
Staphylococcus aureus Infection-Related Glomerulonephritis with Dominant IgA Deposition

 ,
,
Abstract
:1. Introduction
2. Review Methods
2.1. Literature Search
2.2. Categorize of Selected Cases
3. Clinical Features
3.1. Epidemiology and Characteristics
3.2. Epidemiology and Characteristics
3.3. Clinical Renal Features
3.4. Laboratory Findings
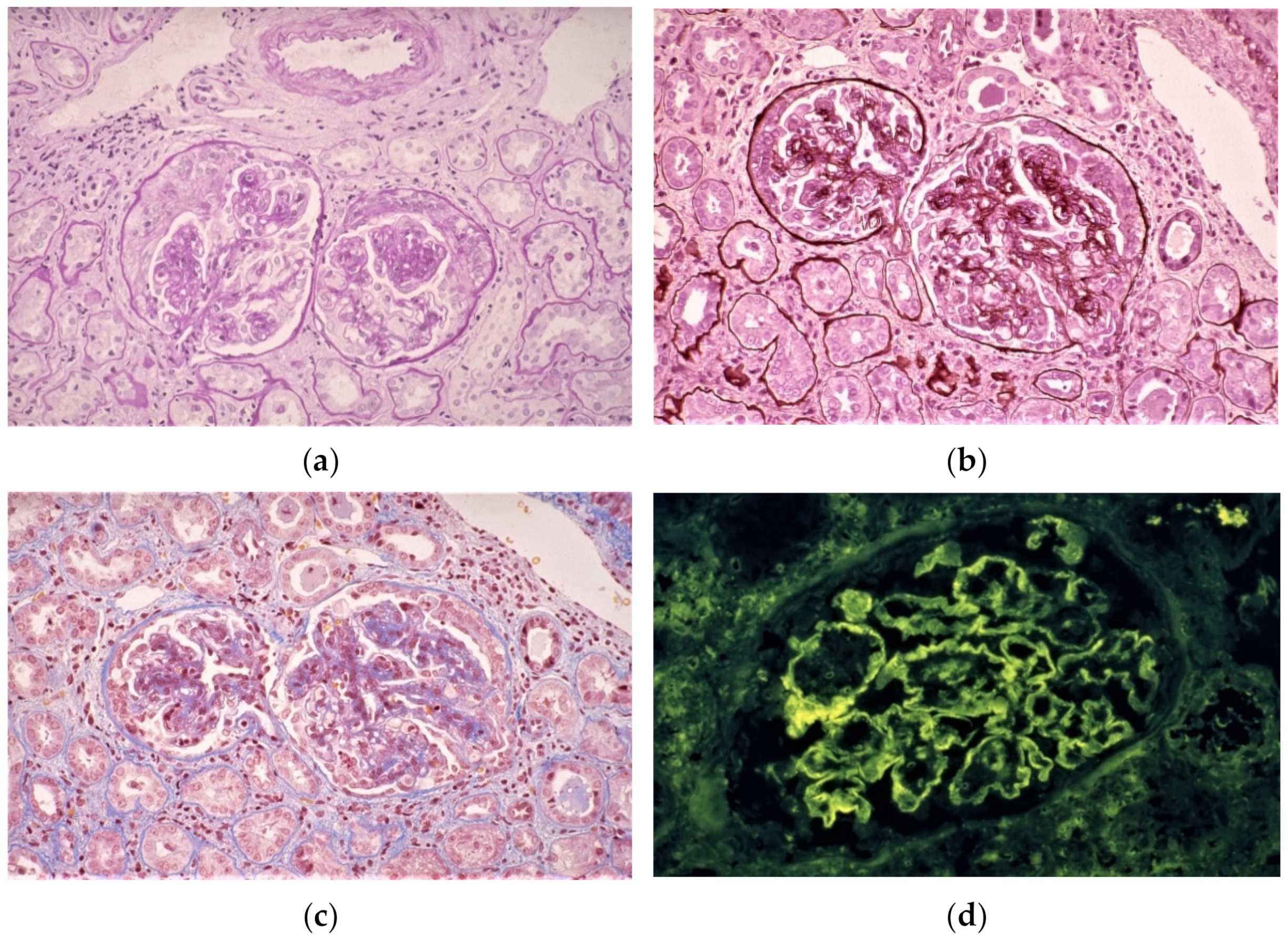
4. Histological Findings
4.1. Light Microscopy Findings
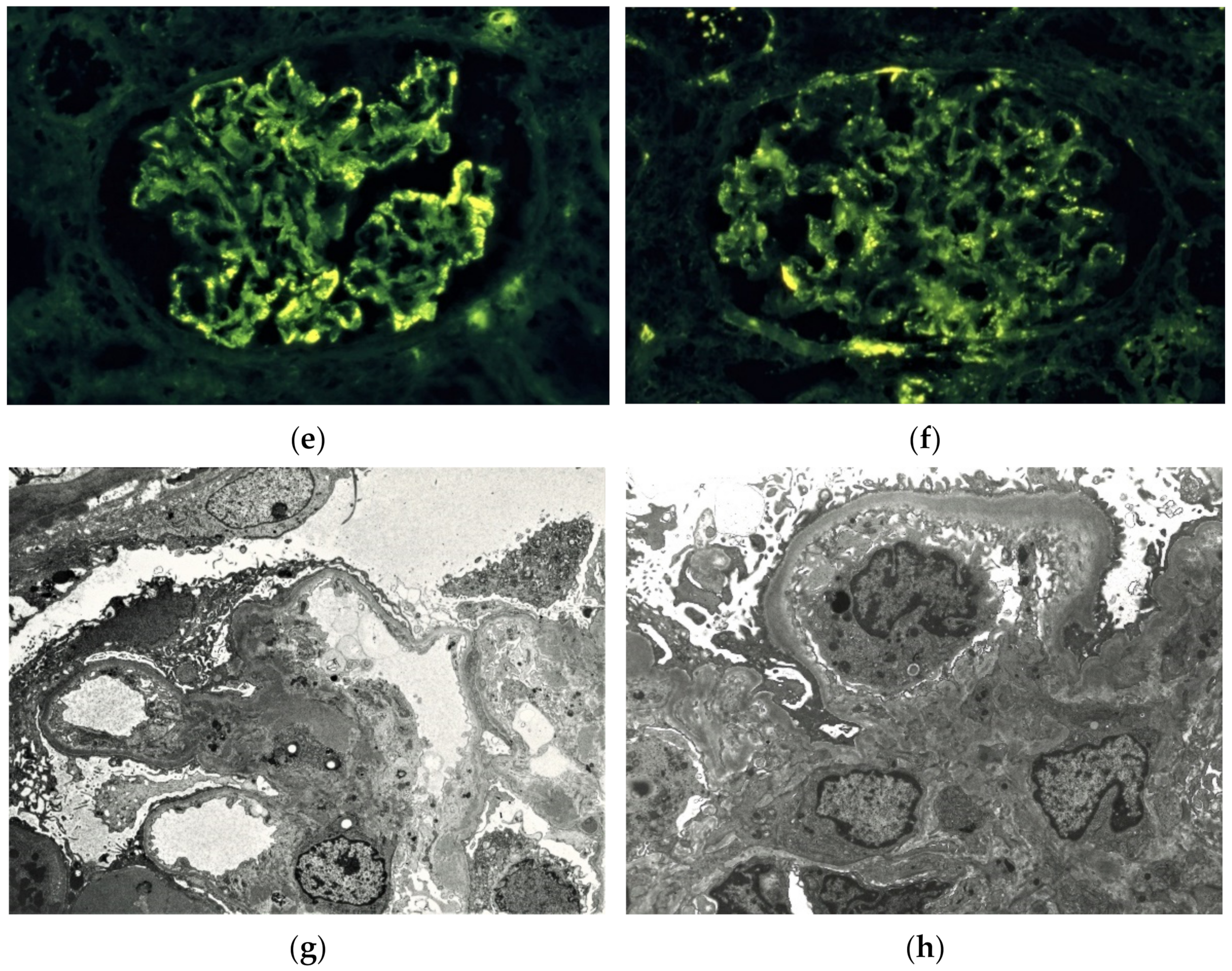
4.2. Immunofluorescence Findings
4.3. Electron Microscopy Findings
5. Pathogenesis
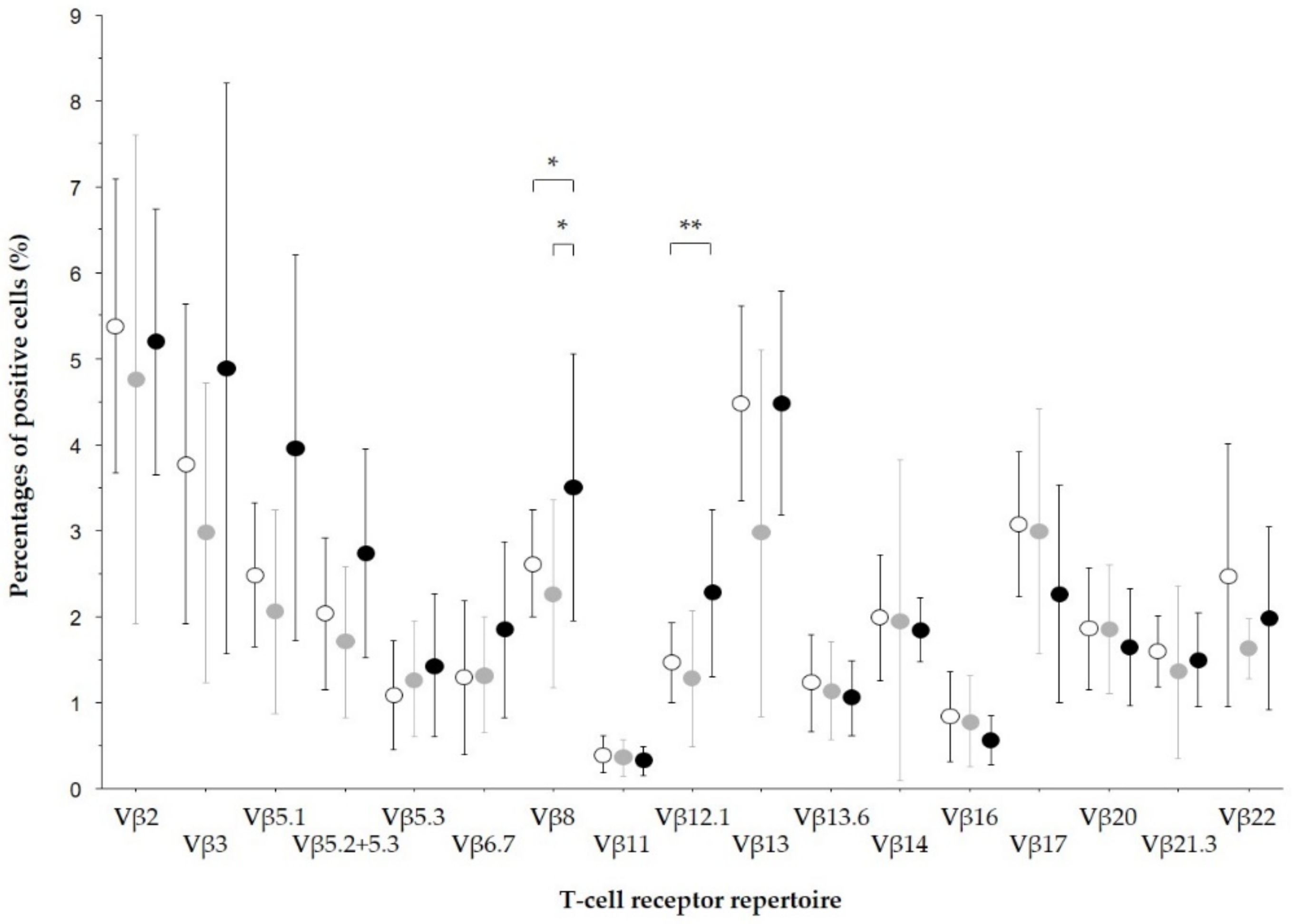
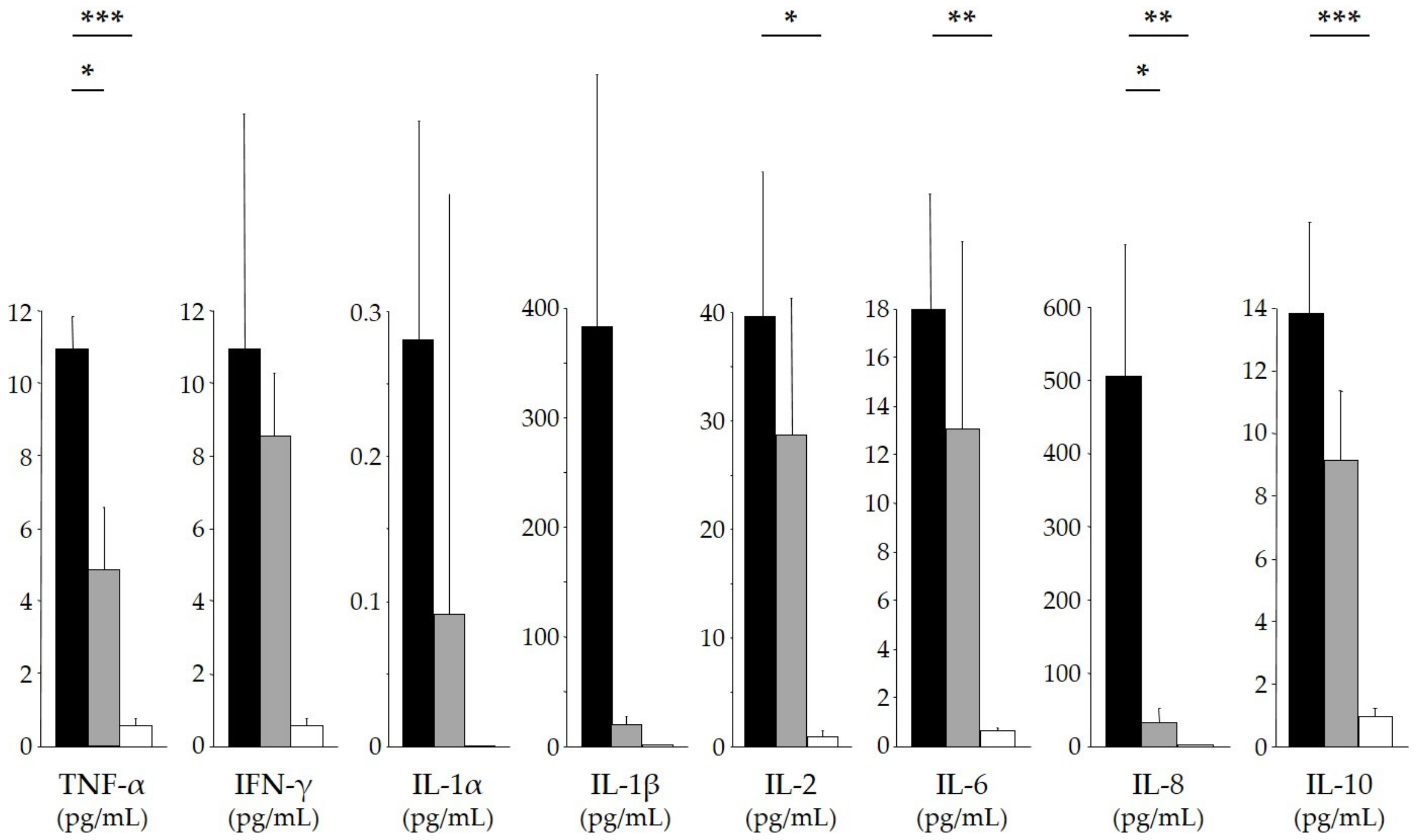
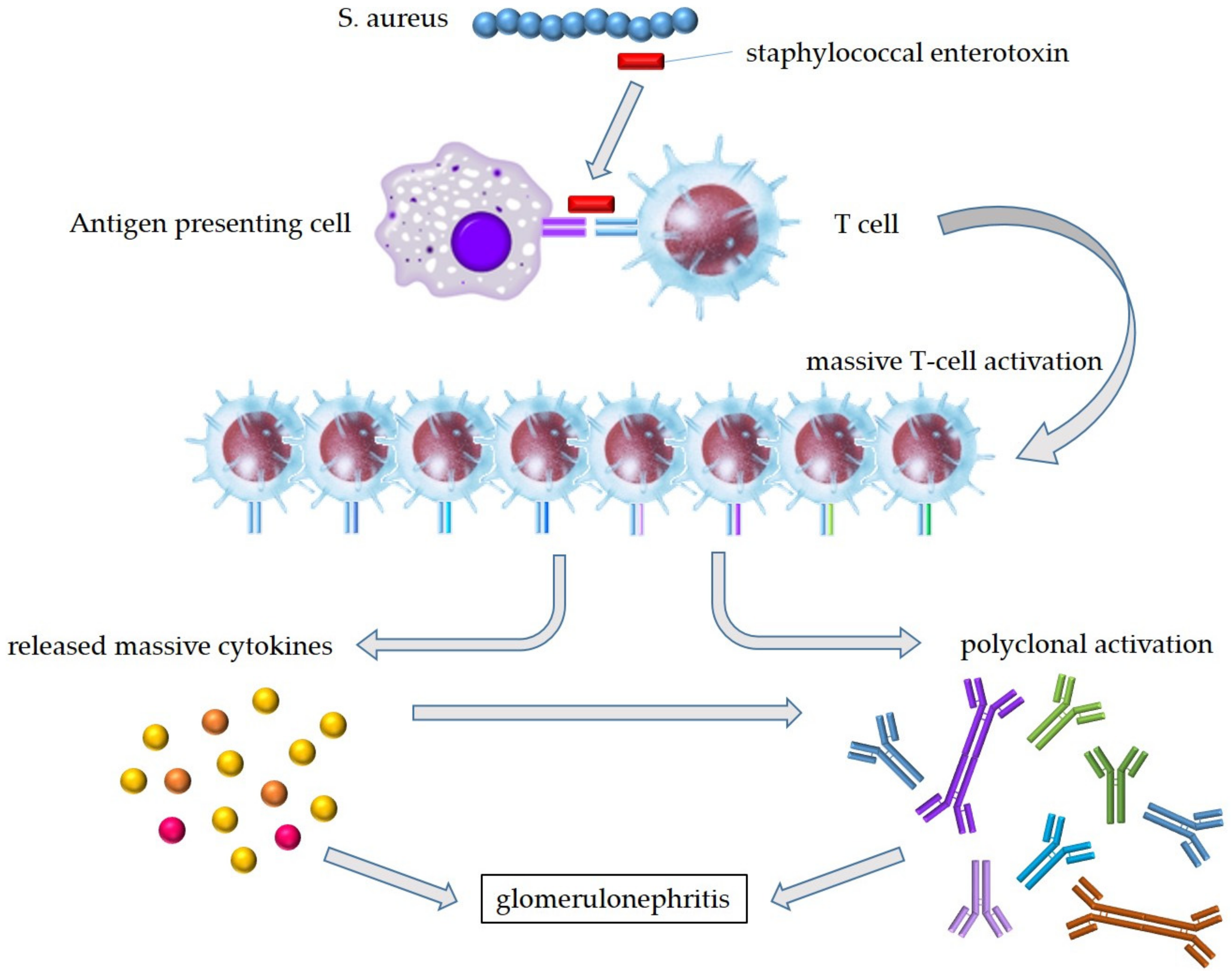
5.1. Bacterial Superantigens
5.2. Neutrophil Extracellular Traps (NETs)
5.3. Dominant IgA Deposition
6. Treatments and Outcomes
6.1. Treatments
6.2. Outcomes
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dobrin, R.S.; Day, N.K.; Quie, P.G.; Moore, H.L.; Vernier, H.L.; Michael, A.F.; Fish, A.J. The role of complement, immunoglobulin and bacterial antigen in coagulase-negative staphylococcal shunt nephritis. Am. J. Med. 1975, 59, 660–673. [Google Scholar] [CrossRef]
- Pertschuk, L.P.; Vuletin, J.C.; Sutton, A.L.; Velazquez, L.A. Demonstration of antigen and immune complex in glomerulonephritis due to Staphylococcus aureus. Am. J. Clin. Pathol. 1976, 66, 1027. [Google Scholar] [CrossRef] [PubMed]
- Koyama, A.; Kobayashi, M.; Yamaguchi, N.; Yamagata, K.; Takano, K.; Nakajima, M.; Irie, F.; Goto, M.; Igarashi, M.; Iitsuka, T.; et al. Glomerulonephritis associated with MRSA infection: A possible role of bacterial superantigen. Kidney Int. 1995, 47, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denton, M.D.; Digumarthy, S.R.; Chua, S.; Colvin, R.B. Case records of the Massachusetts General Hospital. Case 20-2006. An 84-year-old man with staphylococcal bacteremia and renal failure. N. Engl. J. Med. 2006, 354, 2803–2813. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.Y.; Bu, R.; Zhang, Q.; Liang, S.; Wu, J.; Liu, X.Z.S.; Cai, G.Y.; Chen, X.M. Clinical, Pathological, and Prognostic Characteristics of Glomerulonephritis Related to Staphylococcal Infection. Medicine 2016, 95, e3386. [Google Scholar] [CrossRef]
- Satoskar, A.A.; Parikh, S.V.; Nadasdy, T. Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis. Nat. Rev. Nephrol. 2020, 16, 32–50. [Google Scholar] [CrossRef] [PubMed]
- Bu, R.; Li, Q.; Duan, Z.Y.; Wu, J.; Chen, P.; Chen, X.M.; Cai, G.Y. Clinicopathologic features of IgA-dominant infection-associated glomerulonephritis: A pooled analysis of 78 cases. Am. J. Nephrol. 2015, 41, 98–106. [Google Scholar] [CrossRef]
- Nasr, S.H.; D’Agati, V.D. IgA-dominant postinfectious glomerulonephritis: A new twist on an old disease. Nephron Clin. Pract. 2011, 119, c18–c25. [Google Scholar] [CrossRef]
- Hirayama, K.; Kobayashi, M.; Muro, K.; Yoh, K.; Yamagata, K.; Koyama, A. Specific T-cell receptor usage with cytokinemia in Henoch-Schonlein purpura nephritis associated with Staphylococcus aureus infection. J. Intern. Med. 2001, 249, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Yoh, K.; Kobayashi, M.; Yamaguchi, N.; Hirayama, K.; Ishizu, T.; Kikuchi, S.; Iwabuchi, S.; Muro, K.; Nagase, S.; Aoyagi, K.; et al. Cytokines and T-cell responses in superantigen-related glomerulonephritis following methicillin-resistant Staphylococcus aureus infection. Nephrol. Dial. Transplant. 2000, 15, 1170–1174. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Koyama, A. Methicillin-resistant Staphylococcus aureus (MRSA) infection in glomerulonephritis—A novel hazard emerging on the horizon. Nephrol. Dial. Transplant. 1998, 13, 2999–3001. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, K.; Kobayashi, M.; Kondoh, M.; Muro, K.; Iwabuchi, S.; Yoh, K.; Ishizu, T.; Kikuchi, S.; Yamaguchi, N.; Nagase, S.; et al. Henoch-Schonlein purpura nephritis associated with methicillin-resistant Staphylococcus aureus infection. Nephrol. Dial. Transplant. 1998, 13, 2703–2704. [Google Scholar] [CrossRef] [Green Version]
- Yoh, K.; Kobayashi, M.; Hirayama, A.; Hirayama, K.; Yamaguchi, N.; Nagase, S.; Koyama, A. A case of superantigen-related glomerulonephritis after methicillin-resistant Staphylococcus aureus (MRSA) infection. Clin. Nephrol. 1997, 48, 311–316. [Google Scholar]
- Garcia, R.A.; Gaznabi, S.; Musoke, L.; Osnard, M.; Balakumaran, K.; Armitage, K.B.; Al-Kindi, S.G.; Ginwalla, M.; Abu-Omar, Y.; Elamm, C.A. LVAD vasculitis case series: Suggestion of a new ratal LVAD-related phenomenon. JACC Case Rep. 2021, 3, 1013–1017. [Google Scholar] [CrossRef]
- Nogueira, R.F.; Oliveira, N.; Sousa, V.; Alves, R. Staphylococcus-induced glomerulonephritis: Potential role for corticosteroids. BMJ Case Rep. 2021, 14, e237011. [Google Scholar] [CrossRef]
