
Covered Stent Herniation into Coronary Aneurysm Sac—A Case-Inspired Review of Neurointerventional Realignment Techniques
Abstract
:1. Introduction
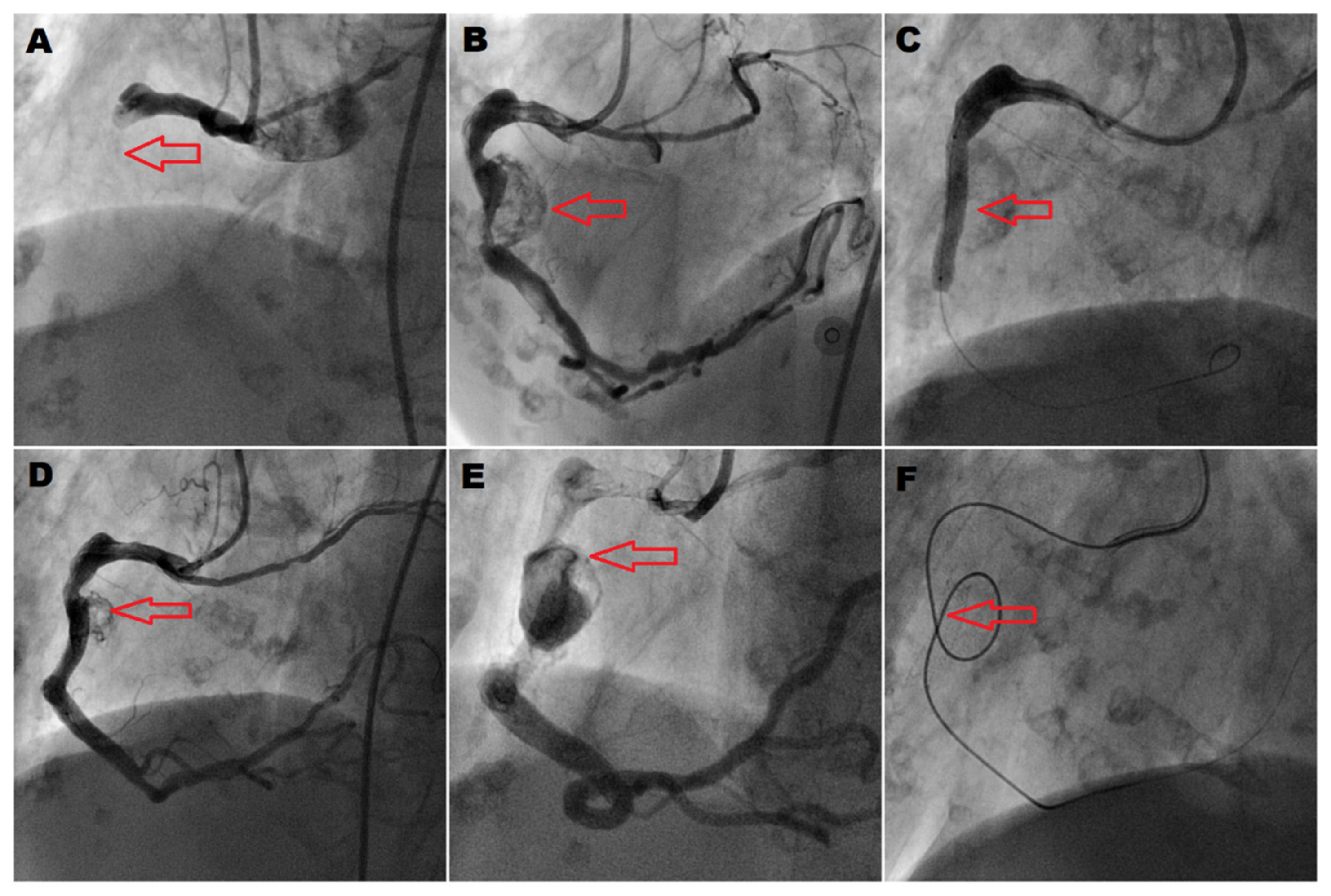
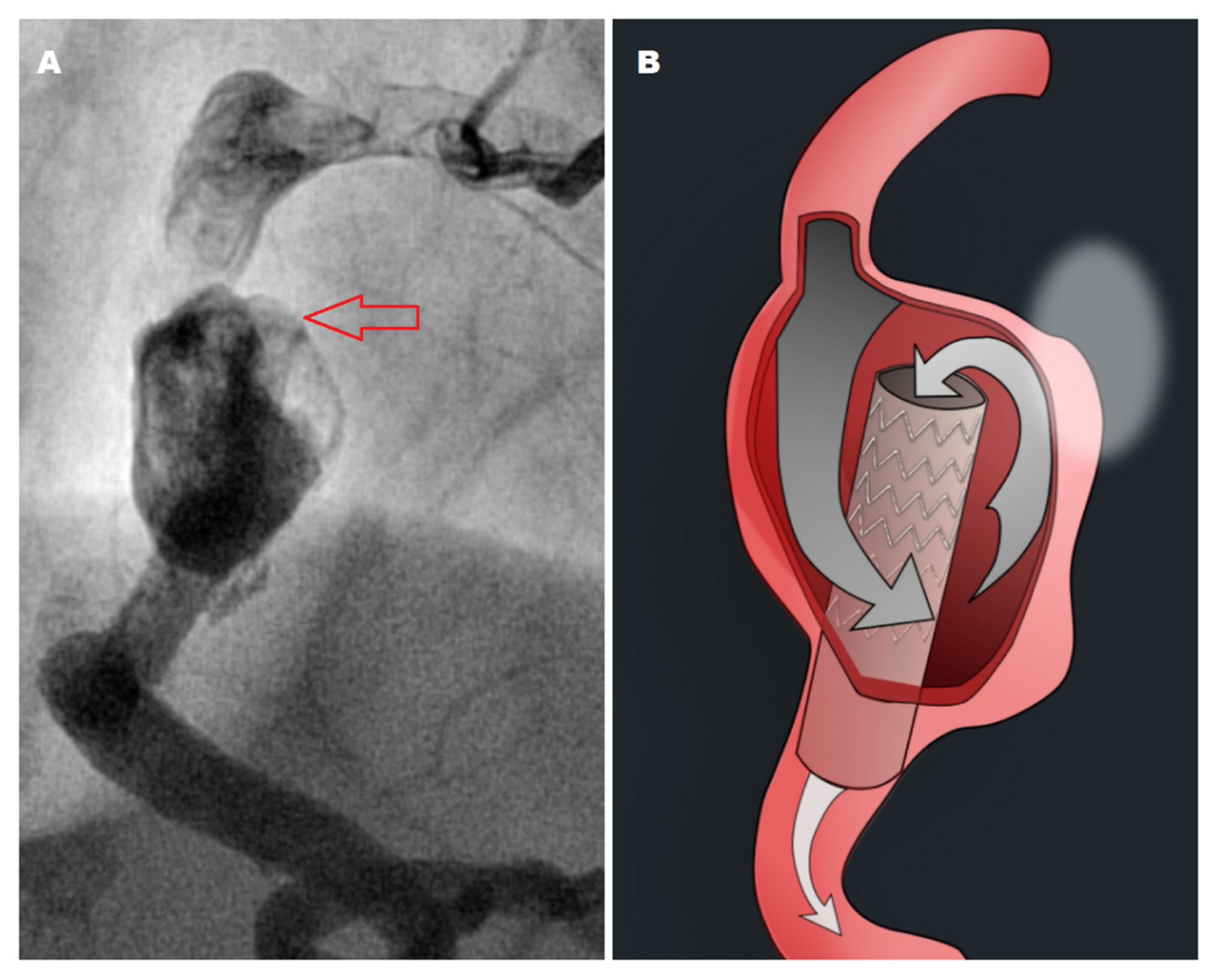
2. Case Presentation
3. Discussion
3.1. Pitfalls of Coronary Aneurysm Sizing
3.2. Complications of Covered Stent Deployment
3.3. Coronary and Neurointerventional Techniques for Management of Stent Migration
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Núñez-Gil, I.J.; Cerrato, E.; Bollati, M.; Nombela-Franco, L.; Terol, B.; Alfonso-Rodríguez, E.; Camacho Freire, C.J.; Villablanca, P.A.; Amat Santos, I.J.; de la Torre Hernández, J.M.; et al. Coronary artery aneurysms, insights from the international coronary artery aneurysm registry (CAAR). Int. J. Cardiol. 2020, 299, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Khubber, S.; Chana, R.; Meenakshisundaram, C.; Dhaliwal, K.; Gad, M.; Kaur, M.; Banerjee, K.; Verma, B.R.; Shekhar, S.; Khan, M.Z.; et al. Coronary artery aneurysms: Outcomes following medical, percutaneous interventional and surgical management. Open Heart 2021, 8, e001440. [Google Scholar] [CrossRef] [PubMed]
- Aoki, J.; Kirtane, A.; Leon, M.B.; Dangas, G. Coronary artery aneurysms after drug-eluting stent implantation. JACC Cardiovasc. Interv. 2008, 1, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Yip, H.K.; Chen, M.C.; Wu, C.J.; Hang, C.L.; Hsieh, K.Y.; Fang, C.Y.; Yeh, K.H.; Fu, M. Clinical features and outcome of coronary artery aneurysm in patients with acute myocardial infarction undergoing a primary percutaneous coronary intervention. Cardiology 2002, 98, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Campanile, A.; Sozzi, F.B.; Consonni, D.; Piscione, F.; Sganzerla, P.; Indolfi, C.; Stabile, A.; Migliorini, A.; Antoniucci, D.; Ferraresi, R.; et al. Primary PCI for the treatment of ectatic infarct-related coronary artery. Minerva Cardioangiol. 2014, 62, 327–333. [Google Scholar]
- Ipek, G.; Gungor, B.; Karatas, M.B.; Onuk, T.; Keskin, M.; Tanik, O.; Hayiroglu, M.I.; Oz, A.; Borklu, E.B.; Bolca, O.; et al. Risk factors and outcomes in patients with ectatic infarct-related artery who underwent primary percutaneous coronary intervention after ST elevated myocardial infarction. Catheter. Cardiovasc. Interv. 2016, 88, 748–753. [Google Scholar] [CrossRef]
- Nagaraja, V.; Schwarz, K.; Moss, S.; Kwok, C.S.; Gunning, M. Outcomes of patients who undergo percutaneous coronary intervention with covered stents for coronary perforation: A systematic review and pooled analysis of data. Catheter. Cardiovasc. Interv. 2020, 96, 1360–1366. [Google Scholar] [CrossRef]
