
The Management of Diabetes Mellitus Using Medicinal Plants and Vitamins
 ,
,
Abstract
:1. Introduction
2. Approaches
Data Sources and Data Extraction
3. Results and Discussions
3.1. Medicinal Plants and Their Anti-Diabetic Properties
3.1.1. Allium sativum and Its Application to Diabetes Mellitus
3.1.2. Momordica charantia and Its Application to Diabetes Mellitus
3.1.3. Hibiscus sabdariffa L. (Roselle) and Its Application to Diabetes Mellitus
3.1.4. Zingiber officinale and Its Application to Diabetes Mellitus
3.2. Vitamins and Their Anti-Diabetic Properties
3.2.1. Vitamin D and Its Application to Diabetes Mellitus
3.2.2. Vitamin E and Its Application to Diabetes Mellitus
3.2.3. Vitamin C and Its application to Diabetes Mellitus
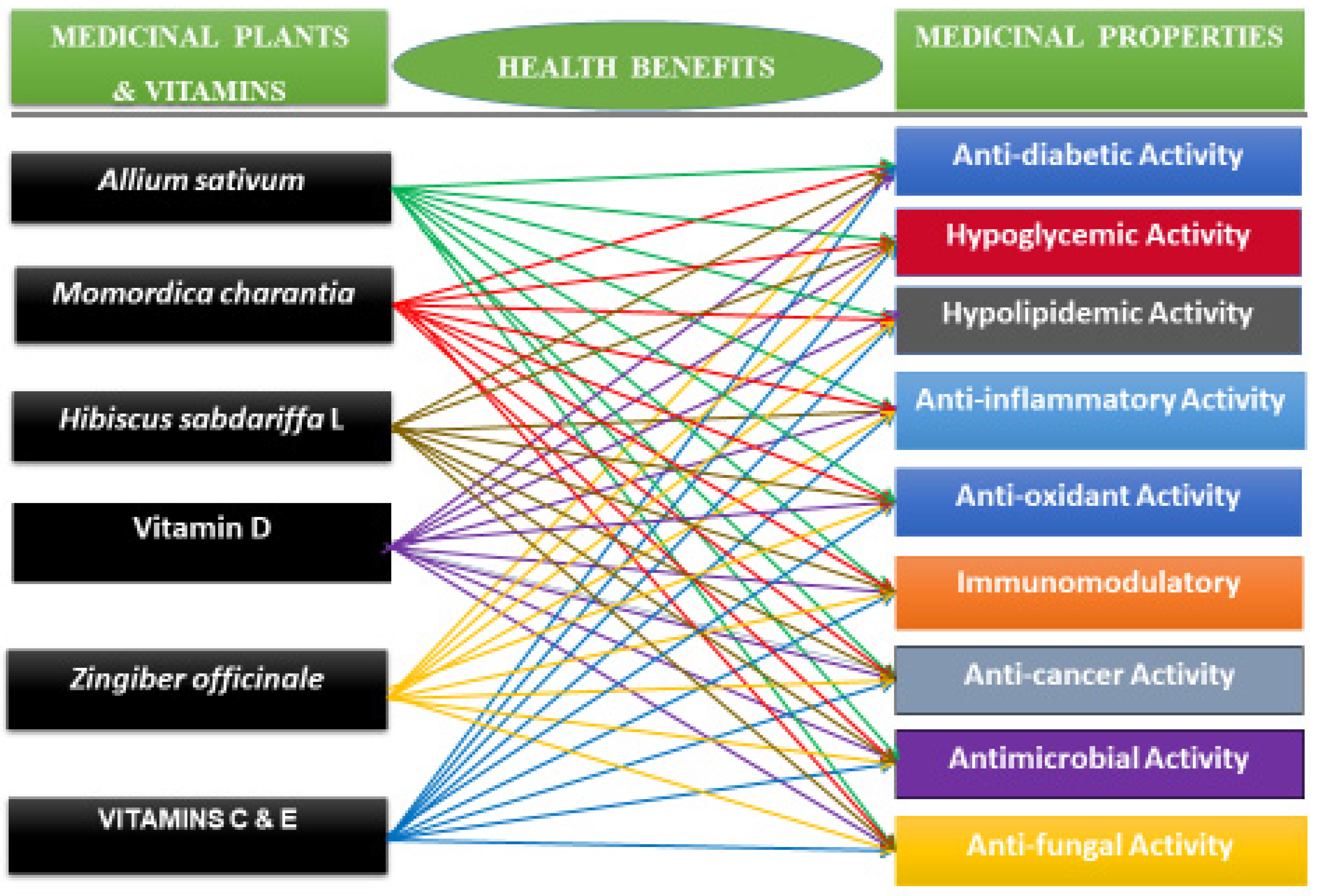
3.3. Medicinal Properties of Selected Medicinal Plants and Vitamins


{kind=link}
{kind=link}
| Medicinal Plants & Vitamins | Mechanisms of Action | Clinical Studies |
|---|---|---|
Allium Sativum | Allium Sativum plays a role in the treatment of diabetes by enhancing the gene expression of caspase 3 and caspase 9, reducing IL-1β, IL-6, and TNF-α level and increasing IFN-γ in vitro and in vivo [101]. | A double-blind clinical trial in diabetic patients demonstrated garlic intake at a dose of 750 mg three times per day for 12 weeks had potential effects for treating diabetes by reducing fasting glucose blood levels through the decrease in hemoglobin A1c (HbA1C) [102]. |
Vitamin C | Vitamin C enhances the immune system by stimulating IFN production and lymphocyte proliferation, enhancing neutrophil phagocytic capability [103]. Vitamin C intake regulates fasting blood glucose (FBG) and glycosylated hemoglobin A1c (HbA1C) and improves insulin resistance [104,105]. | More clinical trials are needed to confirm whether Vitamin C shows promise as an effective therapeutic agent for diabetes mellitus. |
Momordica charantia | Momordica charantia exerts its hypoglycemic effect through multiple mechanisms of action including the stimulation or inhibition of the key enzymes of hexose monophosphate pathways. It can stimulate key enzymes of the hexose monophosphate pathway, inhibit glucose uptake by the intestine, increase the utilization of peripheral and skeletal muscle glucose, inhibit gluconeogenesis and adipocytes differentiation, and normalize the islet βcells [39,106,107,108]. | Clinical trials are needed (clinical studies of Momordica charantia for the treatment of diabetes have been sparse and sporadic). |
Hibiscus sabdariffa | The mechanism of action of Hibiscus sabdariffa is based on the strong ability to delay the digestion of complex sugars into simple sugars, reduce the absorption of simple sugar, and lower total blood glucose [109,110]. | Clinical trials are needed. |
Vitamin D | Studies showed that Vitamin D promotes the conversion of proinsulin to insulin, increases insulin output, and enhances insulin action through the regulation of the calcium pool [81,82]. | A randomized control double-blind intervention study noted a significant improvement of insulin sensitivity in diabetic patients supplementing 4000 IU of Vitamin D for 6 months compared to placebo [84]. |
Vitamin E | Animal models and human studies have demonstrated that vitamin E intake blocks LDL lipid peroxidation, prevents the oxidative stress linked to T2DM-associated abnormal metabolic patterns (hyperglycemia, dyslipidemia, and elevated levels of FFAs), and, subsequently, attenuates cytokine gene expression. | A recent report evaluated the effects of a combination of Vitamin C (1000 mg/day) and vitamin E (400 IU/day) for four weeks on insulin sensitivity in untrained and trained healthy young men and concluded that such supplement may preclude the exercise-induced amelioration of insulin resistance in humans [111]. |