- Sahoo, R.R.; Pradhan, S.; Goel, A.P.; Wakhlu, A. Staphylococcus-associated acute glomerulonephritis in a patient with dermatomyositis. BMJ Case Rep. 2021, 14, e236695. [Google Scholar] [CrossRef]
- Pérez, A.; Torregrosa, I.; D’Marco, L.; Juan, I.; Terradez, L.; Solís, M.Á.; Moncho, F.; Carda-Batalla, C.; Forner, M.J.; Gorriz, J.L. IgA-dominant infection-associated glomerulonephritis following SARS-CoV-2 infection. Viruses 2021, 13, 587. [Google Scholar] [CrossRef]
- Han, W.; Suzuki, T.; Watanabe, S.; Nakata, M.; Ichikawa, D.; Koike, J.; Oda, T.; Suzuki, H.; Suzuki, Y.; Shibagaki, Y. Galactose-deficient IgA1 and nephritis-associated plasmin receptors as markers for IgA-dominant infection-related glomerulonephritis: A case report. Medicine 2021, 100, e24460. [Google Scholar] [CrossRef]
- Hellwege, R.S.; Gawaz, M. Right-sided infective endocarditis in association with a left-to-right shunt complicated by haemoptysis and acute renal failure: A case report. BMC Cardiovasc. Disord. 2020, 20, 494. [Google Scholar] [CrossRef]
- Brunet, A.; Julien, G.; Cros, A.; Beaudoux, O.; Hittinger-Roux, A.; Bani-Sadr, F.; Servettaz, A.; N’Guyen, Y. Vasculitides and glomerulonephritis associated with Staphylocococcus aureus infective endocarditis: Case reports and mini-review of the literature. Ann. Med. 2020, 52, 265–274. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, H.B.; Chu, B.; Zhao, H.Z.; Li, H.; Zhou, H.M.; Wang, T. Disparate effects of methicillin-resistant Staphylococcus aureus infection on renal function in IgA-dominant infection-associated glomerulonephritis and menstrual toxic shock syndrome: A case report and literature review. J. Int. Med. Res. 2020, 48, 300060520933810. [Google Scholar] [CrossRef]
- Nguyen, N.; Chikkalingaiah, K.M.; Walker, P.D.; Wall, B.M. Resolution of IgA and C3 immune deposits in Staphylococcus infection-associated glomerulonephritis in a kidney transplant recipient. Clin. Nephrol. 2020, 94, 97–102. [Google Scholar] [CrossRef]
- Indhumathi, E.; Dhanapriya, J.; Dineshkumar, T.; Sakthirajan, R.; Gopalakrishnan, N. Hansen’s disease with lepra reaction presenting with IgA dominant infection related glomerulonephritis. Indian J. Pathol. Microbiol. 2020, 63, 289–291. [Google Scholar] [CrossRef]
- Shirai, Y.; Miura, K.; Yabuuchi, T.; Nagasawa, T.; Ishizuka, K.; Takahashi, K.; Taneda, S.; Honda, K.; Yamaguchi, Y.; Suzuki, H.; et al. Rapid progression to end-stage renal disease in a child with IgA-dominant infection-related glomerulonephritis associated with parvovirus B19. CEN Case Rep. 2020, 9, 423–430. [Google Scholar] [CrossRef]
- Klimko, A.; Toma, G.A.; Ion, L.; Mehedinti, A.M.; Andreiana, I. A Case Report of Generalized Pustular Psoriasis Associated With IgA Nephropathy. Cureus 2020, 12, e10090. [Google Scholar] [CrossRef]
- Völker, L.A.; Burkert, K.; Scholten, N.; Grundmann, F.; Kurschat, C.; Benzing, T.; Hampl, J.; Becker, J.U.; Müller, R.U. A case report of recurrent membranoproliferative glomerulonephritis after kidney transplantation due to ventriculoatrial shunt infection. BMC Nephrol. 2019, 20, 296. [Google Scholar] [CrossRef] [Green Version]
- Carbayo, J.; Rodriguez-Benitez, P.; Diaz-Crespo, F.; Muñoz de Morales, A.M. IgA dominant postinfectious glomerulonephritis secondary to cutaneous infection by methicillin-resistant Staphylococcus aureus. Nefrologia 2019, 39, 447–449. [Google Scholar] [CrossRef]
- Alqahtani, H.; Alqahtani, F.Y.; Aleanizy, F.S.; Baloch, S.; Tabb, D. IgA Nephropathy Flare-Up Mimicking Staphylococcus Post-Infection Glomerulonephritis in Patient with Staphylococcus Aureus Infection Treated with Cefazolin: A Case Report and Brief Review of the Literature. Am. J. Case Rep. 2019, 20, 508–510. [Google Scholar] [CrossRef]
- Parente, Y.D.M.; Castro, A.L.; Araújo, F.B.; Teixeira, A.C.; Lima, Í.C.; Daher, E.F. Acute renal failure by rapidly progressive glomerulonephritis with IgA deposition in a patient concomitantly diagnosed with multibacillary Hansen’s disease: A case report. J. Bras. Nefrol. 2019, 41, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Molina-Andújar, A.; Montagud-Marrahí, E.; Cucchiari, D.; Ventura-Aguiar, P.; De Sousa-Amorim, E.; Revuelta, I.; Cofan, F.; Solé, M.; García-Herrera, A.; Diekmann, F.; et al. Postinfectious acute glomerulonephritis in renal transplantation: An emergent aetiology of renal allograft loss. Case Rep. Transplant. 2019, 2019, 7438254. [Google Scholar] [CrossRef] [Green Version]