- Hachinohe, D.; Latib, A.; Laricchia, A.; Iannopollo, G.; Demir, O.M.; Ancona, M.B.; Mangieri, A.; Regazzoli, D.; Giannini, F.; Azzalini, L.; et al. Long-term follow-up of covered stent implantation for various coronary artery diseases. Catheter. Cardiovasc. Interv. 2019, 94, 571–577. [Google Scholar] [CrossRef]
- Jurado-Román, A.; Rodríguez, O.; Amat, I.; Romani, S.A.; García-Touchard, A.; Cruz-González, I.; Benito-González, T.; Fernández-Cisnal, A.; Córdoba-Soriano, J.G.; Subinas, A.; et al. Clinical Outcomes After Implantation of Polyurethane-Covered Cobalt-Chromium Stents: Insights from the Papyrus-Spain Registry. Cardiovasc. Revasc. Med. 2021, 29, 22–28. [Google Scholar] [CrossRef]
- Takano, M.; Yamamoto, M.; Inami, S.; Xie, Y.; Murakami, D.; Okamatsu, K.; Ohba, T.; Seino, Y.; Mizuno, K. Delayed endothelialization after polytetrafluoroethylene-covered stent implantation for coronary aneurysm. Circ. J. 2009, 73, 190–193. [Google Scholar] [CrossRef]
- Harnek, J.; James, S.K.; Lagerqvist, B. Very long-term outcome of coronary covered stents: A report from the SCAAR registry. EuroIntervention 2019, 14, 1660–1667. [Google Scholar] [CrossRef] [PubMed]
- Bartuś, J.; Januszek, R.; Hudziak, D.; Kołodziejczak, M.; Kuźma, L.; Tajstra, M.; Figatowski, T.; Pawłowski, T.; Gruz-Kwapisz, M.; Smolarek-Nicpoń, M.; et al. Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry). J. Clin. Med. 2021, 10, 5441. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Cioffi, G.M.; Yildirim, M.; Moccetti, F.; Wolfrum, M.; Attinger, A.; Toggweiler, S.; Kobza, R.; Cuculi, F. “Burying” covered coronary stents under drug-eluting stents: A novel approach to ensure long-term stent patency. Cardiol. J. 2023, 14, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Boi, A.; Sanna, F.; Rossi, A.; Loi, B. Exclusion of a giant saphenous vein graft pseudo-aneurysm with a “double-layer bridging” technique. Cardiovasc. Revasc. Med. 2018, 19, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Will, M.; Kwok, C.S.; Nagaraja, V.; Potluri, R.; Weiss, T.W.; Mascherbauer, J.; Schwarz, K. Outcomes of Patients Who Undergo Elective Covered Stent Treatment for Coronary Artery Aneurysms. Cardiovasc. Revasc. Med. 2022, 36, 91–96. [Google Scholar] [CrossRef]
- Papafaklis, M.I.; Sianos, G.; Cost, B.; Vaina, S.; Manginas, A.; Dardas, P.S.; Tsikaderis, D.; van Mieghem, C.A.; Michalis, L.K.; Serruys, P.W. Clinical and angiographic follow-up after overlapping implantation of polytetrafluoroethylene covered stents with drug eluting stents. EuroIntervention 2006, 2, 218–223. [Google Scholar] [PubMed]
