
Intraarticular Injections of Mesenchymal Stem Cells in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Efficacy

Abstract
:1. Introduction
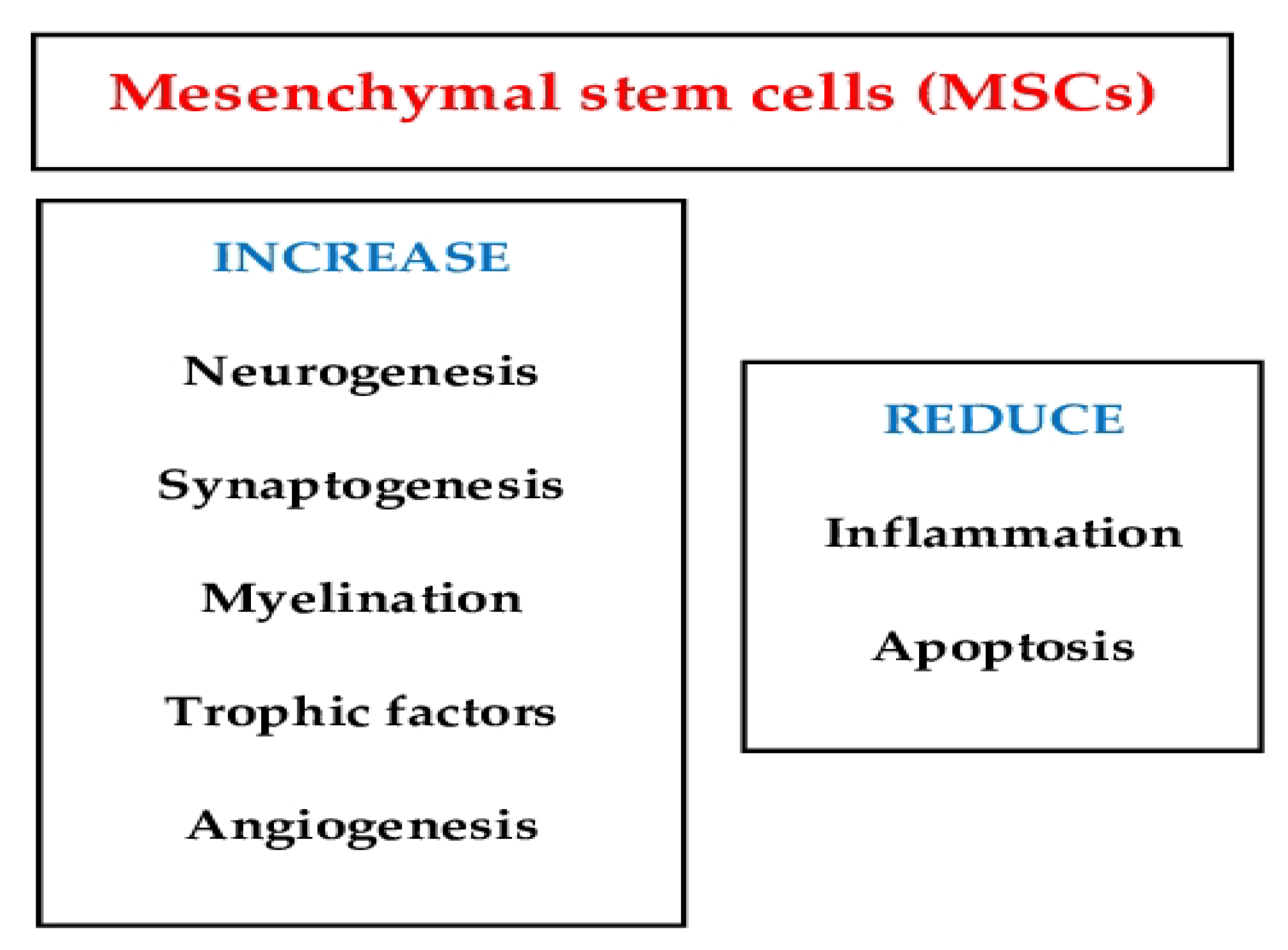
2. MSCs’ Molecular Mechanisms of Action
3. Efficacy of Intraarticular MSCs Injections in Knee Osteoarthritis
3.1. Experimental Studies
3.2. Clinical Studies
3.2.1. Systematic Reviews
3.2.2. Randomized Controlled Trials (RCTs)
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodriguez-Merchan, E.C. Intra-articular injections of hyaluronic acid and other drugs in the knee joint. HSS J. 2013, 9, 180–182. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Pan, J.; Lu, Z.; Zhu, H.; Guo, J.; Xie, D. The application of platelet-rich plasma in the treatment of knee osteoarthritis: A literature review. J. Orthop. Sci. 2022, 27, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Losina, E.; Weinstein, A.M.; Reichmann, W.M.; Burbine, S.A.; Solomon, D.H.; Daigle, M.E.; Rome, B.N.; Chen, S.P.; Hunter, D.J.; Suter, E.G.; et al. Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US. Arthritis Care Res. 2013, 65, 703–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyère, O.; Honvo, G.; Veronese, N.; Arden, N.K.; Branco, J.; Curtis, E.M.; Al-Daghri, N.M.; Herrero-Beaumont, G.; Martel-Pelletier, J.; Pelletier, J.P.; et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Semin. Arthritis Rheum. 2019, 49, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Machado, G.C.; Maher, C.G.; Ferreira, P.H.; Pinheiro, M.B.; Lin, C.W.; Day, R.O.; McLachlan, A.J.; Ferreira, M.L. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: Systematic review and meta-analysis of randomised placebo controlled trials. BMJ 2015, 350, h1225. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2015, 1, CD004376. [Google Scholar] [CrossRef]
- Cohen, S.A.; Zhuang, T.; Xiao, M.; Michaud, J.B.; Amanatullah, D.F.; Kamal, R.N. Google trends analysis shows increasing public interest in platelet-rich plasma injections for hip and knee osteoarthritis. J. Arthroplast. 2021, 36, 3616–3622. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Intra-articular platelet-rich plasma injections in knee osteoarthritis: A review of their current molecular mechanisms of action and their degree of efficacy. Int. J. Mol. Sci. 2022, 23, 1301. [Google Scholar] [CrossRef]
- Bovis, S.; Jarocha, D.; Majka, M. Mesenchymal stem cells: Characteristics and clinical applications. Folia Histochem. Cytobiol. 2006, 44, 215–230. [Google Scholar]
- Jang, S.; Lee, K.; Ju, J.H. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int. J. Mol. Sci. 2021, 22, 2619. [Google Scholar] [CrossRef] [PubMed]
- Doyle, E.C.; Wragg, N.M.; Wilson, S.L. Intraarticular injection of bone marrow-derived mesenchymal stem cells enhances regeneration in knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3827–3842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Yu, D.; Liu, Z.; Zhou, F.; Dai, J.; Wu, B.; Zhou, J.; Heng, B.C.; Zou, X.H.; Ouyang, H.; et al. Exosomes from embryonic mesenchymal stem cells alleviate osteoarthritis through balancing synthesis and degradation of cartilage extracellular matrix. Stem Cell Res. Ther. 2017, 8, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, C.; Huang, W.; Chen, Q.; Xu, J.; Yao, G.; Li, B.; Wu, T.; Yin, C.; Cheng, X. LncRNA Malat-1 From MSCs-Derived extracellular vesicles suppresses inflammation and cartilage degradation in osteoarthritis. Front. Bioeng. Biotechnol. 2021, 9, 772002. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wang, X.; Fan, Y.; Song, X.; Wu, J.; Fu, Z.; Li, T.; Huang, Y.; Tang, Z.; Meng, S.; et al. Tropoelastin improves adhesion and migration of intra-articular injected infrapatellar fat pad MSCs and reduces osteoarthritis progression. Bioact. Mater. 2021, 10, 443–459. [Google Scholar] [CrossRef]
- Lee, Y.; Park, Y.S.; Choi, N.Y.; Kim, Y.I.; Koh, Y.G. Proteomic analysis reveals commonly secreted proteins of mesenchymal stem cells derived from bone marrow, adipose tissue, and synovial membrane to show potential for cartilage regeneration in knee osteoarthritis. Stem Cells Int. 2021, 2021, 6694299. [Google Scholar] [CrossRef]