Zingiber Officinale | Diabetic patients who took 2 g of ginger for 2 months revealed a reduction in insulin, homeostasis model assessment (HOMA), and low-density lipoprotein (LDL), with no impact on fasting plasma glucose (FPG), HbA1C, total cholesterol, and HDL levels [112]. | A double-blinded placebo-controlled randomized clinical trial conducted on two groups of patients with type 2 diabetes reported that ginger powder improved glycemic indices as well as TAC and PON-1 activity in patients [64]. However, more clinical trials are needed to shed light on the effectiveness of ginger in human subjects with diabetes. |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ozougwu, J.C.; Obimba, K.C.; Belonwu, C.D.; Unakalamba, C.B. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J. Physiol. Pathophysiol. 2013, 4, 46–57. [Google Scholar] [CrossRef]
- Kim, H.-G. Cognitive dysfunctions in individuals with diabetes mellitus. Yeungnam Univ. J. Med. 2019, 36, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.J.; Gregg, E.W.; Brinks, R.; Saydah, S.H.; Albright, A.L.; Imperatore, G. 103-OR: Change in Lifetime Risk for Diabetes in the United States, 1997–2015. Diabetes 2020, 69, 103-OR. [Google Scholar] [CrossRef]
- Olokoba, A.B.; Obateru, O.A.; Olokoba, L.B. Type 2 Diabetes Mellitus: A Review of Current Trends. Oman Med. J. 2012, 27, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.-S.; Ko, S.-H. Current trends in epidemiology of cardiovascular disease and cardiovascular risk management in type 2 diabetes. Metab. Clin. Exp. 2021, 123, 154838. [Google Scholar] [CrossRef] [PubMed]
- E Garcia, D.; Narvaez-Mendez, M.; Morgan, S.; Coronado-Malagon, M.; Arce-Salinas, C.A.; Barajas, A.; Arenas, I.; Svarch, A. Biomarkers Through The Development, Progression and Chronic Complications of Diabetes Mellitus: A Mini-Review. J. Endocrinol. Diabetes 2018, 5, 1–7. [Google Scholar] [CrossRef]
- Lotfy, M.; Adeghate, J.; Kalasz, H.; Singh, J.; Adeghate, E. Chronic complications of diabetes mellitus: A mini review. Curr. Diabetes Rev. 2016, 13, 3–10. [Google Scholar] [CrossRef]
- Ramtahal, R.; Khan, C.; Maharaj-Khan, K.; Nallamothu, S.; Hinds, A.; Dhanoo, A.; Yeh, H.-C.; Hill-Briggs, F.; Lazo, M. Prevalence of self-reported sleep duration and sleep habits in type 2 diabetes patients in South Trinidad. J. Epidemiol. Glob. Health 2015, 5, S35–S43. [Google Scholar] [CrossRef]
- Shidlovskaya, T.A.; Navalkivska, N.Y. Distortion product otoacoustic emissions among the patients suffering diabetes mellitus type II with hearing impairment. Otorhinolaryngology 2020, 47–52. [Google Scholar] [CrossRef]
- Chaudhury, A.; Duvoor, C.; Reddy Dendi, V.S.; Kraleti, S.; Chada, A.; Ravilla, R.; Marco, A.; Shekhawat, N.S.; Montales, M.T.; Kuriakose, K.; et al. Clinical Review of Antidiabetic Drugs: Implications for Type 2 Diabetes Mellitus Management. Front. Endocrinol. 2017, 8, 6. [Google Scholar] [CrossRef]
- Roglic, G. WHO Global report on diabetes: A summary. Int. J. Noncommunicable Dis. 2016, 1, 3. [Google Scholar] [CrossRef]
- da Rocha Fernandes, J.; Ogurtsova, K.; Linnenkamp, U.; Guariguata, L.; Seuring, T.; Zhang, P.; Cavan, D.; Makaroff, L.E. IDF Diabetes Atlas estimates of 2014 global health expenditures on diabetes. Diabetes Res. Clin. Pract. 2016, 117, 48–54. [Google Scholar] [CrossRef]
- Ekor, M. The growing use of herbal medicines: Issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef]
- Choudhury, H.; Pandey, M.; Hua, C.K.; Mun, C.S.; Jing, J.K.; Kong, L.; Ern, L.Y.; Ashraf, N.A.; Kit, S.W.; Yee, T.S.; et al. An update on natural compounds in the remedy of diabetes mellitus: A systematic review. J. Tradit. Complement. Med. 2018, 8, 361–376. [Google Scholar] [CrossRef]
- Bharali, S.; Gupta, O.P. Potential of plant medicine in the management of Type II diabetes mellitus. J. Ayurveda Integr. Med. 2013, 4. [Google Scholar]
- Dineshkumar, B.; Analava, M.; Manjunatha, M. Antidiabetic and hypolipidaemic effects of few common plants extract in type 2 diabetic patients at Bengal. Dubai Diabetes Endocrinol. J. 2010, 18, 59–65. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Pivina, L.; Doşa, M.D.; Semenova, Y.; Aaseth, J. The Role of Zinc and Copper in Insulin Resistance and Diabetes Mellitus. Curr. Med. Chem. 2019, 27, 6643–6657. [Google Scholar] [CrossRef]
- Al-brakati, A.Y. Protective effect of garlic against diabetic retinopathy in adult albino rats. Res. J. Pharm. Biol. Chem. Sci. 2016, 7, 2748–2759. [Google Scholar]