- Orozco Guillén, A.O.; Velazquez Silva, R.I.; Moguel González, B.; Guell, Y.A.; Garciadiego Fossas, P.; Custodio Gómez, I.G.; Miranda Araujo, O.; Soto Abraham, V.; Piccoli, G.B.; Madero, M. Acute IgA-dominant glomerulonephritis associated with syphilis infection in a pregnant teenager: A new disease association. J. Clin. Med. 2019, 8, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sá, D.C.; Rodrigues, L.; Santos, L.; Romãozinho, C.; Macário, F.; Marinho, C.; Pratas, J.; Alves, R.; Figueiredo, A. Staphylococcus Infection–Associated Glomerulonephritis in a Kidney Transplant Patient: Case Report. Transplant. Proc. 2018, 50, 853–856. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, Y.; Maeda, T.; Gocho, Y.; Ogawa, Y.; Takizawa, H. IgA-dominant infection-related glomerulonephritis. Nefrologia 2018, 38, 669–670. [Google Scholar] [CrossRef] [PubMed]
- Basic-Jukic, N.; Coric, M.; Kastelan, Z. IgA-dominant extracapillary proliferative glomerulonephritis following Escherichia coli sepsis in a renal transplant recipient. Transpl. Infect. Dis. 2018, 20, e12927. [Google Scholar] [CrossRef]
- Mahmood, T.; Puckrin, R.; Sugar, L.; Naimark, D. Staphylococcus-Associated Glomerulonephritis Mimicking Henoch-Schonlein Purpura and Cryoglobulinemic Vasculitis in a Patient With an Epidural Abscess: A Case Report and Brief Review of the Literature. Can. J. Kidney Health Dis. 2018, 5, 2054358118776325. [Google Scholar] [CrossRef]
- Liang, J.H.; Fang, Y.W.; Yang, A.H.; Tsai, M.H. Devastating renal outcome caused by skin infection with methicillin-resistant Staphylococcus aureus: A case report. Medicine 2016, 95, e4023. [Google Scholar] [CrossRef]
- Okada, M.; Sato, M.; Ogura, M.; Kamei, K.; Matsuoka, K.; Ito, S. Central venous catheter infection-related glomerulonephritis under long-term parenteral nutrition: A report of two cases. BMC Res. Notes 2016, 9, 196. [Google Scholar] [CrossRef] [Green Version]
- Srinivasaraghavan, R.; Krishnamurthy, S.; Dubey, A.K.; Parameswaran, S.; Biswal, N.; Srinivas, B.H. IgA Dominant Post-infectious Glomerulonephritis in a 12-year-old Child. Indian J. Pediatr. 2016, 83, 470–472. [Google Scholar] [CrossRef]
- Nayer, A.; Davda, G.; Pai, R.; Ortega, L.M. IgA-dominant post-infectious glomerulonephritis; making another case in support of renal biopsy in type 2 diabetic nephropathy. J. Ren. Inj. Prev. 2016, 5, 45–47. [Google Scholar] [CrossRef] [Green Version]
- Caetano, J.; Pereira, F.; Oliveira, S.; Delgado Alves, J. IgA-dominant postinfectious glomerulonephritis induced by methicillin-sensitive Staphylococcus aureus. BMJ Case Rep. 2015, 2015, bcr2014208513. [Google Scholar] [CrossRef]
- Hayashi, S.; Mori, A.; Kawamura, T.; Ito, S.; Shibuya, T.; Fushimi, N. Glomerulonephritis Caused by CV Catheter-related Blood Stream Infection. Intern. Med. 2015, 54, 2219–2223. [Google Scholar] [CrossRef] [Green Version]
- Rus, R.R.; Toplak, N.; Vizjak, A.; Mraz, J.; Ferluga, D. IgA-dominant acute poststreptococcal glomerulonephritis with concomitant rheumatic fever successfully treated with steroids: A case report. Croat. Med. J. 2015, 56, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Saad, M.; Daoud, M.; Nasr, P.; Syed, R.; El-Sayegh, S. IgA-dominant post-infectious glomerulonephritis presenting as a fatal pulmonary-renal syndrome. Int. J. Nephrol. Renovasc. Dis. 2015, 8, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, H.; Aoyagi, M.; Nagahama, K.; Yamamura, C.; Arai, Y.; Hirasawa, S.; Aki, S.; Inaba, N.; Tanaka, H.; Tamura, T. IgA-dominant postinfectious glomerulonephritis associated with Escherichia coli infection caused by cholangitis. Intern. Med. 2014, 53, 2619–2624. [Google Scholar] [CrossRef] [Green Version]
- Mandai, S.; Aoyagi, M.; Nagahama, K.; Arai, Y.; Hirasawa, S.; Aki, S.; Inaba, N.; Tanaka, H.; Tsuura, Y.; Tamura, T.; et al. Post-Staphylococcal infection Henoch–Schonlein purpura nephritis: A case report and review of the literature. Ren. Fail. 2013, 35, 869–874. [Google Scholar] [CrossRef]
- Erqou, S.; Kamat, N.; Moschos, S.; Im, A.; Bastacky, S. A 61 year diabetic man with methicillin-sensitive Staphylococcus aureus septic arthritis and acute renal failure: A case of IgA-dominant postinfectious glomerulonephritis. Nephrology 2012, 17, 780–781. [Google Scholar] [CrossRef]
- Kimata, T.; Tsuji, S.; Yoshimura, K.; Tsukaguchi, H.; Kaneko, K. Methicillin-resistant Staphylococcus aureus-related glomerulonephritis in a child. Pediatr. Nephrol. 2012, 27, 2149–2152. [Google Scholar] [CrossRef]
- Chen, Y.-R.; Wen, Y.-K. Favorable Outcome of Crescentic IgA Nephropathy Associated with Methicillin-Resistant Staphylococcus aureus Infection. Ren. Fail. 2011, 33, 96–100. [Google Scholar] [CrossRef] [Green Version]
- Wehbe, E.; Salem, C.; Simon, J.F.; Navaneethan, S.D.; Pohl, M. IgA-dominant Staphylococcus infection-associated glomerulonephritis: Case reports and review of the literature. NDT Plus 2011, 4, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Kapadia, A.S.; Panda, M.; Fogo, A.B. Postinfectious glomerulonephritis: Is there a role for steroids? Indian J. Nephrol. 2011, 21, 116–119. [Google Scholar] [CrossRef]