- Sekiya, I.; Katano, H.; Ozeki, N. Characteristics of MSCs in synovial fluid and mode of action of intra-articular injections of synovial MSCs in knee osteoarthritis. Int. J. Mol. Sci. 2021, 22, 2838. [Google Scholar] [CrossRef]
- Zhai, Q.; Chen, X.; Fei, D.; Guo, X.; He, X.; Zhao, W.; Shi, S.; Gooding, J.J.; Jin, F.; Jin, Y.; et al. Nanorepairers rescue inflammation-induced mitochondrial dysfunction in mesenchymal stem cells. Adv. Sci. 2022, 9, e2103839. [Google Scholar] [CrossRef]
- Xing, D.; Kwong, J.; Yang, Z.; Hou, Y.; Zhang, W.; Ma, B.; Lin, J. Intra-articular injection of mesenchymal stem cells in treating knee osteoarthritis: A systematic review of animal studies. Osteoarthr. Cartil. 2018, 26, 445–461. [Google Scholar] [CrossRef] [Green Version]
- Xia, T.; Yu, F.; Zhang, K.; Wu, Z.; Shi, D.; Teng, H.; Shen, J.; Yang, X.; Jiang, Q. The effectiveness of allogeneic mesenchymal stem cells therapy for knee osteoarthritis in pigs. Ann. Transl. Med. 2018, 6, 404. [Google Scholar] [CrossRef]
- Cheng, J.H.; Wang, C.J.; Chou, W.Y.; Hsu, S.L.; Chen, J.H.; Hsu, T.C. Comparison efficacy of ESWT and Wharton’s jelly mesenchymal stem cell in early osteoarthritis of rat knee. Am. J. Transl. Res. 2019, 11, 586–598. [Google Scholar]
- Wu, J.; Kuang, L.; Chen, C.; Yang, J.; Zeng, W.N.; Li, T.; Chen, H.; Huang, S.; Fu, Z.; Li, J.; et al. miR-100-5p-abundant exosomes derived from infrapatellar fat pad MSCs protect articular cartilage and ameliorate gait abnormalities via inhibition of mTOR in osteoarthritis. Biomaterials 2019, 206, 87–100. [Google Scholar] [CrossRef]
- Geng, Y.; Chen, J.; Alahdal, M.; Chang, C.; Duan, L.; Zhu, W.; Mou, L.; Xiong, J.; Wang, M.; Wang, D. Intra-articular injection of hUC-MSCs expressing miR-140-5p induces cartilage self-repairing in the rat osteoarthritis. J. Bone Miner. Metab. 2020, 38, 277–288. [Google Scholar] [CrossRef]
- Mostafa, A.; Korayem, H.E.; Fekry, E.; Hosny, S. The effect of intra-articular versus intravenous injection of mesenchymal stem sells on experimentally-induced knee joint osteoarthritis. J. Microsc. Ultrastruct. 2020, 9, 31–38. [Google Scholar]
- Xu, X.; Liang, Y.; Li, X.; Ouyang, K.; Wang, M.; Cao, T.; Li, W.; Liu, J.; Xiong, J.; Li, B.; et al. Exosome-mediated delivery of kartogenin for chondrogenesis of synovial fluid-derived mesenchymal stem cells and cartilage regeneration. Biomaterials 2021, 269, 120539. [Google Scholar] [CrossRef]
- Jin, Y.; Xu, M.; Zhu, H.; Dong, C.; Ji, J.; Liu, Y.; Deng, A.; Gu, Z. Therapeutic effects of bone marrow mesenchymal stem cells-derived exosomes on osteoarthritis. J. Cell Mol. Med. 2021, 25, 9281–9294. [Google Scholar] [CrossRef]
- Xia, P.; Wang, Q.; Song, J.; Wang, X.; Wang, X.; Lin, Q.; Cheng, K.; Chen, A.; Li, X. Low-intensity pulsed ultrasound enhances the efficacy of bone marrow-derived MSCs in osteoarthritis cartilage repair by regulating autophagy-mediated exosome release. Cartilage 2022, 13, 19476035221093060. [Google Scholar] [CrossRef]
- Wu, H.; Peng, Z.; Xu, Y.; Sheng, Z.; Liu, Y.; Liao, Y.; Wang, Y.; Wen, Y.; Yi, J.; Xie, C.; et al. Engineered adipose-derived stem cells with IGF-1-modified mRNA ameliorates osteoarthritis development. Stem Cell Res. Ther. 2022, 13, 19. [Google Scholar] [CrossRef]
- Andersen, C.; Uvebrant, K.; Mori, Y.; Aarsvold, S.; Jacobsen, S.; Berg, L.C.; Lundgren-Åkerlund, E.; Lindegaard, C. Human integrin α10β1-selected mesenchymal stem cells home to cartilage defects in the rabbit knee and assume a chondrocyte-like phenotype. Stem Cell Res. Ther. 2022, 13, 206. [Google Scholar] [CrossRef]
- Hamdalla, H.M.; Ahmed, R.R.; Galaly, S.R.; Ahmed, O.M.; Naguib, I.A.; Alghamdi, B.S.; Abdul-Hamid, M. Assessment of the efficacy of bone marrow-derived mesenchymal stem cells against a monoiodoacetate-induced osteoarthritis model in Wistar rats. Stem Cells Int. 2022, 2022, 1900403. [Google Scholar] [CrossRef]