- Hou, J.; Jia, H.; Huang, X.; Yu, H.; Ren, X.; Fang, Y.; Han, Z.; Yang, S.; Meng, L.; Zhang, S.; et al. Optical coherence tomographic observations of polytetrafluoroethylene-covered sirolimus-eluting coronary arterial stent. Am. J. Cardiol. 2013, 111, 1117–1122. [Google Scholar] [CrossRef]
- Visrodia, K.; Matthews, R.; Shriki, J. Double-stent method: An alternative technique to treat coronary artery aneurysms. Catheter. Cardiovasc. Interv. 2011, 77, 1036–1041. [Google Scholar] [CrossRef]
- Dai, H.L.; Guang, X.F.; Jiang, L.H.; Xue, Q.; Zhang, W.H. Overlapping-Stent Intervention Treatment of a Giant Right Coronary Artery Pseudoaneurysm. JACC Cardiovasc. Interv. 2015, 8, e255–e256. [Google Scholar] [CrossRef]
- Barioli, A.; Pellizzari, N.; Favero, L.; Cernetti, C. Unconventional treatment of a giant coronary aneurysm presenting as ST-elevation myocardial infarction: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab385. [Google Scholar] [CrossRef]
- Danzi, G.B.; Pomidossi, G.A.; Casolo, F.; Centola, M.; Ferraresi, R.; Lotan, C. A new device to seal large coronary aneurysms: A case report. J. Med. Case Rep. 2010, 4, 238. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuka, M.; Uchida, E.; Yamaguchi, H.; Nakajima, T.; Akazawa, H.; Funabashi, N.; Kobayashi, Y.; Shiojima, I.; Komuro, I. Coronary aneurysm reduced after coronary stenting. Int. J. Cardiol. 2007, 121, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Khemani, H.; Singla, R.; Shaikh, S.; Patil, V.; Bansal, N.O. Intravascular Ultrasound-Guided Management of Proximal Left Anterior Descending Artery Aneurysm With Covered Stent—A Case Report. Cardiol. Res. 2018, 9, 318–323. [Google Scholar] [CrossRef] [PubMed]
- La Manna, A.; Geraci, S.; Tamburino, C. A self-expandable coronary stent system to treat complex coronary stenosis complicated by poststenotic aneurysm: An optical coherence tomographic evidence-based case report. J. Invasive Cardiol. 2011, 23, E277–E280. [Google Scholar]
- López-Meneses, M.; Alfonso, F.; Fernández-Ortíz, A.; Escaned, J.; Flores, A.; García, P.; Arias, J.; Sabaté, M.; Hernández, R.; Bañuelos, C.; et al. Treatment of a giant coronary aneurysm with a novel technique: Scaffolding (tunnel) stenting to support PTFE-covered stents: Insights from intravascular ultrasound. J. Invasive Cardiol. 2002, 14, 273–276. [Google Scholar]
- Dutary, J.; Zakhem, B.; DE Lucas, C.B.; Paulo, M.; Gonzalo, N.; Alfonso, F. Treatment of a giant coronary artery aneurysm: Intravascular ultrasound and optical coherence tomography findings. J. Interv. Cardiol. 2012, 25, 82–85. [Google Scholar] [CrossRef]