- Upadhaya, B.K.; Sharma, A.; Khaira, A.; Dinda, A.K.; Agarwal, S.K.; Tiwari, S.C. Transient IgA nephropathy with acute kidney injury in a patient with dengue fever. Saudi J. Kidney Dis. Transplant. 2010, 21, 521–525. [Google Scholar]
- Riley, A.M.; Wall, B.M.; Cooke, C.R. Favorable Outcome After Aggressive Treatment of Infection in a Diabetic Patient With MRSA-Related IgA Nephropathy. Am. J. Med. Sci. 2009, 337, 221–223. [Google Scholar] [CrossRef]
- Okuyama, S.; Wakui, H.; Maki, N.; Kuroki, J.; Nishinari, T.; Asakura, K.; Komatsuda, A.; Sawada, K. Successful treatment of post-MRSA infection glomerulonephritis with steroid therapy. Clin. Nephrol. 2008, 70, 344–347. [Google Scholar] [CrossRef]
- Kusaba, T.; Nakayama, M.; Kato, H.; Uchiyama, H.; Sato, K.; Kajita, Y. Crescentic glomerulonephritis associated with totally implantable central venous catheter-related Staphylococcus epidermidis infection. Clin. Nephrol. 2008, 70, 54–58. [Google Scholar] [CrossRef]
- Ho, C.-I.; Wen, Y.-K.; Chen, M.-L. Glomerulonephritis with Acute Renal Failure Related to Osteomyelitis. J. Chin. Med. Assoc. 2008, 71, 315–317. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, M.; Kuhlmann, U.; Alscher, D.M. Pacemaker infection with propionibacterium and a nephritic sediment. Clin. Nephrol. 2008, 69, 127–129. [Google Scholar] [CrossRef]
- Hashimoto, M.; Nogaki, F.; Oida, E.; Tanaka, M.; Ito-Ihara, T.; Nomura, K.; Liu, N.; Muso, E.; Fukatsu, A.; Kita, T.; et al. Glomerulonephritis induced by methicillin-resistant Staphylococcus aureus infection that progressed during puerperal period. Clin. Exp. Nephrol. 2007, 11, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, C.; Satoh, N.; Sugawara, S.; Kuriyama, C.; Kikuchi, A.; Ohta, M. Community-Acquired Staphylococcus aureus Pneumonia Accompanied by Rapidly Progressive Glomerulonephritis and Hemophagocytic Syndrome. Intern. Med. 2007, 46, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, J.A.; Cook, W.J. IgA Deposits and Acute Glomerulonephritis in a Patient With Staphylococcal Infection. Am. J. Kidney Dis. 2006, 48, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, T.; Nakase, H.; Iizuka, H. Henoch-Schonlein purpura after postoperative Staphylococcus aureus infection with hepatic IgA nephropathy. J. Nephrol. 2006, 19, 687–690. [Google Scholar] [PubMed]
- Ohara, S.; Kawasaki, Y.; Takano, K.; Isome, M.; Nozawa, R.; Suzuki, H.; Hosoya, M. Glomerulonephritis associated with chronic infection from long-term central venous catheterization. Pediatr. Nephrol. 2006, 21, 427–429. [Google Scholar] [CrossRef]
- Iyoda, M.; Hato, T.; Matsumoto, K.; Ito, J.; Ajiro, Y.; Kuroki, A.; Shibata, T.; Kitazawa, K.; Sugisaki, T. Rapidly progressive glomerulonephritis in a patient with Chlamydia pneumoniae infection: A possibility of superantigenic mechanism of its pathogenesis. Clin. Nephrol. 2006, 65, 48–52. [Google Scholar] [CrossRef]
- Manzoor, K.; Khan, S.; Ahmed, E.; Akhter, F.; Mubarak, M.; Naqvi, S.A.A.; Rizvi, A.H. Crescentic glomerulonephritis associated with bacterial endocarditis—Antibiotics alone may be sufficient. A case report. J. Pak. Med. Assoc. 2005, 55, 352–354. [Google Scholar]
- Cheema, S.R.; Arif, F.; Charney, D.; Meisels, I.S. IgA-dominant glomerulonephritis associated with hepatitis A. Clin. Nephrol. 2004, 62, 138–143. [Google Scholar] [CrossRef]
- Handa, T.; Ono, T.; Watanabe, H.; Takeda, T.; Muso, E.; Kita, T. Glomerulonephritis induced by methicillin-sensitive Staphylococcus aureus infection. Clin. Exp. Nephrol. 2003, 7, 247–249. [Google Scholar] [CrossRef]
- Arrizabalaga, P.; Saurina, A.; Solé, M.; Bladé, J. Henoch-Schonlein IgA glomerulonephritis complicating myeloma kidneys: Case report. Ann. Hematol. 2003, 82, 526–528. [Google Scholar] [CrossRef]
- Pola, E.; Logroscino, G.; De Santis, V.; Canducci, F.; Delcogliano, A.; Gasbarrini, A. Onset of Berger disease after Staphylococcus aureus infection: Septic arthritis after anterior cruciate ligament reconstruction. Arthroscopy 2003, 19, E29. [Google Scholar] [CrossRef]
- Peel, R.; Sellars, L.; Long, E.D.; Bhandari, S. A man with backache and renal failure. Am. J. Kidney Dis. 2003, 41, e1.1–e1.3. [Google Scholar] [CrossRef]
- Kubota, M.; Sakata, Y.; Saeki, N.; Yamaura, A.; Ogawa, M. A case of shunt nephritis diagnosed 17 years after ventriculoatrial shunt implantation. Clin. Neurol. Neurosurg. 2001, 103, 245–246. [Google Scholar] [CrossRef]
- Balogun, R.A.; Palmisano, J.; Kaplan, A.A.; Khurshid, H.; Yamase, H.; Adams, N.D. Shunt nephritis from Propionibacterium acnes in a solitary kidney. Am. J. Kidney Dis. 2001, 38, e18.1–e18.7. [Google Scholar] [CrossRef]
- Yamashita, Y.; Tanase, T.; Terada, Y.; Tamura, H.; Akiba, T.; Inoue, H.; Ida, T.; Sasaki, S.; Marumo, F.; Nakamoto, Y. Glomerulonephritis after methicillin-resistant Staphylococcus aureus infection resulting in end-stage renal failure. Intern. Med. 2001, 40, 424–427. [Google Scholar] [CrossRef] [Green Version]