- Ai, M.; Hotham, W.E.; Pattison, L.A.; Ma, Q.; Henson, F.M.D.; Smith, E.S.J. Human mesenchymal stem cells and derived extracellular vesicles reduce sensory neuron hyperexcitability and pain behaviors in murine osteoarthritis. Arthritis Rheumatol. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- McKinney, J.M.; Pucha, K.A.; Doan, T.N.; Wang, L.; Weinstock, L.D.; Tignor, B.T.; Fowle, K.L.; Levit, R.D.; Wood, L.B.; Willett, N.J. Sodium alginate microencapsulation of human mesenchymal stromal cells modulates paracrine signaling response and enhances efficacy for treatment of established osteoarthritis. Acta Biomater. 2022, 141, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Xing, D.; Liu, W.; Zhu, Y.; Liu, H.; Yan, L.; Fan, K.; Liu, P.; Yu, B.; Li, J.J.; et al. Preclinical studies and clinical trials on mesenchymal stem cell therapy for knee osteoarthritis: A systematic review on models and cell doses. Int. J. Rheum. Dis. 2022, 25, 532–562. [Google Scholar] [CrossRef] [PubMed]
- Xia, P.; Wang, X.; Lin, Q.; Li, X. Efficacy of mesenchymal stem cells injection for the management of knee osteoarthritis: A systematic review and meta-analysis. Int. Orthop. 2015, 39, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- Cui, G.H.; Wang, Y.Y.; Li, C.J.; Shi, C.H.; Wang, W.S. Efficacy of mesenchymal stem cells in treating patients with osteoarthritis of the knee: A meta-analysis. Exp. Ther. Med. 2016, 12, 3390–3400. [Google Scholar] [CrossRef] [Green Version]
- Ha, C.W.; Park, Y.B.; Kim, S.H.; Lee, H.J. Intra-articular mesenchymal stem cells in osteoarthritis of the knee: A systematic review of clinical outcomes and evidence of cartilage repair. Arthroscopy 2019, 35, 277–288.e2. [Google Scholar] [CrossRef]
- Kim, S.H.; Ha, C.W.; Park, Y.B.; Nam, E.; Lee, J.E.; Lee, H.J. Intra-articular injection of mesenchymal stem cells for clinical outcomes and cartilage repair in osteoarthritis of the knee: A meta-analysis of randomized controlled trials. Arch. Orthop. Trauma Surg. 2019, 139, 971–980. [Google Scholar] [CrossRef]
- Di Matteo, B.; Vandenbulcke, F.; Vitale, N.D.; Iacono, F.; Ashmore, K.; Marcacci, M.; Kon, E. Minimally manipulated mesenchymal stem cells for the treatment of knee osteoarthritis: A systematic review of clinical evidence. Stem Cells Int. 2019, 2019, 1735242. [Google Scholar] [CrossRef] [Green Version]
- D’Arrigo, D.; Roffi, A.; Cucchiarini, M.; Moretti, M.; Candrian, C.; Filardo, G. Secretome and extracellular vesicles as new biological therapies for knee osteoarthritis: A systematic review. J. Clin. Med. 2019, 8, 1867. [Google Scholar] [CrossRef] [Green Version]
- Álvarez Hernández, P.; de la Mata Llord, J. Expanded mesenchymal stromal cells in knee osteoarthritis: A systematic literature review. Reumatol. Clin. Engl. Ed. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, J.; Xu, H.; Lin, Z.; Chang, H.; Liu, W.; Kong, L. Mesenchymal stem cells in knee osteoarthritis treatment: A systematic review and meta-analysis. J. Orthop. Transl. 2020, 24, 121–130. [Google Scholar] [CrossRef]
- Dai, W.; Leng, X.; Wang, J.; Shi, Z.; Cheng, J.; Hu, X.; Ao, Y. Intra-articular mesenchymal stromal cell injections are no different from placebo in the treatment of knee osteoarthritis: A systematic review and meta-analysis of randomized controlled rrials. Arthroscopy 2021, 37, 340–358. [Google Scholar] [CrossRef]
- Maheshwer, B.; Polce, E.M.; Paul, K.; Williams, B.T.; Wolfson, T.S.; Yanke, A.; Verma, N.N.; Cole, B.J.; Chahla, J. Regenerative potential of mesenchymal stem cells for the treatment of knee osteoarthritis and chondral defects: A systematic review and meta-analysis. Arthroscopy 2021, 37, 362–378. [Google Scholar] [CrossRef]
- Qu, H.; Sun, S. Efficacy of mesenchymal stromal cells for the treatment of knee osteoarthritis: A meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2021, 16, 11. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Kwan, Y.T.; Neo, W.J.; Chong, J.Y.; Kuek, T.Y.J.; See, J.Z.F.; Wong, K.L.; Toh, W.S.; Hui, J.H.P. Intra-articular injections of mesenchymal stem cells without adjuvant therapies for knee osteoarthritis: A systematic review and meta-analysis. Am. J. Sports Med. 2021, 49, 3113–3124. [Google Scholar] [CrossRef]
- Naja, M.; Fernandez De Grado, G.; Favreau, H.; Scipioni, D.; Benkirane-Jessel, N.; Musset, A.M.; Offner, D. Comparative effectiveness of nonsurgical interventions in the treatment of patients with knee osteoarthritis: A PRISMA-compliant systematic review and network meta-analysis. Medicine 2021, 100, e28067. [Google Scholar] [CrossRef]