- Shah, S.C.; Patel, T.M.; Patel, G.A.; Pancholy, S.B. Percutaneous Treatment of Long Coronary Aneurysms: Novel Technique for Increased Efficacy and Safety. JACC Case Rep. 2019, 1, 628–632. [Google Scholar] [CrossRef]
- Orlic, D.; Vitrella, G.; Corvaja, N.; Colombo, A. New technique to seal a long giant coronary aneurysm with PTFE-covered stents: A case report. Catheter. Cardiovasc. Interv. 2006, 67, 41–45. [Google Scholar] [CrossRef]
- Megaly, M.; Zordok, M.; Mentias, A.; Chugh, Y.; Buttar, R.S.; Basir, M.B.; Burke, M.N.; Karmpaliotis, D.; Azzalini, L.; Alaswad, K.; et al. Complications and Failure Modes of Covered Coronary Stents: Insights From the MAUDE Database. Cardiovasc. Revasc. Med. 2022, 35, 157–160. [Google Scholar] [CrossRef]
- Zvavanjanja, R.C. Percutaneous retrieval of migrated Viabahn stent from a segmental pulmonary artery. CVIR Endovasc. 2020, 6, 1. [Google Scholar] [CrossRef]
- Al-Obaidi, F.R.; Al-Ali, M.H.; Al-Kinani, T.; Al-Myahi, M. Covered Stent Embolization: A case of acute coronary intervention with a series of multiple complications. Interv. Akut. Kardiol. 2020, 19, 232–235. [Google Scholar] [CrossRef]
- Panigrahi, N.K.; Raju, J.; Baruah, D.K.; Srinivas, M.; Varma, R.K. Extraluminal Migration of a Drug-Eluting Stent Into a Thrombosed Coronary Aneurysm With Preserved Antegrade Flow in the Right Coronary Artery. JACC Cardiovasc. Interv. 2017, 10, 834–836. [Google Scholar] [CrossRef]
- Virmani, R.; Robinowitz, M.; Atkinson, J.B.; Forman, M.B.; Silver, M.D.; McAllister, H.A. Acquired coronary arterial aneurysms: An autopsy study of 52 patients. Hum. Pathol. 1986, 17, 575–583. [Google Scholar] [CrossRef]
- Kaneko, U.; Kashima, Y.; Hashimoto, M.; Fujita, T. Very Late Stent Migration Within a Giant Coronary Aneurysm in a Patient With Kawasaki Disease: Assessment With Multidetector Computed Tomography. JACC Cardiovasc. Interv. 2017, 10, 1799–1800. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.H.; Huang, H.L.; Ko, Y.L. Acute Myocardial Infarction Due to Prolapse of Covered Stent Into Coronary Artery Aneurysm. JACC Cardiovasc. Interv. 2018, 11, e147–e148. [Google Scholar] [CrossRef]
- Wu, Z.B.; Wang, S.; Song, L.G.; Yang, X.J.; Mu, S.Q. Pipeline Embolization Device for Salvage Treatment of a Willis Covered Stent Prolapse Into the Aneurysmal Sac. Front. Neurol. 2019, 10, 1099. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, V.M.; Carlson, A.P.; Mokin, M.; Cherian, J.; Chen, S.R.; Puri, A.; Kan, P. Prolapse of the Pipeline embolization device in aneurysms: Incidence, management, and outcomes. Neurosurg. Focus 2017, 42, E16. [Google Scholar] [CrossRef]