- Velu, G.; Palanichamy, V.; Rajan, A.P. Phytochemical and pharmacological importance of plant secondary metabolites in modern medicine. In Bioorganic Phase in Natural Food: An Overview; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Gonfa, Y.H.; Beshah, F.; Tadesse, M.G.; Bachheti, A.; Bachheti, R.K. Phytochemical investigation and potential pharmacologically active compounds of Rumex nepalensis: An appraisal. Beni-Suef Univ. J. Basic Appl. Sci. 2021, 10, 18. [Google Scholar] [CrossRef]
- Shaikh, J.R.; Patil, M. Qualitative tests for preliminary phytochemical screening: An overview. Int. J. Chem. Stud. 2020, 8, 603–608. [Google Scholar] [CrossRef]
- Gavamukulya, Y.; Abou-Elella, F.; Wamunyokoli, F.; Ael-Shemy, H. Phytochemical screening, anti-oxidant activity and in vitro anticancer potential of ethanolic and water leaves extracts of Annona muricata (Graviola). Asian Pac. J. Trop. Med. 2014, 7, S355–S363. [Google Scholar] [CrossRef] [PubMed]
- Prabu, K.; Rajasekaran, A.; Bharathi, D.; Ramalakshmi, S. Anti-oxidant activity, phytochemical screening and HPLC profile of rare endemic Cordia diffusa. J. King Saud Univ. Sci. 2019, 31, 724–727. [Google Scholar] [CrossRef]
- Jacob, B.; Narendhirakannan, R.T. Role of medicinal plants in the management of diabetes mellitus: A review. 3 Biotech 2019, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Bora, K.S. Role of Medicinal Plants in the Management of Diabetes Mellitus: A Review. J. Pharm. Res. Int. 2021, 33, 2196–2207. [Google Scholar] [CrossRef]
- Nagalievska, M.; Sabadashka, M.; Hachkova, H.; Sybirna, N. Galega officinalis extract regulate the diabetes mellitus related violations of proliferation, functions and apoptosis of leukocytes. BMC Complement. Altern. Med. 2018, 18, 4. [Google Scholar] [CrossRef]
- Hachkova, H.; Nagalievska, M.; Soliljak, Z.; Kanyuka, O.; Kucharska, A.Z.; Sokół-Łętowska, A.; Belonovskaya, E.; Buko, V.; Sybirna, N. Medicinal Plants Galega officinalis L. and Yacon Leaves as Potential Sources of Antidiabetic Drugs. Antioxidants 2021, 10, 1362. [Google Scholar] [CrossRef]
- Shang, A.; Cao, S.-Y.; Xu, X.-Y.; Gan, R.-Y.; Tang, G.-Y.; Corke, H.; Mavumengwana, V.; Li, H.-B. Bioactive Compounds and Biological Functions of Garlic (Allium sativum L.). Foods 2019, 8, 246. [Google Scholar] [CrossRef]
- Melino, S.; Leo, S.; Papajani, V.T. Natural Hydrogen Sulfide Donors from Allium sp. as a Nutraceutical Approach in Type 2 Diabetes Prevention and Therapy. Nutrients 2019, 11, 1581. [Google Scholar] [CrossRef]
- Ried, K. Garlic Lowers Blood Pressure in Hypertensive Individuals, Regulates Serum Cholesterol, and Stimulates Immunity: An Updated Meta-analysis and Review. J. Nutr. 2016, 146, 389S–396S. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, Y.; Zhou, T.; Zheng, J.; Li, S.; Li, H.-B. Dietary Natural Products for Prevention and Treatment of Liver Cancer. Nutrients 2016, 8, 156. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, X.; Lan, H.; Wang, W. Effect of garlic supplement in the management of type 2 diabetes mellitus (T2DM): A meta-analysis of randomized controlled trials. Food Nutr. Res. 2017, 61, 1377571. [Google Scholar] [CrossRef]
- Ota, A.; Ulrih, N.P. An Overview of Herbal Products and Secondary Metabolites Used for Management of Type Two Diabetes. Front. Pharmacol. 2017, 8, 436. [Google Scholar] [CrossRef]
- Poonam, T.; Prakash, G.P.; Kumar, L.V. Influence of Allium sativum extract on the hypoglycemic activity of glibenclamide: An approach to possible herb-drug interaction. Drug Metab. Drug Interactions 2013, 28, 225–230. [Google Scholar] [CrossRef]
- Afzaal, M.; Saeed, F.; Rasheed, R.; Hussain, M.; Aamir, M.; Hussain, S.; Mohamed, A.A.; Alamri, M.S.; Anjum, F.M. Nutritional, biological, and therapeutic properties of black garlic: A critical review. Int. J. Food Prop. 2021, 24, 1387–1402. [Google Scholar] [CrossRef]
- Alam, M.A.; Uddin, R.; Subhan, N.; Rahman, M.M.; Jain, P.; Reza, H.M. Beneficial role of bitter melon supplementation in obesity and related complications in metabolic syndrome. J. Lipids 2015, 2015, 496169. [Google Scholar] [CrossRef]