- Muthu, S.; Kartheek, R.R.; Jeyaraman, N.; Rajendran, R.L.; Khanna, M.; Jeyaraman, M.; Packkyarathinam, R.P.; Gangadaran, P.; Ahn, B.C. Is culture expansion necessary in autologous mesenchymal stromal cell therapy to obtain superior results in the management of knee osteoarthritis?—Meta-analysis of randomized controlled trials. Bioengineering 2021, 8, 220. [Google Scholar] [CrossRef]
- Zhao, D.; Pan, J.K.; Yang, W.Y.; Han, Y.H.; Zeng, L.F.; Liang, G.H.; Liu, J. Intra-articular injections of platelet-rich plasma, adipose mesenchymal stem cells, and bone marrow mesenchymal stem cells associated with better outcomes than hyaluronic acid and saline in knee osteoarthritis: A systematic review and network meta-analysis. Arthroscopy 2021, 37, 2298–2314.e10. [Google Scholar] [CrossRef]
- Jeyaraman, M.; Muthu, S.; Ganie, P.A. Does the source of mesenchymal stem cell have an effect in the management of osteoarthritis of the knee? Meta-analysis of randomized controlled trials. Cartilage 2021, 13 (Suppl. S1), 1532S–1547S. [Google Scholar] [CrossRef]
- Muthu, S.; Mir, A.A.; Kumar, R.; Yadav, V.; Jeyaraman, M.; Khanna, M. What is the clinically significant ideal mesenchymal stromal cell count in the management of osteoarthritis of the knee?—Meta-analysis of randomized controlled trials. J. Clin. Orthop. Trauma 2021, 25, 101744. [Google Scholar] [CrossRef]
- Wei, Z.J.; Wang, Q.Q.; Cui, Z.G.; Inadera, H.; Jiang, X.; Wu, C.A. Which is the most effective one in knee osteoarthritis treatment from mesenchymal stem cells obtained from different sources?-A systematic review with conventional and network meta-analyses of randomized controlled trials. Ann. Transl. Med. 2021, 9, 452. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, T.G.; Winters, M.; Van den Boom, N.A.; Haisma, H.J.; Moen, M.H. Autologous stem cell therapy in knee osteoarthritis: A systematic review of randomised controlled trials. Br. J. Sports Med. 2021, 55, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, J.; Kraeutler, M.J.; Belk, J.W.; Scillia, A.J. Umbilical cord-derived stem cells for the treatment of knee osteoarthritis: A systematic review. Orthop. J. Sports Med. 2022, 10, 23259671221104409. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraman, M.; Shivaraj, B.; Bingi, S.K.; Ranjan, R.; Muthu, S.; Khanna, M. Does vehicle-based delivery of mesenchymal stromal cells give superior results in knee osteoarthritis? Meta-analysis of randomized controlled trials. J. Clin. Orthop. Trauma 2022, 25, 101772. [Google Scholar] [CrossRef] [PubMed]
- Shoukrie, S.I.; Venugopal, S.; Dhanoa, R.K.; Selvaraj, R.; Selvamani, T.Y.; Zahra, A.; Malla, J.; Hamouda, R.K.; Hamid, P.F. Safety and efficacy of injecting mesenchymal stem cells into a human knee joint to treat osteoarthritis: A systematic review. Cureus 2022, 14, e24823. [Google Scholar] [CrossRef]
- Vega, A.; Martín-Ferrero, M.A.; Del Canto, F.; Alberca, M.; García, V.; Munar, A.; Orozco, L.; Soler, R.; Fuertes, J.J.; Huguet, M.; et al. Treatment of knee osteoarthritis with allogeneic bone marrow mesenchymal stem cells: A randomized controlled trial. Transplantation 2015, 99, 1681–1690. [Google Scholar] [CrossRef]
- Lamo-Espinosa, J.M.; Mora, G.; Blanco, J.F.; Granero-Moltó, F.; Núñez-Córdoba, J.M.; López-Elío, S.; Andreu, E.; Sánchez-Guijo, F.; Aquerreta, J.D.; Bondía, J.M.; et al. Intra-articular injection of two different doses of autologous bone marrow mesenchymal stem cells versus hyaluronic acid in the treatment of knee osteoarthritis: Long-term follow up of a multicenter randomized controlled clinical trial (phase I/II). J. Transl. Med. 2018, 16, 213. [Google Scholar] [CrossRef] [Green Version]
- Matas, J.; Orrego, M.; Amenabar, D.; Infante, C.; Tapia-Limonchi, R.; Cadiz, M.I.; Alcayaga-Miranda, F.; González, P.L.; Muse, E.; Khoury, M.; et al. Umbilical cord-derived mesenchymal stromal cells (MSCs) for knee osteoarthritis: Repeated MSC dosing is superior to a single MSC dose and to hyaluronic acid in a controlled randomized phase I/II trial. Stem Cells Transl. Med. 2019, 8, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.S.; Kim, H.J.; Kim, K.I.; Kim, G.B.; Jin, W. Intra-articular injection of autologous adipose tissue-derived mesenchymal stem cells for the treatment of knee osteoarthritis: A phase IIb, randomized, placebo-controlled clinical trial. Stem Cells Transl. Med. 2019, 8, 504–511. [Google Scholar] [CrossRef] [Green Version]