- Pan, L.; Hum, B.; David, C.; Lee, S.K. Management of intraprocedural spontaneous stent migration into target aneurysm during stent-assisted coiling procedure. J. Neurointerv. Surg. 2010, 2, 352–355. [Google Scholar] [CrossRef] [PubMed]
- El Ouadih, Y.; Coll, G.; Jean, B.; Coste, A.; Chaix, R.; Sakka, L.; Lemaire, J.J. A rare complication of flow diverter: Delayed migration causing aneurysm expansion and brainstem compression. Br. J. Neurosurg. 2019, 37, 741–744. [Google Scholar] [CrossRef]
- Lubicz, B.; Collignon, L.; Raphaeli, G.; Pruvo, J.P.; Bruneau, M.; De Witte, O.; Leclerc, X. Flow-diverter stent for the endovascular treatment of intracranial aneurysms: A prospective study in 29 patients with 34 aneurysms. Stroke 2010, 41, 2247–2253. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.E.; Gomori, J.M.; Moscovici, S.; Leker, R.R.; Itshayek, E. Delayed complications after flow-diverter stenting: Reactive in-stent stenosis and creeping stents. J. Clin. Neurosci. 2014, 21, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Chalouhi, N.; Tjoumakaris, S.I.; Gonzalez, L.F.; Hasan, D.; Pema, P.J.; Gould, G.; Rosenwasser, R.H.; Jabbour, P.M. Spontaneous delayed migration/shortening of the pipeline embolization device: Report of 5 cases. AJNR Am. J. Neuroradiol. 2013, 34, 2326–2330. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Galdámez, M.; Ortega-Quintanilla, J.; Hermosín, A.; Crespo-Vallejo, E.; Ailagas, J.J.; Pérez, S. Novel balloon application for rescue and realignment of a proximal end migrated pipeline flex embolization device into the aneurysmal sac: Complication management. BMJ Case Rep. 2016, 2016, bcr2016012263. [Google Scholar] [CrossRef] [PubMed]
- Crowley, R.W.; Abla, A.A.; Ducruet, A.F.; McDougall, C.G.; Albuquerque, F.C. Novel application of a balloon-anchoring technique for the realignment of a prolapsed pipeline embolization device: A technical report. J. Neurointerv. Surg. 2014, 6, 439–444. [Google Scholar] [CrossRef]
- Jagadeesan, B.D.; Sandhu, D.; Hong, K.J.; Roshan Khanipour, S.; Grande, A.W.; Tummala, R.P. Salvage of Herniated Flow Diverters Using Stent and Balloon Anchoring Techniques: A Technical Note. Interv. Neurol. 2017, 6, 31–35. [Google Scholar] [CrossRef]
- Ding, D.; Starke, R.M.; Evans, A.J.; Jensen, M.E.; Liu, K.C. Balloon anchor technique for pipeline embolization device deployment across the neck of a giant intracranial aneurysm. J. Cerebrovasc. Endovasc. Neurosurg. 2014, 16, 125–130. [Google Scholar] [CrossRef]