- Barnadas, M.A.; Gelpí, C.; Rocamora, V.; Baró, E.; Ballarín, J.; Nadal, C.; Bielsa, A.; Aróstegui, J.; Alomar, A. Bullous pemphigoid associated with acute glomerulonephritis. Br. J. Dermatol. 1998, 138, 867–871. [Google Scholar] [CrossRef]
- Griffin, M.D.; Björnsson, J.; Erickson, S.B. Diffuse proliferative glomerulonephritis and acute renal failure associated with acute staphylococcal osteomyelitis. J. Am. Soc. Nephrol. 1997, 8, 1633–1639. [Google Scholar] [CrossRef]
- Kitazawa, M.; Tomosugi, N.; Ishii, T.; Hotta, F.; Nishizawa, M.; Itou, T.; Nakano, S.; Kigoshi, T.; Ishikawa, I.; Uchida, K. Rapidly progressive glomerulonephritis concomitant with diabetic nephropathy. Intern. Med. 1997, 36, 906–911. [Google Scholar] [CrossRef] [Green Version]
- Pulik, M.; Lionnet, F.; Genet, P.; Petitdidier, C.; Vacher, B. Immune-complex glomerulonephritis associated with Staphylococcus aureus infection of a totally implantable venous device. Support Care Cancer 1995, 3, 324–326. [Google Scholar] [CrossRef]
- Ramineni, S.; Bandi, V.K. Clinicopathological profile and outcomes of infection-related glomerulonephritis in adults. Clin. Nephrol. 2021, 95, 93–98. [Google Scholar] [CrossRef]
- Ai, S.; Ma, G.; Liu, J.; Bai, X.; Hu, R.; Fan, X.; Miao, Q.; Qin, Y.; Li, X. Infective endocarditis-associated purpura and glomerulonephritis mimicking IgA vasculitis: A diagnostic pitfall. Am. J. Med. 2021, 134, 1539–1545. [Google Scholar] [CrossRef]
- Grosser, D.S.; Persad, P.; Talento, R.V.; Shoemaker, L.R.; Hunley, T.E.; Hidalgo, G.; Subtirelu, M.M.; Coventry, S.; Baliga, R.; Fogo, A.B. IgA-dominant infection-associated glomerulonephritis in the pediatric population. Pediatr. Nephrol. 2021, 37, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Chen, B.; Zhou, Y.; Liang, Y.; Qiu, W.; Lv, Y.; Ding, X.; Zhang, J.; Chen, C. Clinicopathological and prognostic study of IgA-dominant postinfectious glomerulonephritis. BMC Nephrol. 2021, 22, 248. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhou, W.; Liu, S.; Zhang, L.; Ni, Z.; Hao, C. KM55 Monoclonal antibody staining in IgA-dominant infection-related glomerulonephritis. Nephron 2021, 145, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Miquelestorena-Standley, E.; Jaulerry, C.; Machet, M.-C.; Rabot, N.; Barbet, C.; Hummel, A.; Karras, A.; Garrouste, C.; Crepin, T.; Ducloux, D.; et al. Clinicopathologic features of infection-related glomerulonephritis with IgA deposits: A French Nationwide study. Diagn. Pathol. 2020, 15, 62. [Google Scholar] [CrossRef]
- Kitamura, M.; Obata, Y.; Ota, Y.; Muta, K.; Yamashita, H.; Harada, T.; Mukae, H.; Nishino, T. Significance of subepithelial deposits in patients diagnosed with IgA nephropathy. PLoS ONE 2019, 14, e0211812. [Google Scholar] [CrossRef] [Green Version]
- Sakthirajan, R.; Dhanapriya, J.; Nagarajan, M.; Dineshkumar, T.; Balasubramaniyan, T.; Gopalakrishnan, N. Crescentic infection related glomerulonephritis in adult and its outcome. Saudi J. Kidney Dis. Transplant. 2018, 29, 623–629. [Google Scholar]
- Handa, T.; Kakita, H.; Tateishi, Y.; Endo, T.; Suzuki, H.; Katayama, T.; Tsukamoto, T.; Muso, E. The features in IgA-dominant infection-related glomerulonephritis distinct from IgA nephropathy: A single-center study. Clin. Exp. Nephrol. 2018, 22, 1116–1127. [Google Scholar] [CrossRef]
- Khalighi, M.A.; Al-Rabadi, L.; Chalasani, M.; Smith, M.; Kakani, S.; Revelo, M.P.; Meehan, S.M. Staphylococcal infection-related glomerulonephritis with cryoglobulinemic features. Kidney Int. Rep. 2018, 3, 1128–1134. [Google Scholar] [CrossRef]
- Hemminger, J.; Arole, V.; Ayoub, I.; Brodsky, S.V.; Nadasdy, T.; Satoskar, A.A. Acute glomerulonephritis with large confluent IgA-dominant deposits associated with liver cirrhosis. PLoS ONE 2018, 13, e0193274. [Google Scholar] [CrossRef]
- Ramanathan, G.; Abeyaratne, A.; Sundaram, M.; Fernandes, D.K.; Pawar, B.; Perry, G.J.; Sajiv, C.; Majoni, S.W. Analysis of clinical presentation, pathological spectra, treatment and outcomes of biopsy-proven acute postinfectious glomerulonephritis in adult indigenous people of the Northern Territory of Australia. Nephrology 2017, 22, 403–411. [Google Scholar] [CrossRef]
- Satoskar, A.A.; Suleiman, S.; Ayoub, I.; Hemminger, J.; Parikh, S.; Brodsky, S.V.; Bott, C.; Calomeni, E.; Nadasdy, G.M.; Rovin, B.; et al. Staphylococcus infection-associated GN–spectrum of IgA staining and prevalence of ANCA in a single-center cohort. Clin. J. Am. Soc. Nephrol. 2017, 12, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Dhanapriya, J.; Balasubramaniyan, T.; Maharajan, S.P.; Dineshkumar, T.; Sakthirajan, R.; Gopalakrishnan, N.; Nagarajan, M. IgA-dominant infection-related glomerulonephritis in India: A single-center experience. Indian J. Nephrol. 2017, 27, 435–439. [Google Scholar] [CrossRef]