- Lamo-Espinosa, J.M.; Blanco, J.F.; Sánchez, M.; Moreno, V.; Granero-Moltó, F.; Sánchez-Guijo, F.; Crespo-Cullel, Í.; Mora, G.; San Vicente, D.D.; Pompei-Fernández, O.; et al. Phase II multicenter randomized controlled clinical trial on the efficacy of intra-articular injection of autologous bone marrow mesenchymal stem cells with platelet rich plasma for the treatment of knee osteoarthritis. J. Transl. Med. 2020, 18, 356. [Google Scholar] [CrossRef]
- Bastos, R.; Mathias, M.; Andrade, R.; Amaral, R.J.F.C.; Schott, V.; Balduino, A.; Bastos, R.; Miguel Oliveira, J.; Reis, R.L.; Rodeo, S.; et al. Intra-articular injection of culture-expanded mesenchymal stem cells with or without addition of platelet-rich plasma is effective in decreasing pain and symptoms in knee osteoarthritis: A controlled, double-blind clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1989–1999. [Google Scholar] [CrossRef] [Green Version]
- Hernigou, P.; Bouthors, C.; Bastard, C.; Flouzat Lachaniette, C.H.; Rouard, H.; Dubory, A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: What better postpone knee arthroplasty at fifteen years? A randomized study. Int. Orthop. 2021, 45, 391–399. [Google Scholar] [CrossRef]
- Liu, X.; Robbins, S.; Wang, X.; Virk, S.; Schuck, K.; Deveza, L.A.; Oo, W.M.; Carmichael, K.; Antony, B.; Eckstein, F.; et al. Efficacy and cost-effectiveness of Stem Cell injections for symptomatic relief and strUctural improvement in people with Tibiofemoral knee OsteoaRthritis: Protocol for a randomised placebo-controlled trial (the SCUlpTOR trial). BMJ Open 2021, 11, e056382. [Google Scholar] [CrossRef]
- Ossendorff, R.; Walter, S.G.; Schildberg, F.A.; Khoury, M.; Salzmann, G.M. Controversies in regenerative medicine: Should knee joint osteoarthritis be treated with mesenchymal stromal cells? Eur. Cell Mater. 2022, 43, 98–111. [Google Scholar] [CrossRef]
- Neefjes, M.; Housmans, B.A.C.; van Beuningen, H.M.; Vitters, E.L.; van den Akker, G.G.H.; Welting, T.J.M.; van Caam, A.P.M.; van der Kraan, P.M. Prediction of the effect of the osteoarthritic joint microenvironment on cartilage repair. Tissue Eng. Part A 2022, 28, 27–37. [Google Scholar] [CrossRef]
- Li, C.; Zhao, H.; Cheng, L.; Wang, B. Allogeneic vs. autologous mesenchymal stem/stromal cells in their medication practice. Cell Biosci. 2021, 11, 187. [Google Scholar] [CrossRef]
- Rakian, R.; Block, T.J.; Johnson, S.M.; Marinkovic, M.; Wu, J.; Dai, Q.; Dean, D.D.; Chen, X.D. Native extracellular matrix preserves mesenchymal stem cell “stemness” and differentiation potential under serum-free culture conditions. Stem Cell Res. Ther. 2015, 6, 235. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.T.; Luo, J.; Sui, L.S.; Ma, X.; Yan, Z.J.; Lin, J.H.; Wang, Y.S.; Chen, Y.Z.; Jiang, X.D.; Xu, R.X. Effects of differentiated versus undifferentiated adipose tissue-derived stromal cell grafts on functional recovery after spinal cord contusion. Cell Mol. Neurobiol. 2009, 29, 1283–1292. [Google Scholar] [CrossRef]
- Cassano, J.M.; Schnabel, L.V.; Goodale, M.B.; Fortier, L.A. Inflammatory licensed equine MSCs are chondroprotective and exhibit enhanced immunomodulation in an inflammatory environment. Stem Cell Res. Ther. 2018, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Lynch, K.; Treacy, O.; Chen, X.; Murphy, N.; Lohan, P.; Islam, M.N.; Donohoe, E.; Griffin, M.D.; Watson, L.; McLoughlin, S.; et al. TGF-β1-licensed murine MSCs show superior therapeutic efficacy in modulating corneal allograft immune rejection in vivo. Mol. Ther. 2020, 28, 2023–2043. [Google Scholar] [CrossRef]