- Kwatra, D.; Dandawate, P.; Padhye, S.; Anant, S. Bitter melon as a therapy for diabetes, inflammation, and cancer: A panacea? Curr. Pharmacol. Rep. 2016, 2, 34–44. [Google Scholar] [CrossRef]
- Murugesan, A.; Yadav, S.K.R.; Dixit, A. Anti-hyperglycemic activity of HPLC-fractionated Momordica charantia seed extract enriched in a novel napin-like protein in experimental diabetic rats and its validation with recombinant napin-like protein. Curr. Res. Biotechnol. 2022, 4, 179–189. [Google Scholar] [CrossRef]
- Salleh, N.H.; Zulkipli, I.N.; Yasin, H.M.; Ja’afar, F.; Ahmad, N.; Ahmad, W.A.N.W.; Ahmad, S.R. Systematic Review of Medicinal Plants Used for Treatment of Diabetes in Human Clinical Trials: An ASEAN Perspective. Evid.-Based Complement. Altern. Med. 2021, 2021, 5570939. [Google Scholar] [CrossRef]
- Choudhary, S.K.; Chhabra, G.; Sharma, D.; Vashishta, A.; Ohri, S.; Dixit, A. Comprehensive Evaluation of Anti-hyperglycemic Activity of Fractionated Momordica charantia Seed Extract in Alloxan-Induced Diabetic Rats. Evid.-Based Complement. Altern. Med. 2012, 2012, 293650. [Google Scholar] [CrossRef]
- Wang, S.; Li, Z.; Yang, G.; Ho, C.-T.; Li, S. Momordica charantia: A popular health-promoting vegetable with multifunctionality. Food Funct. 2017, 8, 1749–1762. [Google Scholar] [CrossRef]
- Turdu, G.; Gao, H.; Jiang, Y.; Kabas, M. Plant dipeptidyl peptidase-IV inhibitors as antidiabetic agents: A brief review. Futur. Med. Chem. 2018, 10, 1229–1239. [Google Scholar] [CrossRef] [PubMed]
- Olawale, F.; Olofinsan, K.; Iwaloye, O.; Ologuntere, T.E. Phytochemicals from Nigerian medicinal plants modulate therapeutically-relevant diabetes targets: Insight from computational direction. Adv. Tradit. Med. 2022, 22, 723–737. [Google Scholar] [CrossRef]
- Chou, W.-L. Therapeutic potential of targeting intestinal bitter taste receptors in diabetes associated with dyslipidemia. Pharmacol. Res. 2021, 170, 105693. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Shan, B.; Liao, C.-H.; Xie, J.-H.; Wen, P.-W.; Shi, J.-Y. Anti-diabetic properties of Momordica charantia L. polysaccharide in alloxan-induced diabetic mice. Int. J. Biol. Macromol. 2015, 81, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Fuangchan, A.; Sonthisombat, P.; Seubnukarn, T.; Chanouan, R.; Chotchaisuwat, P.; Sirigulsatien, V.; Ingkaninan, K.; Plianbangchang, P.; Haines, S.T. Hypoglycemic effect of bitter melon compared with metformin in newly diagnosed type 2 diabetes patients. J. Ethnopharmacol. 2011, 134, 422–428. [Google Scholar] [CrossRef]
- Bortolotti, M.; Mercatelli, D.; Polito, L. Momordica charantia, a Nutraceutical Approach for Inflammatory Related Diseases. Front. Pharmacol. 2019, 10, 486. [Google Scholar] [CrossRef]
- Kim, S.K.; Jung, J.; Jung, J.H.; Yoon, N.; Kang, S.S.; Roh, G.S.; Hahm, J.R. Hypoglycemic efficacy and safety of Momordica charantia (bitter melon) in patients with type 2 diabetes mellitus. Complement. Ther. Med. 2020, 52, 102524. [Google Scholar] [CrossRef]
- Patel, S. Hibiscus sabdariffa: An ideal yet under-exploited candidate for nutraceutical applications. Biomed. Prev. Nutr. 2014, 4, 23–27. [Google Scholar] [CrossRef]
- Riaz, G.; Chopra, R. A review on phytochemistry and therapeutic uses of Hibiscus sabdariffa L. Biomed. Pharmacother. 2018, 102, 575–586. [Google Scholar] [CrossRef]
- Amos, A.; Khiatah, B. Mechanisms of Action of Nutritionally Rich Hibiscus sabdariffa’s Therapeutic Uses in Major Common Chronic Diseases: A Literature Review. J. Am. Nutr. Assoc. 2022, 41, 116–124. [Google Scholar] [CrossRef]
- Shen, C.-Y.; Zhang, T.-T.; Zhang, W.-L.; Jiang, J.-G. Anti-inflammatory activities of essential oil isolated from the calyx of Hibiscus sabdariffa L. Food Funct. 2016, 7, 4451–4459. [Google Scholar] [CrossRef]
