, 8, e77251. [Google Scholar] [CrossRef]
- Iacob, S.A.; Iacob, D.G. Non-Alcoholic Fatty Liver Disease in HIV/HBV Patients—A Metabolic Imbalance Aggravated by Antiretroviral Therapy and Perpetuated by the Hepatokine/Adipokine Axis Breakdown. Front. Endocrinol. 2022, 13, 814209. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Rinaldi, L.; Guerrera, B.; Restivo, L.; Marrone, A.; Giordano, M.; Zampino, R. NAFLD and NASH in HCV Infection: Prevalence and Significance in Hepatic and Extrahepatic Manifestations. Int. J. Mol. Sci. 2016, 17, 803. [Google Scholar] [CrossRef] [PubMed]
- Adenote, A.; Dumic, I.; Madrid, C.; Barusya, C.; Nordstrom, C.W.; Rueda Prada, L. NAFLD and Infection, a Nuanced Relationship. Can. J. Gastroenterol. Hepatol. 2021, 2021, 5556354. [Google Scholar] [CrossRef] [PubMed]
- Nseir, W.; Taha, H.; Khateeb, J.; Grosovski, M.; Assy, N. Fatty liver is associated with recurrent bacterial infections independent of metabolic syndrome. Dig. Dis. Sci. 2011, 56, 3328–3334. [Google Scholar] [CrossRef]
- Parameswaran, M.; Hasan, H.A.; Sadeque, J.; Jhaveri, S.; Avanthika, C.; Arisoyin, A.E.; Dhanani, M.B.; Rath, S.M. Factors That Predict the Progression of Non-alcoholic Fatty Liver Disease (NAFLD). Cureus 2021, 13, e20776. [Google Scholar] [CrossRef] [PubMed]
- Lesmana, C.R.; Pakasi, L.S.; Inggriani, S.; Aidawati, M.L.; Lesmana, L.A. Development of non-alcoholic fatty liver disease scoring system among adult medical check-up patients: A large cross-sectional and prospective validation study. Diabetes Metab. Syndr. Obes. Targets Ther. 2015, 8, 213–218. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NAFLD Group (n = 38) | Control Group (n = 103) | p-Value | |
|---|---|---|---|
| Male | 22 (57.9%) | 57 (55.3%) | |
| Female | 16 (42.1%) | 46 (44.7%) | 0.936 |
| Age | 62.2 ± 8.50 | 64.9 ± 9.96 | 0.138 |
| Type of polyp | |||
| Hyperplastic | 6 | 11 | |
| Tubular adenoma | 25 | 81 | |
| Others | 3 | 5 | |
| Mixed types | 4 | 6 | 0.470 |
| Complications: | |||
| Diabetes only | 8 | 13 | |
| Obesity/overweight only | 5 | 14 | |
| Diabetes and obesity/overweight | 11 | 9 | 0.366 |
| Probable NAFLD Group (n = 10) | Control Group (n = 12) | p-Value | |
|---|---|---|---|
| Male | 7 | 9 | |
| Female | 3 | 3 | 1.000 |
| Age | 61.3 ± 5.95 | 63.8 ± 9.31 | 0.481 |
| Type of polyp | |||
| Hyperplastic | 2 | 2 | |
| Tubular adenoma | 6 | 8 | |
| Mixed types | 2 | 2 | 0.949 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, L.; Sin, R.W.-Y.; Cheung, D.H.; Leung, W.-K.; Man, A.T.-K.; Lo, O.S.-H.; Law, W.-L.; Foo, D.C.-C. Serum microRNA Levels as a Biomarker for Diagnosing Non-Alcoholic Fatty Liver Disease in Chinese Colorectal Polyp Patients. Int. J. Mol. Sci. 2023, 24, 9084. https://doi.org/10.3390/ijms24109084
Ng L, Sin RW-Y, Cheung DH, Leung W-K, Man AT-K, Lo OS-H, Law W-L, Foo DC-C. Serum microRNA Levels as a Biomarker for Diagnosing Non-Alcoholic Fatty Liver Disease in Chinese Colorectal Polyp Patients. International Journal of Molecular Sciences. 2023; 24(10):9084. https://doi.org/10.3390/ijms24109084
Chicago/Turabian StyleNg, Lui, Ryan Wai-Yan Sin, David Him Cheung, Wai-Keung Leung, Abraham Tak-Ka Man, Oswens Siu-Hung Lo, Wai-Lun Law, and Dominic Chi-Chung Foo. 2023. "Serum microRNA Levels as a Biomarker for Diagnosing Non-Alcoholic Fatty Liver Disease in Chinese Colorectal Polyp Patients" International Journal of Molecular Sciences 24, no. 10: 9084. https://doi.org/10.3390/ijms24109084