- Bhoopalan, K.; Rajendran, R.; Alagarsamy, S.; Kesavamoorthy, N. Successful extraction of refractory thrombus from an ectatic coronary artery using stent retriever during primary angioplasty for acute myocardial infarction: A case report. Eur. Heart J. Case Rep. 2019, 3, yty161. [Google Scholar] [CrossRef]
- Spirito, A.; Quagliana, A.; Coiro, M.; Melaku, G.D.; Vandenberghe, S.; Leibundgut, G.; Häner, J.; Moccetti, M.; Araco, M.; Garcia-Garcia, H.M.; et al. A prospective, first-in-human use of the NeVa mechanical thrombectomy device for patients with acute coronary syndromes. EuroIntervention 2022, 18, 242–252. [Google Scholar] [CrossRef]
- Hanna, E.B.; Rossen, J.; Eustes, A.S.; Dayal, S. Heavy lone coronary artery thrombosis treated by stent retriever, in the setting of COVID-19 infection. Catheter. Cardiovasc. Interv. 2022, 99, 457–461. [Google Scholar] [CrossRef]
- Chapot, R.; Stracke, C.P.; Wallocha, M.; Rikhtegar, R.; Yamac, E.; Mosimann, P.J. Bailout stentectomy of 47 self-expandable intracranial stents. J. Neurointerv. Surg. 2022, 14, 160–163. [Google Scholar] [CrossRef]
- Mitchell, B.; Jou, L.D.; Mawad, M. Retrieval of distorted pipeline embolic device using snare-loop. J. Vasc. Interv. Neurol. 2014, 7, 1–4. [Google Scholar] [PubMed]
- Hauck, E.F.; Natarajan, S.K.; Langer, D.J.; Hopkins, L.N.; Siddiqui, A.H.; Levy, E.I. Retrograde trans-posterior communicating artery snare-assisted rescue of lost access to a foreshortened pipeline embolization device: Complication management. Neurosurgery 2010, 67 (Suppl. S2), 495–502. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.M.; Guo, X.F.; Midia, M. Repositioning of covered stents: The grip technique. Cardiovasc. Interv. Radiol. 2011, 34, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Capretti, G.; Mitomo, S.; Giglio, M.; Carlino, M.; Colombo, A.; Azzalini, L. Subintimal Crush of an Occluded Stent to Recanalize a Chronic Total Occlusion Due to In-Stent Restenosis: Insights From a Multimodality Imaging Approach. JACC Cardiovasc. Interv. 2017, 10, e81–e83. [Google Scholar] [CrossRef]
- Chen, M.; Goldstein-Smith, L. Endovascular rescue of a misshapen intracranial stent: Report of two cases. J. Neurointerv. Surg. 2011, 3, 25–26. [Google Scholar] [CrossRef]
- Samaan, A.; Amin, A.; Wagdy Shaker, K.; Osman, A.; El Mozy, W.; ElGuindy, A. Percutaneous Management of a Giant Left Anterior Descending Artery Aneurysm via the Retrograde Approach. Circ. Cardiovasc. Interv. 2018, 11, e006967. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Realignment Technique | Elements of the Technique | Technique Description |