- Lu, S.; Qiao, X. Single-cell profiles of human bone marrow-derived mesenchymal stromal cells after IFN-γ and TNF-α licensing. Gene 2021, 771, 145347. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Li, X.; Xu, X.; Xu, L.; Wang, D.; Ouyang, K.; Liang, Y. Large-scale preparation of synovial fluid mesenchymal stem cell-derived exosomes by 3D bioreactor culture. J. Vis. Exp. 2022. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.; Meng, H.; Zhao, J.; Lin, W.; Liu, X.; Tian, Z.; Lan, L.; Yang, H.; Zou, Y.; Xu, Y.; et al. Injectable adipose-derived stem cells-embedded alginate-gelatin microspheres prepared by electrospray for cartilage tissue regeneration. J. Orthop. Transl. 2022, 33, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.N.; Zhu, S.Y.; He, H.C.; Yu, X.; Xu, Y.; He, C.Q. Mesenchymal stromal cell-based therapy for cartilage regeneration in knee osteoarthritis. Stem Cell Res. Ther. 2022, 13, 14. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors [Reference] | Year | Methods and Results | Participants | Level of Evidence | Conclusions |
|---|---|---|---|---|---|
| Xia et al. [34] | 2015 | MSCs injection had no substantial impact on pain. | 314 patients (7 RCTs) | I | The results of this review should be validated utilizing methodologically precise trials. |
| Cui et al. [35] | 2016 | MSC therapy in subjects with knee OA demonstrated continual effectiveness for 2 years. | 565 patients (18 clinical trials) | I | MSC utilization improved the overall results. |
| Xing et al. [19] | 2018 | This study demonstrated that modest reliance could be placed on safety of MSCs treatment for knee OA. | 23 animal studies | I | More high-quality research with high internal and external validity is still needed. |
| Ha et al. [36] | 2019 | All reports except two found significantly superior clinical results in the MSCs group. | 17 studies in patients with knee OA (6 RCTs, 8 prospective observational studies, 3 retrospective case-control studies). | III | Intraarticular MSCs render ameliorations in pain and function in knee OA at short-run follow-up (<28 months) in many cases. |
| Kim et al. [37] | 2019 | This study found significant improvements after treatment. | 220 patients (5 RCTs) | II | Intraarticular MSCs have limited evidence in pain alleviation and functional betterment in knee OA. |
| Di Matteo et al. [38] | 2019 | Twenty-three manuscripts were included in the final analysis. | 23 manuscripts about patients with knee OA (only 4 were RCTs) | NA | The poor quality of the reported studies averted any recommendation on the utilization of either product in a clinical practice. |
| D’Arrigo et al. [39] | 2019 | Encouraging in vitro outcomes were obtained in terms of enhanced cell proliferation, decrease of swelling. | Twenty in vivo and in vitro studies were analyzed. | NA | The different effects of EVs and secretome, and the identification of subjects who may benefit more from intraarticular injections of MSCs must be clarified. |
| Álvarez Hernández et al. [40] | 2020 | Data demonstrated clinical amelioration in 60% of subjects. Structural benefit was found in 50% of subjects. | 169 patients (3 RCTs, 6 QCTs) | NA | Intraarticular implants of MSCs appeared to be safe with no serious complications. Low-quality evidence averts conclusions regarding efficacy. |
| Song et al. [41] | 2020 | MSC therapy could substantially reduce VAS in a 1-year follow-up study compared with controls. | 58 patients (15 RCTs, two retrospective studies and two cohort studies) | NA | These authors suggested that MSC treatment could be efficacious and safe therapy for the treatment of OA. |
| Dai et al. [42] | 2021 | Compared with placebo, there was no significant difference in VAS for pain, WOMAC pain score, WOMAC function score, or WOMAC stiffness score for MSCs. | 13 RCTs (patients) | I | Intraarticular MSC injection was not encountered to be superior to placebo in pain alleviation and functional betterment for subjects with knee OA. |
| Maheshwer et al. [43] | 2021 | There was no substantial difference in pain alleviation between MSC treatment and controls. | 439 patients (25 studies) | II | MSCs rendered functional benefit only in subjects who experienced concurrent surgery. |
| Qu et al. [44] | 2021 | MSC treatment substantially diminished VAS, WOMAC pain, WOMAC stiffness, and WOMAC function scores at a long-run follow-up (1 or 2 years). | 476 patients (9 RCTs) | NA | The results of this study suggested that MSCs were a promising alternative for the management of subjects with knee OA. |
| Tan et al. [45] | 2021 | All studies reported amelioration in the results after MSC therapy. | 440 knees (19 studies) | NA | Intraarticular injections of MSCs without any adjuvant therapies improved pain and function for OA. |