- Morales-Luna, E.; Pérez-Ramírez, I.F.; Salgado, L.M.; Castaño-Tostado, E.; A Gómez-Aldapa, C.; Reynoso-Camacho, R. The main beneficial effect of roselle (Hibiscus sabdariffa) on obesity is not only related to its anthocyanin content. J. Sci. Food Agric. 2019, 99, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Hapsari, B.W.; Setyaningsih, W. Methodologies in the analysis of phenolic compounds in roselle (Hibiscus sabdariffa L.): Composition, biological activity, and beneficial effects on human health. Horticulturae 2021, 7, 35. [Google Scholar] [CrossRef]
- Izquierdo-Vega, J.A.; Arteaga-Badillo, D.A.; Sánchez-Gutiérrez, M.; Morales-González, J.A.; Vargas-Mendoza, N.; Gómez-Aldapa, C.A.; Madrigal-Santillán, E. Organic acids from Roselle (Hibiscus sabdariffa L.)—A brief review of its pharmacological effects. Biomedicines 2020, 8, 100. [Google Scholar] [CrossRef]
- Kapoor, M.; Kaur, G.; Kaur, N.; Sharma, C.; Batra, K.; Singh, D. The Traditional Uses, Phytochemistry and Pharmacology of Genus Hibiscus: A Review. Eur. J. Med. Plants 2021, 32, 1–37. [Google Scholar] [CrossRef]
- Mardiah, M.; Zakaria, F.R.; Prangdimurti, E.; Damanik, R. The effect of roselle extract (Hibiscus sabdariffa Linn.) on blood glucose level and total antioxidant level on diabetic rat induced by streptozotocin. IOSR J. Pharm. 2014, 4, 8–16. [Google Scholar]
- Harrison, A.P.; Cooper, R.G.; Suliman, M.A.; Alalami, U. The Efficacy of Karkadeh Tea in Controlling Post-Prandial Blood Glucose Levels. Am. J. Pharmacol. Toxicol. 2009, 4, 151–157. [Google Scholar] [CrossRef]
- Lechner, J.F.; Stoner, G.D. Gingers and Their Purified Components as Cancer Chemopreventative Agents. Molecules 2019, 24, 2859. [Google Scholar] [CrossRef]
- Li, Y.; Tran, V.H.; Duke, C.C.; Roufogalis, B.D. Preventive and protective properties of Zingiber officinale (ginger) in diabetes mellitus, diabetic complications, and associated lipid and other metabolic disorders: A brief review. Evid. Based Complement. Altern. Med. 2012, 2012, 516870. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Zhang, Y. Research Progress on Chemical Constituents of Zingiber officinale Roscoe. BioMed Res. Int. 2019, 2019, 1–21. [Google Scholar] [CrossRef]
- Anh, N.H.; Kim, S.J.; Long, N.P.; Min, J.E.; Yoon, Y.C.; Lee, E.G.; Kim, M.; Kim, T.J.; Yang, Y.Y.; Son, E.Y.; et al. Ginger on Human Health: A Comprehensive Systematic Review of 109 Randomized Controlled Trials. Nutrients 2020, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.-Q.; Xu, X.-Y.; Cao, S.-Y.; Gan, R.-Y.; Corke, H.; Beta, T.; Li, H.-B. Bioactive Compounds and Bioactivities of Ginger (Zingiber officinale Roscoe). Foods 2019, 8, 185. [Google Scholar] [CrossRef]
- Shidfar, F.; Rajab, A.; Rahideh, T.; Khandouzi, N.; Hosseini, S.; Shidfar, S. The effect of ginger (Zingiber officinale) on glycemic markers in patients with type 2 diabetes. J. Complement. Integr. Med. 2015, 12, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Jafri, S.A.; Abass, S.; Qasim, M. Hypoglycemic effect of ginger (Zingiber officinale) in alloxan induced diabetic rats (Rattus norvagicus). Pak. Vet. J. 2011, 31, 160–162. [Google Scholar]
- Arablou, T.; Aryaeian, N.; Valizadeh, M.; Sharifi, F.; Hosseini, A.F.; Djalali, M. The effect of ginger consumption on glycemic status, lipid profile and some inflammatory markers in patients with type 2 diabetes mellitus. Int. J. Food Sci. Nutr. 2014, 65, 515–520. [Google Scholar] [CrossRef]
- Priya Rani, M.; Padmakumari, K.P.; Sankarikutty, B.; Lijo Cherian, O.; Nisha, V.M.; Raghu, K.G. Inhibitory potential of ginger extracts against enzymes linked to type 2 diabetes, inflammation and induced oxidative stress. Int. J. Food Sci. Nutr. 2011, 62, 106–110. [Google Scholar] [CrossRef]
- Misawa, K.; Hashizume, K.; Yamamoto, M.; Minegishi, Y.; Hase, T.; Shimotoyodome, A. Ginger extract prevents high-fat diet-induced obesity in mice via activation of the peroxisome proliferator-activated receptor δ pathway. J. Nutr. Biochem. 2015, 26, 1058–1067. [Google Scholar] [CrossRef]
- Kalra, S.; Aggarwal, S. Vitamin D and diabetes. J. Pak. Med. Assoc. 2021, 71, 383–384. [Google Scholar]
- Puvvada, R.C. Association of vitamin C status in diabetes mellitus: Prevalence and predictors of vitamin C deficiency. Futur. J. Pharm. Sci. 2020, 6, 30. [Google Scholar] [CrossRef]