- Boils, C.L.; Nasr, S.H.; Walker, P.D.; Couser, W.G.; Larsen, C.P. Update on endocarditis-associated glomerulonephritis. Kidney Int. 2015, 87, 1241–1249. [Google Scholar] [CrossRef] [Green Version]
- Murakami, C.A.; Attia, D.; Carter-Monroe, N.; Lucas, G.M.; Estrella, M.M.; Fine, D.M.; Atta, M.G. The Clinical Characteristics and Pathological Patterns of Postinfectious Glomerulonephritis in HIV-Infected Patients. PLoS ONE 2014, 9, e108398. [Google Scholar] [CrossRef]
- Hamouda, M.; Mrabet, I.; Dhia, N.B.; Aloui, S.; Letaif, A.; Frih, M.A.; Skhiri, H.; Elmay, M. Acute post-infectious glomerulonephritis in adults: A single center report. Saudi J. Kidney Dis. Transplant. 2014, 25, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Cossey, L.N.; Messias, N.; Messias, E.; Walker, P.D.; Silva, F.G. Defining the spectrum of immunoglobulin A–dominant/codominant glomerular deposition in diabetic nephropathy. Hum. Pathol. 2014, 45, 2294–2301. [Google Scholar] [CrossRef] [PubMed]
- Satoskar, A.A.; Molenda, M.; Scipio, P.; Shim, R.; Zirwas, M.; Variath, R.S.; Brodsky, S.V.; Nadasdy, G.M.; Hebert, L.; Rovin, B.; et al. Henoch-Schonlein purpura-like presentation in IgA-dominant Staphylococcus infection–associated glomerulonephritis—A diagnostic pitfall. Clin. Nephrol. 2013, 79, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.Y.; Kim, G.H.; Park, M.H. Clinicopathologic features of IgA-dominant postinfectious glomerulonephritis. Korean J. Pathol. 2012, 46, 105–114. [Google Scholar] [CrossRef]
- Worawichawong, S.; Girard, L.; Trpkov, K.; Gough, J.C.; Gregson, D.B.; Benediktsson, H. Immunoglobulin A–dominant postinfectious glomerulonephritis: Frequent occurrence in nondiabetic patients with Staphylococcus aureus infection. Hum. Pathol. 2011, 42, 279–284. [Google Scholar] [CrossRef]
- Wen, Y.K.; Chen, M.L. IgA-dominant postinfectious glomerulonephritis: Not peculiar to staphylococcal infection and diabetic patients. Ren. Fail. 2011, 33, 480–485. [Google Scholar] [CrossRef]
- Nasr, S.H.; Fidler, M.E.; Valeri, A.M.; Cornell, L.D.; Sethi, S.; Zoller, A.; Stokes, M.B.; Markowitz, G.S.; D’Agati, V.D. Postinfectious Glomerulonephritis in the Elderly. J. Am. Soc. Nephrol. 2011, 22, 187–195. [Google Scholar] [CrossRef]
- Wen, Y.K. Clinicopathological study of infection-associated glomerulonephritis in adults. Int. Urol. Nephrol. 2010, 42, 477–485. [Google Scholar] [CrossRef]
- Wen, Y.K.; Chen, M.L. The significance of atypical morphology in the changes of spectrum of postinfectious glomerulonephritis. Clin. Nephrol. 2010, 73, 173–179. [Google Scholar] [CrossRef]
- Wen, Y.K.; Chen, M.L. Discrimination between postinfectious IgA-dominant glomerulonephritis and idiopathic IgA nephropathy. Ren. Fail. 2010, 32, 572–577. [Google Scholar] [CrossRef]
- Hsieh, Y.P.; Wen, Y.K.; Chen, M.L. Comparison of Typical Endocapillary and Atypical Mesangial Proliferation in Postinfectious Glomerulonephritis. Ren. Fail. 2010, 32, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.K. The Spectrum of Adult Postinfectious Glomerulonephritis in the New Millennium. Ren. Fail. 2009, 31, 676–682. [Google Scholar] [CrossRef]
- Haas, M.; Racusen, L.C.; Bagnasco, S.M. IgA-dominant postinfectious glomerulonephritis: A report of 13 cases with common ultrastructural features. Hum. Pathol. 2008, 39, 1309–1316. [Google Scholar] [CrossRef]
- Zeledon, J.I.; McKelvey, R.L.; Servilla, K.S.; Hofinger, D.; Konstantinov, K.N.; Kellie, S.; Sun, Y.; Massie, L.W.; Hartshorne, M.F.; Tzamaloukas, A.H. Glomerulonephritis causing acute renal failure during the course of bacterial infections. Histological varieties, potential pathogenetic pathways and treatment. Int. Urol. Nephrol. 2008, 40, 461–470. [Google Scholar] [CrossRef]
- Nasr, S.H.; Markowitz, G.S.; Stokes, M.B.; Said, S.M.; Valeri, A.M.; D’Agati, V.D. Acute postinfectious glomerulonephritis in the modern era: Experience with 86 adults and review of the literature. Medicine 2008, 87, 21–32. [Google Scholar] [CrossRef]
- Satoskar, A.A.; Nadasdy, G.; Plaza, J.A.; Sedmak, D.; Shidham, G.; Hebert, L.; Nadasdy, T. Staphylococcus Infection-Associated Glomerulonephritis Mimicking IgA Nephropathy. Clin. J. Am. Soc. Nephrol. 2006, 1, 1179–1186. [Google Scholar] [CrossRef] [Green Version]
- Nasr, S.H.; Markowitz, G.S.; Whelan, J.D.; Albanese, J.J.; Rosen, R.M.; Fein, D.A.; Kim, S.S.; D’Agati, V.D. IgA-dominant acute poststaphylococcal glomerulonephritis complicating diabetic nephropathy. Hum. Pathol. 2003, 34, 1235–1241. [Google Scholar] [CrossRef]
- Nakamura, T.; Ushiyama, C.; Suzuki, Y.; Osada, S.; Inoue, T.; Shoji, H.; Hara, M.; Shimada, N.; Koide, H. Hemoperfusion with polymyxin B-immobilized fiber in septic patients with methicillin-resistant Staphylococcus aureus-associated glomerulonephritis. Nephron Clin. Pract. 2003, 94, c33–c39. [Google Scholar] [CrossRef]