| Naja et al. [46] | 2021 | This study assessed 7 approaches with WOMAC at 1 year: injection of PRP, corticosteroids, MSCs, hyaluronic acid, ozone, administration of NSAIDs with or without the association of physiotherapy. | 13 trials (patients) | NA | The results of treatments utilizing MSCs and PRP for the management of knee OA were associated with long-run improvements in pain and function. |
| Muthu et al. [47] | 2021 | At 6 months, culture expanded MSCs demonstrated pain alleviation. | 767 patients (17 studies) | NA | Culture expansion of autologous MSCs was not a necessary factor to attain better results in the treatment of knee OA. |
| Zhao et al. [48] | 2021 | This meta-analysis compared AD-MSCs, LP-PRP, and placebo. At 6 months, VAS scores and WOMAC pain subscores demonstrated that AD-MSCs were the best treatment alternative. | 43 studies (patients) | II | During 6 months of follow-up, AD-MSCs alleviated pain the best; LP-PRP was most efficacious for functional amelioration. |
| Jeyaraman et al. [49] | 2021 | At 6 months, 1 year and 2 years, AD-MSCs demonstrated substantially better VAS and WOMAC amelioration than BM-MSCs, respectively, compared to controls. | 811 patients (9 studies) | NA | This study established the effectiveness, safety, and superiority of AD-MSC transplantation, compared to BM-MSC, in the treatment of OA. |
| Muthu et al. [50] | 2021 | These authors categorized the studies based on the MSC count used in them into four cohorts, namely <1 × 107 MSCs (Cohort I), 1–5 × 107 MSCs (Cohort II), 5–10 × 107 MSCs (Cohort III), and >10 × 107 MSCs (Cohort IV). | 564 patients (14 studies) | NA | Cohort III demonstrated consistent substantial amelioration in pain and functional result analyzed compared to the other cohorts. Therefore, these authors advised a cell volume of 5–10 × 107 cells. |
| Wei et al. [51] | 2021 | The MSCs were deemed superior over placebo for pain alleviation and ameliorated function in KOA, but demonstrated no substantial differences for cartilage regeneration. Among all the MSCs, the AD-MSCs most effectively alleviated pain. | 203 patients (8 studies) | NA | The findings of this study suggested that MSCs were effective in the treatment of knee OA. However, the evidence did not support the utilization of MSCs for ameliorating cartilage repair in subjects with knee OA. |
| Wiggers et al. [52] | 2021 | After 1 year, 19 of 26 (73%) clinical outcome parameters ameliorated with MSCs compared with control. | 408 patients (14 RCTs) | NA | These authors encountered a positive impact of autologous MSC therapy compared with control treatments on PROMs, and illness severity. The quality of this evidence was low. |
| Álvarez Hernández et al. [40] | 2022 | Clinical improvement was found in 60% of subjects. Structural benefit was seen in 50% of subjects. | 169 patients (252 articles) | NA | Intraarticular implants of MSCs appeared to be safe, with no serious complications. Low-quality evidence precludes conclusions regarding effectiveness in this review. |
| Dhillon et al. [53] | 2022 | After a follow-up 23.4 months, weighted averages of the WOMAC, macroscopic ICRS, subjective IKDC, and VAS scores all demonstrated amelioration from before to after treatment. | 385 patients (7 studies) | NA | Subjects experiencing management of knee OA with hUC-MSCs might be expected to improve. |
| Jeyaraman et al. [54] | 2022 | At 6 months, both direct and vehicle-based delivery of MSCs demonstrated substantially better VAS amelioration. | 963 patients (21 studies) | NA | Employed methods of vehicle-based delivery of MSCs, such as PRP and hyaluronic acid, did not show better outcomes compared to direct delivery. |
| Shoukrie et al. [55] | 2022 | Substantial ameliorations were seen in the MSCs cohorts regarding KOOS, VAS, WOMAC, and MRI. Moreover, no serious complications were found. | 10 studies (723 patients) | NA | Intraarticular injections of MSCs were efficacious and safe in alleviating pain and ameliorating motor function in subjects with knee OA in the short run. |
| Authors [Reference] | Year | Methods and Results | Participants | Level of Evidence | Conclusions |