|---|---|---|
| Parallel balloon inflation |  | A parallel balloon is inflated to push the stent out of the aneurysm sac and enable a rewiring of the distal vessel [43]. |
| Balloon inflation at prolapsed stent edge |  | If enough space is left at the herniated stent edge to wire it and pass another device, several balloon techniques may be employed, including balloon inflation at the prolapsed stent edge to coaxially realign the prosthesis [44,45,46]. |
| Distal balloon anchoring |  | In this technique, a balloon is deployed distal to the stent with gentle traction applied to use the balloon shaft for stent repositioning. |
| Stent retriever-assisted repositioning |  | Stent retrievers may also be considered for stent rearrangement with a technique similar to the one used for bailout stentectomy of intracranial stents, whereby a stent retriever is deployed inside a prolapsed stent and pulled back to reposition it coaxially [50]. |
| Snare-assisted stent realignment |  | For proximal stent edge realignment, snares may be used, preferably with a deflated balloon inserted distally through the stent to expand the snare-crimped stent after its rearrangement [51,52,53]. |
| Snare-and-balloon technique |  | A balloon is deployed at the prolapsed proximal edge of stent to be caught by a snare and repositioned coaxially. |
| Stent crush |  | The prolapsed stent is crushed with a balloon, with subsequent deployment of additional covered stents to exclude the aneurysm. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaudel, J.; Radowski, P.; Trenkner, W.; Glaza, M.; Pawłowski, K.; Surman, D.; Krasowski, W.; Szołkiewicz, M. Covered Stent Herniation into Coronary Aneurysm Sac—A Case-Inspired Review of Neurointerventional Realignment Techniques. J. Vasc. Dis. 2023, 2, 402-412. https://doi.org/10.3390/jvd2040031
Klaudel J, Radowski P, Trenkner W, Glaza M, Pawłowski K, Surman D, Krasowski W, Szołkiewicz M. Covered Stent Herniation into Coronary Aneurysm Sac—A Case-Inspired Review of Neurointerventional Realignment Techniques. Journal of Vascular Diseases. 2023; 2(4):402-412. https://doi.org/10.3390/jvd2040031
Chicago/Turabian StyleKlaudel, Jacek, Piotr Radowski, Wojciech Trenkner, Michał Glaza, Krzysztof Pawłowski, Dariusz Surman, Włodzimierz Krasowski, and Marek Szołkiewicz. 2023. "Covered Stent Herniation into Coronary Aneurysm Sac—A Case-Inspired Review of Neurointerventional Realignment Techniques" Journal of Vascular Diseases 2, no. 4: 402-412. https://doi.org/10.3390/jvd2040031