- Nagaba, Y.; Hiki, Y.; Aoyama, T.; Sano, T.; Matsuo, T.; Shimizu, T.; Tateno, S.; Sakamoto, H.; Kamata, K.; Shigematsu, H.; et al. Effective antibiotic treatment of methicillin-resistant Staphylococcus aureus-associated glomerulonephritis. Nephron 2002, 92, 297–303. [Google Scholar] [CrossRef]
- Majumdar, A.; Chowdhary, S.; Ferreira, M.A.S.; Hammond, L.A.; Howie, A.J.; Lipkin, G.W.; Littler, W.A. Renal pathological findings in infective endocarditis. Nephrol. Dial. Transplant. 2000, 15, 1782–1787. [Google Scholar] [CrossRef] [Green Version]
- Deacy, A.M.; Gan, S.K.E.; Derrick, J.P. Superantigen Recognition and Interactions: Functions, Mechanisms and Applications. Front. Immunol. 2021, 12, 731845. [Google Scholar] [CrossRef]
- Murphy, K.; Weaver, C. T-Cell Receptor Gene Rearrangement. In Janeway’s Immunobiology, 9th ed.; Murphy, K., Weaver, C., Eds.; Garland Science: New York, NY, USA, 2017; pp. 187–191. [Google Scholar]
- Tuffs, S.W.; Haeryfar, S.M.M.; McCormick, J.K. Manipulation of innate and adaptive immunity by Staphylococcal superantigens. Pathogens 2018, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Sfriso, P.; Ghirardello, A.; Botsios, C.; Tonon, M.; Zen, M.; Basso, N.; Bassetto, F.; Doria, A. Infections and autoimmunity: The multifaceted relationship. J. Leukoc. Biol. 2020, 87, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.S.; Park, J.Y.; Terman, D.S.; Bohach, G.A. A quantitative real time PCR method to analyze T cell receptor Vbeta subgroup expansion by staphylococcal superantigens. J. Transl. Med. 2010, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdurrahman, G.; Schmiedeke, F.; Bachert, C.; Broker, B.M.; Holtfreter, S. Allergy—A new role for T cell superantigens of Staphylococcus aureus? Toxins 2020, 12, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamdy, A.; Leonardi, A. Superantigens and SARS-CoV-2. Pathogens 2022, 11, 390. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Z.; Zhu, Y.; Dong, B.; Cai, Z.; Liang, Q.; Wang, K. T Cell Receptor Immune Repertoires Are Promptly Reconstituted After Methicillin-Resistant Staphylococcus aureus Infection. Front. Microbiol. 2019, 10, 2012. [Google Scholar] [CrossRef] [Green Version]
- DeLorenze, G.N.; Nelson, C.L.; Scott, W.K.; Allen, A.S.; Ray, G.T.; Tsai, A.L.; Quesenberry, C.P., Jr.; Fowler, V.G., Jr. Polymorphisms in HLA class II genes are associated with susceptibility to Staphylococcus aureus infection in a white population. J. Infect. Dis. 2016, 213, 816–823. [Google Scholar] [CrossRef] [Green Version]
- Dan, J.M.; Havenar-Daughton, C.; Kendric, K.; Al-Kolla, R.; Kaushik, K.; Rosales, S.L.; Anderson, E.L.; LaRock, C.N.; Vija-yanand, P.; Seumois, G.; et al. Recurrent group A Streptococcus tonsillitis is an immunosusceptibility disease involving antibody deficiency and aberrant TFH cells. Sci. Transl. Med. 2019, 11, eaau3776. [Google Scholar] [CrossRef] [Green Version]
- Csernok, E.; Lamprecht, P.; Gross, W.L. Clinical and immunological features of drug-induced and infection-induced proteinase 3-antineutrophil cytoplasmic antibodies and myeloperoxidase-antineutrophil cytoplasmic antibodies and vasculitis. Curr. Opin. Rheumatol. 2010, 22, 43–48. [Google Scholar] [CrossRef]
- Schnabel, A.; Renz, H.; Petermann, R.; Csernok, E.; Gross, W.L. T Cell Receptor Vβ Repertoire in Bronchoalveolar Lavage in Wegener’s Granulomatosis and Sarcoidosis. Int. Arch. Allergy Immunol. 1999, 119, 223–230. [Google Scholar] [CrossRef]
- Hirayama, K.; Ishizu, T.; Shimohata, H.; Miyamoto, Y.; Kakita, T.; Nagai, M.; Ogawa, Y.; Fujita, S.; Hirayama, A.; Yamagata, K.; et al. Analysis of T-cell receptor usage in myeloperoxidase-antineutrophil cytoplasmic antibody-associated renal vasculitis. Clin. Exp. Nephrol. 2010, 14, 36–42. [Google Scholar] [CrossRef]
- Kessenbrock, K.; Krumbholz, M.; Schönermarck, U.; Back, W.; Gross, W.L.; Werb, Z.; Gröne, H.J.; Brinkmann, V.; Jenne, D.E. Netting neutrophils in autoimmune small-vessel vasculitis. Nat. Med. 2009, 15, 623–625. [Google Scholar] [CrossRef]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef]
- Schreiber, A.; Rousselle, A.; Becker, J.U.; von Mässenhausen, A.; Linkermann, A.; Kettritz, R. Necroptosis controls NET generation and mediates complement activation, endothelial damage, and autoimmune vasculitis. Proc. Natl. Acad. Sci. USA 2017, 114, E9618–E9625. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.U.S.; O’Sullivan, K.M. The Expanding Role of Extracellular Traps in Inflammation and Autoimmunity: The New Players in Casting Dark Webs. Int. J. Mol. Sci. 2022, 23, 3793. [Google Scholar] [CrossRef]