- Alkholy, U.M.; Abdalmonem, N.; Zaki, A.; Elkoumi, M.A.; Hashim, M.I.A.; Basset, M.A.; Salah, H.E. The antioxidant status of coenzyme Q10 and vitamin E in children with type 1 diabetes. J. Pediatr. 2019, 95, 224–230. [Google Scholar] [CrossRef]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. [Google Scholar] [CrossRef]
- Khan, M.U.; Gautam, G.; Jan, B.; Zahiruddin, S.; Parveen, R.; Ahmad, S. Vitamin D from Vegetable VV Sources: Hope for the Future. Phytomed. Plus 2022, 2, 100248. [Google Scholar] [CrossRef]
- Baur, A.C.; Brandsch, C.; König, B.; Hirche, F.; Stangl, G.I. Plant Oils as Potential Sources of Vitamin D. Front. Nutr. 2016, 3, 29. [Google Scholar] [CrossRef]
- Saponaro, F.; Saba, A.; Zucchi, R. An update on vitamin D metabolism. Int. J. Mol. Sci. 2020, 21, 6573. [Google Scholar] [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [Google Scholar] [CrossRef]
- Tao, S.; Yuan, Q.; Mao, L.; Chen, F.-L.; Ji, F.; Cui, Z.-H. Vitamin D deficiency causes insulin resistance by provoking oxidative stress in hepatocytes. Oncotarget 2017, 8, 67605–67613. [Google Scholar] [CrossRef]
- Di Nisio, A.; De Toni, L.; Sabovic, I.; Rocca, M.S.; De Filippis, V.; Opocher, G.; Azzena, B.; Vettor, R.; Plebani, M.; Foresta, C. Impaired Release of Vitamin D in Dysfunctional Adipose Tissue: New Cues on Vitamin D Supplementation in Obesity. J. Clin. Endocrinol. Metab. 2017, 102, 2564–2574. [Google Scholar] [CrossRef]
- Zakhary, C.M.; Rushdi, H.; Hamdan, J.A.; Youssef, K.N.; Khan, A.; Abdalla, M.A.; Khan, S. Protective Role of Vitamin D Therapy in Diabetes Mellitus Type II. Cureus 2021, 13, e17317. [Google Scholar] [CrossRef]
- Nakashima, A.; Yokoyama, K.; Yokoo, T.; Urashima, M. Role of vitamin D in diabetes mellitus and chronic kidney disease. World J. Diabetes 2016, 7, 89–100. [Google Scholar] [CrossRef]
- Memon, F.P.; Bano, E.; Shamaun, S.; Afsheen, S. Role of Vitamins D Supplements in Preventing Development of Gestational Diabetes Mellitus. Pak. J. Med. Health Sci. 2022, 16, 545. [Google Scholar]
- von Hurst, P.R.; Stonehouse, W.; Coad, J. Vitamin D supplementation reduces insulin resistance in South Asian women living in New Zealand who are insulin resistant and vitamin D deficient–A randomised, placebo-controlled trial. Br. J. Nutr. 2010, 103, 549–555. [Google Scholar] [CrossRef]
- Harris, S.S.; Pittas, A.G.; Palermo, N.J. A randomized, placebo-controlled trial of vitamin D supplementation to improve glycaemia in overweight and obese African Americans. Diabetes Obes. Metab. 2012, 14, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Barzegari, M.; Sarbakhsh, P.; Mobasseri, M.; Noshad, H.; Esfandiari, A.; Khodadadi, B.; Gargari, B.P. The effects of vitamin D supplementation on lipid profiles and oxidative indices among diabetic nephropathy patients with marginal vitamin D status. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 542–547. [Google Scholar] [CrossRef]
- Tabesh, M.; Azadbakht, L.; Faghihimani, E.; Tabesh, M.; Esmaillzadeh, A. Effects of calcium–vitamin D co-supplementation on metabolic profiles in vitamin D insufficient people with type 2 diabetes: A randomised controlled clinical trial. Diabetologia 2014, 57, 2038–2047. [Google Scholar] [CrossRef]
- Aghadavod, E.; Soleimani, A.; Hamidi, G.; Keneshlou, F.; Heidari, A.; Asemi, Z. Effects of High-dose Vitamin E Supplementation on Markers of Cardiometabolic Risk and Oxidative Stress in Patients with Diabetic Nephropathy: A Randomized Double-blinded Controlled Trial. Iran. J. Kidney Dis. 2018, 12, 156–162. [Google Scholar]
- Dalan, R.; Ling, G.L. The protean role of haptoglobin and haptoglobin genotypes on vascular complications in diabetes mellitus. Eur. J. Prev. Cardiol. 2018, 25, 1502–1519. [Google Scholar] [CrossRef]
- Doseděl, M.; Jirkovský, E.; Macáková, K.; Krčmová, L.K.; Javorská, L.; Pourová, J.; On Behalf Of The Oemonom. Vitamin C—Sources, physiological role, kinetics, deficiency, use, toxicity, and determination. Nutrients 2021, 13, 615. [Google Scholar] [CrossRef]
- Rajendiran, D.; Packirisamy, S.; Gunasekaran, K. A review on role of antioxidants in diabetes. Asian J. Pharm. Clin. Res. 2018, 11, 48–53. [Google Scholar] [CrossRef]
- Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate Vitamin C Status in Prediabetes and Type 2 Diabetes Mellitus: Associations with Glycaemic Control, Obesity, and Smoking. Nutrients 2017, 9, 997. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.; Herrero, M.; Mendiola, J.; Oliva-Teles, M.; Ibáñez, E.; Delerue-Matos, C.; Oliveira, M. Fresh-cut aromatic herbs: Nutritional quality stability during shelf-life. LWT 2014, 59, 101–107. [Google Scholar] [CrossRef]
- Kevers, C.; Pincemail, J.; Tabart, J.; Defraigne, J.-O.; Dommes, J. Influence of Cultivar, Harvest Time, Storage Conditions, and Peeling on the Antioxidant Capacity and Phenolic and Ascorbic Acid Contents of Apples and Pears. J. Agric. Food Chem. 2011, 59, 6165–6171. [Google Scholar] [CrossRef] [PubMed]
- Ellong, E.N.; Billard, C.; Adenet, S.; Rochefort, K. Polyphenols, Carotenoids, Vitamin C Content in Tropical Fruits and Vegetables and Impact of Processing Methods. Food Nutr. Sci. 2015, 06, 299–313. [Google Scholar] [CrossRef]
- Wang, J.; Law, C.L.; Mujumdar, A.S.; Xiao, H.W. The degradation mechanism and kinetics of vitamin C in fruits and vegetables during thermal processing. Dry. Technol. Foods Fundam. Appl. 2018. [Google Scholar]
- Njoku, P.; Ayuk, A.; Okoye, C. Temperature Effects on Vitamin C Content in Citrus Fruits. Pak. J. Nutr. 2011, 10, 1168–1169. [Google Scholar] [CrossRef]
- Olofsson, C.; Discacciati, A.; Åkesson, A.; Orsini, N.; Brismar, K.; Wolk, A. Changes in fruit, vegetable and juice consumption after the diagnosis of type 2 diabetes: A prospective study in men. Br. J. Nutr. 2017, 117, 712–719. [Google Scholar] [CrossRef]
- Mason, S.A.; Rasmussen, B.; van Loon, L.J.; Salmon, J.; Wadley, G.D. Ascorbic acid supplementation improves postprandial glycaemic control and blood pressure in individuals with type 2 diabetes: Findings of a randomized cross-over trial. Diabetes Obes. Metab. 2019, 21, 674–682. [Google Scholar] [CrossRef]
- Carr, A.C.; Spencer, E.; Heenan, H.; Lunt, H.; Vollebregt, M.; Prickett, T.C.R. Vitamin C Status in People with Types 1 and 2 Diabetes Mellitus and Varying Degrees of Renal Dysfunction: Relationship to Body Weight. Antioxidants 2022, 11, 245. [Google Scholar] [CrossRef]
- Nani, D.; Proverawati, A. Immunomodulatory effects of black solo garlic (Allium sativum L.) on streptozotocin-induced diabetes in Wistar rats. Heliyon 2021, 7, e08493. [Google Scholar]
- Parham, M.; Bagherzadeh, M.; Asghari, M.; Akbari, H.; Hosseini, Z.; Rafiee, M.; Vafaeimanesh, J. Evaluating the effect of a herb on the control of blood glucose and insulin-resistance in patients with advanced type 2 diabetes (a double-blind clinical trial). Casp. J. Intern. Med. 2020, 11, 12–20. [Google Scholar] [CrossRef]
- Cheng, R.Z. Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID-19)? Med. Drug Discov. 2020, 5, 100028. [Google Scholar] [CrossRef]
- Gillani, S.W.; Sulaiman, S.A.S.; Abdul, M.I.M.; Baig, M.R. Combined effect of metformin with ascorbic acid versus acetyl salicylic acid on diabetes-related cardiovascular complication; a 12-month single blind multicenter randomized control trial. Cardiovasc. Diabetol. 2017, 16, 103. [Google Scholar] [CrossRef]
- Ashor, A.; Werner, A.D.; Lara, J.; Willis, N.D.; Mathers, J.C.; Siervo, M. Effects of vitamin C supplementation on glycaemic control: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2017, 71, 1371–1380. [Google Scholar] [CrossRef]
- Joseph, B.; Jini, D. Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac. J. Trop. Dis. 2013, 3, 93–102. [Google Scholar] [CrossRef]
- Aljohi, A.; Matou-Nasri, S.; Ahmed, N. Antiglycation and Antioxidant Properties of Momordica charantia. PLoS ONE 2016, 11, e0159985. [Google Scholar] [CrossRef]
- Ratwita, W.; Djamaludin, M.; Sa’adah, H.; Maharani, S. Subchronic Toxicity of Ethanol Extract of Bitter Melon PULP (Momordica Charantia L.) on Liver Function and Histopathological Changes in Wistar Rats. Pharmacogn. J. 2021, 13, 949–957. [Google Scholar] [CrossRef]
- Yusof, N.M.; Zainalabidin, S.; Fauzi, N.M.; Budin, S. Cardioprotective Effects of Roselle (Hibiscus Sabdariffa Linn.) Polyphenol-Rich Extract in Streptozotocin-Induced Diabetic Rats. Int. J. Cardiol. 2017, 249, S4. [Google Scholar] [CrossRef]