|---|---|---|---|---|---|
| Vega et al. [56] | 2015 | These authors randomized 30 subjects with chronic knee pain unresponsive to conservative management and exhibiting radiological evidence of OA into two cohorts of 15 subjects. The test cohort was treated with allogeneic bone marrow MSCs by intra-articular injection of 40 × 10(6) cells. The control cohort received intra-articular hyaluronic acid (60 mg, single dose). | 30 patients | NA | Allogeneic MSC treatment might be a valid option for the treatment of chronic knee OA. The procedure was simple, did not need surgery, provided pain alleviation, and substantially ameliorated cartilage quality. |
| Lamo-Espinosa et al. [57] | 2018 | In this phase I/II multicenter randomized clinical trial with active control, no complications were found after autologous bone marrow-derived MSCs (BM-MSCs) administration or during the follow-up. BM-MSCs-administered subjects improved according to VAS at the end of follow up. | 30 patients | NA | Single intraarticular injection of in vitro expanded autologous BM-MSCs was a safe and feasible technique that resulted in long-run clinical and functional amelioration of knee OA. |
| Matas et al. [58] | 2019 | Subjects with symptomatic knee OA were randomized to receive hyaluronic acid at baseline and 6 months (hyaluronic acid, n = 8), single-dose (20 × 106) UC-MSC at baseline (MSC-1, n = 9), or repeated UC-MSC doses at baseline and 6 months (20 × 106 × 2; MSC-2, n = 9). | 26 patients | NA | In this phase I/II trial, repeated UC-MSC therapy was safe and better than the comparative group at 1-year follow-up. |
| Lee et al. [59] | 2019 | Single injection of AD-MSCs led to a substantial amelioration of the WOMAC score at 6 months. In the control group, there was no significant change in the WOMAC score at 6 months. | 24 patients | NA | An intraarticular injection of autologous AD-MSCs rendered satisfactory functional amelioration and pain alleviation for subjects with knee OA without causing complications at 6-month follow-up. |
| Lamo-Espinosa et al. [60] | 2020 | These authors assessed the clinical impact of a dose of 100 × 106 cultured autologous BM-MSCs in combination with PRP (PRGF®) as adjuvant. No complications were found after BM-MSC administration or during follow-up. | 60 patients | NA | Treatment with BM-MSC associated with PRGF® was shown to be a viable therapeutic option for OA of the knee, with clinical improvement at the end of follow-up. |
| Bastos et al. [61] | 2020 | This study compared the clinical and laboratory results of intraarticular injections of culture-expanded bone-derived MSCs with or without PRP to intraarticular corticosteroid injections for the management of knee OA. | 47 patients | II | An intraarticular injection of bone marrow-derived culture-expanded MSCs with or without the addition of PRP was efficacious in ameliorating the diminishing function and symptoms caused by knee OA at 12-month follow-up. |
| Hernigou et al. [62] | 2021 | These authors compared subchondral bone to intraarticular injection of bone marrow concentrate MSCs in bilateral knee OA. The aim was to determine which one of them was better at postponing TKA at 15 years. | 60 patients (120 knees) | NA | Implantation of MSCs in the subchondral bone of an osteoarthritic knee was more efficacious at delaying TKA than injection of the same intraarticular dose in the contralateral knee with the same degree of OA. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Merchán, E.C. Intraarticular Injections of Mesenchymal Stem Cells in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Efficacy. Int. J. Mol. Sci. 2022, 23, 14953. https://doi.org/10.3390/ijms232314953
Rodríguez-Merchán EC. Intraarticular Injections of Mesenchymal Stem Cells in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Efficacy. International Journal of Molecular Sciences. 2022; 23(23):14953. https://doi.org/10.3390/ijms232314953
Chicago/Turabian StyleRodríguez-Merchán, Emérito Carlos. 2022. "Intraarticular Injections of Mesenchymal Stem Cells in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Efficacy" International Journal of Molecular Sciences 23, no. 23: 14953. https://doi.org/10.3390/ijms232314953