- Brodsky, S.V.; Nadasdy, T.; Cassol, C.; Satoskar, A. IgA Staining Patterns Differentiate Between IgA Nephropathy and IgA-Dominant Infection-Associated Glomerulonephritis. Kidney Int. Rep. 2020, 5, 909–911. [Google Scholar] [CrossRef]
- Satoskar, A.A.; Shapiro, J.P.; Jones, M.; Bott, C.; Parikh, S.V.; Brodsky, S.V.; Yu, L.; Nagaraja, H.N.; Wilkey, D.W.; Merchant, M.L.; et al. Differentiating Staphylococcus infection-associated glomerulonephritis and primary IgA nephropathy: A mass spectrometry-based exploratory study. Sci. Rep. 2020, 10, 17179. [Google Scholar] [CrossRef]
- Suzuki, H.; Yasutake, J.; Makita, Y.; Tanbo, Y.; Yamasaki, K.; Sofue, T.; Kano, T.; Suzuki, Y. IgA nephropathy and IgA vasculitis with nephritis have a shared feature involving galactose-deficient IgA1-oriented pathogenesis. Kidney Int. 2018, 93, 700–705. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IgA-IRGN n = 336 | SAGN n = 218 | |||
|---|---|---|---|---|
| Incidence: | ||||
| In patients with biopsy | 0.40% | 117/29,562 | 0.45% | 96/21,257 |
| In patients with IgA deposition | 4.31% | 40/927 | 1.66% | 12/722 |
| In patients with IRGN | 10.18% | 34/334 | 11.90% | 5/42 |
| Mean age, years | 54.7 | 3–90 | 57.4 | 6–90 |
| Male gender | 74.8% | 237/317 | 78.4% | 171/218 |
| Underlying disease: | ||||
| Diabetes | 42.1% | 118/280 | 33.1% | 52/157 |
| Cancer | 6.2% | 12/194 | 16.4% | 11/67 |
| IgA-IRGN n = 336 | SAGN n = 218 | |||
|---|---|---|---|---|
| Causative bacteria | ||||
| Staphylococcal strain: | 58.4% | 185/317 | 100.0% | 218/218 |
| S. aureus | 54.9% | 174/305 | 81.7% | 178/218 |
| S. epidermidis | 1.7% | 5/298 | 6.9% | 15/218 |
| Other Staphylococcus | 1.7% | 5/298 | 11.5% | 25/218 |
| Streptococcus strain | 5.5% | 17/310 | 0.5% | 1/211 |
| Other bacteria | 21.0% | 65/310 | 3.3% | 7/211 |
| Unknown/not detected | 23.6% | 73/310 | 0% | 0/211 |
| Infection site: | ||||
| Cellulitis/skin infection | 25.1% | 68/271 | 23.6% | 45/191 |
| Endocarditis | 4.1% | 11/271 | 12.6% | 24/191 |
| Osteomyelitis/joint infection | 11.4% | 31/271 | 17.3% | 33/191 |
| Respiratory infection | 18.8% | 51/271 | 12.0% | 23/191 |
| Visceral abscess | 9.2% | 25/271 | 15.7% | 30/191 |
| Others | 22.9% | 62/271 | 19.4% | 37/191 |
| Unknown | 17.0% | 46/271 | 0% | 0/271 |
| IgA-IRGN n = 336 | SAGN n = 218 | |||
|---|---|---|---|---|
| Clinical features: | ||||
| AKI or RPGN | 79.1% | 178/225 | 75.0% | 78/104 |
| Nephrotic syndrome | 59.1% | 101/171 | 52.4% | 75/143 |
| Proteinuria | 98.9% | 183/185 | 98.4% | 183/186 |
| Hematuria | 95.0% | 226/238 | 91.4% | 106/116 |
| Purpura | 40.7% | 46/113 | 29.5% | 49/166 |
| Laboratory data: | ||||
| Excretion of urinary protein, g/day | 4.79 (n = 272) | 0–19.06 | 4.68 (n = 125) | 0–16.0 |
| Serum creatinine level, mg/dL | 3.54 (n = 312) | 0.38–21.94 | 3.61 (n = 138) | 0.38–10.4 |
| Serum IgA level, mg/dL | 642.5 (n = 98) | 97–1850 | 685.4 (n = 77) | 97–1850 |
| Elevated serum IgA level | 76.0% | 73/96 | 78.0% | 46/59 |
| Decreased serum C3 level | 33.3% | 74/222 | 34.3% | 60/175 |
| Decreased serum C4 level | 11.0% | 18/163 | 15.5% | 26/168 |
| Positive test for ANCA | 5.1% | 5/99 | 11.4% | 12/105 |
| IgA-IRGN n = 336 | SAGN n = 218 | |||
|---|---|---|---|---|
| Light microscopy: | ||||
| Mesangial hypercellularity | 73.9% | 209/283 | 64.1% | 66/103 |
| Endocapillary proliferation | 71.7% | 203/283 | 58.6% | 106/181 |
| Membranoproliferative GN | 5.9% | 16/270 | 7.8% | 8/103 |
| Necrotizing/crescentic GN | 9.1% | 21/231 | 10.7% | 11/103 |
| Presence of crescents | 56.1% | 143/255 | 47.6% | 78/164 |
| Immunofluorescence: | ||||
| Positive staining with IgG | 44.4% | 118/266 | 51.3% | 79/154 |
| Positive staining with IgA | 100.0% | 303/303 | 85.1% | 149/175 |
| Positive staining with C3 | 97.0% | 291/300 | 90.4% | 161/178 |
| Electron microscopy: | ||||
| Subepithelial EDD | 54.3% | 119/219 | 40.5% | 62/153 |
| Subendothelial EDD | 43.1% | 81/188 | 47.1% | 33/70 |
| Intramembranous EDD | 15.6% | 31/199 | 6.9% | 4/58 |
| Mesangial EDD | 78.2% | 147/188 | 85.3% | 64/75 |
| Humps | 37.5% | 90/240 | 31.7% | 46/145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takayasu, M.; Hirayama, K.; Shimohata, H.; Kobayashi, M.; Koyama, A. Staphylococcus aureus Infection-Related Glomerulonephritis with Dominant IgA Deposition. Int. J. Mol. Sci. 2022, 23, 7482. https://doi.org/10.3390/ijms23137482
Takayasu M, Hirayama K, Shimohata H, Kobayashi M, Koyama A. Staphylococcus aureus Infection-Related Glomerulonephritis with Dominant IgA Deposition. International Journal of Molecular Sciences. 2022; 23(13):7482. https://doi.org/10.3390/ijms23137482
Chicago/Turabian StyleTakayasu, Mamiko, Kouichi Hirayama, Homare Shimohata, Masaki Kobayashi, and Akio Koyama. 2022. "Staphylococcus aureus Infection-Related Glomerulonephritis with Dominant IgA Deposition" International Journal of Molecular Sciences 23, no. 13: 7482. https://doi.org/10.3390/ijms23137482