- Kaur, N.; Kumar, V.; Nayak, S.K.; Wadhwa, P.; Kaur, P.; Sahu, S.K. Alpha-amylase as molecular target for treatment of diabetes mellitus: A comprehensive review. Chem. Biol. Drug Des. 2021, 98, 539–560. [Google Scholar] [CrossRef]
- Khodaeian, M.; Tabatabaei-Malazy, O.; Qorbani, M.; Farzadfar, F.; Amini, P.; Larijani, B. Effect of vitamins C and E on insulin resistance in diabetes: A meta-analysis study. Eur. J. Clin. Investig. 2015, 45, 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Mahluji, S.; Attari, V.E.; Mobasseri, M.; Payahoo, L.; Ostadrahimi, A.; Golzari, S.E. Effects of ginger (Zingiber officinale) on plasma glucose level, HbA1c and insulin sensitivity in type 2 diabetic patients. Int. J. Food Sci. Nutr. 2013, 64, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.M.; Maahs, D.M.; Daniels, S.R.; de Ferranti, S.D.; Dichek, H.L.; Flynn, J.; Goldstein, B.I.; Kelly, A.S.; Nadeau, K.J.; Martyn-Nemeth, P.; et al. Highlighting Diabetes Mellitus. Arter. Thromb. Vasc. Biol. 2018, 38, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Duran-Lopez, L.; Dominguez-Morales, J.P.; Rios-Navarro, A.; Gutierrez-Galan, D.; Jimenez-Fernandez, A.; Vicente-Diaz, S.; Linares-Barranco, A. Performance Evaluation of Deep Learning-Based Prostate Cancer Screening Methods in Histopathological Images: Measuring the Impact of the Model’s Complexity on Its Processing Speed. Sensors 2021, 21, 1122. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Gupta, M.; Popli, H.; Aggarwal, G. Diabetes mellitus treatment using herbal drugs. Int. J. Phytomed. 2018, 10, 1–10. [Google Scholar] [CrossRef]
- Hasanpour, M.; Iranshahy, M.; Iranshahi, M. The application of metabolomics in investigating anti-diabetic activity of medicinal plants. Biomed. Pharmacother. 2020, 128, 110263. [Google Scholar] [CrossRef]
- Policardo, L.; Seghieri, G.; Anichini, R.; De Bellis, A.; Franconi, F.; Francesconi, P.; Mannucci, E. Effect of diabetes on hospitalization for ischemic stroke and related in-hospital mortality: A study in Tuscany, Italy, over years 2004–2011. Diabetes/Metab. Res. Rev. 2015, 31, 280–286. [Google Scholar] [CrossRef]
- Bragg, F.; Holmes, M.V.; Iona, A.; Guo, Y.; Du, H.; Chen, Y.; Bian, Z.; Yang, L.; Herrington, W.; Bennett, D.; et al. Association Between Diabetes and Cause-Specific Mortality in Rural and Urban Areas of China. JAMA 2017, 317, 280–289. [Google Scholar] [CrossRef]
- Yang, J.J.; Yu, D.; Wen, W.; Saito, E.; Rahman, S.; Shu, X.O.; Zheng, W. Association of diabetes with all-cause and cause-specific mortality in Asia: A pooled analysis of more than 1 million participants. JAMA Netw. Open 2019, 2, e192696. [Google Scholar] [CrossRef]
- Malode, L.L.; Manwar, J.V.; Panchale, W.A.; Bartere, S.A.; Bakal, R.L. Potential of medicinal plants in management of diabetes: An updates. GSC Adv. Res. Rev. 2021, 8, 149–159. [Google Scholar] [CrossRef]
- Ansari, P.; Akther, S.; Hannan, J.M.A.; Seidel, V.; Nujat, N.J.; Abdel-Wahab, Y.H.A. Pharmacologically Active Phytomolecules Isolated from Traditional Antidiabetic Plants and Their Therapeutic Role for the Management of Diabetes Mellitus. Molecules 2022, 27, 4278. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yedjou, C.G.; Grigsby, J.; Mbemi, A.; Nelson, D.; Mildort, B.; Latinwo, L.; Tchounwou, P.B. The Management of Diabetes Mellitus Using Medicinal Plants and Vitamins. Int. J. Mol. Sci. 2023, 24, 9085. https://doi.org/10.3390/ijms24109085
Yedjou CG, Grigsby J, Mbemi A, Nelson D, Mildort B, Latinwo L, Tchounwou PB. The Management of Diabetes Mellitus Using Medicinal Plants and Vitamins. International Journal of Molecular Sciences. 2023; 24(10):9085. https://doi.org/10.3390/ijms24109085
Chicago/Turabian StyleYedjou, Clement G., Jameka Grigsby, Ariane Mbemi, Daryllynn Nelson, Bryan Mildort, Lekan Latinwo, and Paul B. Tchounwou. 2023. "The Management of Diabetes Mellitus Using Medicinal Plants and Vitamins" International Journal of Molecular Sciences 24, no. 10: 9085. https://doi.org/10.3390/ijms24109085